 Link to Medscape article by Pauline Anderson Here:
Link to Medscape article by Pauline Anderson Here:
Link to illegible, post-dated and undated documents submitted as evidence and mentioned in article can be seen here> board-records-obtained-june-2016
Link to document written June 6, 2013 but date-stamped as being received in 2012 ( both by hand and apparently by the Board’s Document Imaging Unit (DIU) > Back to the Future: Massachusetts Board of Registration in Medicine


Michael Langan, MD, a Boston-based internal medicine specialist who has fought the Massachusetts Physician Health Service (PHS) and Board of Registration in Medicine for years to reinstate his license, has suffered a setback but is bolstered by a new development.
A justice of the Supreme Judicial Court of Massachusetts has denied Dr Langan’s petition to invalidate the 2013 suspension of his medical license for not meeting conditions to have his license reinstated.
However, a new law has enabled Dr Langan to access his records. According to Dr Langan, these documents show that the court did not consider key evidence in his case, as demonstrated by the fact that his hearing occurred after the date of receipt that is stamped on the documents. This may offer an opportunity to reopen his case.
The court decision, which was handed down in December by Associate Justice Geraldine Hines, states that although Dr Langan completed required psychiatric evaluations, he “did not submit a suitable worksite or substance abuse monitoring plan. In combination with his violation of the LoA [Letter of Agreement] meeting requirement, the board’s decision to affirm its prior suspension of petitioner’s license to practice medicine is supported by the record. The board’s decision to deny reinstatement in the absence of an acceptable plan is affirmed.”
“It’s unbelievable; everyone is dumbfounded,” said Dr Langan of the decision.
Dr Langan is appealing the denial of his petition, a process that will take an estimated 6 months.
He maintains that the PHS committed “forensic fraud” and concealed doing so.
“If I couldn’t win with all the direct evidence of felony crimes that you don’t need to be a lawyer to recognize, then I don’t think anyone can,” he told Medscape Medical News.
The PHS is a confidential resource for physicians and medical students seeking help for a variety of physical and behavioral health concerns, which may include difficulties with substance use.
In 2007, Dr Langan was at Massachusetts General Hospital (MGH) and Harvard University when he approached the PHS to help him with his dependence on Vicodin, an opioid analgesic.
He became dependent on Vicodin after a bout of chickenpox during residency, when he developed shingles. He stressed that there were no work-related problems associated with use of this drug.
He was an inpatient at the Talbott Recovery Center in Georgia for more than 3 months, after which he signed the requisite 5-year contract with the PHS that included regular drug testing.
According to Dr Langan, there were no problems until mid-2011, when a report from the US Drug Testing Laboratories found he was positive for phosphatidylethanol (PEth), a blood marker for chronic alcohol use.
The level detected was 365.4 ng/mL, which “is the equivalent of drinking a half gallon of whisky a day,” or a sign of end-stage alcoholism, said Dr Langan, who insists he has never had an alcohol problem.
“That the test was invalid at this point should have been self-evident,” said Dr Langan.
Lab Fraud?
Suspecting that there had been “lab fraud” and that he would “end up being admitted for 3 months,” Dr Langan said he requested, but was denied, an independent evaluation outside the 12-step PHP-approved list of facilities. Because his request was denied, he attended one of the approved facilities, Hazelden Addiction Treatment Center, in Minnesota, where he “was cleared.”
“They noted no past or present history of alcohol use or abuse and sent me back after a 4-day evaluation,” he said.
An independent investigation by James G. Flood, PhD, who has been chief of toxicology at MGH for nearly 30 years, concluded in a November 5, 2012, letter to Dr Langan’s lawyer “that there is a purposeful and intentional act by PHS” to show Dr Langan’s test as valid “when in reality this test was invalid and involved both fatal laboratory errors” and inadequate review of the results.
Any confirmatory, positive finding based on the July 2011 test “should be reversed, rectified and remediated,” Dr Flood writes.
Among the “many errors in sample collection, processing and transportation,” said Dr Flood, was that the documentation that was received with the specimen did not have a date and time of specimen collection. Moreover, the person who collected the specimen was not properly identified, the signature of the sample donor was missing, and there was no tamper-proof seal affixed to the specimen.
Dr Flood claims the sample was directed to the wrong laboratory, where it sat for several days. The storage conditions of the sample while at that laboratory were not documented.
Following an investigation by the College of American Pathologists, in October 2012, Dr Langan’s laboratory test result was corrected from having a positive result to being an invalid test, but he said he did not learn of this change until months later.
In a letter to the Massachusetts Board of Registration in Medicine, Luis T. Sanchez, MD, who at the time was the director of the Massachusetts PHS, said the amended report indicates that the “external chain of custody protocol [for that sample] was not followed per standard protocol.”
Dr Sanchez noted that, on the basis of the revised report, “PHS will continue to disregard the July 2011 PEth test result.”
Dr Langan requested the record of the chain of custody pertaining to his testing. This document showed that the test was “not only invalid but falsely created,” said Dr Langan. He added that it included a fax from the PHS requesting that his identification number be added to an already positive test and that the chain of custody be updated.
“You can’t update a chain of custody, as it is generated in real time,” said Dr Langan. “This is forensic fraud. It clearly shows collusion between the PHS and the lab.”
In an October 2012 letter, Dr Sanchez alleged that Dr Langan did not attend required peer support group meetings, but according to Dr Langan, this claim is “without fact or support.” Dr Langan maintains that he attended all required meetings. He also maintains that the PHS actions were in “retaliation” for requesting the chain of custody record.
Massachusetts PHS Director Dr Sanchez did not respond to a request from Medscape Medical News for clarification.
Medscape Medical News also sought comment on recent developments in Dr Langan’s case from the Massachusetts Attorney General’s Office, which declined to comment.
“The AG’s [Attorney General’s] Office often defends state agencies in litigation and we typically do not comment on behalf of our clients, who in this case is the Board of Registration in Medicine,” Emily Snyder, deputy press secretary, Office of Massachusetts Attorney General, told Medscape Medical News in an email.
Intentional Delay?
Dr Langan alleges that the PHS “intentionally delayed” his efforts to undergo a psychiatric evaluation that was necessary to have his license reinstated. He said the PHS insisted he get this evaluation out of state, even though he suggested three Boston-area board-certified experts.
The Board of Registration in Medicine eventually approved an evaluation by Patricia Recupero, MD, from the Law and Behavioral Health Program at the University of Rhode Island.
Dr Recupero’s November 2013 report determined that Dr Langan “is safe to return to the practice of medicine without further supervision,” that he “has an excellent prognosis and a very low risk of relapse,” and he “has not had an alcohol use, abuse or dependence problem.”
Many of the conflicts between the PHS and Dr Langan revolve around positive test findings, Dr Recupero notes in her letter.
It is “critical to understand” the inadequacies of such tests for physician monitoring for purposes of relapse, she notes. She added that the source of the alcohol in Dr Langan’s test results cannot be determined and that many products – mouthwash and hand sanitizers among them – can create a false-positive test.
Dr Langan acknowledges he used hand sanitizers in the course of his work as a physician. Owing to severe allergies, he also uses prescribed asthma inhalers, which contain alcohol as a propellant.
Dr Recupero also notes that “almost without exception,” Dr Langan’s test findings have been below the minimum level to declare a test positive and that positive findings “are not a sign of relapse.”
It was her opinion that, should he require additional treatment and supervision, the PHS should not be involved. A spokesperson for the PHS confirmed that it has not been involved in matters related to Dr Langan for at least 3 years.
Dr Langan said that since it suspended his medical license, the board has “engaged in a persistent pattern of ignoring my every reasonable effort at trying to be reinstated” and has “abused the administrative law process to accomplish this.”
Medscape Medical News contacted the Massachusetts medical board as well as its counsel, Deb Stoller, but received no response.
“Close to Homeless”
A memorandum to the Supreme Judicial Court, filed May 13, 2016, proposed a settlement between Dr Langan and the board. In return for the immediate reinstatement of Dr Langan’s license, he would be monitored for a maximum of 3 months by Dr Recupero and Timothy E. Wilens, MD, codirector of the Center for Addiction Medicine at MGH.
That memorandum was accompanied by letters from Dr Recupero and Dr Wilens agreeing to the terms, but according to Dr Langan, it has been “ignored.”
“The board did not acknowledge or address the proposals in any way,” said Dr Langan.
Dr Langan maintains that he “never ever” had any patient care or malpractice problems during his 15 years at MGH. In fact, his supervisors and colleagues reported that his work performance has been “superlative” on all counts, he said.
Many in the addiction medicine and psychiatric community support Dr Langan. He has letters from high-profile physicians in the field who verify that he is safe to practice medicine.
A first petition was filed in the Supreme Court on October 22, 2014, but the judge dismissed it because it had not been filed within the required 60-day period. Dr Langan’s most recent petition was filed July 3, 2015.
The past few years, he said, have taken a toll on his family. They have lost their home and health insurance because of his inability to practice his profession.
Disheartened by this latest setback, Dr Langan is looking into the possibility of becoming licensed in another state and leaving Massachusetts.
But Dr Langan has renewed hope. Under Massachusetts’ new Public Records Reform Law, which went into effect January 1, 2017, “the board was forced to comply with my request for records within 10 days,” and has done so, he said.
According to Dr Langan, these records show some irregularities that may bolster his case.
“A letter dated December 15, 2011, introducing exculpatory evidence was date-stamped January 17, 2012, almost 1 month after the hearing where it was submitted as evidence. All of the other documents had either illegible or absent date-stamps,” he said.





































 Examining the specific practice and policy pushed reveals a body of false-claims making designed to facilitate the systemic use of coercion and threats, remove all due process protections and fundamental rights from physicians and prevent, block and eliminate the evidence. This
Examining the specific practice and policy pushed reveals a body of false-claims making designed to facilitate the systemic use of coercion and threats, remove all due process protections and fundamental rights from physicians and prevent, block and eliminate the evidence. This 

 The
The  The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.  “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.” Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal. Research on street criminals suggests the certainty of punishment has the strongest deterrent effect (basically will I be caught) and the more people think they will be arrested for a crime the less likely they are to commit it. Criminals weigh their actions against possible gains and consequences and the risk of consequences in this system have been essentially zero. Diagnosis rigging, coercion, threats and abuse are rampant because they have no fear of punishment. The Chairman of the commission that examined the causes of the 2008 financial collapse compared the
Research on street criminals suggests the certainty of punishment has the strongest deterrent effect (basically will I be caught) and the more people think they will be arrested for a crime the less likely they are to commit it. Criminals weigh their actions against possible gains and consequences and the risk of consequences in this system have been essentially zero. Diagnosis rigging, coercion, threats and abuse are rampant because they have no fear of punishment. The Chairman of the commission that examined the causes of the 2008 financial collapse compared the 





 What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (
What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones ( 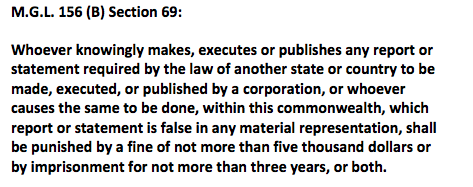 It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.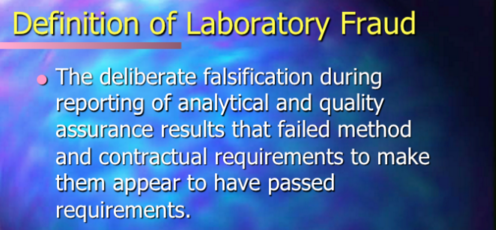 Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
 board’s position on the fraudulent practice of medicine is quite clear.
board’s position on the fraudulent practice of medicine is quite clear.
































































 diagnosis. Pervasive problems include:
diagnosis. Pervasive problems include:
 The primary architects of this system can be found on a list of Fellows of the American Society of Addiction Medicine. The list can be seen
The primary architects of this system can be found on a list of Fellows of the American Society of Addiction Medicine. The list can be seen 





