Physician Suicide and Organizational Justice: The Role of Hopelessness, Helplessness and Defeat
Michael Langan, M.D.
They can be a terror to your mind and show you how to hold your tongue They got mystery written all over their forehead They kill babies in the crib and say only the good die young They don’t believe in mercy Judgement on them is something that you’ll never see They can exalt you up or bring you down main route Turn you into anything that they want you to be–Bob Dylan, Foot of Pride
In F. Scott Fitzgerald’s The Great Gatsby, Nick Carraway observes that “the loneliest moment in someone’s life is when they are watching their whole world fall apart, and all they can do is stare blankly” In 1896 Émile Durkheimdescribed “melancholy suicide” as being “connected with a general state of extreme depression and exaggerated sadness, causing the patient no longer to realize sanely the bonds which connect him with people and things about him. Pleasures no longer attract.” Heightened perceptions of defeat and entrapment are known to be powerful predictors of suicide. According to the “Cry of Pain” model people are particularly prone to suicide when life experiences are interpreted as signaling defeat, defined as a sense of a “failed struggle.” Unable to find some sort of resolution to a defeating situation, a sense of entrapment proliferates and the perception of no way out provides the central impetus for ending one’s life.
Although no reliable statistics yet exist, anecdotal reports suggest a marked rise in physician suicide in recent years. From the reports I am receiving it is a lot more than the oft cited “medical school class” of 400 per year.
This necessitates an evaluation of predisposing risk factors such as substance abuse and depression, but also requires a critical examination of what external forces may be involved. What acute and cumulative situational and psychosocial factors are involved in the descent from suicidal ideation to planning to completion? What makes suicide a potential option for doctors and what acute events precipitate and trigger the final act?
Depression and Substance Abuse no Different from General Population
The prevalence of depression in physicians is close to that of the general population1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria indicate that physicians have the same rates (8-14%) of substance abuse and dependence as the general population,3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 reported a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
Job Stress and Untreated Mental Illness Risk Factors
Job stress coupled with inadequate treatment for mental illness may be factors contributing to physician suicide according to one recent study. Using data from the National Violent Death Reporting System, Gold, Sen, & Schwenk, 2013 8 compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians. They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”8
Few studies have evaluated the psychosocial stressors surrounding physician suicide but there is no reason to believe they are any different from the rest of the population. Although the triggering life events and specific stressors may vary outside, the inner psyche and undercurrent of thoughts and feelings should remains the same. Perhaps the same drivers of suicide identified in other populations are contributing to physician suicide.
Experts discuss the coverup of doctor suicides, the reasons behind depression in doctors, and why doctors who are depressed are less likely than normal to get help.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to doctors and how they might be involved in the descent from suicidal ideation to suicidal planning to completed suicide.
Depression and Substance Abuse Comparable to General Population
Depression and substance abuse are the two biggest risk factors for suicide. The prevalence of depression in physicians is close to that of the general population1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria suggest that physicians have the same rates (8-14%) of substance abuse and dependence as the rest of the population 3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 found a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
State Physician Health Programs
Perhaps it is how physicians are treated differently when they develop a substance abuse or mental health problem.
Physician Health Programs (PHP) may be considered the equivalent to Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Originally developed as “impaired physician” programs, the PHPs were created to help doctors who developed problems with substance abuse or addiction as an alternative to disciplinary action by State Medical Boards. These programs existed in almost every state by 1980. Often staffed by volunteer physicians and funded by State Medical Societies, “impaired physician” programs served the dual purpose of both helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation (so long as the public was protected from imminent danger) most medical boards accepted the concept with support and referral. However, most EAPs were developed with the collaboration of workers unions or some other group supporting the rights and interests of the workers. Not so with PHPs as there is no such organization representing doctors. PHPs developed in the absence of regulation or oversight. As a consequence there is no meaningful accountability.
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”8
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “that the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 8 They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”8 Unfortunately this has not happened. Most physicians have no idea that the state physician health programs have been taken over by the “impaired physicians movement.”
In his Psychology Todayblog, Boyd again recommends oversight and regulation of PHPs. He cites the North Carolina Physicians Health Program Audit released in April of 2014 that reported the below key findings:
As with Knight and Boyd’s paper outlining the ethical and managerial problems in PHPs, the NC PHP audit finding that abuse could occur and not be detected generated little interest from either the medical community or the media.
Although state PHPs present themselves as confidential caring programs of benevolence they are essentially monitoring programs for physicians who can be referred to them for issues such as being behind on chart notes. If the PHP feels a doctor is in need of PHP “services” they must then abide by any and all demands of the PHP or be reported to their medical board under threat of loss of licensure.
LDTs bypass the FDA approval process and have no meaningful regulatory oversight. The LDT pathway was not designed for “forensic” tests but clinical tests with low risk. Some are arguing for regulation and oversight of LDTs due to questionable validity and risk of patient harm.13
These same physicians are claiming a high success rate for PH programs9 and suggesting that they be used for random testing of all physicians.14
As with LDTs, the state PHPs are unregulated, and without oversight. State medical societies and departments of health have no control over state PHPs.
Their opacity is bolstered by peer-review immunity, HIPPA, HCQIA, and confidentiality agreements. The monitored physician is forced to abide by any and all demands of the PHP no matter how unreasonable-all under the coloration of medical utility and without any evidentiary standard or right to appeal.
The ASAM has a certification process for physicians and claim to be “addiction” specialists. This“board certification” is not recognized by the American Board of Medical Specialties and is not a recognized medical specialty. The goal of the ASAM is to be recognized as the experts in addiction medicine with the consensus expert opinion based on the 12-step prohibitionist brain disease model. The ASAM has aligned itself with a number of inpatient drug treatment centers (Hazelden, Talbott, Marworth, Bradford,etc) and are heavily funded by the drug testing industry. It is in fact a “rigged game.”
State PHPs are non-profit non-governmental organizations and have been granted quasi-governmental immunity by most State legislatures from legal liability.
By infiltrating “impaired physician” programs they have established themselves in almost every state by joining, gaining power, and removing dissenters. Groupthink and 12-step indoctrination are the goals. By advertising as advocates for doctors who are “caring,” “confidential resources,” “giving help,” and advocating for “colleagues in need” the outward appearance is one of benevolence.
The biggest obstacle is that this system allows them to throw the normal rules of conduct under the imperative of a higher goal assumed to trump all other consideration. Those outside of programs either defend or ignore the reports of ethical and criminal violations, complacent in their trust of these “experts” claiming they are just helping sick doctors and protecting the public.
With no oversight or regulatory body involved this is all done with impunity, immunity, and undercover. They use the accusation of substance abuse as an indication to disregard the claims of the accused. The physician is left without rights, depersonalized, and dehumanized. The imposition of confinement, stigmatization, lack of oversight of the organizations, peer-review protected confidentiality, and lack of procedural protection is a one-way train to hopelessness and despair.
By establishing a system that of coercion, control, secrecy, and misinformation, the FSPHP is claiming an “80% success rate” 15and deeming the “PHP-blueprint” as “the new paradigm in addiction medicine treatment.
The ASAM/FSPHP had a major influence on the DSM-V where drug abuse and dependence are no longer separate entities. They are also working behind the scenes to get legislation to randomly drug test all physicians.
They are now after the “disruptive physician” and the evidentiary criteria are fairly low and red flags include “deviating from workplace norm in dress or conduct” and being tardy for meetings.
They have identified “the aging physician” as a potential problem because “as the population of physicians ages,””cognitive functioning” becomes “a more common threat to the quality of medical care.”
The majority of physicians are unaware that the Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment in 2011 that uses addiction as an example of a “potentially impairing illness.” According to the Federation of State Physician Health Programs …”physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years. This is a critically important distinction. Illness is the existence of a disease. Impairment is a functional classification and implies the inability of the person affected by disease to perform specific activities.”
“Process addiction” was added as a potentially impairing illness including compulsive gambling, compulsive spending, compulsive video gaming, and “workaholism.” According to the FSPHP “the presence of a process addiction can be problematic or even impairing in itself, and it can contribute to relapse of a physician in recovery. As such, process addictions should be identified and treated.” They define three levels of relapse including the novel “relapse without use.”
Bullying, Helplessness, Hopelessness and Despair
Perceived helplessness is significantly associated with suicide.16 So too is hopelessness, and the feeling that no matter what you do there is simply no way out17,18 Bullying is known to be a predominant trigger for adolescent suicide19-21 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.22
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.23,24 The “Cry of Pain” model 25,26 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life.
There is also evidence that rescue factors such as social supports may play a role in preventing suicide. These rescue factors act buffers to protect against suicide in the face of varying degrees of life stress.27,28 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 29 and support at work when difficulties arose appeared to be a protective factor for the male physicians.30 Research involving Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.31,32 Organizational justice is related to fairness and refers to an individuals perception of an organizations behaviors, decisions, and actions and how these influence one’s own attitudes and behaviors and has been identified as a psychosocial predictor of health and wellbeing3334Low organizational justice has been identified as a notable risk factor for psychological distress and depression.35,36
A recent report indicates that job stress, coupled with inadequate treatment for mental illness may play a role in physician suicide..
Using data from the National Violent Death Reporting System the investigators compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.1
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians.
They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity.
We have heard of numerous suicides due to these institutionally unjust programs. Three doctors died by suicide in Oklahoma in a one month period alone (August 2014). All three were being monitored by the Oklahoma PHP. I went to an all boys high-school of less than 350 students yet a classmate a couple years ahead of me died by suicide a few months ago. He was being monitored by the Washington PHP. His crime? A DUI in 2009–a one-off situational mistake that in all likelihood would never have recurred. But as is often the case with those ensnared by state PHPs he was forced to have a “re-assessment” as his five-year monitoring contract was coming to an end. These re-assessments are often precipitated by a positive Laboratory Developed Test (LDT) and state medical boards mandate these assessments can only be done at an out-of-state “PHP-approved” facility. Told he could no longer operate and was unsafe to practice medicine by the PHP and assessment center he then hanged himself. And at the conclusion of Dr. Pamela Wible’s haunting video below are listed just the known suicides of doctors; many were being monitored by their state PHPs–including the first name on the list– Dr. Gregory Miday.
None of these deaths were investigated. None were covered in the mainstream media. These are red flags that need to be acknowledged and addressed! This anecdotal evidence suggests the oft-used estimate of 400 suicides per year (an entire medical school class) is a vast underestimation of reality—extrapolating just the five deaths above to the entire population of US doctors suggests we are losing at least an entire medical school per year.
As physicians we need to demand transparency, oversight, regulation and auditing by outside groups. This is a public health emergency.
To wit:
They first came after the substance abusers and I did not speak out because I was not a substance abuser.
They then came for those with psychiatric diagnoses and I did not speak out because I was not diagnosed with a psychiatric disorder.
They then came after the “disruptive physician” and I did not speak out because I was not disruptive.
They then came after the aging physician and I did not speak out because I was young.
They then came after me and there was no one else to speak out for me.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res.1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication.Archives of general psychiatry.Jun 2005;62(6):593-602.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ Health Programs. Journal of Medical Regulation. Mar 2010;95(4):10-25.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol and alcoholism.Sep-Oct 2004;39(5):445-449.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results.Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study.European addiction research.2014;20(3):137-142.
Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
Pham JC, Pronovost PJ, Skipper GE. Identification of physician impairment.JAMA : the journal of the American Medical Association. May 22 2013;309(20):2101-2102.
McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. Bmj. 2008;337:a2038.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school.The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody.Crisis.2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors.Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample.Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
They can be a terror to your mind and show you how to hold your tongue
They got mystery written all over their forehead
They kill babies in the crib and say only the good die young
They don’t believe in mercy
Judgement on them is something that you’ll never see
They can exalt you up or bring you down main route
Turn you into anything that they want you to be–Bob Dylan, Foot of Pride
Although no reliable statistics yet exist, anecdotal reports suggest a marked rise in physician suicide in recent years. From the reports I am receiving it is a lot more than the oft cited “medical school class” of 400 per year.
This necessitates an evaluation of predisposing risk factors such as substance abuse and depression, but also requires a critical examination of what external forces may be involved in the descent from suicidal ideation to suicidal planning to completed suicide. What are the cumulative situational and psychosocial factors in physicians that make suicide a potential option and what acute events precipitate the final act?
Depression and Substance Abuse no Different from General Population
The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria indicate that physicians have the same rates (8-14%) of substance abuse and dependence as the general population,3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 reported a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
Job Stress and Untreated Mental Illness Risk Factors
Job stress coupled with inadequate treatment for mental illness may be factors contributing to physician suicide according to one recent study. Using data from the National Violent Death Reporting System, Gold, Sen, & Schwenk, 2013 8 compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician. Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians. They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”8
Few studies have evaluated the psychosocial stressors surrounding physician suicide but there is no reason to believe they are any different from the rest of the population. Although the triggering life events and specific stressors may vary outside, the inner psyche and undercurrent of thoughts and feelings should remains the same. Perhaps the same drivers of suicide identified in other populations are contributing to physician suicide.
Perceived Helplessness, Hopelessness, Bullying and Defeat
Perceived helplessness is significantly associated with suicide as is9 Hopelessness10,11 Bullying is known to be a predominant trigger for adolescent suicide12-14 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.15
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.16,17 The “Cry of Pain” model 18,19 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life. There is a helplessness and hopelessness that precipitates the descent from ideation, to planning, and then to finality.
Organizational Justice Important Protective Factor
In a study on Italian and Swedish female physicians, degrading experiences and harassment at work were found to be the most powerful independent variables contributing to suicidal thoughts.20 Degrading work experiences harassment, and lack of control over working conditions were found to be associated with suicidal thoughts among Italian and Swedish male university physicians.21
Evidence exists for the role of rescue factors (i.e. social support) as buffers against suicide in the face of varying degrees of life stress.22,23 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 20 and support at work when difficulties arose appeared to be a protective factor for the male physicians.21 In line with this, studies of Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.24,25 Organizational justice has been identified as a psychosocial predictor of health and wellbeing2627 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.28,29
Historical Precedent-the Suicides at Ridgeview
Could these factors be playing a role in physician suicide? They evidently did at the Ridgeview Institute, a drug and alcohol treatment program for impaired physicians in Metropolitan Atlanta created by G. Douglas Talbott. Talbott helped organize and served as past president of the American Society of Addiction Medicine (ASAM) and was a formative figure in the American Medical Association’s (AMA’s) Impaired Physician Program. He has owned and directed a number of treatment facilities for impaired professionals, most recently the Talbott Recovery Campus in Atlanta, one of the preferred referrals for physicians ordered into evaluation and treatment by licensing boards.
After creating the DeKalb County Impaired Physicians Committee for the Medical Association of Georgia, Talbott founded the Georgia Disabled Doctors Program in 1975 in part because “traditional one-month treatment programs are inadequate for disabled doctors.” According to Talbott, rehabilitation programs that evaluate and treat the rest of the population for substance abuse issues are incapable of doing so in doctors as they are unlike others. He bases this uniqueness on “incredibly high denial”, and what he calls the “four MDs,” “M-Deity”, “Massive Denial” “Militant Defensiveness”, and “More Drugs.”30
Contingency Management = Extortion Using Medical License
According to Talbott, “impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.” “Terminal uniqueness “ is a phrase Talbott uses to describe doctors’ tendency to think they can heal themselves. “M-Deity” refers to doctors “being trained to think they’re God,”31 an unfounded generalization considering the vast diversity of individuals that make up our profession. This attitude, according to some critics, stems from the personal histories of the treatment staff, including Talbott, who are recovering alcoholics and addicts themselves. One such critic was Assistant Surgeon General under C. Everett Koop John C. Duffy who said that Ridgeview suffered from a “boot-camp mentality” toward physicians under their care and “assume every physician suffering from substance abuse is the same lying, stealing, cheating, manipulating individual they were when they had the illness. Certainly some physicians are manipulative, but it’s naïve to label all physicians with these problems.”32
American Society of Addiction Medicine (ASAM) President (1981-1983) LeClair Bissell was also highly critical of Talbott’s approach. Bissell, co-author of the first textbook of ethics for addiction professionals33 when asked if there was any justification to the claim that doctors are sicker than other people and more vulnerable to addiction replied:
“Well, based on my treatment experience, I think they are less sick and much easier to treat than many other groups. I think one reason for that is that in order to become a physician…one has to have jumped over a great many hurdles. One must pass the exams, survive the screening tests and the interviews, be able to organize oneself well enough to do examinations and so on, and be observed by a good many colleagues along the way. Therefore I think the more grossly psychotic, or sicker, are frequently screened out along the way. The ones we get in treatment are usually people who are less brain-damaged, are still quite capable of learning, are reasonably bright. Not only that, but they are quite well motivated in most cases to hang on to their licenses, the threat of the loss of which is frequently what puts them in treatment in the first place. So are they hard to treat? No! Are they easy patients? Yes! Are they more likely to be addicted than other groups? We don’t know.”34
“I’m not much for the bullying that goes along with some of these programs,” Bissell commented to the Atlanta Journal and Constitution in 1987.31 The constitution did a series of reports after five inpatients committed suicide during a four-year period at Ridgeview.35 In addition there were at least 20 more who had killed themselves over the preceding 12 years after leaving the treatment center.32
Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.”31According to Bissell: “There’s a lot of debate in the field over whether treatment imposed by threats is worthwhile…To a large degree a person has to seek the treatment on his own accord before it will work for him.”31
A jury awarded $1.3 million to the widow of one of the deceased physicians against Ridgeview,36 and other lawsuits initiated on behalf of suicides were settled out of court.35
The Constitution reported that doctors entered the program under threats of loss of licensure “even when they would prefer treatment that is cheaper and closer to home.” 37 The paper also noted that Ridgeview “enjoys unparalleled connections with many local and state medical societies that work with troubled doctors,” “licensing boards often seek recommendations from such groups in devising an approved treatment plan,” and those in charge are often “physicians who themselves have successfully completed Ridgeview’s program.”37
The cost of a 28-day program for nonprofessionals at Ridgeview in 1987 was $10,000 while the cost was “higher for those going through impaired-health professionals program,” which lasted months rather than 28 days.32
In 1997 William L. White interviewed Bissell whom he called “one of the pioneers in the treatment of impaired professionals.” The interview was not published until after hear death in 2008 per her request. Noting her book Alcoholism in the Professions38“remains one of the classics in the field”, White asked her when those in the field began to see physicians and other professionals as a special treatment population. She replied:
“When they started making money in alcoholism. As soon as insurance started covering treatment, suddenly you heard that residential treatment was necessary for almost everybody. And since alcoholic docs had tons of money compared to the rest of the public, they not only needed residential treatment, they needed residential treatment in a special treatment facility for many months as opposed to the shorter periods of time that other people needed.”39
Talbott claimed a “92.3 percent recovery rate, according to information compiled from a five-year follow-up survey based on complete abstinence and other treatment.”40
“There is nothing special about a doctor’s alcoholism,” said Bissel
“these special facilities will tell you that they come up with really wonderful recovery rates. They do. And the reason they do is that any time you can grab a professional person by the license and compel him or her into treatment and force them to cooperate with that treatment and then monitor them for years, you’ll get good outcomes—in the high 80s or low 90s in recovery rates—no matter what else you do.”39
“The ones I think are really the best ones were not specialized. There were other well-known specialty clinics that claimed all the docs they treated got well, which is sheer rot. They harmed a great many people, keeping them for long, unnecessary treatments and seeing to it that they hit their financial bottom for sure: kids being yanked out of college, being forced to sell homes to pay for treatment, and otherwise being blackmailed on the grounds that your husband has a fatal disease. It’s ugly.”39
Stanton Peele’s “In the Belly of the American Society of Addiction Medicine Beast” describes the coercion, bullying, threats and indoctrination that are standard operating procedure in Talbott’s facilities.41 Uncooperative patients, “and this covers a range of sins of commission or omission including offering one’s opinion about one’s treatment,” are “threatened with expulsion and with not being certified-or advocated for with their Boards.”41 The cornerstone of treatment is 12-step spiritual recovery. All new patients are indoctrinated into A.A. and coerced to confess they are addicts or alcoholics. Failure to participate in A.A. and 12-step spirituality means expulsion from the program with the anticipated result being loss of one’s medical license.
Fraud, Malpractice, False Diagnoses and False imprisonment
In May 1999 Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for fraud, malpractice, and the novel claim of false imprisonment.42 The fraud finding required a finding that errors in the diagnosis were intentional. After being accused of excessive prescribing of narcotics to his chronic pain patients, Masters was told by the director of the Florida PHP that he could either surrender his medical license until the allegations were disproved or submit to a four-day evaluation. Masters agreed to the latter, thinking he would have an objective and fair evaluation, but was instead diagnosed as “alcohol dependent” and coerced into the Talbott recovery program. He was forced to stay in the program under threat of his medical license as staff would routinely threaten to report any doctor who questioned any aspect of their diagnosis or treatment to their state medical boards “as being an impaired physician, leaving necessary treatment against medical advice”42 which would mean the loss of his licensure. However, Masters was not an alcoholic. According to his attorney, Eric. S. Block, “No one ever accused him of having a problem with alcohol. Not his friends, not his wife, not his seven children, not his fellow doctors, not his employees, not his employers, No one.” 43 He was released 4 months later and forced to sign a five-year “continuing care” contract with the PHP, also under continued threat of his medical license. Talbott faced no professional repercussions and no changes in the treatment protocols were made. Talbott continued to present himself and ASAM as the most qualified advocate for the assessment and treatment of medical professionals for substance abuse and addiction up until his death last year.44
Same System Imposed on Doctors Today—Institutional Injustice Worse due to Laboratory Developed Tests. Fortified Scaffold and Tightened the Noose.
In almost all states today any physician referred for an assessment for substance abuse will be mandated to do so in a facility just like Ridgeview. There is no choice. There is one difference however. When the Ridgeview suicides occurred the plethora of laboratory developed tests were not yet introduced. A decade ago Dr. Gregory Skipper introduced the first laboratory developed test for forensic testing and used it on doctors in physician health programs. These non-FDA approved tests of unknown validity presented a new unpredictable variable into the mix with a positive test necessitating another assessment at an out of state treatment facility—a “PHP-approved” assessment facility. The addition of this laboratory Russian Roulette renders the current system much worse than it was at the time of the Ridgeview suicides.
And if a positive test occurs there are no safeguards protecting the donor. LDTs are unregulated by the FDA. There is no oversight and no one to file a complaint with.
In addition the PHPs have no oversight by the medical boards, departments of health or medical societies. They police themselves. The PHPs have convinced law enforcement that when it comes to doctors it is a “parochial issue” best handled by the medical community. I have been hearing from doctors all over the country who have tried to report crimes to the local police, the state Attorney General and other law enforcement agencies only to be turned back over to the very perpetrators of the crimes. “He’s a sick doctor, we’ll take care of him.” The “swift and certain consequences” of this are an effective means of keeping the rest of the inmates silent. Likewise doctors have been going to the media only to have the door slammed in their faces because the media has generally bought in to the “impaired” and “disruptive” physician construct these same people developed through propaganda, misinformation and moral panics and crusades.
Urgent Need to Admit to the Problem
There has been an increase in physician suicide in the past decade. By my estimate the numbers are going to be far higher than the oft-cited 400 per year. The speculation as to cause has been unenlightening and in fact frustrating. Knowledge of anatomy, access to dangerous drugs, increased workload and even student loans have been proposed as contributing factors. Although there has been some tangential mention of physician health programs it has been indirect. Direct and defined discussion is necessary and state PHPs need to be named as a possible contributor to suicide. Admitting the possibility there is a problem is the first crucial step in defining and addressing the problem. The 1980s historical precedent is correlated with physician suicide. The current system is not only based on Ridgeview but has been fortified in scope and power. The physician health movement has effectively removed due process from doctors while removing answerability and accountability from themselves. And they have not only fortified the scaffold but widened it from substance abusing doctors to all doctors. “Potential impairment” and “relapse without use” were introduced without any meaningful resistance and they are now using a panoply of non-FDA approved laboratory developed tests of unknown validity to test for substances of abuse in a zero-tolerance abstinence based monitoring program. With no regulatory oversight the stage is set not only for error but misuse as witch-pricking devices for punishment and control. Doctors across the country are complaining of the very same abuses Leonard Masters did–false diagnoses, misdiagnosis, unneeded treatment and fraud.
In summary, any doctor who is referred to their state PHP today is required to have any assessment and treatment at a “PHP-approved” facility based on Ridgeview. It is mandated. There is no choice. Coercion, control and abuse at Ridgeview was associated with multiple suicides in doctors in the 1980s. The use of non-FDA approved tests of unknown validity worsens the abuse and fits the “cry of pain” model of hopelessness, helplessness and despair. Locus of control is lost. Organizational justice is absent.
The temporal relationship is clear.
Why is this still the elephant in the room?
This needs to be named, defined and openly discussed and debated. How many more must die before we speak up?
Please help me get the conversation going.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication.Archives of general psychiatry. Jun 2005;62(6):593-602.
Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. General hospital psychiatry. Jan-Feb 2013;35(1):45-49.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school.The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis.2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors.Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
Gonzales L. When Doctors are Addicts: For physicians getting Molly Kellogg is easy. Getting help is not. Chicago Reader. July 28, 1988, 1988.
King M, Durcanin C. The suicides at Ridgeview Institute: A Doctor’s treatment program may be too tough, some say. Atlanta Journal and Constitution. December 18, 1987a, 1987: A12.
Durcanin C, King M. The suicides at Ridgeview Institute: Suicides mar success at Ridgeview with troubled professionals. Atlanta Journal and Constitution. December 18, 1987, 1987: A13.
Bissell L, Royce JE. Ethics for Addiction Professionals. Center City, Minnesota: Hazelden; 1987.
Addiction Scientists from the USA: LeClair Bissell. In: Edwards G, ed. Addiction: Evolution of a Specialist Field. 1 ed: Wiley, John & Sons, Incorporated; 2002:408.
Durcanin C. The suicides at Ridgeview Institute: Staff members didn’t believe Michigan doctor was suicidal. Atlanta Journal and Constitution. December 18, 1987, 1987: A8.
Ricks WS. Ridgeview Institute loses $1.3 million in suit over suicide. Atlanta Journal and Constitution. October 11, 1987, 1987: A1.
King M, Durcanin C. The suicides at Ridgeview Institute: Many drug-using doctors driven to Ridgeview by fear of losing licenses. Atlanta Journal and Constitution. December 18, 1987b, 1987: A1.
Bissell L, Haberman PW. Alcoholism in the Professions. Oxford University Press; 1984.
White W. Reflections of an addiction treatment pioneer. An Interview with LeClair Bissell, MD (1928-2008), conducted January 22, 1997. Posted at http://www.williamwhitepapers.com. 2011.
Williams c. Health care field chemical dependency threat cited. The Tuscaloosa News. January 16, 1988, 1988: 16.
They can be a terror to your mind and show you how to hold your tongue
They got mystery written all over their forehead
They kill babies in the crib and say only the good die young
They don’t believe in mercy
Judgement on them is something that you’ll never see
They can exalt you up or bring you down main route
Turn you into anything that they want you to be–Bob Dylan, Foot of Pride
Although no reliable statistics yet exist, anecdotal reports suggest a marked rise in physician suicide in recent years. From the reports I am receiving it is a lot more than the oft cited “medical school class” of 400 per year.
This necessitates an evaluation of predisposing risk factors such as substance abuse and depression, but also requires a critical examination of what external forces may be involved in the descent from suicidal ideation to suicidal planning to completed suicide. What are the cumulative situational and psychosocial factors in physicians that make suicide a potential option and what acute events precipitate the final act?
Depression and Substance Abuse no Different from General Population
The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria indicate that physicians have the same rates (8-14%) of substance abuse and dependence as the general population,3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 reported a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
Job Stress and Untreated Mental Illness Risk Factors
Job stress coupled with inadequate treatment for mental illness may be factors contributing to physician suicide according to one recent study. Using data from the National Violent Death Reporting System, Gold, Sen, & Schwenk, 2013 8 compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician. Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians. They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”8
Few studies have evaluated the psychosocial stressors surrounding physician suicide but there is no reason to believe they are any different from the rest of the population. Although the triggering life events and specific stressors may vary outside, the inner psyche and undercurrent of thoughts and feelings should remains the same. Perhaps the same drivers of suicide identified in other populations are contributing to physician suicide.
Perceived Helplessness, Hopelessness, Bullying and Defeat
Perceived helplessness is significantly associated with suicide as is9 Hopelessness10,11 Bullying is known to be a predominant trigger for adolescent suicide12-14 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.15
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.16,17 The “Cry of Pain” model 18,19 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life. There is a helplessness and hopelessness that precipitates the descent from ideation, to planning, and then to finality.
Organizational Justice Important Protective Factor
In a study on Italian and Swedish female physicians, degrading experiences and harassment at work were found to be the most powerful independent variables contributing to suicidal thoughts.20 Degrading work experiences harassment, and lack of control over working conditions were found to be associated with suicidal thoughts among Italian and Swedish male university physicians.21
Evidence exists for the role of rescue factors (i.e. social support) as buffers against suicide in the face of varying degrees of life stress.22,23 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 20 and support at work when difficulties arose appeared to be a protective factor for the male physicians.21 In line with this, studies of Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.24,25 Organizational justice has been identified as a psychosocial predictor of health and wellbeing2627 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.28,29
Historical Precedent-the Suicides at Ridgeview
Could these factors be playing a role in physician suicide? They evidently did at the Ridgeview Institute, a drug and alcohol treatment program for impaired physicians in Metropolitan Atlanta created by G. Douglas Talbott. Talbott helped organize and served as past president of the American Society of Addiction Medicine (ASAM) and was a formative figure in the American Medical Association’s (AMA’s) Impaired Physician Program. He has owned and directed a number of treatment facilities for impaired professionals, most recently the Talbott Recovery Campus in Atlanta, one of the preferred referrals for physicians ordered into evaluation and treatment by licensing boards.
After creating the DeKalb County Impaired Physicians Committee for the Medical Association of Georgia, Talbott founded the Georgia Disabled Doctors Program in 1975 in part because “traditional one-month treatment programs are inadequate for disabled doctors.” According to Talbott, rehabilitation programs that evaluate and treat the rest of the population for substance abuse issues are incapable of doing so in doctors as they are unlike others. He bases this uniqueness on “incredibly high denial”, and what he calls the “four MDs,” “M-Deity”, “Massive Denial” “Militant Defensiveness”, and “More Drugs.”30
Contingency Management = Extortion Using Medical License
According to Talbott, “impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.” “Terminal uniqueness “ is a phrase Talbott uses to describe doctors’ tendency to think they can heal themselves. “M-Deity” refers to doctors “being trained to think they’re God,”31 an unfounded generalization considering the vast diversity of individuals that make up our profession. This attitude, according to some critics, stems from the personal histories of the treatment staff, including Talbott, who are recovering alcoholics and addicts themselves. One such critic was Assistant Surgeon General under C. Everett Koop John C. Duffy who said that Ridgeview suffered from a “boot-camp mentality” toward physicians under their care and “assume every physician suffering from substance abuse is the same lying, stealing, cheating, manipulating individual they were when they had the illness. Certainly some physicians are manipulative, but it’s naïve to label all physicians with these problems.”32
American Society of Addiction Medicine (ASAM) President (1981-1983) LeClair Bissell was also highly critical of Talbott’s approach. Bissell, co-author of the first textbook of ethics for addiction professionals33 when asked if there was any justification to the claim that doctors are sicker than other people and more vulnerable to addiction replied:
“Well, based on my treatment experience, I think they are less sick and much easier to treat than many other groups. I think one reason for that is that in order to become a physician…one has to have jumped over a great many hurdles. One must pass the exams, survive the screening tests and the interviews, be able to organize oneself well enough to do examinations and so on, and be observed by a good many colleagues along the way. Therefore I think the more grossly psychotic, or sicker, are frequently screened out along the way. The ones we get in treatment are usually people who are less brain-damaged, are still quite capable of learning, are reasonably bright. Not only that, but they are quite well motivated in most cases to hang on to their licenses, the threat of the loss of which is frequently what puts them in treatment in the first place. So are they hard to treat? No! Are they easy patients? Yes! Are they more likely to be addicted than other groups? We don’t know.”34
“I’m not much for the bullying that goes along with some of these programs,” Bissell commented to the Atlanta Journal and Constitution in 1987.31 The constitution did a series of reports after five inpatients committed suicide during a four-year period at Ridgeview.35 In addition there were at least 20 more who had killed themselves over the preceding 12 years after leaving the treatment center.32
Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.”31 According to Bissell: “There’s a lot of debate in the field over whether treatment imposed by threats is worthwhile…To a large degree a person has to seek the treatment on his own accord before it will work for him.”31
A jury awarded $1.3 million to the widow of one of the deceased physicians against Ridgeview,36 and other lawsuits initiated on behalf of suicides were settled out of court.35
The Constitution reported that doctors entered the program under threats of loss of licensure “even when they would prefer treatment that is cheaper and closer to home.” 37 The paper also noted that Ridgeview “enjoys unparalleled connections with many local and state medical societies that work with troubled doctors,” “licensing boards often seek recommendations from such groups in devising an approved treatment plan,” and those in charge are often “physicians who themselves have successfully completed Ridgeview’s program.”37
The cost of a 28-day program for nonprofessionals at Ridgeview in 1987 was $10,000 while the cost was “higher for those going through impaired-health professionals program,” which lasted months rather than 28 days.32
In 1997 William L. White interviewed Bissell whom he called “one of the pioneers in the treatment of impaired professionals.” The interview was not published until after hear death in 2008 per her request. Noting her book Alcoholism in the Professions38“remains one of the classics in the field”, White asked her when those in the field began to see physicians and other professionals as a special treatment population. She replied:
“When they started making money in alcoholism. As soon as insurance started covering treatment, suddenly you heard that residential treatment was necessary for almost everybody. And since alcoholic docs had tons of money compared to the rest of the public, they not only needed residential treatment, they needed residential treatment in a special treatment facility for many months as opposed to the shorter periods of time that other people needed.”39
Talbott claimed a “92.3 percent recovery rate, according to information compiled from a five-year follow-up survey based on complete abstinence and other treatment.”40
“There is nothing special about a doctor’s alcoholism,” said Bissel
“these special facilities will tell you that they come up with really wonderful recovery rates. They do. And the reason they do is that any time you can grab a professional person by the license and compel him or her into treatment and force them to cooperate with that treatment and then monitor them for years, you’ll get good outcomes—in the high 80s or low 90s in recovery rates—no matter what else you do.”39
“The ones I think are really the best ones were not specialized. There were other well-known specialty clinics that claimed all the docs they treated got well, which is sheer rot. They harmed a great many people, keeping them for long, unnecessary treatments and seeing to it that they hit their financial bottom for sure: kids being yanked out of college, being forced to sell homes to pay for treatment, and otherwise being blackmailed on the grounds that your husband has a fatal disease. It’s ugly.”39
Stanton Peele’s “In the Belly of the American Society of Addiction Medicine Beast” describes the coercion, bullying, threats and indoctrination that are standard operating procedure in Talbott’s facilities.41 Uncooperative patients, “and this covers a range of sins of commission or omission including offering one’s opinion about one’s treatment,” are “threatened with expulsion and with not being certified-or advocated for with their Boards.”41 The cornerstone of treatment is 12-step spiritual recovery. All new patients are indoctrinated into A.A. and coerced to confess they are addicts or alcoholics. Failure to participate in A.A. and 12-step spirituality means expulsion from the program with the anticipated result being loss of one’s medical license.
From a talk given by FSPHP
Fraud, Malpractice, False Diagnoses and False imprisonment
In May 1999 Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for fraud, malpractice, and the novel claim of false imprisonment.42 The fraud finding required a finding that errors in the diagnosis were intentional. After being accused of excessive prescribing of narcotics to his chronic pain patients, Masters was told by the director of the Florida PHP that he could either surrender his medical license until the allegations were disproved or submit to a four-day evaluation. Masters agreed to the latter, thinking he would have an objective and fair evaluation, but was instead diagnosed as “alcohol dependent” and coerced into the Talbott recovery program. He was forced to stay in the program under threat of his medical license as staff would routinely threaten to report any doctor who questioned any aspect of their diagnosis or treatment to their state medical boards “as being an impaired physician, leaving necessary treatment against medical advice”42 which would mean the loss of his licensure. However, Masters was not an alcoholic. According to his attorney, Eric. S. Block, “No one ever accused him of having a problem with alcohol. Not his friends, not his wife, not his seven children, not his fellow doctors, not his employees, not his employers, No one.” 43 He was released 4 months later and forced to sign a five-year “continuing care” contract with the PHP, also under continued threat of his medical license. Talbott faced no professional repercussions and no changes in the treatment protocols were made. Talbott continued to present himself and ASAM as the most qualified advocate for the assessment and treatment of medical professionals for substance abuse and addiction up until his death last year.44
Same System Imposed on Doctors Today—Institutional Injustice Worse due to Laboratory Developed Tests. Fortified Scaffold and Tightened the Noose.
In almost all states today any physician referred for an assessment for substance abuse will be mandated to do so in a facility just like Ridgeview. There is no choice. There is one difference however. When the Ridgeview suicides occurred the plethora of laboratory developed tests were not yet introduced. A decade ago Dr. Gregory Skipper introduced the first laboratory developed test for forensic testing and used it on doctors in physician health programs. These non-FDA approved tests of unknown validity presented a new unpredictable variable into the mix with a positive test necessitating another assessment at an out of state treatment facility—a “PHP-approved” assessment facility. The addition of this laboratory Russian Roulette renders the current system much worse than it was at the time of the Ridgeview suicides.
And if a positive test occurs there are no safeguards protecting the donor. LDTs are unregulated by the FDA. There is no oversight and no one to file a complaint with.
In addition the PHPs have no oversight by the medical boards, departments of health or medical societies. They police themselves. The PHPs have convinced law enforcement that when it comes to doctors it is a “parochial issue” best handled by the medical community. I have been hearing from doctors all over the country who have tried to report crimes to the local police, the state Attorney General and other law enforcement agencies only to be turned back over to the very perpetrators of the crimes. “He’s a sick doctor, we’ll take care of him.” The “swift and certain consequences” of this are an effective means of keeping the rest of the inmates silent. Likewise doctors have been going to the media only to have the door slammed in their faces because the media has generally bought in to the “impaired” and “disruptive” physician construct these same people developed through propaganda, misinformation and moral panics and crusades.
Urgent Need to Admit to the Problem
There has been an increase in physician suicide in the past decade. By my estimate the numbers are going to be far higher than the oft-cited 400 per year. The speculation as to cause has been unenlightening and in fact frustrating. Knowledge of anatomy, access to dangerous drugs, increased workload and even student loans have been proposed as contributing factors. Although there has been some tangential mention of physician health programs it has been indirect. Direct and defined discussion is necessary and state PHPs need to be named as a possible contributor to suicide. Admitting the possibility there is a problem is the first crucial step in defining and addressing the problem. The 1980s historical precedent is correlated with physician suicide. The current system is not only based on Ridgeview but has been fortified in scope and power. The physician health movement has effectively removed due process from doctors while removing answerability and accountability from themselves. And they have not only fortified the scaffold but widened it from substance abusing doctors to all doctors. “Potential impairment” and “relapse without use” were introduced without any meaningful resistance and they are now using a panoply of non-FDA approved laboratory developed tests of unknown validity to test for substances of abuse in a zero-tolerance abstinence based monitoring program. With no regulatory oversight the stage is set not only for error but misuse as witch-pricking devices for punishment and control. Doctors across the country are complaining of the very same abuses Leonard Masters did–false diagnoses, misdiagnosis, unneeded treatment and fraud.
In summary, any doctor who is referred to their state PHP today is required to have any assessment and treatment at a “PHP-approved” facility based on Ridgeview. It is mandated. There is no choice. Coercion, control and abuse at Ridgeview was associated with multiple suicides in doctors in the 1980s. The use of non-FDA approved tests of unknown validity worsens the abuse and fits the “cry of pain” model of hopelessness, helplessness and despair. Locus of control is lost. Organizational justice is absent.
The temporal relationship is clear.
Why is this still the elephant in the room?
This needs to be named, defined and openly discussed and debated. How many more must die before we speak up?
Please help me get the conversation going.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. General hospital psychiatry. Jan-Feb 2013;35(1):45-49.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis. 2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors. Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
Gonzales L. When Doctors are Addicts: For physicians getting Molly Kellogg is easy. Getting help is not. Chicago Reader. July 28, 1988, 1988.
King M, Durcanin C. The suicides at Ridgeview Institute: A Doctor’s treatment program may be too tough, some say. Atlanta Journal and Constitution. December 18, 1987a, 1987: A12.
Durcanin C, King M. The suicides at Ridgeview Institute: Suicides mar success at Ridgeview with troubled professionals. Atlanta Journal and Constitution. December 18, 1987, 1987: A13.
Bissell L, Royce JE. Ethics for Addiction Professionals. Center City, Minnesota: Hazelden; 1987.
Addiction Scientists from the USA: LeClair Bissell. In: Edwards G, ed. Addiction: Evolution of a Specialist Field. 1 ed: Wiley, John & Sons, Incorporated; 2002:408.
Durcanin C. The suicides at Ridgeview Institute: Staff members didn’t believe Michigan doctor was suicidal. Atlanta Journal and Constitution. December 18, 1987, 1987: A8.
Ricks WS. Ridgeview Institute loses $1.3 million in suit over suicide. Atlanta Journal and Constitution. October 11, 1987, 1987: A1.
King M, Durcanin C. The suicides at Ridgeview Institute: Many drug-using doctors driven to Ridgeview by fear of losing licenses. Atlanta Journal and Constitution. December 18, 1987b, 1987: A1.
Bissell L, Haberman PW. Alcoholism in the Professions. Oxford University Press; 1984.
White W. Reflections of an addiction treatment pioneer. An Interview with LeClair Bissell, MD (1928-2008), conducted January 22, 1997. Posted at http://www.williamwhitepapers.com. 2011.
Williams c. Health care field chemical dependency threat cited. The Tuscaloosa News. January 16, 1988, 1988: 16.
Although no reliable statistics yet exist, anecdotal reports suggest a marked rise inphysician suicide in recent years. From the reports I am receiving it is a lot more than the oft cited “medical school class” of 400 per year.
This necessitates an evaluation of predisposing risk factors such as substance abuse and depression, but also requires a critical examination of what external forces may be involved. What acute and cumulative situational and psychosocial factors are involved in the descent from suicidal ideation to planning to completion? What makes suicide a potential option for doctors and what acute events precipitate and trigger the final act?
Depression and Substance Abuse no Different from General Population
The prevalence of depression in physicians is close to that of the general population1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria indicate that physicians have the same rates (8-14%) of substance abuse and dependence as the general population,3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 reported a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
Job Stress and Untreated Mental Illness Risk Factors
Job stress coupled with inadequate treatment for mental illness may be factors contributing to physician suicide according to one recent study. Using data from the National Violent Death Reporting System, Gold, Sen, & Schwenk, 2013 8 compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians. They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”8
Few studies have evaluated the psychosocial stressors surrounding physician suicide but there is no reason to believe they are any different from the rest of the population. Although the triggering life events and specific stressors may vary outside, the inner psyche and undercurrent of thoughts and feelings should remains the same. Perhaps the same drivers of suicide identified in other populations are contributing to physician suicide.
Perceived Helplessness, Hopelessness, Bullying and Defeat
Perceived helplessness is significantly associated with suicide as is9Hopelessness10,11 Bullying is known to be a predominant trigger for adolescent suicide12-14 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.15
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.16,17
The “Cry of Pain” model 18,19 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life. There is a helplessness and hopelessness that precipitates the descent from ideation, to planning, and then to finality.
Organizational Justice Important Protective Factor
In a study on Italian and Swedish female physicians, degrading experiences and harassment at work were found to be the most powerful independent variables contributing to suicidal thoughts.20 Degrading work experiences harassment, and lack of control over working conditions were found to be associated with suicidal thoughts among Italian and Swedish male university physicians.21
Evidence exists for the role of rescue factors (i.e. social support) as buffers against suicide in the face of varying degrees of life stress.22,23 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 20 and support at work when difficulties arose appeared to be a protective factor for the male physicians.21 In line with this, studies of Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.24,25 Organizational justice has been identified as a psychosocial predictor of health and wellbeing. 2627 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.28,29
Historical Precedent-the Suicides at Ridgeview
Could these factors be playing a role in physician suicide? They evidently did at the Ridgeview Institute, a drug and alcohol treatment program for impaired physicians in Metropolitan Atlanta created by G. Douglas Talbott.
Talbott helped organize and served as past president of the American Society of Addiction Medicine (ASAM) and was a formative figure in the American Medical Association’s (AMA’s) Impaired Physician Program. He has owned and directed a number of treatment facilities for impaired professionals, most recently the Talbott Recovery Campus in Atlanta, one of the preferred referrals for physicians ordered into evaluation and treatment by licensing boards.
After creating the DeKalb County Impaired Physicians Committee for the Medical Association of Georgia, Talbott founded the Georgia Disabled Doctors Program in 1975 in part because “traditional one-month treatment programs are inadequate for disabled doctors.” According to Talbott, rehabilitation programs that evaluate and treat the rest of the population for substance abuse issues are incapable of doing so in doctors as they are unlike others. He bases this uniqueness on “incredibly high denial”, and what he calls the “four MDs,” “M-Deity”, “Massive Denial” “Militant Defensiveness”, and “More Drugs.”30
Contingency Management = Extortion Using Medical License
According to Talbott, “impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.” “Terminal uniqueness “ is a phrase Talbott uses to describe doctors’ tendency to think they can heal themselves. “M-Deity” refers to doctors “being trained to think they’re God,”31 an unfounded generalization considering the vast diversity of individuals that make up our profession. This attitude, according to some critics, stems from the personal histories of the treatment staff, including Talbott, who are recovering alcoholics and addicts themselves. One such critic was Assistant Surgeon General under C. Everett Koop John C. Duffy who said that Ridgeview suffered from a “boot-camp mentality” toward physicians under their care and “assume every physician suffering from substance abuse is the same lying, stealing, cheating, manipulating individual they were when they had the illness. Certainly some physicians are manipulative, but it’s naïve to label all physicians with these problems.”32
American Society of Addiction Medicine (ASAM) President (1981-1983) LeClair Bissell was also highly critical of Talbott’s approach. Bissell, co-author of the first textbook of ethics for addiction professionals 33 when asked if there was any justification to the claim that doctors are sicker than other people and more vulnerable to addiction replied:
“Well, based on my treatment experience, I think they are less sick and much easier to treat than many other groups. I think one reason for that is that in order to become a physician…one has to have jumped over a great many hurdles. One must pass the exams, survive the screening tests and the interviews, be able to organize oneself well enough to do examinations and so on, and be observed by a good many colleagues along the way. Therefore I think the more grossly psychotic, or sicker, are frequently screened out along the way. The ones we get in treatment are usually people who are less brain-damaged, are still quite capable of learning, are reasonably bright. Not only that, but they are quite well motivated in most cases to hang on to their licenses, the threat of the loss of which is frequently what puts them in treatment in the first place. So are they hard to treat? No! Are they easy patients? Yes! Are they more likely to be addicted than other groups? We don’t know.”34
“I’m not much for the bullying that goes along with some of these programs,” Bissell commented to the Atlanta Journal and Constitution in 1987.31
The Constitution did a series of reports after five inpatients committed suicide during a four-year period at Ridgeview.35 In addition there were at least 20 more who had killed themselves over the preceding 12 years after leaving the treatment center.32
Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.” 31
According to Bissell: “There’s a lot of debate in the field over whether treatment imposed by threats is worthwhile…To a large degree a person has to seek the treatment on his own accord before it will work for him.”31
A jury awarded $1.3 million to the widow of one of the deceased physicians against Ridgeview,36 and other lawsuits initiated on behalf of suicides were settled out of court.35
The Constitution reported that doctors entered the program under threats of loss of licensure “even when they would prefer treatment that is cheaper and closer to home.” 37
The paper also noted that Ridgeview “enjoys unparalleled connections with many local and state medical societies that work with troubled doctors,” “licensing boards often seek recommendations from such groups in devising an approved treatment plan,” and those in charge are often “physicians who themselves have successfully completed Ridgeview’s program.”37
The cost of a 28-day program for nonprofessionals at Ridgeview in 1987 was $10,000 while the cost was “higher for those going through impaired-health professionals program,” which lasted months rather than 28 days.32
In 1997 William L. White interviewed Bissell whom he called “one of the pioneers in the treatment of impaired professionals.” The interview was not published until after hear death in 2008 per her request. Noting her book Alcoholism in the Professions 38“remains one of the classics in the field”, White asked her when those in the field began to see physicians and other professionals as a special treatment population. She replied:
“When they started making money in alcoholism. As soon as insurance started covering treatment, suddenly you heard that residential treatment was necessary for almost everybody. And since alcoholic docs had tons of money compared to the rest of the public, they not only needed residential treatment, they needed residential treatment in a special treatment facility for many months as opposed to the shorter periods of time that other people needed.”39
Talbott claimed a “92.3 percent recovery rate, according to information compiled from a five-year follow-up survey based on complete abstinence and other treatment.”40
“There is nothing special about a doctor’s alcoholism,” said Bissel
“”These special facilities will tell you that they come up with really wonderful recovery rates. They do. And the reason they do is that any time you can grab a professional person by the license and compel him or her into treatment and force them to cooperate with that treatment and then monitor them for years, you’ll get good outcomes—in the high 80s or low 90s in recovery rates—no matter what else you do.”39
“The ones I think are really the best ones were not specialized. There were other well-known specialty clinics that claimed all the docs they treated got well, which is sheer rot. They harmed a great many people, keeping them for long, unnecessary treatments and seeing to it that they hit their financial bottom for sure: kids being yanked out of college, being forced to sell homes to pay for treatment, and otherwise being blackmailed on the grounds that your husband has a fatal disease. It’s ugly.”39
Stanton Peele’s “In the Belly of the American Society of Addiction Medicine Beast” describes the coercion, bullying, threats and indoctrination that are standard operating procedure in Talbott’s facilities.41 Uncooperative patients, “and this covers a range of sins of commission or omission including offering one’s opinion about one’s treatment,” are “threatened with expulsion and with not being certified-or advocated for with their Boards.”41 The cornerstone of treatment is 12-step spiritual recovery. All new patients are indoctrinated into A.A. and coerced to confess they are addicts or alcoholics. Failure to participate in A.A. and 12-step spirituality means expulsion from the program with the anticipated result being loss of one’s medical license.
Fraud, Malpractice, False Diagnoses and False imprisonment
In May 1999 Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for fraud, malpractice, and the novel claim of false imprisonment.42 The fraud finding required a finding that errors in the diagnosis were intentional. After being accused of excessive prescribing of narcotics to his chronic pain patients, Masters was told by the director of the Florida PHP that he could either surrender his medical license until the allegations were disproved or submit to a four-day evaluation. Masters agreed to the latter, thinking he would have an objective and fair evaluation, but was instead diagnosed as “alcohol dependent” and coerced into the Talbott recovery program. He was forced to stay in the program under threat of his medical license as staff would routinely threaten to report any doctor who questioned any aspect of their diagnosis or treatment to their state medical boards “as being an impaired physician, leaving necessary treatment against medical advice”42 which would mean the loss of his licensure.
However, Masters was not an alcoholic. According to his attorney, Eric. S. Block, “No one ever accused him of having a problem with alcohol. Not his friends, not his wife, not his seven children, not his fellow doctors, not his employees, not his employers, No one.” 43 He was released 4 months later and forced to sign a five-year “continuing care” contract with the PHP, also under continued threat of his medical license. Talbott faced no professional repercussions and no changes in the treatment protocols were made. Talbott continued to present himself and ASAM as the most qualified advocate for the assessment and treatment of medical professionals for substance abuse and addiction up until his death last year.44
Same System Imposed on Doctors Today—Institutional Injustice Worse due to Laboratory Developed Tests. Fortified Scaffold and Tightened the Noose.
In almost all states today any physician referred for an assessment for substance abuse will be mandated to do so in a facility just like Ridgeview. There is no choice. There is one difference however. When the Ridgeview suicides occurred the plethora of laboratory developed tests were not yet introduced.
In addition state PHPs have no oversight or regulation. They police themselves. Medical boards, departments of public health and medical societies provide no oversight. Accountability is absent.
Moreover they have apparently convinced law enforcement that when it comes to doctors it is a “parochial issue” best handled by the medical community. I have been hearing from doctors all over the country who have tried to report crimes to the local police, the state Attorney General and other law enforcement agencies only to be turned back over to the very perpetrators of the crimes. “He’s a sick doctor, we’ll take care of him.”
The “swift and certain consequences” of this are an effective means of keeping the majority silent. Likewise doctors have been going to the media only to have the door slammed in their faces because the media has generally bought in to the “impaired” and “disruptive” physician construct these same people developed through propaganda, misinformation and moral panics.
Urgent Need to Admit to the Problem
There has been an increase in physician suicide in the past decade. By my estimate the numbers are going to be far higher than the oft-cited 400 per year. The speculation as to cause has been unenlightening and in fact frustrating. Knowledge of anatomy, access to dangerous drugs, increased workload and even student loans have been proposed as contributing factors. Although there has been some tangential mention of physician health programs it has been indirect.
Direct and defined discussion is necessary and state PHPs need to be named as a possible contributor to suicide. Admitting the possibility there is a problem is the first crucial step in defining and addressing the problem. The 1980s historical precedent is correlated with physician suicide. The current system is not only based on Ridgeview but has been fortified in scope and power. The physician health movement has effectively removed due process from doctors while removing answerability and accountability from themselves.
And they have not only fortified the scaffold but widened it from substance abusing doctors to all doctors. “Potential impairment” and “relapse without use” were introduced without any meaningful resistance and they are now using a panoply of non-FDA approved laboratory developed tests of unknown validity to test for substances of abuse in a zero-tolerance abstinence based monitoring program.
With no regulatory oversight the stage is set not only for error but misuse as witch-pricking devices for punishment and control. Doctors across the country are complaining of the very same abuses Leonard Masters did–false diagnoses, misdiagnosis, unneeded treatment and fraud.
In summary, any doctor who is referred to their state PHP today is required to have any assessment and treatment at a “PHP-approved” facility based on Ridgeview. It is mandated. There is no choice. Coercion, control and abuse at Ridgeview was associated with multiple suicides in doctors in the 1980s.
The use of non-FDA approved tests of unknown validity worsens the abuse and fits the “cry of pain” model of hopelessness, helplessness and despair.
Locus of control is lost. Organizational justice is absent. The temporal relationship is clear.
Why is this still the elephant in the room?
This needs to be named, defined and openly discussed and debated. How many more must die before we speak up?
Please help me get the conversation going. I need allies.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication.Archives of general psychiatry. Jun 2005;62(6):593-602.
Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. General hospital psychiatry. Jan-Feb 2013;35(1):45-49.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school.The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach.The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis.2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors.Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
Gonzales L. When Doctors are Addicts: For physicians getting Molly Kellogg is easy. Getting help is not. Chicago Reader. July 28, 1988, 1988.
King M, Durcanin C. The suicides at Ridgeview Institute: A Doctor’s treatment program may be too tough, some say. Atlanta Journal and Constitution.December 18, 1987a, 1987: A12.
Durcanin C, King M. The suicides at Ridgeview Institute: Suicides mar success at Ridgeview with troubled professionals. Atlanta Journal and Constitution.December 18, 1987, 1987: A13.
Bissell L, Royce JE. Ethics for Addiction Professionals. Center City, Minnesota: Hazelden; 1987.
Addiction Scientists from the USA: LeClair Bissell. In: Edwards G, ed.Addiction: Evolution of a Specialist Field. 1 ed: Wiley, John & Sons, Incorporated; 2002:408.
Durcanin C. The suicides at Ridgeview Institute: Staff members didn’t believe Michigan doctor was suicidal. Atlanta Journal and Constitution. December 18, 1987, 1987: A8.
Ricks WS. Ridgeview Institute loses $1.3 million in suit over suicide. Atlanta Journal and Constitution. October 11, 1987, 1987: A1.
King M, Durcanin C. The suicides at Ridgeview Institute: Many drug-using doctors driven to Ridgeview by fear of losing licenses. Atlanta Journal and Constitution. December 18, 1987b, 1987: A1.
Bissell L, Haberman PW. Alcoholism in the Professions. Oxford University Press; 1984.
White W. Reflections of an addiction treatment pioneer. An Interview with LeClair Bissell, MD (1928-2008), conducted January 22, 1997. Posted athttp://www.williamwhitepapers.com. 2011.
Williams c. Health care field chemical dependency threat cited. The Tuscaloosa News. January 16, 1988, 1988: 16.
The bad science, bad medicine, bad policy and bad actors are easy to identify. It would be like shooting fish in a barrel.
So what are the barriers?
Why has this not been done?
The answer to that is complex but involves a confluence of factors including psychological, political and cultural. “Feel good fallacy,” “political correctness, and moral and policy entrepreneurship have effectively swayed the targets intended. The well-funded misinformation and propaganda was cast with a large net using the same techniques others have successfully used throughout history to accomplish the same. Moral panics, moral crusades, and a plethora of logical fallacy have been used and used with considerable resources and skill.
So what can we do about it?
The first “step into the breach” is to identify the problem with the first one being the Emperor has no clothes. Once this is acknowledged it would not take long to address directly the specific problems and erroneous assumptions of this paradigm through the lenses of science, critical reasoning, ethics and common sense. If this were to be done the entire Potemkin village would fall like a house of cards.
But the very first and simplest step is to use your voice to question this authority. Neutrality is not an option. Either support what these groups are doing or question them with your voice and the written word.
The bad science, medicine, policy and actors are obvious. It would be like shooting fish in a barrel and the first target needs to be the “PHP-Blueprint.” It would be so easy to take down this “research” they are using to promote PHPs as a “gold-standard” and replicable model. Shooting fish in a barrel requires someone take aim and at this point hardly anyone is even willing to pick up the gun.
What we need is a Marcia Angell to take on the multi-billion dollar drug and alcohol testing, assessment and treatment industry.
While all eyes were focused on the drug companies these multi-billion dollar industries erected a scaffold of immunity and profit by removing (and blocking) themselves from essentially all aspects of accountability; answerability, justification for actions and the ability to be punished by outside actors. The 2009 quote in reference to “big pharma” is just as applicable to the drug and alcohol testing industry,” the inpatient assessment and treatment centers and the “authorities” pushing public policy and swaying public opinion to accept irrational and illegitimate authoritative opinion as truth.
And unlike the pharmaceutical industries carefully constructed “bent science” which requires a keen eye and critical analysis , the evidence-base supporting the testing, assessment and treatment industry rests on a foundation that can…
Pharmacard: A Prescription Drug Monitoring System Designed to Record Drug Histories and Reduce the Incidence of “Drug Misadventuring.”
As a medical student in 1990 I saw a 79 year old woman in the emergency room with intractable nausea and vomiting. Earlier that week she had seen her primary care physician for nausea and a mild cough. Diagnosed with bronchitis, she was given a prescription for erythromycin. Her husband brought in her medications including digoxin which can cause nausea
when blood levels are too high. A markedly high level came back on the blood draw indicating digitalis toxicity. I spoke to her primary care physician who was unaware of her digoxin prescription; completely clueless that she was prescribed the foxglove plant extract by a cardiologist for an irregular heart beat.
Digitalis was first described by William Withering in 1785 for heart conditions and this is considered the beginning of modern therapeutics. Sometime after erythromycin became available in 1952 it was discovered that taking the two drugs together increased digoxin levels. This simplest type of drug interaction is called interference and occurs when one drug either accelerates of slows down the metabolism or excretion of the other.
Based on the progression of symptoms her husband reported and the elevated levels on admission this woman undoubtedly had elevated digitalis levels when she was seen by her doctor earlier in the week. Unaware of the digitalis he inadvertently worsened her condition by giving her a medication that elevated her levels even further. She was lucky.
The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).
Digitalis toxicity in those who die outside of the hospital often goes unrecognized as most are elderly and assumed to have died from age related causes.
Seeing several more cases of drug related problems caused by ignorance of current medications and lack of communication prompted an interest in drug misadventures. I also became interested in developing a computerized up to date and accurate record accessible by all health care providers in real time , a closed loop system of “portable” information easily transferred among all health care providers be they primary doctors, pharmacists or emergency room personnel.
Research pharmacologist Dr. Edward Gallaher and I brainstormed over ideas and eventually came up with a computer program using WORM (write-once-read-many) optical technology used in compact disc systems. much like a CD-R but without the spinning disc. The credit-card sized disk could store up to two megabytes of data on an optical layer that could be written once and never changed. An optical card-reader interfaced with any IBM compatible PC. The plan was to place card readers at pharmacies, medical offices and emergency rooms. We called it Pharmacard.
Pharmacard System Developed. ASTI Connections. Vol 4. Eugene, OR: Advanced Science and Technology Institute; 1992.
Although computerized medical records existed in 1992 they were predominantly stand alone with many just replicating the paper record without word search capability. Moreover these programs did not communicate with one another so no information portability existed between the entities involved. Communication of information from pharmacy to doctors to emergency room was not an option. The system was fragmented and the search for information long.
But drug mishaps were a real problem. As with digoxin they could be fatal. Multiple reports of drug induced morbidity and mortality were found in literature searches. An obvious problem existed. . Many were drug interactions such as that with digitalis and erythromycin. From my viewpoint the need for addressing the problems caused by inadequate and and incomplete records was not only self-evident but a priority. Solutions however were few. “Brown-bag” sessions in which patients bring in a paper bag containing all of their meds were held periodically. Little booklets titled “patient medication records” were given to patients to update and record their new and current prescriptions.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
An available baseline EKG was decided based on its presence making it much easier to detect a problem by looking for differences. A baseline EKG would conceivably facilitate the timing and accuracy of diagnosis. In addition it would save money because without a comparison the default is admission.
We then applied for multiple research grants for funding to do a pilot study. All were rejected and contained comments suggesting we pitch our wares to the computer people not the medical people-this is computer science not medical science.
We received very little interest at an AMA poster presentation in Washington D.C. Few people would even read the poster with most taking a quick glance and redirecting straight ahead as if they were avoiding a street-corner pollster. Those who did read it were either non-plussed, perplexed or cynical.
A research psychopharmacologist M.D.,PhD from France asked permission to give me some advice. He then told me it would not work. He said the idea was great, it would work as intended and probably help prevent drug related problems. But that did not matter because no one
gets it yet.”
Aside from a handful of people intimately involved in the research most everyone else finds this useless as do most people at the conference. This means nothing to them.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
In 1999 the Institute of Medicine published To Err is Human: Building a Safer Health Care System placing patient safety high on the nation’s health care agenda. Medical errors, adverse drug reactions and interactions were deemed a big problem. Identifying ways to keep track of medications became a priority and multiple business ventures popped up and got their hats in the ring. Suddenly everyone not only recognized the problem but imparted the sense they knew it all along. Seven years had gone by and our project had then fallen by the wayside. In addition our optical platform was obsolete.
As with firefighter arson this illustrates the most crucial step in addressing a problem is admitting the problem exists. Firefighter arson had been documented for over a century but not properly addressed. The extent of the problem was not publicly recognized until a Special Report: Firefighter Arson was done by the Department of Homeland Security, the United States Fire Administration and the National Fire Data Center in 2003. The most crucial step was admitting the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.
Skipper’s introduction of junk science drug and alcohol testing and use of cutoff points he pulls out of a hat and then moves upward as the problems are exposed is shameful. The fact that he unleashed this on other doctors knowing full well what would happen in a zero tolerance program needs to be revealed.
My survey is revealing many suicides as a direct result of these tests, including those of medical students and residents. And most of those who have died were not even remotely addicts or alcoholics. They were reported anonymously, given one of these tests and asked to be evaluated at a “PHP-approved” assessment center where a diagnosis was confirmed followed by 3-4 months of inpatient treatment. I am finding out most of the doctors referred to PHPs do not have any problems but the PHPs and their affiliates are giving false diagnoses, false drug testing and using threats to control them and there is little they can do about it. Skipper’s complete lack of empathy for his victims as he continues to put coins in his purse is abhorrent. Meanwhile the death count continues to rise.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to doctors and how they might be involved in the descent from suicidal ideation to suicidal planning to completed suicide.
Depression and Substance Abuse Comparable to General Population
Depression and substance abuse are the two biggest risk factors for suicide. The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria suggest that physicians have the same rates (8-14%) of substance abuse and dependence as the rest of the population 3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 found a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
State Physician Health Programs
Perhaps it is how physicians are treated differently when they develop a substance abuse or mental health problem.
Physician Health Programs (PHP) can be considered an equivalent to Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Originally developed as “impaired physician” programs, the PHPs were created to help doctors who developed problems with substance abuse or addiction an alternative to disciplinary action by State Medical Boards. These programs existed in almost every state by 1980. Often staffed by volunteer physicians and funded State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referrals. Most EAPs were developed with the collaboration of workers unions or some other group supporting the rights and interests of the workers. As there is no such organization representing doctors, PHPs developed in the absence of regulation or oversight. As a consequence there is no meaningful accountability.
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”8
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “that the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 8 They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”8 Unfortunately this has not happened. Most physicians have no idea that the state physician health programs have been taken over by the “impaired physicians movement.”
In his Psychology Todayblog, Boyd again recommends oversight and regulation of PHPs. He cites the North Carolina Physicians Health Program Audit released in April of 2014 that reported the below key findings:
As with Knight and Boyd’s paper outlining the ethical and managerial problems in PHPs, the NC PHP audit finding that abuse could occur and not be detected generated little interest from either the medical community or the media.
Although state PHPs present themselves as confidential caring programs of benevolence they are essentially monitoring programs for physicians who can be referred to them for issues such as being behind on chart notes. If the PHP feels a doctor is in need of PHP “services” they must then abide by any and all demands of the PHP or be reported to their medical board under threat of loss of licensure.
LDTs bypass the FDA approval process and have no meaningful regulatory oversight. The LDT pathway was not designed for “forensic” tests but clinical tests with low risk. Some are arguing for regulation and oversight of LDTs due to questionable validity and risk of patient harm.13
These same physicians are claiming a high success rate for PH programs9 and suggesting that they be used for random testing of all physicians.14
As with LDTs, the state PHPs are unregulated, and without oversight. State medical societies and departments of health have no control over state PHPs.
Their opacity is bolstered by peer-review immunity, HIPPA, HCQIA, and confidentiality agreements. The monitored physician is forced to abide by any and all demands of the PHP no matter how unreasonable-all under the coloration of medical utility and without any evidentiary standard or right to appeal.
The ASAM has a certification process for physicians and claim to be “addiction” specialists. This“board certification” is not recognized by the American Board of Medical Specialties and is not a recognized medical specialty. The goal of the ASAM is to be recognized as the experts in addiction medicine with the consensus expert opinion based on the 12-step prohibitionist brain disease model. The ASAM has aligned itself with a number of inpatient drug treatment centers (Hazelden, Talbott, Marworth, Bradford,etc) and are heavily funded by the drug testing industry. It is in fact a “rigged game.”
State PHPs are non-profit non-governmental organizations and have been granted quasi-governmental immunity by most State legislatures from legal liability.
By infiltrating “impaired physician” programs they have established themselves in almost every state by joining, gaining power, and removing dissenters. Groupthink and 12-step indoctrination are the goals. By advertising as advocates for doctors who are “caring,” “confidential resources,” “giving help,” and advocating for “colleagues in need” the outward appearance is one of benevolence.
The biggest obstacle is that this system allows them to throw the normal rules of conduct under the imperative of a higher goal assumed to trump all other consideration. Those outside of programs either defend or ignore the reports of ethical and criminal violations, complacent in their trust of these “experts” claiming they are just helping sick doctors and protecting the public.
With no oversight or regulatory body involved this is all done with impunity, immunity, and undercover. They use the accusation of substance abuse as an indication to disregard the claims of the accused. The physician is left without rights, depersonalized, and dehumanized. The imposition of confinement, stigmatization, lack of oversight of the organizations, peer-review protected confidentiality, and lack of procedural protection is a one-way train to hopelessness and despair.
By establishing a system that of coercion, control, secrecy, and misinformation, the FSPHP is claiming an “80% success rate” 15and deeming the “PHP-blueprint” as “the new paradigm in addiction medicine treatment.
The ASAM/FSPHP had a major influence on the DSM-V where drug abuse and dependence are no longer separate entities. They are also working behind the scenes to get legislation to randomly drug test all physicians.
They are now after the “disruptive physician” and the evidentiary criteria are fairly low and red flags include “deviating from workplace norm in dress or conduct” and being tardy for meetings.
They have identified “the aging physician” as a potential problem because “as the population of physicians ages,””cognitive functioning” becomes “a more common threat to the quality of medical care.”
The majority of physicians are unaware that the Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment in 2011 that uses addiction as an example of a “potentially impairing illness.” According to the Federation of State Physician Health Programs …”physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years. This is a critically important distinction. Illness is the existence of a disease. Impairment is a functional classification and implies the inability of the person affected by disease to perform specific activities.”
“Process addiction” was added as a potentially impairing illness including compulsive gambling, compulsive spending, compulsive video gaming, and “workaholism.” According to the FSPHP “the presence of a process addiction can be problematic or even impairing in itself, and it can contribute to relapse of a physician in recovery. As such, process addictions should be identified and treated.” They define three levels of relapse including the novel “relapse without use.”
Bullying, Helplessness, Hopelessness and Despair
Perceived helplessness is significantly associated with suicide.16 So too is hopelessness, and the feeling that no matter what you do there is simply no way out17,18 Bullying is known to be a predominant trigger for adolescent suicide19-21 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.22
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.23,24 The “Cry of Pain” model 25,26 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life.
There is also evidence that rescue factors such as social supports may play a role in preventing suicide. These rescue factors act buffers to protect against suicide in the face of varying degrees of life stress.27,28 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 29 and support at work when difficulties arose appeared to be a protective factor for the male physicians.30 Research involving Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.31,32 Organizational justice is related to fairness and refers to an individuals perception of an organizations behaviors, decisions, and actions and how these influence one’s own attitudes and behaviors and has been identified as a psychosocial predictor of health and wellbeing3334 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.35,36
A recent report indicates that job stress, coupled with inadequate treatment for mental illness may play a role in physician suicide..
Using data from the National Violent Death Reporting System the investigators compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.1
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians.
They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity.
We have heard of numerous suicides due to these institutionally unjust programs. Three doctors died by suicide in Oklahoma in a one month period alone (August 2014). All three were being monitored by the Oklahoma PHP. I went to an all boys high-school of less than 350 students yet a classmate a couple years ahead of me died by suicide a few months ago. He was being monitored by the Washington PHP. His crime? A DUI in 2009–a one-off situational mistake that in all likelihood would never have recurred. But as is often the case with those ensnared by state PHPs he was forced to have a “re-assessment” as his five-year monitoring contract was coming to an end. These re-assessments are often precipitated by a positive Laboratory Developed Test (LDT) and state medical boards mandate these assessments can only be done at an out-of-state “PHP-approved” facility. Told he could no longer operate and was unsafe to practice medicine by the PHP and assessment center he then hanged himself. And at the conclusion of Dr. Pamela Wible’s haunting video below are listed just the known suicides of doctors; many were being monitored by their state PHPs–including the first name on the list– Dr. Gregory Miday.
None of these deaths were investigated. None were covered in the mainstream media. These are red flags that need to be acknowledged and addressed! This anecdotal evidence suggests the oft-used estimate of 400 suicides per year (an entire medical school class) is a vast underestimation of reality—extrapolating just the five deaths above to the entire population of US doctors suggests we are losing at least an entire medical school per year.
As physicians we need to demand transparency, oversight, regulation and auditing by outside groups. This is a public health emergency.
To wit:
They first came after the substance abusers and I did not speak out because I was not a substance abuser.
They then came for those with psychiatric diagnoses and I did not speak out because I was not diagnosed with a psychiatric disorder.
They then came after the “disruptive physician” and I did not speak out because I was not disruptive.
They then came after the aging physician and I did not speak out because I was young.
They then came after me and there was no one else to speak out for me.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res.1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ Health Programs. Journal of Medical Regulation. Mar 2010;95(4):10-25.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol and alcoholism.Sep-Oct 2004;39(5):445-449.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results.Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study. European addiction research.2014;20(3):137-142.
Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
Pham JC, Pronovost PJ, Skipper GE. Identification of physician impairment. JAMA : the journal of the American Medical Association. May 22 2013;309(20):2101-2102.
McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. Bmj. 2008;337:a2038.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis.2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors.Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
I get many e-mails, letters and phone calls from doctors, nurses and others who have been abused by “professional health programs” (PHPs).
Most are anonymous. Afraid of being identified and punished by the PHP, very few leave comments on my blog revealing their names or potentially identifiable information.
This is understandable. By simply reporting “noncompliance” to the medical boards a state PHP can end their careers. As it was with the Inquisition this system relies above all else on silence and secrecy. Speaking out can result in “swift and certain consequences.”
They are afraid. Some are undoubtedly suffering from PTSD. Most have developed a “learned-helplessness” Many have reported abuse and even crimes to their medical societies, medical boards, law enforcement, the media and others only to have the door slammed in their faces.-myself included.. They have no advocacy or support and feel no one cares. Their locus of control, identify and self-worth have been suddenly ripped from them without recourse. There is no lifeline.
PHPs are ostensibly Employee Assistance Programs (EAPs) for doctors in both mechanics and mentality. EAPs assist employees with substance abuse, personal problems and other issues. They do not diagnose or treat “patients” but refer to outside professionals who do. The critical difference between EAPs and PHPs is PHPs have mandated all assessment and treatment be done by their own. These “PHP-approved” facilities are economically and ideologically intertwined with the PHP. The conflicts of interest are serious and many.
PHPs also use non-FDA approved junk-science drug and alcohol testing they introduced. The procedural safeguards most EAPs use to protect the donor ( certified labs, FDA-approved validated tests, split-specimen, strict chain-of-custody, MRO review) have been reviewed. Unvalidated “personality” assessments they also introduces are being used in “disruptive” physician evaluations guaranteed to find “character defects” to justify monitoring contracts. They implement polygraphs despite the AMAs previous conclusion they are scientifically unsupportable.
But regulatory agencies have readily adopted policies not only unsupported by science and evidence-based research but outside the normative principles and practice of medicine.
Granting PHPs authority to limit assessments and treatment to their own facilities offends the fundamental rights of the individual.
Informed consent (or refusal) constitutes a basic rule of the lawfulness of medical practice according to national and state medical practice acts governing the profession. It is a basic principle of all published principles of medical ethics.
Involuntary treatment is motivated by either potential harm to others (for the good of society) or by need for treatment and/or potential self harm.
Involuntary treatment should be a confined to those gravely disabled by psychiatric disorders or substance abuse. It necessitates reflection under the ethical principles of autonomy and beneficence.
A single DUI, transient psychological issue such as grief or anxiety, and even sham peer-review can easily land a doctor into forced assessment and involuntary treatment at a “PHP-approved” facility.
Involuntary assessment and treatment involves legal, clinical ethical, and deontological consideration in its demarcation.
The economic and ideological aspects need to be considered here.
How is it this paradoxical assessment and treatment paradigm legitimized and justified within a profession that emphasizes evidenced based decision making and beneficence and autonomy as two of the basic principles of medical ethics?
To sell the “PHP Blueprint” to other EAPs it is necessary to prevent doctors from speaking the truth. Very few want their names, states or other unique identifiers published for fear of consequences and retaliation.
The letters below have only been posted after being approved by their authors-MLL
4/20/15
Dear Michael Langan
I love your writings analysing the power relations and psychopathy that is running rampant in every sphere of life, including sadly, medicine…
Your logo of the the two serpents represents the fight between good and evil, to me…
It was encouraging that you ‘liked’ the post from the blog as writing in relative isolation is very hard.
So thanks a bunch !
Take good care of yourself – truth tellers are precious and rarer than gold dust !
3/5/2015
Comment: I am Board Certified in Internal medicine. I have endured years of emotional, psychological and spiritual abuse at the hands of the Washington Physician’s Health Program. I have suffered through a long list of injustices without recourse. They include, but are not limited to discrimination, abuse of power, breach of contract and repeated and WILLFUL medical negligence.
Because the actions of the WPHP have been SO egregious, I assumed what was happening to me must be extraordinarily rare.
I have nothing to hide. And I have shared my story with any and all who would listen. To date, my voice, my rights and now my life have been dismissed as unimportant. MY LIFE!! It’s apparently better that I die than my tormentors be questioned and compelled to defend their indefensible and evil behavior.
I am meeting with one last attorney tomorrow. I fully expect him to ignore the basic, indisputable and well documented facts of my case. Namely, there is massive and systematic malfeasance being committed by a tax payer funded agency in the State of Washington who act with omnipotence and without oversight. I have no reason to believe he will respond any differently than the others with whom I have met. HE WON’T CARE! HE WILL NOT BE MOVED. He will make statements that suggest I DESERVE this treatment. And that my life, as well as my imminent death, is unworthy of his time or efforts.
Once my assumptions about this last meeting are officially confirmed, I am committed to the only course of action available to me. The only thing which will put an end to this nightmare.
Today I stumbled upon your website. And today, for the first time, I have learned that my case is not rare. I suspect the other physician victims in this matter have occasionally allowed themselves to dream wistfully of justice. Justice which they have seen thwarted at every turn. Perhaps they, like me, have dreamily imagined the relief and joy and LIFE they would experience if the truth were simply presented and the perpetrators held accountable. I have imagined standing up in court and triumphantly affecting justice for myself as well as all of the other current and future victims. I deliver a powerful defense of justice. My ‘dream speech’. I have imagined that I might still live. And then I wake up.
And so today, imagine my shock, when I found my ‘dream speech’ here. My speech. Reasonable. Honest. Consistent. And based firmly in truth, justice and defense of the powerless against the (arbitrarily) powerful. My speech, it seemed, but authored by another.
Thank you, Dr. Langan. You have given a voice to my struggles. Please never stop speaking for me, and people like me, many of whom, I fear, will not survive to see justice.
Despite my intention to die, I actually WANT TO LIVE! And I will live and fight on if I ever believe that there is even a small chance of justice for me and the other innocent victims of PHP’s and the ‘treatment’ centers with whom they contract (Talbott in my case. Purely evil and loathsome human beings, for the record).
So, because I do WANT to live…PLEASE HELP ME, SIR!
Can you refer me to attorneys, individuals or groups who might advocate for me and the other victims? Do you have any specific words of hope or encouragement?
Please note my name. Please add me to the list of innocent victims of these power hungry, narcissistic BULLIES.
I don’t expect to live through this. And in a way, the PHP, Talbott and the addiction ‘experts’ with whom I have been tragically acquainted are correct…My life is worth very little. But this issue is so much larger than I. I can die with some serenity if I believe there will be meaningful justice for others like me. And that those responsible will be held to account.
Thank you Dr. Langan. Thanks to all of those involved in the creation and maintenance of this website. Although your shining beacon is barely perceivable through the darkness of injustice which surrounds and seeks to extinguish it…it is the only glimmer of hope I have found during my slow death by PHP.
3/2/2015
Dr. Langan:
Thank you for your articles and research regarding PHPs and “impaired” physicians. I have become involved in this issue after someone close to me struggled with depression during residency. Sadly, they lacked the resources, support and coping skills and ended up committing a crime with a misdemeanor charge. Despite their treatment and rehabilitation, they were dismissed from residency. Not sure if they will ever get to practice clinical medicine. It is very sad. they are very smart, great doctor and very empathetic towards patients.
After their situation, I started looking on blogs and found that many residents had shared similar instances. Many reported struggling with depression and the stresses of residency put them over the edge– like the perfect storm of stress, fatigue, and loneliness that could exploit anyone’s weaknesses. It seems like during residency, we are emotionally as well as legally vulnerable. Many of these residents have never been able to resume training at their institutions despite their demonstration of clinical competence and emotional maturation. According to that medscape article, that is a huge loss to society, socially and financially.
Sadly, there still so much stigma surrounding mental health, and I think it may be worse in our profession.
I am very concerned regarding the future of our profession. We are becoming robots in a health care factory. Our own personal lives are being compromised as well as quality patient care.
I appreciate all you are doing to shed light on this very important issue.
Thank you for your time and consideration
2/17/2015
Dear Dr. Langan:
Thank you for your insight, eloquence, and concern for all of us. These Boards and other administrative bodies claim that they are “protecting the public,” but healthcare providers are the public too. And they’re killing us.
The problem is not unique to physicians. I am a nurse practitioner, and we share some of the same burdens. Although the numbers are growing, there are so few NPs nobody has studied suicidality among our profession. There is still the same fear of malpractice, professional bullying (nurses “eat their young,”) and the taboo of asking for help.
A trivial, third-party complaint to the State Board didn’t cost me my license, but it did cost me my job and my mental health. The pain I endured: the relentless questions about my personal life… it was jarringly intrusive. All of this was conducted by a bullying investigator: a man who had no medical training. The Board took it upon itself to ask detailed questions about my personal life and relationships, as if they would somehow psychoanalyze me. The investigator started his conversation by advising me that the Board does not honor the Fifth Amendment.
I’ve heard others—physicians—tell me of similarly murky complaints that dragged on. A cardiologist I know was instantly fired and rendered unemployable for year under similar circumstances. He struggled to feed his kids. Nobody died. Nobody got hurt. He didn’t have a substance abuse problem or divert drugs. He practiced within his scope. The case was eventually dismissed, and he’s back in business. But he has never totally recovered.
A simple, free email to the Board can cost a physician or nurse practitioner his or her livelihood in a split second.
All of this detracts from the dangers posed by inept or otherwise dangerous clinicians. We’ve all met them, seen them in practice, seen their charts, or heard stories. I think everyone I know can name a clinician who showed up drunk to work, billed fraudulently, or who was so incompetent that he or she should not be practicing.
It has been ten months. The Board hasn’t had any further questions, but they never dismissed the case, claiming that they have a massive backlog. My health and livelihood are inconsequential to them. I’m still being prescribed scheduled benzos and z-drugs just so I can make it day to day.
I came very close to suicide more than once, but I evaded psychiatric admission because then I’d lose my license without a doubt. Again, “protecting the public?” I deliberately avoided emergent medical care because of the Board.
I chose another path: I left the profession, and I have lost my sense of self. Twelve years of school, $350,000 in tuition, and four degrees were rendered worthless by a single third-party email. Above all, my pride in my clinical acumen, passion for learning, anal retentive charts, sensitivity, and professionalism also went down the drain.
The Board’s notion of “protecting the public” also means kicking good providers out of the business. Our emotional lives are destroyed, our finances wrecked, and we live in fear. There is no “speedy and public trial,” no “jury of our peers.” Although Conrad Murray MD fled to Trinidad, where he is working as a cardiologist (hopefully not prescribing propofol for insomnia), an open complaint renders me ineligible for licensure in all fifty states, all Canadian provinces, the Netherlands, and Australia.
Assuming that the Board dismisses the case, I don’t know if I could ever return to practice. It’s too hard to live in fear of a backstabbing patient or family member, and the ineptitude and glacial pace of a medical board. I want to clobber anyone who says, “and this too shall pass.” It’s not quite like that.
I am trying to re-establish myself in some second career, but that is hard to face. I cringe every time I open my email and mailbox in fear of a letter from the Board. I know I did nothing wrong, but that’s not how the system works.
I still fight the urge to take my own life.
1/17/2015
Great website. Presents an alternate view I have never seen in action and I have had to report a number of MDs to our state’s PHP. Thanks for the insights.
2/8/2015
I am an RN in a monitored program in PA which includes forced AA attendance. I have 22 years as an RN with 10 years of military service which includes a one year deployment to Iraq. I am willing to speak out. Too many are afraid of losing their licenses to practice.
1/14/2015
A review of 14 studies found that the relative risk of suicide in physicians compared with the general population is between 1.1 and 3.4 for men and 2.5 to 5.7 for women, http://www.currentpsychiatry.com/index.php?id=22661&tx_ttnews[tt_news]=175910, furthermore, studies have indicated higher rates of suicide among psychiatrists and anesthesiologists.
There are a variety of theories on why physicians commit suicide. Depression is the most common explanation given. Certainly, there’s a lot of stress involved in our profession. We deal with death and dying. We’re held to impossible standards. Managed/mangled care and the restrictions of government plans/laws/policies on the one hand restrict what we can do for our patients. On the other hand however, are the viscous packs of attorneys waiting to cull the herd. Let’s not forget the State Medical Boards, out there striving to “protect the patients”, generally done in cahoots with the “Physicians Health Programs”. These two entities form a deadly collusion that is inescapable—and of course, linked to the packs of predators circling to ensure that we will suffer the consequences for actions that we may have little if any control over.
I am one of the unfortunates.
I haven’t committed suicide (obviously), nor made an attempt at it. Certainly I’ve had thoughts about it—who among us hasn’t? My strong religious convictions prevent any serious consideration of this “permanent solution to a temporary problem”.
I am also one of the fortunates.
This is largely due to the foundation of faith that I have. Years ago I made what may have been a mistake. I prayed for patience & humility. We tend to be an impatient and yes, at times an arrogant lot. I recognized those character flaws in myself and asked Him for help.
I should have asked for the grace to overcome these shortcomings. Grace is a gift, a “freebie” if you will.
Patience is gained through trials. Humility generally through humiliation.
I have learned that where there is pain in life, there is often a lesson—look for it, learn from it. Running from it merely guarantees that it’ll be presented again, and again and again until it’s learned, often with a few extra presentations after the initial effort to dodge the trial.
The study of theology has lead to the interesting concept that suicide is actually a sin of pride. Yes, depression is involved, but the pride plays it’s role with the thought that; “I don’t deserve this trial so I’m choosing to take myself out of the game”.
My personal belief is that only God has the power to give and take life. The reader is certainly entitled to their own belief. Mine has evolved by study and prayer over decades.
There is a growing movement afoot across all 50 states for attorneys employed by State Medical Boards to direct their investigators to report possible transgressions directly to the attorneys instead of to the physician board members http://woundedhealersnc.net/. The attorneys have thus usurped the role of a professional board; to ensure that we’re held accountable by our peers. These attorneys then draft their own perspective of what happened, often putting “spin” or “slant” to the report to prejudice the board members to carry out the actions that these attorneys deem to be appropriate. The Board Members have unwittingly abdicated their responsibilities. This leaves physicians at the mercy of Board attorneys. These attorneys were initially tasked with ensuring that the Board members didn’t violate any laws in their disciplinary actions against wayward licensees. Board members are busy physicians in their own rights. They have their practices and with the attendant problems associated with them, as do the rest of us. Typically, they go to their state capital for a couple of days a month to do their “official duties”. The attorneys present the information for the “rubber stamp” of the Board’s approval.
Worse still are the “consent orders” drafted by the State Board attorneys. A key part of such an order is the “findings of fact” describing the (alleged) transgressions. The hapless licensee is often coerced to signing these flagrantly fictitious documents with threats that the attorney-derived discipline will be much lighter than what the Board will mete out. It’s actually not uncommon for “defense” attorneys to collude with the Board attorneys, urging the clients that they are supposed to be defending into signing the consent order. Signing the order will have many grave consequences http://woundedhealersnc.net/documents/lip/index.htm. As a hapless victim, I had no concept of such unethical yet commonplace activities.
There is documentation of an extremely arbitrary nature of punishments on www.woundedhealersnc.net ; A physician and his mid-level go out to a dinner presentation by the local pharmaceutical representative. Driving home afterwards, the physician crashes the vehicle. Both are intoxicated. The mid-level spends 2 weeks recuperating in the hospital. The physician/driver gets a “Public Letter of Concern”.
Another physician is out of state on vacation, gets a DUI, truthfully reports it during his annual license renewal and is taken out of practice for four years. Some practitioners NEVER return to practice. Substance abuse issues are treated extremely harshly.
Killed somebody with negligence? Oh, no problem, that will only get you a “Public Letter of Concern” in North Carolina.
You were seduced by a patient? Big problem! There’s to much of a “power imbalance” since you’re a medical practitioner, mid-level or otherwise. You may possibly NEVER practice medicine again. There’s documentation of a psychiatrist who married a patient, the State Board found out about it and took her license away; she was to much of a risk for sexually assaulting other patients. Ultimately she was allowed to have her license back on the condition that she never practice psychiatry again!
I was also unaware that state boards are incentivized to discipline as many physicians as possible, as harshly as possible, for as long as possible.
I was indeed one of the innocents.
Knowledge is indisputably power. The site quoted above provides a wealth of information of the workings of the “system” in North Carolina. The “Great North State” is hardly alone in their approach.
The Physician Health Programs (PHP’s) are another area of concern. It’s a shame that the stated purpose of the PHP’s is to help return impaired practitioners to active practice. These groups throw the very physicians who need help the most the furthest under the bus in full collusion with the Board. They’re typically staffed by psychiatrists who are members of “addiction societies” that aren’t much more than diploma mills. The PHP’s often claim to be performing “peer review” while disregarding the legal requirements for peer review. The PHP’s/Medical Societies/State Boards are parasitic symbionts that prey upon those of us who have been used up and burnt out by the non-system of healthcare that exists.
Does this sound like a pattern is developing? “Disregarding the legal requirements…”
In North Carolina, the complaints were of such a volume that the NCPHP was audited and found to have numerous deficiencies. Next, all 57 of their licensing and professional boards were audited. All of them showed problems—the most common that they did not report to anybody for supervision! These are routine violations of the General Statutes of the state.
Every state has a state auditor whose function is to ensure that state agencies fulfill their assigned duties efficiently and honestly. Most State Medical Boards and PHP’s have NEVER been audited. Anybody can report their concerns to their state auditor.
Attorneys are supposed to uphold the law; isn’t this ironic?
There is ample evidence of collusion among the players; Defense attorneys who should be defending their clients against their Board (sometimes the Boards actually recommend individual attorneys that they “work well together” with to wayward licensees). Board Attorneys are clearly involved as are the PHP’s.
State Medical Societies are also generally in the same bed with the Boards & PHP’s. Governor’s generally rely on the Societies to recommend prospective Board members. It’s not uncommon for the first question at an “investigative hearing” to request information on whether the licensee is a member of the local state society. What would the purpose of such a question be? Simple. It’s well-documented that membership has a “protective” function. It’s not absolute, but exists nonetheless.
In one case, the Board remanded a full mental health evaluation. The result was that the licensee had a mild autism spectrum syndrome (something a good many of us have), an autism spectrum disorder that is characterized by difficulties with social skills and non-verbal communication—but with benefits such as intense interest and expertise in certain areas (like medicine!).
The function of a Board is to maintain scope of practice. Family physicians don’t do craniotomies. Yet, despite the absence of a single mental health professional on the Board, the recommendations of 3 independent professional organizations, all recommending immediate return to practice for the licensee were ignored.
The Board posted the practitioners protected health information, including mental health information on their website. The most basic rights to privacy were clearly violated. The licensee never gave permission for such an intrusion!
The ADA covered disability was dealt with by an indefinite suspension—all with the full collusion of the NCPHP. The ADA requires “reasonable accommodations”. Indefinite suspension is punitive—certainly not a reasonable accommodation! Again, it cannot be over-emphasized that Board attorneys have a strong desire to punish whenever, wherever, for as long as possible.
The licensee signed the contract with the NCPHP. The licensee was held to the terms, but the advocacy mandated by the contract was never delivered; “the Board attorney said he wasn’t interested in anything I have to say in your favor, his mind is made up, there’s nothing I can do to help…” was the limit of advocacy received.
Advocacy?
Collusion is a more accurate description.
The theme song from the hit movie and TV show M*A*S*H* is “Suicide is Painless” by Johnny Mandell. This epidemic is more of an endemic among our profession. We can’t keep “looking the other way”.
There are two major forms of suicide.
Active suicide would best be described as a former colleague who went into the recovery room one Sunday afternoon when it was deserted, took a scalpel and did a full-length carotidotomy on himself. He made a posthumous statement. Another ran out in front of a box truck on the interstate. It took his head off.
Passive suicide is best shown by 5 of the NC Medical Board victims. This Board tends to pursue physicians from their mid-40’s to mid-60’s, the top income-producing time of our careers. They usually have assets to poach. Usually by that age, we’re taking some form of medications for our own health issues. A diabetic who purposely forgoes his insulin… Suicide? It won’t be reported as such. What do YOU think?
We will never eliminate all of our stressors. There will always be the “less fit members of the herd”, which is sad. This is more appropriate for other animals at other positions on the evolutionary tree. Why should the most noble of professions be relegated to those branches of that tree?
We need to reach out to each other. We need to reach out to our state auditors. Another resource that surprised me is a different agency. There is an agency whose primary function is “to deal with corruption in public officials both appointed and elected”.
Does this sound like an appropriate agency to engage against our Boards & PHP’s? It’s the Federal Bureau of Investigation, commonly known as the FBI!
All that it takes for evil to triumph is for good men to do nothing. When we organize we change from individual targets to a formidable force. State Medical Societies, unfortunately, are not the answer. Typically state governor’s turn to them for nominations to staff the boards. In North Carolina, lawsuits have been settled out of court that involve the alliance between the Board, Medical Society & PHP.
Perhaps the best solution would be to revamp the system. Maybe it’s time for a Federal Medical Board. At the very least, State Boards should be restructured so that investigators do not report to the attorneys, but directly to the Board Members. It will mean more work for the Boards, but they’ll at least resume functioning in the manner originally intended.
–Wounded Healer
12/31/2014
This whole lack of accountability and oversight within the PHP’s makes me sick. I was sent to PHP for evaluation and suspicion of drug abuse by my employer hospital. I was only suffering from side effects of Paxil causing a SSRI Discontinuation Syndrome. The diagnosis was completely missed because the PHP sent me to a rehab center in Los Angeles. I am sure you know this one very well.
I was coming there for IDE, Intensive Diagnostic Evaluation not recovery and rehab. After arrival I was forced to enter their rehab program completely against my will. I was on my way out the door and about to call a cab when the program director threatened me with absolute coercion.
He said if I left he would assume I had drugs in my possession and that this would negatively affect my evaluation and would be reported to the PHP and state medical board as a form of noncompliance, and that my career and license would be in jeopardy. How is that possible when I was not sent there by any state board or regulatory agency as I was there voluntarily.
The only incentive to force me into admission rather than having my workup done as an outpatient was purely financial. Employer was paying the bill, so it was in their best financial interest to force me into admission at $1800/day and $1400/urine sample and charge for all the transportation to and from all the outsourced facilities for my “evaluation”.
The facility was run by the most inept, unethical group of charlatans I have ever encountered in any field of service not just healthcare. I could not understand how they were qualified to provide medical evaluations when they are not legally allowed to provide any form of treatment for anything. These people were nothing more than middle-management screw ups. They have to outsource everything. They did not even have a crash cart on site. One of their clients had a tonic-clonic seizure during group therapy as a result of a brilliant PA who decided to withhold the clients chronic benzodiazepine therapy because of her personal beliefs that benzos are horrible medications for anyone. Where is the physician co-signature and oversight on this brilliant therapeutic decision? No one except the doctors in rehab even knew how to react. It was a total fiasco and state of panic for all the rehab employees. Luckily the client didn’t dislocate something, die or worse, suffer anoxic encephalopathy. I was in fear for my life after witnessing this my first day.
What’s even more concerning is that this rehab center is supposedly one of the best and has exclusive referral from every state PHP.
They had me stay with recidivist junkies and participate in 12 step when I had no substance abuse issues at all, in fact my social life was so boring, that my hair test wasn’t even positive for alcohol. I had to recite scriptures in group therapy, admit that I was helpless, and powerless, and a weakling. Admit that I had to submit to a higher power since I was an addict. I had to submit to random urine drug tests which costs $1400 each 3-5 times per week.
Then when I cannot produce a sample on the spot (paruresis) I am threatened to be reported to the State Medical Board for noncompliance. A college dropout working as a technician at a rehab does not even have the authority to make this type of threat. I was also forced to shave in front of a female technician with the bathroom door open; she stated that this was policy and I had to relinquish my razor after every shave because I could use it to inflict harm on myself. I then asked why is there a whole drawer full of sharp cutlery in the kitchen that me and my junkie roommates have access to 24/7???
I saw a psychiatrist and handed him my diagnosis on a silver platter from my history , i.e. Paxil withdrawal yet SSRI Discontinuation Syndrome was not even on his differential. I was in a state of constant agitation, sleep deprivation from insomnia, severe depersonalization. Ended up in the ER at UCLA for intractable Migraine HA, Sleep deprivation, Dehydration, mild AKI and had to be medicated with IV crystalloid, Phenergan to combat emesis and finally induce sleep (going on 4th day of insomnia at that point).
Less than 24 hours after the ER visit I am sent for Neuropsychological testing extensively, which violated just about every code of conduct and ethics under the American Psychological Association in regards to testing validity. I was then labeled “disabled” based on the results. the treatment center was then going to recommend that I stay and additional extended period so they could “rehabilitate” me. They realized now that they did not have my credit card on file because I refused to provide them with it at admission as my employer, was paying for everything for the first month. Next they discover that I do not have disability insurance, and now know that they have just ruined my life. It will take a minimum of 6 months before I can be retested to prove that I have no cognitive impairment and am not disabled. Now my chances of getting disability insurance in the future are ruined.
The treatment center then released me and I returned home to the PHP. I then had to sign a five year contract, enlist in a drug monitoring contact with “RecoveryTrek” which I had to perjure myself and illegally claim that I was a substance abuser and was in “recovery.” I immediately sought legal counsel because of this nonsense. Shortly into my so called recovery I had to take my Maintenance of Certification Board Exam in Internal Medicine. Passed exceptionally and with ease. How could I be cognitively impaired?
Go figure! The neuropsychological test was readministered locally by a different provider as I told the PHP there was no way I would ever consent to going back to the treatment center. The neuropsychologist was pretty pissed off about everyone’s mismanagement of my case starting with my employer. I tested fine, and then the PHP released me from the program and cleared me to return to work. The entire experience has jaded my enthusiasm in medicine. I had to take almost a year off to reflect on how I was used as a pawn in everyone’s game.
I experienced coercion, collusion, fraud, incompetence, and saw a part of evil in this world that I never new existed. I was a prisoner, starting my day by having to call a monitoring center to see if I had to be drug tested for that day, every day of the week. I was not allowed to leave the state; how can a PHP legally restrict my civil rights this way when I was not under a court order, and not even under state medical board referral? I was not allowed to have a sip of alcohol during my monitoring, even though I had tested negative for any evidence of drug use. I had to meet with board of directors every month and discuss my case, which no one had clue about regarding why I was even in a PHP. This violated all of my rights to privacy regarding my medical condition. The contract that I initially had to sign with the PHP had statements within claiming they could report any information about me to any regulatory agency without even substantiating any facts or validity. This is just a clever way of saying they can lie about you and there is nothing you can do about it legally. There is complete lack of due process. Your civil rights are stripped. You are beaten down into despair and desperation. You are told if you don’t comply your license would be in jeopardy and your career will be over. This cost me thousands of dollars in legal fees, thousands of dollars to be retested and prove I was not impaired, hundreds of dollars each month for PHP dues and random urine drug screening.
I put up with this B.S. for six months, and honestly could not have fulfilled a 5 year contract. If I had not been released (since there was no condition to monitor) I would probably be dead today. I would not be surprised that PHPs have actually caused in increase in physician suicide rate. I cannot fathom the degree of humility physicians experience having to do this for five years. And the only reason these rehab centers claim such a high success rate for recovery is that they hold a gun to your head and threaten you to be in compliance with everything they recommend. So yeah, doctors have a lot more to lose. I now understand how these PHP’s are in collusion with rehab centers. What they are doing is a violation of fair trade acts and would fall under the RICO act. The problem is nobody is investigating them for conspiracy and fraud. They all fly under the radar because they believe they are providing a service that ensures public safety. Its a multi-billion dollar scam industry. What’s more sad is that nobody really cares what physicians are subjected to. In fact the public likely finds joy in fact that docs are treated this way. The state of California hates doctors, so the rest of the country probably does too. People probably enjoy knowing doctors are held to higher standards than the rest. That they are usually required to stay 90 days in rehab while all other professionals stay 28 days, that they are financially ruined by rehab centers. That they have been stripped of all their rights while in a PHP monitoring program. That they are more subject to discrimination based on age or coexisting medical problems like diabetes and hypertension. I have actually seen cases of MDs sent to PHPs for monitoring of hypertension and regardless of why you are sent there you must comply with drug monitoring.
The rehab centers are now tapping into other territory that further identify this as a conspiracy. Department of Transportation, Aviation, and Law Enforcement are going to be their next victims. I can’t wait to see how the police officers are going to respond to this nonsense.
This was an eye opening experience. There is no profession that is worth going through this amount of humility. PHP’s will likely remain above the law, continue to have no accountability and oversight, which is a travesty of justice. I hope you will share my experience. My case is rather unique in my opinion. It’s evidence that no physician should ever voluntarily enter a PHP at an employer’s request. You would be much better off to simply quit/resign.
12/27/2014
I know of pharmacist who are forced into the program and held hostage by their license. They are also required to do “inpatient” treatments of at least three months and continued random monitoring for five years as well.
Once they have you by the proverbial ball, they milk you till you are dry. It is nothing but a scam. The funny thing is that for healthcare professionals who relapse while in the program, they are sent back to “rehab”(inpatient) again once more for milking while they feed you the same b.s. they did the first time.
What is becoming even more alarming is that at least in one case, Texas, if you call PHP for help or to inquire about help, even though nothing has been reported at work or to the board, and you identify yourself and spill your guts about your issue/s asking for your options you are automatically signing up for a trip to rehab and five years of monitoring.
If you decided that you are not interested what they have to offer, they will tell you they would report you to the board at that stage (of course at the beginning of the conversation they tell you it is confidential, but it is confidential as long as you voluntarily start their program since you spilled the beans.
I would be very careful calling the state PHPs asking for information. I would do it from a blocked phone and use an alias before talking to them.
Maybe others who information about other states can also shed some light on this.
12/7/2014
It is really tragic that so many valuable doctors are lost without reason. That State Medical Boards can strip a physician of his hard earned license without due process. That there is no oversite of these boards. That boards and PHPs bully and harass physicians, even to the point of suicide. About 400 physician commit suicide every year. That’s a loss of an entire medical school every year! A colleague of mine committed suicide after facing medical board charges that had no signifigance anyway. This is occurring in the face of a physician shortage as baby boomers age.
12/30/2014
Turns out, I am one of those recovering alcoholics (9+ years) with a lot of experience in AA. It was a large part, though not all, of my treatment. I found it personally helped me a lot. And I also agree with your position.
Based on my experience in AA, things I heard at AA meetings and things I read in AA literature:
– the AA message should be spread via “attraction, rather than promotion”
– AA does not claim to be any kind monopoly in the field of addiction treatment
– AA is fully self-supporting, declining outside contributions
– AA is not professional and not organized
And so having a large body of physicians outside of AA promoting AA is, in my opinion, contrary to multiple AA traditions – particularly if this situation creates controversy. I personally find AA needs no extra promotion, and alternative treatment programs ought to be encouraged just as well as further scientific research into the addiction problem.
The whole thing was meant as a very open, welcoming, non-judgemental, informal gathering of alcoholics talking to each other. Extremism, government coercion, public promotion, money – all those things do a lot more harm than good.
At any rate, thanks for your thoughts, Dr. Langan. Best of luck in the future, I’ll keep following along.
12/25/2014
As an airline pilot who made the monumental mistake of believing that the “E” in EAP (Employee Assistance Program) really meant “assistance”, I can only nod my head in sad agreement to everything above. Between “treatment” (indoctrination in AA dogma) and monitoring my decision to ask for assistance in dealing with a series of health and personal issues that I (for the first and so far only time in my life) tried to use alcohol to numb has changed my life forever. I have lost 7 years of my life. My faith in the rule of law in our society is completely gone. The stress and humiliation of having my career depend on my ability to convince people in this program that I have been “converted” (let’s call it what it is: living a lie) have been indescribably painful. It has affected every aspect of my life. My physical and mental health has suffered as has my personal relationships. My only hope is that court decisions like the recent one in the Hazle trial will once and for all end this damaging and unconstitutional practice.
12/1/2014
Comment: Excellent research. What is astounding is that some (if not all) PHPs are using EtGs and EtSs and PEths DESPITE explicit advisories by SAMHSA over a span of 6 years! These advisories noted that a) they were not FDA approved; b) there was insufficient research; c) that there were too many false positives; and d) using such tests in such a setting as the forensic environment where someone’s career and reputation could be put at risk was highly dangerous. Further, as I discovered only recently, NCPHP not only runs these tests on new evaluations it conducts on involuntary (and unsuspecting) physicians who have been ordered (under specious circumstances) to be evaluated by NCPHP, NCPHP adamantly refused to release the results of the tests to the physician, though you can be assured the results were used to “make their case” for a pre-determined diagnosis.
I think it is fair to say that their use of these tests is not simply unethical; it constitutes highly risky human experimentation conducted with neither the subject’s consent nor with approval of an IRB.
One can also presume that PHPs have sold this junk science to their associated medical boards in giving them what appears to be substantial evidence to bolster their case. And one can also presume that medical boards have simply accepted it as though it were valid, essentially doing nothing to challenge the invalidity of the test and the violation of due process and thus virtually rubber-stamping the annihilation of a physician’s career.
When you engage these research epidemiologists in this endeavor (is there yet a group called “Epidemiologists for Social Responsibility?”), you may also ask them to review data form board and PHP actions in which this data was – in any way – involved in the assessment of their case, whether playing a major role or only an incidental one. The introduction of this misleading – and therefore fraudulent – laboratory data into these physicians’ adjudication would seem to serve as a solid basis for invalidating their fraudulent assessment and ensuing “conviction.”
Personally, I believe this is of such immense importance that it ranks up there with the flawed hair and fiber analysis assessments that were done by the FBI which my courageous colleague Dr. Fred Whitehurst called attention to in the late ’90’s (and lost his job over, via a massive campaign of discrediting and innuendo of “mental illness.”) It took nearly 15 years but finally, the DOJ saw the immensity and breadth of the false prosecution based on flawed “evidence” and ordered the FBI to reopen over 21,000 cases of potentially flawed hair and fiber analysis!
I truly believe the same outcome is going to materialize here – it has to! Physicians (and soon many other seemingly well-paid professionals who are judged able to afford the “private addictions treatment for professionals” scam) have been falsely assessed and compelled into costly (and embarrassing) treatment programs and prolonged monitoring (with extra time for balking – i.e. “being disruptive”) by the PHP prison-industrial complex. All with no chance of fair hearing, no chance to challenge the validity of the evidence, and high likelihood of reprisal if one doesn’t “go along.” This pervasive abuse of authority and process must be aggressively confronted.
11/27/2014
Great site! There is so much corruption in medical boards & PHP’s. We need to take it upon ourselves to evaluate what our agencies are doing and turn them into the state auditor of every sight for performance and forensic auditing. Auditors DO listen and DO investigate, but they need to be led to the need for an audit. The best way to do this is for those of us who have been assaulted and battered by these agencies to document what has been done to ourselves and our peers and let the auditors know what is going on!
11/22/2014
I have enjoyed reading your web log. I have empathy for your plight. I am involved in a parallel organization known as the HIMS program (Human Intervention and Motivational Study)
I can’t help but notice that several of the names you have listed under ‘like-minded docs’, are ‘professionals’ I have also encountered. Namely, Joe Garbely who did my initial psychiatric evaluation, Lynn Hankes, a urologist who advises HIMS and the FAA, and William Green, my current psychiatrist. I am told a component of my $1500 dollar meeting with Dr Green (Physical and Psychiatric) will be composed of inquisitions into my involvement in Alcoholics Anonymous and progress in my step work. This is the man who told me I must attend three AA meetings weekly and my aftercare group therapy must involve AA in order to be approved for FAA Special Issuance (the FAA Gold Standard). I was also informed that non compliance would mean a rejection of my application by the Feds. All of this after I informed Dr. Green that there simply was ‘no correlation’ between Alcoholics Anonymous involvement and my sobriety and that I found the program to be psychologically harmful to my well being.
If you have any further information on the three ‘like-minded docs’ I have encountered in my journey kindly point this out to me. I am sure there are more but I must thank you for providing the missing pieces of the puzzle from the medical perspective. Its eye opening to say the least. Have you spoken with the same attorneys the pilots have? I am sympathetic with your plight. The worst mistake I ever made was asking for help and the process of psychological hazing, indoctrination, and coercion did nothing but steepen my situational depression.
Jonathan
Thank you for your earnest work on this subject. We are not alone in this.


























 Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.”
Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.” 















 In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG. They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
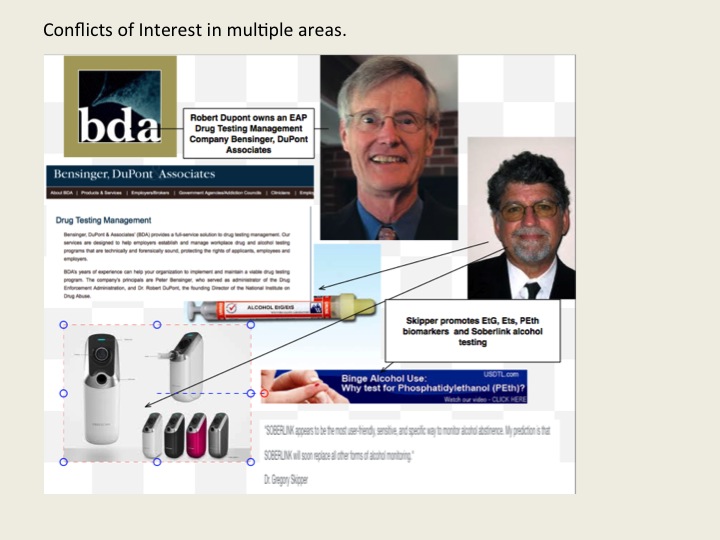




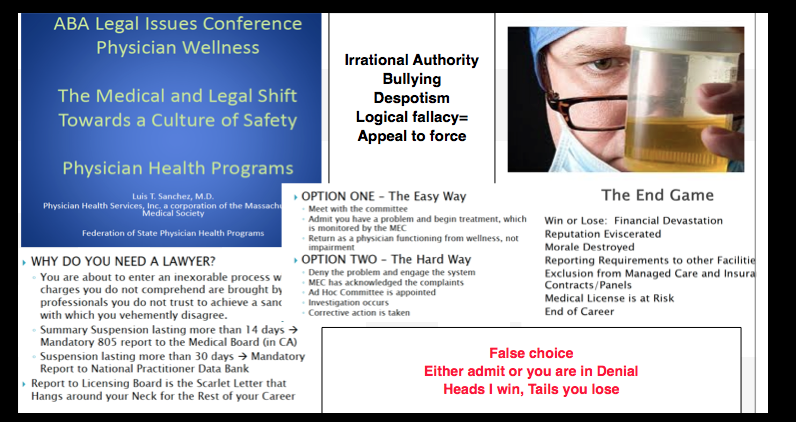



 I get many e-mails, letters and phone calls from doctors, nurses and others who have been abused by “professional health programs” (PHPs).
I get many e-mails, letters and phone calls from doctors, nurses and others who have been abused by “professional health programs” (PHPs).

Be the first to comment and start the conversation!