







Physician Impairment
The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence, published by the American Medical Association’s (AMA) Council on Mental Health in The Journal of the American Medical Association in 1973,1 recommended that physicians do a better job of helping colleagues impaired by mental illness, alcoholism or drug dependence. The AMA defined an “impaired physician” as “a physician who is unable to practice medicine with reasonable skill and safety to patients because of mental illness or excessive use or abuse of drugs, including alcohol.”
Recognition of physician impairment in the 1970s by both the medical community and the general public led to the development of “impaired physician” programs with the purpose of both helping impaired doctors and protecting the public from them.
 The 1975 media coverage of the deaths of Drs. Stewart and Cyril Marcus brought the problem of impaired physicians into the public eye.
The 1975 media coverage of the deaths of Drs. Stewart and Cyril Marcus brought the problem of impaired physicians into the public eye.  Leading experts in the field of Infertility Medicine, the twin gynecologists were found dead in their Upper East Side apartment from drug withdrawal that New York Hospital was aware of but did nothing about. Performing surgery with trembling hands and barely able to stand, an investigation revealed that nothing had been done to help the Marcus brothers with their addiction or protect patients. They were 45 –years old.
Leading experts in the field of Infertility Medicine, the twin gynecologists were found dead in their Upper East Side apartment from drug withdrawal that New York Hospital was aware of but did nothing about. Performing surgery with trembling hands and barely able to stand, an investigation revealed that nothing had been done to help the Marcus brothers with their addiction or protect patients. They were 45 –years old.
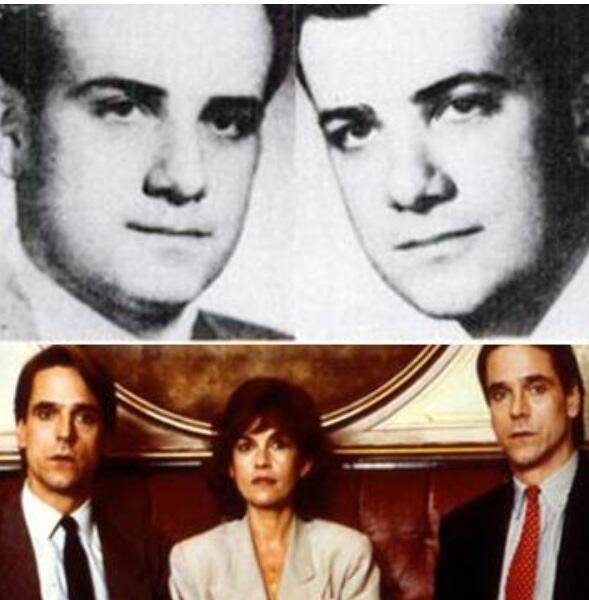
Top: Twin Gynecologists Stewart and Cyril Marcus
Bottom: The Movie “Dead Ringers” starring Jeremy Irons based on the Marcus twins
Although the New York State Medical Society had set up its own voluntary program for impaired physicians three years earlier, the Marcus case prompted the state legislature to pass a law that doctors had to report any colleague suspected of misconduct to the state medical board and those who didn’t would face misconduct charges themselves.
Physician Health Programs
Physician health programs (PHPs) existed in almost every state by 1980. Often staffed by volunteer physicians and funded by State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referral.
As an alternative to discipline the introduction of PHPs created a perception of medical boards as “enforcers” whose job was to sanction and discipline whereas PHPs were perceived as “rehabilitators” whose job was to help sick physicians recover. One of many false dichotomies this group uses and it is perhaps this perceived benevolence that created an absence of the need to guard.
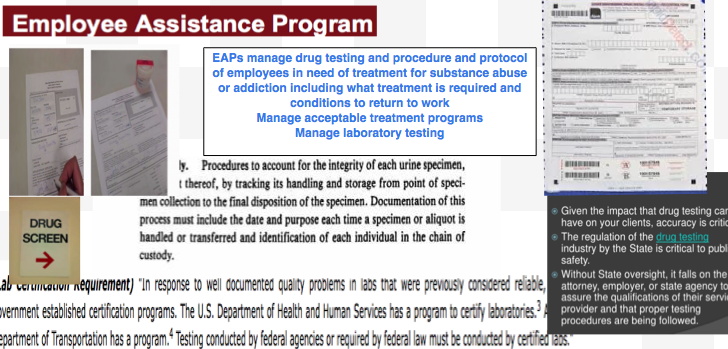
Employee Assistance Programs for Doctors
Physician Health Programs (PHPs) are the equivalent of Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess, and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems.
Most EAPs, however, were developed with the collaboration of workers unions or some other group supporting the rights and best interests of the employees. PHPs were created and evolved without any oversight or regulation.
The American Society of Addiction Medicine can trace its roots to the 1954 founding of theNew York City Medical Society on Alcoholism (NYCMSA) by Ruth Fox, M.D whose husband died from alcoholism.
The society, numbering about 100 members, established itself as a national organization in1967, the American Medical Society on Alcoholism (AMSA).
By 1970 membership was nearly 500.
In 1973 AMSA became a component of the National Council on Alcoholism (NCA) in a medical advisory capacity until 1983.
But by the mid 1980’s ASAM’s membership became so large that they no longer needed to remain under the NCADD umbrella.
In 1985 ASAM’s first certification exam was announced. According to Dr. Bean-Bayog, chair of the Credentialing Committee, “a lot of people in the alcoholism field have long wanted physicians in the field to have a high level of skills and scientific credibility and for this body of knowledge to be accredited.”2 And in 1986 662 physicians took the first ASAM Certification Exam.

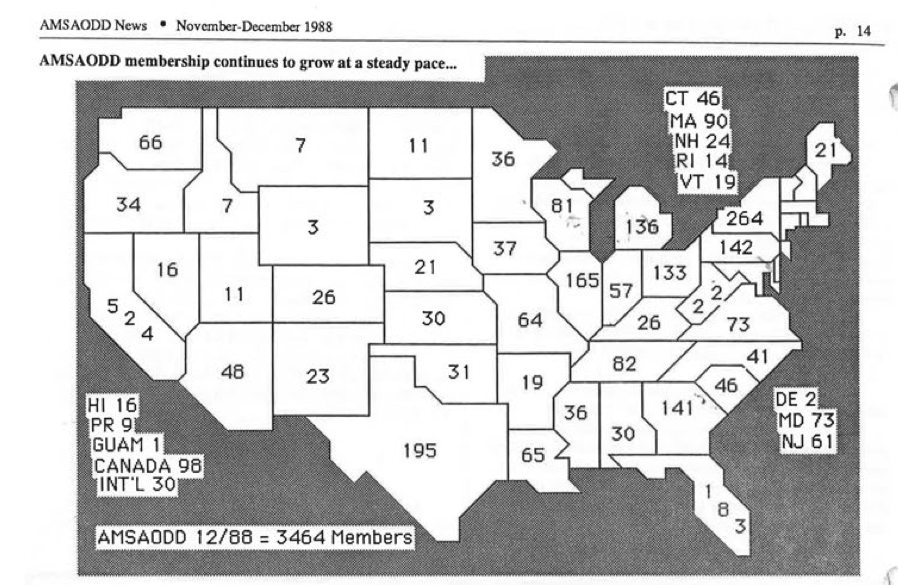
By 1988 membership was over 2,800 with 1,275 of these physicians “certified” as “having demonstrated knowledge and expertise in alcoholism and other drug dependencies commensurate with the standards set forth by the society.”3 “The formation of State Chapters began with California, Florida, Georgia, and Maryland submitting requests.4
In 1988 the AMA House of Delegates voted to admit ASAM to the House. According to ASAM News this “legitimizes the society within the halls of organized medicine.”2
By 1993 ASAM had a membership of 3,500 with a total of 2,619 certifications in Addiction Medicine. The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”5
certifications in Addiction Medicine. The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”5
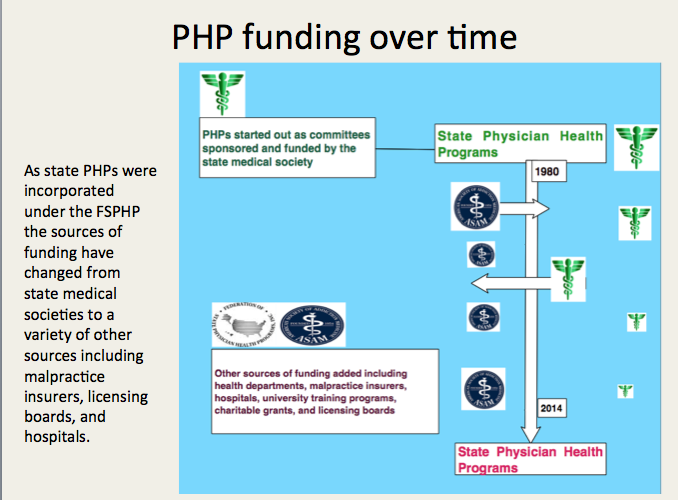
Many of these physicians joined state PHPs and over time have taken over under the umbrella of the FSPHP.
Others became medical directors of treatment centers such as Hazelden, Marworth and Talbott.



“As we express our gratitude, we must never forget that the highest appreciation is not to utter words, but to live by them.”– Thanksgiving Day Proclamation 1963—John F. Kennedy.
 Let us therefore proclaim our gratitude to Providence for manifold blessings–let us be humbly thankful for inherited ideals–and let us resolve to share those blessings and those ideals with our fellow human beings throughout the world.
Let us therefore proclaim our gratitude to Providence for manifold blessings–let us be humbly thankful for inherited ideals–and let us resolve to share those blessings and those ideals with our fellow human beings throughout the world.
On that(this) day let us gather in sanctuaries dedicated to worship and in homes blessed by family affection to express our gratitude for the glorious gifts of God; and let us earnestly and humbly pray that He will continue to guide and sustain us in the great unfinished tasks of achieving peace, justice, and understanding among all men and nations and of ending misery and suffering wherever they exist.
–Thanksgiving Day, 1963



The Medical Profession, Moral Entrepreneurship, Moral Panics, and Social Control.
“Few, no matter how desperate, seek help of their own accord.” says Dr. Marv Seppala, M.D., Chief Medical Officer at Hazelden, one of the “PHP-approved” drug and alcohol assessment and treatment centers located in Center City, Minnesota. “Physicians are intelligent and skilled at hiding their addictions.”
“They’re often described as the best workers in the hospital,” he says. “They’ll overwork to compensate for other ways in which they may be falling short, and to protect their supply. They’ll sign up for extra call and show up for rounds they don’t have to do.”
In reality this is ludicrous–knee slapping absurd. If the results of this authoritative opinion were not so dire these statements would, in fact, be comical. Such is not the case, however, and opinions like Seppala’s have been taken at face value and, as a result, the aftermath has been and continues to be tragedy.
Addiction, alcoholism and substance abuse to any significant degree produce both physiological and behavioral manifestations in the user. It is cause and effect. Pathophysiology conforms to law of nature and not the whims of the impaired physician movement.
What anomalous aspect of intelligence or special skill set would enable a doctor to hide an addiction?
The ASAM definition of addiction is characterized by cognitive, behavioral and emotional changes which include “impaired control” so how would intelligence rein it in? Furthermore, what unique logical, rational, analytical, factual, abstract, intuitive or objective aspect of intelligence is responsible for this preternatural fortitude?
How is the intelligence of a doctor any different from the intelligence of any other human being? And what prodigious abilities do doctors have that enable them them to cloak the behavioral manifestations and stave off the physical consequences chemical addiction to such a degree that they are able to maintain the facade of being “described as the best workers in the hospital?” Is it an innate inborn endowment or an esoteric knack acquired during medical training?
 What ability and artistry would allow a profession to weave such a web of fortitude that they can convincingly shroud the myriad signs and symptoms of drug and alcohol abuse unlike the regular folk? Perhaps access to ophthalmic vasoconstrictors and beta blockers to temper the pupillary dilation and tremulousness associated with stimulants or botox and a testosterone patch to mask the skin changes and maintain lean muscle mass in the throes of alcoholism?
What ability and artistry would allow a profession to weave such a web of fortitude that they can convincingly shroud the myriad signs and symptoms of drug and alcohol abuse unlike the regular folk? Perhaps access to ophthalmic vasoconstrictors and beta blockers to temper the pupillary dilation and tremulousness associated with stimulants or botox and a testosterone patch to mask the skin changes and maintain lean muscle mass in the throes of alcoholism?
How does overworking “protect their supply” and why would they keep it at the hospital? These people have prescription pads and last I checked there were no cocktails shakers or bottles of Jameson in the doctors lounge.
And for the life of me I cannot comprehend why an alcoholic or addict doctor would sign up for extra call and show up for rounds on his day off. What would be the point?
In reality a doctor with a drug or alcohol problem would be erratic with call and show up late for rounds.
This is just another example of authoritative opinion with no substantive value. It is moral entrepreneurship at its finest; the fallacy of appeal to authority and secret knowledge.
If Seppala were asked to provide the evidence-base and rationality of these statements he would be hard pressed to do so. The question would be met with deflection, logical fallacy, references to the opinions of like minds and thought-stopping memes. “You need a check-up from the neck up,” your best thinking got you here,” there is no “I” in “team,” “denial isn’t just a river in Egypt.” Oh, yeah? well “Rogue” isn’t just a river in Oregon and, while we are at it, “Boring” isn’t just a town!
It is this type of misinformation and propaganda that allows the “impaired physician movement” to drag away the “best worker in the hospital” and deem him “in denial.”
“We were so surprised. We didn’t even know he had a problem” say the nurses, patients and colleagues left behind.
Well the truth is he probably didn’t!
Blind-faith and unquestioning allegiance to expert authority deflects scrutiny and analysis. Few red flags are raised as this type of moral preening promotes misguided plausibility and complacency in the belief that these are indeed experts with good intentions. This needs to be addressed.
But if you look at any of the current “moral panics” that are being used to suggest random suspicion-less drug testing of doctors or promoting the Physician Health Programs as successful and replicable models, you will inevitably find a doctor on this list behind it. It is a given.
And the invitation goes out to Seppala to debate this in a public forum on a level playing field. Not gonna happen because it would be impossible for him to address and answer the questions rationally, directly and with any tiny scrap of evidence based data.


Proof of Expertise or License to kill!
Disrupted Physician 101.3 –“For What it’s Worth”— The ASAM/ABAM Diploma Mill.
I can think of no other specialty or subspecialty in the profession of medicine where non-existent expertise can be incontestably announced and implemented. If I claimed to be an ace neurosurgeon or an expert otolaryngologist and started practicing my claimed skills in the hospital I would be called on it pretty quick by both colleagues and patients–deemed a delusional fraud and run out on a rail within a week.
Yet doctors who have not met the usual and customary standards of professional and educational quality and core competencies collectively and summarily identified for medical specialties and subspecialties by the American Board of Medical Specialties, American Council on Graduate Medical Education and Institute of Medicine are able to claim “expertise” in “addiction medicine” and everybody just lets them.

As an experiment to prove this hypothesis I sat for the 2010 American Board of Addiction Medicine (ABAM) Certification Exam.
I have absolutely no training or education in the field of addiction medicine. I didn’t pick up a book or study anything. I did not prepare at all. I went to the testing facility and finished the test within an hour and a half and below is my score. I passed it by a large margin with a score of 459 (passing score is > 394).

Aced it!
The validity and reliability of opinions lie in their underlying methodology and evidence base. Reliance on the personal authority of any expert or group of experts is the fallacy of appeal to authority.
I have asthma but that does not make me a Pulmonologist. That addiction “specialist” diagnosing and treating you may have 5 years prior been a proctologist; and maybe not even a very good one at that.
Somewhere there may be doctor with no post-graduate training in surgery wielding a scalpel and calling himself an expert surgeon, but it is difficult to imagine that he is a very good one.



“Spirituality can go hand-in-hand with ruthless single-mindedness when the individual is convinced his cause is just”
― Michela Wrong, In the Footsteps of Mr. Kurtz: Living on the Brink of Disaster in Mobutu’s Congo

Addiction Medicine is currently not recognized by the American Board of Medical Specialties (ABMS). It is still a a Self-Designated Practice Specialty and the American Board of Addiction Medicine is a Self-Designated Board. So too is the American Academy of Ringside Medicine and Surgery, the American Academy of Bloodless Medicine and Surgery and the Council of Non-Board Certified Physicians. But these Self-Designated Boards do not have the multi-billion dollar drug and alcohol testing and treatment industry supporting them. Addiction Medicine has deep pockets, and if the November 2014 issue of the Journal of the American Medical Association (JAMA) is a harbinger of what’s to come, this self-designated practice specialty currently being certified by a self-designated Board and bereft of anything resembling the educational and professional standards for quality practice in a particular medical specialty or subspecialty as defined by the ABMS, the American Council on Graduate Medical Education (ACGME) and the Institute of Medicine (IOM) may soon robber baron its way into acceptance by the Medical Profession.
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model. The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the drug and alcohol testing and 12-step treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.



“Conformity is the jailer of freedom and the enemy of growth.” – John F. Kennedy.
Born – May 29, 1917
Brookline, Massachusetts,
Died- November 22, 1963
Dallas, Texas, aged 46


“The hardest thing to explain is the glaringly evident which everybody has decided not to see”
― Ayn Rand, The Fountainhead

The Birth of Junk-Science in Drug and Alcohol Testing
The attached article concerns the reliability of hair-strand tests routinely accepted in child welfare cases in Ontario as evidence of parental drug or alcohol abuse. A positive test can lead to loss of parental custody of children.
The risk for false-positive results appears to be higher in women because of the higher use of alcohol-based hair products and the limitations of these tests are addressed in the article.
Almost 98% of ingested alcohol is eliminated through the liver in an oxidation process that involves its conversion to acetaldehyde and acetic acid, but the remaining 2% is eliminated through the urine, sweat, or breath.1
Ethyl Glucuronide (EtG) was introduced in 1999 as a biomarker for alcohol consumption,2 and was subsequently suggested as a tool to monitor health professionals by Dr. Gregory Skipper, M.D., because of its high sensitivity to ethanol ingestion.3

This minor metabolite of alcohol was reported by Skipper, M.D. and Friedrich Wurst, M.D., in November 2002 at an international meeting of the American Medical Society, to provide proof of alcohol consumption as much as 5 days after drinking an alcoholic beverage, well after the alcohol itself had been eliminated from the body.
In his study Dr. Skipper arbitrarily chose a value of 100 as a cut-off for EtG. The rationale behind this value is not cited.
In 2003, because of these and other reportedly remarkable results (e.g., positive findings, confirmed by admissions by the tested individuals, after traditional urine tests had registered negative), Skipper pitched the test to National Medical Services, Inc. (NMS labs) and it was developed as a Laboratory Developed Test (LDT).
So began EtG testing began in the United States, and this paved the way for the hair tests described. The urine EtG test introduced by Skipper is the index case and prototype for an array of unproven forensic tests introduced to the market as LDTs.

The LDT Pathway was not designed for Forensic Drug and Alcohol Testing. It is an Unregulated Industry.
The LDT pathway was developed for laboratory tests that would not otherwise come to market due to the prohibitive costs of FDA approval (for example a test for a rare disease).
Bringing an LDT to market does not require testing in humans (in vivo). Nor does it require that it be shown the test is testing for what it is purportedly testing for (validity). It is essentially an honor system. It was not designed for “forensic” testing but for simple testing with low risk.
None of this testing is approved by the FDA. It is essentially an unregulated industry.
NMS became a leading proponent of EtG testing and, starting in 2003, began publishing claims promoting the absolute validity and reliability of the EtG in detecting alcohol. Akin to the vitamin and supplement industry those promoting and selling the tests could say anything they want—and they did.
NMS initially established a reporting limit or cutoff of 250ng/ml at or over which EtG test results would be reported as “positive” for drinking alcohol. This was later upped to 500ng/ml, then 1000 ng/ml.
NMS reported it as the “Gold Standard” claiming any value above 250 ng/ml indicated “ethanol consumption.”
It was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8
As the cutoff value got higher they added another minor metabolite of alcohol, EtS, as a “confirmatory” LDT.
The authors of a 2011 study demonstrating that hand sanitizer alone could result in EtG and EtS concentrations of 1998 and 94 mug/g creatinine concluded that:
“in patients being monitored for ethanol use by urinary EtG concentrations, currently accepted EtG cutoffs do not distinguish between ethanol consumption and incidental exposures, particularly when uine specimens are obtained shortly after sustained use of ethanol containing hand sanitizer.”9
Sauerkraut and bananas have even recently been shown to cause positive EtG levels.10
![]()
A 2010 study found that consumption of baker’s yeast with sugar and water11 led to the formation of elevated EtG and EtS above the standard cutoff. EtG can originate from post-collection synthesis if bacteria is present in the urine.12 Collection and handling routines can result in false-positive samples.13
EtG varies among individuals.14 Factors that may underlie this variability include gender, age, ethnic group, and genetic polymorphisms.
“Exposure to ethanol-containing medications, of which there are many, is another potential source of “false” positives.15
Problems Exposed by Wall Street Journal and SAMHSA
On August 12, 2006, The Wall Street Journal published a front-page article, titled “A Test for Alcohol – And Its Flaws.”.16
Quoting Dr. Skipper, among others, the article includes:
“Little advertised, though, is that EtG can detect alcohol even in people who didn’t drink. Any trace of alcohol may register, even that ingested or inhaled through food, medicine, personal-care products or hand sanitizer.”
“The test ‘can’t distinguish between beer and Purell’ hand sanitizer, says H. Westley Clark, director of the Federal Substance Abuse and Mental Health Services Administration. . . ‘When you’re looking at loss of job, loss of child, loss of privileges, you want to make sure the test is right”, he says…”
“Use of this screen has gotten ahead of the science,’ says Gregory Skipper…”
Methinks Dr. Skipper might have realized this when he initially proposed it as an accurate test after a pilot study done on only a handful of subjects. Or perhaps when he used the LDT pathway to bypass FDA approval and oversight.
On September 28, 2006, SAMHSA, a federal agency that is part of the U.S. Department of Health and Human Resources, issued an Advisory, which on the first page contained a “grey box” warning, as follows:
 “Currently, the use of an EtG test in determining abstinence lacks sufficient proven specificity for use as primary or sole evidence that an individual prohibited from drinking, in a criminal justice or a regulatory compliance context, has truly been drinking. Legal or disciplinary action based solely on a positive EtG, or other test discussed in this Advisory is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”17
“Currently, the use of an EtG test in determining abstinence lacks sufficient proven specificity for use as primary or sole evidence that an individual prohibited from drinking, in a criminal justice or a regulatory compliance context, has truly been drinking. Legal or disciplinary action based solely on a positive EtG, or other test discussed in this Advisory is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”17
Bias has been identified as a large problem with drug trials.18 Industry-sponsored research is nearly four times as likely to be favorable to the company’s product as NIH-sponsored research.19 As an example, one survey of seventy articles about the safety of Norvasc (amlodipine) found that 96% of the authors who were supportive of the drugs had financial ties to the companies that made them.20
But what about the multi billion dollar drug-testing industry and the financial ties here?
Imagine if this was a drug and not a drug-test.
Essentially Greg Skipper and the FSPHP arm of ASAM launched a very lucrative joint business venture with a commercial drug-testing lab. They introduced the test via a loophole as a laboratory developed test. An LDT has no FDA regulation so the lab was able to promote, market and sell these tests with no meaningful oversight or accountability. Quest Diagnostics and USDTL are now working with the FSPHP and engaging in the same scheme.
The lab then contracted with state licensing boards and their state PHPs (who designed, implemented and managed drug and alcohol testing programs for nurses and doctors). A mutually beneficial scheme for the labs (who collect the samples) and the PHPs (who utilize, interpret and report the results.
The PHPs develop the arbitrary cutoff levels based on alleged “scientific” research and the labs promote whatever they say. “Gold-Standard,” “accurate” and “reliable.” 
EtG, EtS, Scram, PEth, Soberlink–all unsupported junk science introduced by prohibitionist profiteers without conscience.
How many lives were ruined by this test? How many careers were lost, families shattered and futures erased. I would venture to say a lot. Just look through all of the legal cases as I have. It is unconscionable. Sociopathic profiteering.
How many committed suicide feeling helpless, hopeless and entrapped?
At the end of a talk entitled Addicted Professionals: intervention, Evaluation and Treatment, Skipper presents a slide reading “Reporting or Assisting a Troubled Peer? These doctor’s can’t help themselves….” followed by graphic images of physician suicide. (see torrance_meeting_2 (4) ). It is for shock value and morbid humor and it is grotesque. He could not care less that these were human beings with wives, husbands, children and hopes and dreams.
How many scenes like this were repeated across the country because this guy gamed the system to get an ultra-sensitive test with abysmal specificity for a ubiquitous organic compound approved and marketed as a “forensic” test?
Forensic testing needs to be as close to 100% specific as possible because the results of a positive test can be grave and far reaching. Getting this test (and all the others) approved and marketed through a loophole and then getting the state Boards and Federation of State Medical Boards to approve them by moral entrepreneurship is unconscionable. Using the LDT pathway is just another example of how the “impaired physician movement” removes accountability and culpability by bending, ignoring or otherwise making their own rules.
And the labs have taken a “stand your ground” approach. Never admit wrongdoing. Never settle.
In a February 2007 article in the magazine “New Scientist,” Dr. Skipper is quoted
that:
“…there is not yet an agreed threshold concentration that can be used to separate people who have been drinking from those exposed to alcohol from other sources. Below 1000 nanograms of EtG per millilitre of urine is probably ‘innocent’, and above 5000 booze is almost certainly to blame. In between there is a “question zone…”![]()
No Dr. Skipper—it is you who is most certainly to blame. And what of all the people whose lives you ruined by introducing junk science with no evidence base via a regulatory loophole?? “probably innocent?” Shame on you Dr. Skipper…. Shame..shame..shame.

Physician Suicide 101: Secrets, Lies & Solutions by Dr. Pamela Wible, M.D., will hopefully serve as a stepping-stone to start discussing the elephant in the room; Physician Health Programs (PHPs) and their relationship to physician suicide.
The current state-of-affairs in these once benevolent programs that served a dual purpose of helping and protecting the public from “impaired” physicians is one of unrestrained managerial authority and absolute power with no meaningful oversight, regulation or accountability.
Moreover, the authority bestowed on this group is both illegitimate and irrational. The Federation of State Physician Health Programs is composed of American Society of Addiction Medicine “specialists” in “Addiction Medicine.”
The ASAM is not even recognized by the American Board of Medical Specialties as a bona fide specialty. It is a Self-Designated-Medical-Specialty; an AMA term used to keep track of what any group of doctors is calling themselves.
In fact, American Board of Addiction Medicine (ABMS) “board certification” is little more than a diploma mill.
Yet these “specialists” are now in charge of ALL things related to PHYSICIAN HEALTH.
Many of the physicians running these programs had their licenses revoked and got them back by claiming salvation through the good graces of Alcoholics Anonymous and other 12-step methodology. Many have felony convictions. Some have double felonies.
At best we have unqualified zealots. But one major problem I have heard over and over again from physicians forced into these programs is an absolute lack of justice, empathy and even civility by those in charge.
Misconduct, fraud, and even crimes are being reported.
Perhaps the 12-step salvation is just a ruse for some of them; a convenient cloak under which to hide all manner of abuse with impunity and immunity.
These individuals have been granted unrestrained managerial prerogative and absolute power over doctors. They decide not only who to monitor but how that monitoring proceeds in every last detail. Our fates, literally, lie in the hands of this group. No more physicians should die by this system of institutional injustice, bullying and pseudoscience. The conflicts-of-interest are abhorrent and would be incomprehensible in any other venue.
Isn’t it time we take charge? And the solution is fairly simple.
Oversight, regulation, and auditing by OUTSIDE groups. That is how it’s done everywhere else. Why do these guys get a pass? Why would anyone be against procedural fairness and transparency in any situation? These are legitimate questions.
State Medical Societies, Departments of Public Health, the American Medical Association, the American Council on Graduate Medical Education, the Institute of Medicine and other Accreditation and Professional Organizations need to start addressing this.
It is a public heal emergency that is not going away. It needs to be addressed directly and with urgency.
Accountability is without exception. Hopefully this article will succeed in framing certain questions for the medical profession; questions that we all need to think about now before the door closes for good.
Physician Suicide 101: Secrets, Lies & Solutions by Pamela Wible, M.D.


 Educational and Professional Standards in Medical Specialties and Subspecialties
Educational and Professional Standards in Medical Specialties and SubspecialtiesThe increasingly rapid growth and complexity of medical knowledge in twentieth century American medicine resulted in the creation of specialties and subspecialties.
A related development was the creation of “boards” to “certify” physicians as knowledgeable and competent in the specialties and subspecialties in which they claimed to have expertise. The American Board of Ophthalmology, organized in 1917, was the first of these.
As the number of medical specialties proliferated an umbrella organization was formed to accomplish this task. The Advisory Board for Medical Specialties was created in 1933 and reorganized as the American Board of Medical Specialties (ABMS) in 1970. This non-profit organization oversees board certification of all physician specialists and sub-specialists in the United States.
The ABMS recognizes 24 medical specialties in which physicians can pursue additional training and education to pursue Board Certification.
In 1991 the American Board of Medical Genetics was approved as the 24th ABMS board and these 24 boards grant the 37 general certificates and 88 subspecialty certificates available to medical specialists today.
The ABMS Member Boards are responsible for developing and implementing the educational and professional standards for quality practice in a particular medical specialty or subspecialty and evaluate physician candidates for Board Certification. They set the bar of knowledge and competence for their given area of expertise.
All of the ABMS Member Boards are:
“committed to the principle of examining doctors based on six general competencies designed to encompass quality care: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice.”These areas have been collectively identified by the ABMS, the American College of Graduate Medical Education (ACGME) and the Institute of Medicine (IOM) in order to standardize graduate medical education in any specialty from medical school graduation through retirement.1
One of the 24 medical specialties ABMS recognizes in which physicians can pursue additional training and education and pursue Board Certification is Psychiatry.
Founded in 1934, The American Board of Psychiatry and Neurology (ABPN) is one of the 24 ABMS specialty boards. In 1959, the ABPN issued its first subspecialty certificate in Child and Adolescent Psychiatry and was the only ABNP subspecialty until 1991 when the first examination in Geriatric Psychiatry was administered.4 Addiction Psychiatry became a subspecialty of ABPN in 1993.
The ABPN governs the specialty of Psychiatry, of which Addiction Psychiatry is a subspecialty. Board Certification in Addiction Psychiatry requires a four-year psychiatric-residency program for training in the prevention, diagnosis and treatment of mood, anxiety, substance-abuse as well as other psychological and interpersonal problems followed by an additional year of training in one of the 40 accredited Addiction Psychiatry Fellowship programs. The Accreditation Council for Graduate Medical Education (ACGME) is the professional organization responsible for the accreditation residency education programs in the US for ABMS specialty and subspecialty areas of medicine. Addiction Psychiatry training programs are governed by the ACGME and graduates are eligible for ABPN Certification in Addiction Psychiatry.
When this rigorous education and training is complete a candidate is Board Eligible and can then take the subspecialty certification exam. The exam assesses competency in the dand consultation, pharmacotherapy, pharmacology of drugs, psychosocial treatment and behavioral basis of practice to be Board Certified in the subspecialty of Addiction Psychiatry by the ABPN.
Candidates must then be assessed in a number of areas including psychiatric evaluation and consultation, pharmacotherapy, pharmacology, toxicology, psychosocial treatment, behavioral basis of practice, and many other areas in which for the past half-decade they where taught and apprenticed.
The current structure of residency training is little changed from when it was conceived originally by William Stewart Halsted in the late 19th Century. Physicians acquire knowledge and skills necessary to safely and competently manage patients through apprenticeship. Training in a specialty area provides a comprehensive platform that allows medical school graduates to apply a body of knowledge to patient care and the treatment of disease. This forms the foundation of our Guild–undifferentiated and general but pluripotential.
The American Academy of Addiction Psychiatry (AAAP) is the only professional organization in the US focused on the subspecialty of Addiction Psychiatry. The AAAP Mission Statements are to: 2
 The American Medical Association records a physician’s Self-Designated Practice Specialty (SDPS) in response to an annual credentialing survey. According to the AMA, SDPS are “historically related to the record-keeping needs of the American Medical Association and do not imply ‘recognition’ or ‘endorsement’ of any field of medical practice by the Association. SDPS refers to a self-designated specialty and this is not equivalent nor does it imply ABMS [American Board of Medical Specialties] Board Certification.
The American Medical Association records a physician’s Self-Designated Practice Specialty (SDPS) in response to an annual credentialing survey. According to the AMA, SDPS are “historically related to the record-keeping needs of the American Medical Association and do not imply ‘recognition’ or ‘endorsement’ of any field of medical practice by the Association. SDPS refers to a self-designated specialty and this is not equivalent nor does it imply ABMS [American Board of Medical Specialties] Board Certification.
“The fact that a physician chooses to designate a given specialty/area of practice on our records does not necessarily mean that the physician has been trained or has special competence to practice the SDPS.”3
Physicians have been able to list addiction medicine as a self-designated area of practice using the specialty code “ADM” since 1990.
In contrast to these accepted board credentials, American Board of Addiction Medicine (ABAM) certification requires only a medical degree, a valid license to practice medicine, completion of a residency training in ANY specialty, and one year‘s full time involvement plus 50 additional hours of medical education in the field of alcoholism and other drug dependencies. The majority of American Society of Addiction Medicine (ASAM) physicians meet these requirements by “working in a chemical dependency treatment facility, taking continuing medical education courses in addiction, or participating in research.”6
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments,, physicians, purchasers, and consumers of health care products, and the general public.’5 They have succeeded in doing this as many consider them to be the experts in addiction medicine including regulatory agencies.
addiction medicine as a specialty recognized by professional organizations, governments,, physicians, purchasers, and consumers of health care products, and the general public.’5 They have succeeded in doing this as many consider them to be the experts in addiction medicine including regulatory agencies.
The goal of the American Board of Addiction Medicine (ABAM) Foundation is to “gain recognition of Addiction Medicine as a medical specialty by the American Board of Medical Specialties (ABMS).”
But Addiction Medicine is currently not recognized by the ABMS. It is still a a Self-Designated Practice Specialty and the ABAM is a Self-Designated Board. So too is the American Academy of Ringside Medicine and Surgery, the American Academy of Bloodless Medicine and Surgery and the Council of Non-Board Certified Physicians. But these Self-Designated Boards do not have the multi-billion dollar drug and alcohol testing and treatment industry supporting them. Addiction Medicine has deep pockets, and if the November 2014 issue of the Journal of the American Medical Association (JAMA) is a harbinger of what’s to come, this self-designated practice specialty currently being certified by a self-designated Board and bereft of anything resembling the the educational and professional standards for quality practice in a particular medical specialty or subspecialty may soon robber baron its way into acceptance by the American Board of Medical Specialties.
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model. The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the drug and alcohol testing and 12-step treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.








{kind=link}