Anonymous referrals to state PHPs can result in loss of careers, families and even lives. I have heard from doctors targeted due to age , religion, sexual preference , nationality, political stance and appearance. Referred to the state PHP with an anonymous complaint of “alcohol on breath” or “anger issues,” these good doctors were removed from practice under the guise of protecting the public. By claiming a doctor has a “potentially impairing illness” and falsely labelling him or her with a substance use or behavioral disorder they are able to remove due process and remove any doctor from practice. The system is designed to give the appearance of legitimacy. It is not. The stories I have heard and continue to hear from doctors and medical students are as horrific as they are heartbreaking. I have heard from female doctors who refused to go out on a date with, spurned sexual advances and even been raped by other doctors who then reported them to their state PHP for damage control. I have heard from many doctors who discovered misconduct such as insurance or Medicare fraud who were promptly reported to their PHP and doctors who were reported by competitors for patients. I have heard from doctors reported out of jealousy, anger, racism and bigotry. Some of these storied can be seen on who have thwarted sexual advances and even been raped who were reported to their state “letters from those abused and afraid
My work in physician health reform has resulted in some significant gains. For example the Medscape article Physician Health Programs- More Harm Than Good? by Pauline Anderson was the result of Medscape Editor taking an interest in my tweets about a year earlier and contacting me and taking an interest in my blog. Physician Health Programs- More Harm Than Good? broke new ground as it was the first mainstream medical article critical of PHPs. This was read by British Medical Journal Editor Jeanne Lenzer and this led to “Physician health programs under fire.” In this article published in the BMJ she takes on the financial conflicts of interest, abuse and fraud in PHPs and the FSPHP’s response to direct and specific questions revealed what an irrational and illegitimate authority they are. They cannot provide direct and simple answers to direct and simple questions and remain tongue tied to this day.
By all counts their days are numbered and the articles mentioned above and more to come are the direct result of bottom-up activism. So too is a forthcoming audit by Massachusetts state Auditor Suzanne Bump whose office has already interviewed enough abused doctors to warrant an investigation which will hopefully look into the misconduct and fraud being perpetrated by the Massachusetts PHP in collusion with a specific group of attorneys within the medical board that blocks due process and conceals evidence to protect the PHP and harm innocent doctors.
It took 25 years for the FSPHP to rise. Let’s hope their demise is much quicker. They need to be named as the enemy and addressed on a state by state basis. We have dealt some significant blows and I would like to keep throwing some direct punches to the enemy but at this point it is getting difficult due to financial matters and I urgently need funding and support.
The need for allies and funding is urgent as time is critical. We have to expose this group as an illegitimate and irrational authority, expose their fraud and scams and expose the backgrounds of some of the individuals involved. Physician health programs should not longer be considered the elephant in the room. All you have to do is look at documentary facts and evidence to see what is happening and any ignorance at this point would have to be deemed willful ignorance. You cannot continue to ignore the obvious. To those within the PHPs and their sympathizers and apologists your silence speaks volumes To save American Medicine it is essential this be exposed, investigated and the perps held accountable. Silence is no longer an option.
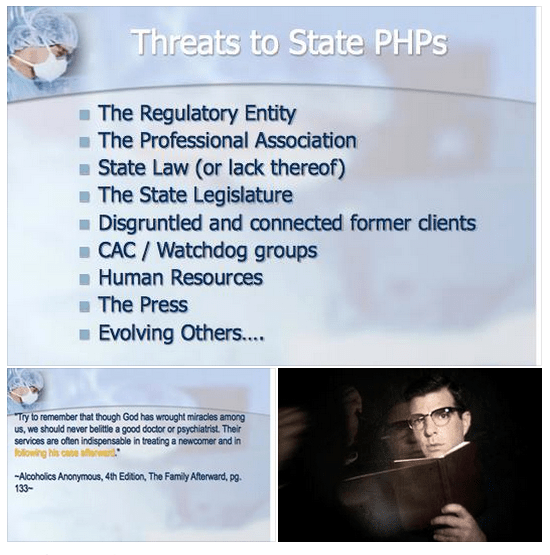
The blue slides below are from a presentation at the 2014 FSPHP spring meeting in Denver, Colorado and can be seen here. The presentation was given by past FSPHP Presidents Gary Carr, MD and Warren Prendergast, MD, West Virginia PHP Director Brad Hall, MD and Montana PHP Director Mike Ramirez, MS.
This needs to be seen as a “to-do” list.
A.A. = ASAM = FSPHP
The quote is from Alcoholics Anonymous and the full passage is as follows:
“We are convinced that a spiritual mode of living is a most powerful health restorative. We, who have recovered from serious drinking, are miracles of mental health. But we have seen remarkable transformations in our bodies. Hardly one of our crowd now shows any mark of dissipation. But this does not mean that we disregard human health measures. God has abundantly supplied this world with fine doctors, psychologists, and practitioners of various kinds. Do not hesitate to take your health problems to such persons. Most of them give freely of themselves, that their fellows may enjoy sound minds and bodies. Try to remember that though God has wrought miracles among us, we should never belittle a good doctor or psychiatrist. Their services are often indispensable in treating a newcomer and in following his case afterward.”–Alcoholics Anonymous, 4th Edition, The Family Afterward
Federation of State Physician Health Program (FSPHP) physicians often quote A.A. because they are defined by A.A. in both mechanics and mentality. The “impaired physician” movement began with evangelical recovered addict and alcoholic physicians whose recovery was based on 12- step spirituality. As this group molded into the American Society of Addiction Medicine (ASAM) many of them found employment at 12-step rehabilitation facilities and others joined their state Physician Health Programs and organized under the FSPHP. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insiders knowledge of recovery as brandished in this A.A. passage which I find condescending toward the medical profession and oddly narcissistic.
This special knowledge, of course, was based on the chronic relapsing brain disease model with lifelong abstinence and participation in 12-step recovery.
These “miracles of mental health” joined their state PHPs and those who did not agree with their rigid inflexible views were removed. Those with access to special secret knowledge were eventually able to outvote those with intelligence and open minds as this groupthink infested and eventually monopolized PHPs.
It is important to understand that the ideology of A.A. is the ideology of the ASAM is the ideology of the FSPHP
Like all “front-groups” the ASAM purports to serve one agenda while in reality serving another. The ASAM claims to be a “physician society with a focus on addiction and its treatment” According to their website their mission is to
increase access to and improve the quality of addiction treatment;
to educate physicians (including medical and osteopathic students), other health care providers and the public;
to support research and prevention;
to promote the appropriate role of the physician in the care of patients with addiction;
and to establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers and consumers of health care services, and the general public
In order to accomplish this the American Board of Addiction Medicine certifies doctors to “provide assurance to the American public that Addiction Medicine physicians have the knowledge and skills to prevent, recognize and treat addiction.”
Ostensibly these are laudable goals that are almost universally endorsed. The perceived organizational purpose and public persona are altruistic and humanitarian. Treating addiction not only saves individual lives but improves the community. It is for the common good.
Abuse Hidden Under Benevolence and Torture as Treatment
History reveals that all manner of abuse can lie underneath a patina of benevolence. In the past few months alone we have both Bill Cosby and the British Parliamentary pedophile ring as prototypical examples. Both cases reveal a decades long coverup of allegations in which the abusers escaped little or no investigation into their alleged crimes. Abuse of power with a large gap between the power of the abuser and the powerlessness of the abused is a common denominator. If the abuser endorses our own beliefs systems it creates a discord that promotes disbelief. It does not fit. Accusations are dismissed, deflected or otherwise suppressed. Power effectively extinguishes the truth. Disbelieved and delegitimized, information is suppressed, charges are not filed and law enforcement and the media turn a blinkered eye for decades. Indifference, disbelief, rationalization and cognitive dissonance prevent exposure and accountability. Hidden in plain site the truth was there and easy to find. The problem was no one was looking. Most did not want to look.
It does not take much sleuthing to uncover what is beneath the veil of the American Society of Addiction Medicine. The history, mentality and mechanics are well documented and reveal where they came from, how they evolved and what they have planned. It is a complicated web and hard to explain but once the pieces of the puzzle are fit together it is clear. But it involves assembling a complex puzzle by finding the individual pieces scattered in disparate areas including the regulatory, clinical, administrative and professional niches of the medical profession, Alcoholics Anonymous and 12-step related organization, public policy, all levels of the political arena and other areas. Once put together the portrait is clear.
In reality the ASAM is a political action group or special interest group that is designed to cement the chronic relapsing brain disease model with lifelong abstinence and spiritual recovery as the one and only treatment for addiction. A.A. is used as the energy source of the operation. By labeling addiction a “disease” requiring “treatment” in which someone is helpless they are able to dictate all aspects by coercion and control. But in my opinion the A.A. ideology is just used as a ruse to support the multi-billion dollar drug and alcohol testing, assessment and treatment industry. The zero-tolerance mindset of the “treaters” combined with the “helplessness” of the diseased enables them to erect a revolving door of testing, assessment and treatment that provides them with both control and a steady stream of money.
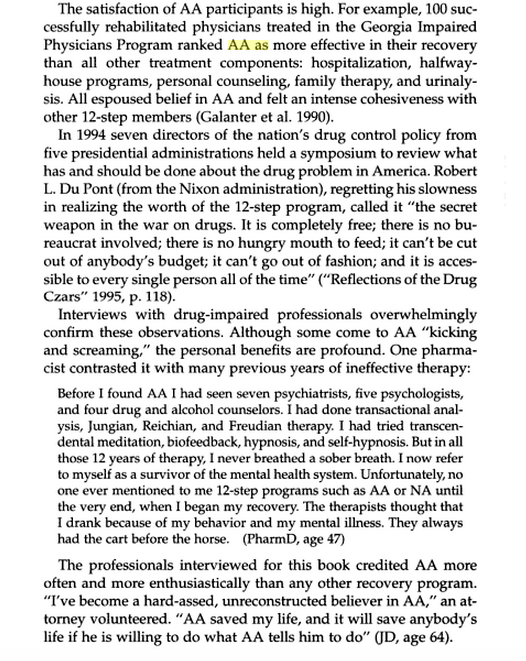
The FSPHP mandates 12-step ideology on all doctors in a zero-tolerance system of abuse and control while at the same time putting out misinformation that the PHP programs are the “new paradigm.” The page below is from the book Drug-Impaired Professionals by Robert Holman Coombs.
This is they type of propaganda these groups have propagated. What is described above is absurd and unrealistic but it is reported, reproduced and repeated to the point that it is accepted as the truth.
The majority of physicians referred to these programs are not even addicts. These programs of Zero-tolerance and 12-step indoctrination are based on coercion and control. They are causing many doctors to die by suicide as they are feeling hopeless, helpless and defeated. This portrayal of a group of blissful 12-stepping doctors over the moon because they found spirituality is nonsense.
But you will not find many doctors speaking out against them for fear of “contingency management.” Disagreeing or even questioning PHP practices including the validity of 12-step can literally cost you your license.
I have spoken to multiple physicians and nurses and have encouraged them to tell their stories here but they are afraid of retribution and “unintended consequences.” And who can blame them?
They can send you back to one of the “PHP-approved” facilities for “stinkin thinkin.”
Unfortunately the ASAM and FSPHP have successfully bamboozled others into believing they are true experts with noble intent. They have bamboozled the Federation of State Medical Boards (FSMB) to the point where they have gained autonomy and unrestrained managerial prerogative. They essentially use the state Boards to impose sanction on doctors who they report doctors for “noncompliance” which includes disagreeing with or questioning mandated A.A or refusing to admit you have a chronic relapsing brain disease when you in fact do not. They are in fact imposing A.A. on doctors and forcing them to accept their thinking under threat of loss of licensure. This violates the Establishment Clause and is a very serious problem that is being ignored. It is a slippery slope we are on.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness” that predates impairment often by many years.”
It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A. A. language –stinking thinking.”
The ASAM has monopolized addiction treatment in the United States. But what the FSPHP arm has done is far more sinister. A.A. has effectively taken over regulatory medicine and the private lives of doctors as a form of social control. A doctor can be referred to a PHP for virtually anything and if the PHP believes he or she is in need of an assessment it will be done by a “PHP-approved” facility which means it will be done by a 12-step facility. The PHP selects who will be monitored and dictates every aspect of what that entails and the entire process is done within the confines of A.A. ideology. It is a, in fact, a rigged game as the medical directors of the PHP approved facilities can all be seen on this list of like-minded docs who refer to theselves as “trusted servants” and “believe that evidence from extensive, well-designed studies demonstrates the great benefits of Twelve-Step recovery modalities including Twelve Step Facilitation in promoting long-term recovery.”
A.A. is imposed on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. And the bottom line is that A.A. has taken over all aspects of “physician health” and is forcing doctors to accept doctrine that is perhaps helpful to a few, useless or unneeded for many, and harmful and sometimes lethal to others. This is unacceptable and it needs to be recognized.
“New Paradigm” of Zero-Tolerance and 12-step Spirituality Based on “success” of PHP to Move to Other Occupations and Kids.
To move this “new paradigm” to other populations they had to gain control of the doctors first. They have not only created a monopoly but buffered themselves from physicians who may disagree with what they are doing to others. This current system essentially stifles them.
The power, immunity and impunity this group yields over doctors was done silently and with no opposition. It was done by sequential public-policy steps. This is why anyone interested in civil liberties and human rights should recognize the menace this presents to society. The scaffold is in place and they are just adding more nooses. Just ask the airline pilots. They plan to impose similar systems on teachers, students and athletes.
And this is all spelled out in the ASAM White Paper on Drug Testing. What people need to realize is what is described therein is just a few public policy steps away from them. The only organization they have to convince is the organization that regulates any type of professional license, employment or benefit.
Gaining regulatory sway in the medical field and control over individual doctors was necessary to move this model to other populations. It is merely a stepping stone for things to come. It is only a few public policy steps from us to you.
This impacts us all. It enables control of research, public policy and public health. It is a system that suppresses dissent and shapes conformity. The FSPHP encourages the confidential referral of outliers.
The ASAM is pro-drug war and anti-medical marijuana. This essentially silences most doctors for fear of being recognized and being brought in. I know many doctors who will not even talk about it in public.
This is fixed doctrine and will not change.
That is why the ACLU and other groups who promote civil rights, those who are against the drug war and anyone involved in Medical Marijuana need to step in. These groups need to recognize the reality of who these people are, what they have planned and understand why they need to be stopped. They are currently not even in the public eye and by outward appearances they appear to be benign. In truth they are malignant and rapidly metastasizing without any symptoms.
In Order to Stop This the Following Must be Done
1) get a team of epidemiologists/statisticians to attack the “evidence-base” and “research” that the ASAM/FSPHP has used to support their claims (junk science, pseudoscience, success of 12-step, etc) and do a Cochrane type meta-analysis that will show there is little to no basis for it.
2) Demand accountability of the PHPs. Assign accountability to the Medical Societies and Departments of Public Health. Demand they be accountable for state-contractors with the Medical Boards (many of whom are complicit–in Massachusetts the Board of Registration in Medicine is simply an extension of the state PHP-i.e. Like-minds.
3) Demand that the criminal activity taking place within these PHPs be addressed by law enforcement.
4) Demand the Attorney General enforce the rampant Establishment Clause Violations occurring with mass 12-step coercion.
5) Identify and expose the backgrounds of many of the individuals involved including felons and double felons who reinvented themselves as “addiction medicine” doctors. Many of these individuals are repeat offenders with a history of manipulating the system who should have never had their licenses returned. In my opinion the ASAM/FSPHP/LMD rigged system is an example of corporate psychopathy. While corporate level psychopathy is estimated at around 3% the numbers here appear to be much higher if one looks at the moral disengagement, unethical decision making, lack of empathy and externalization of blame evident in their personal histories.
6) Correctly identify that this system of institutional injustice is responsible for the astronomical suicide rate in physicians. This is due to the fact that doctors who need help are not getting it for fear of being ensnared by the state PHP and those already ensnared are being subject to coercion, abuse, institutional injustice, degradation, dehumanization, delegitimization and civil and human rights abuses and that this is a public health emergency that needs to be addressed.
7) reveal the scam set up between the PHPs, rogue labs, and “PHP-preferred” assessment and treatment gulags.
8) show how this is only a few public policy steps from Doctors to Pilots to Teachers to students to kids. etc. etc.
This necessitates that we get the conversation going before it is too late.
AA and 12-step may be the best treatment for some individuals with addiction and substance use disorders. If it works for you, then more power to you. I have no problem with that.
What I do have a problem with is imposing and mandating 12-step treatment on others.
Under a dictatorship everything else becomes subordinated to the guiding philosophy of the dictatorship. Corresponding doctrine replaces professional guidelines, standards-of-care, and evidence based medicine. And unfortunately in the case of Addiction Medicine the guiding philosophy often trumps autonomy and ethics.
Inherent in the current chronic brain disease model of addiction is the importance of external control over individuals and political correctness and medicalization of addiction is allowing it. Demanding scientific literacy and discriminating good from bad science would prohibit what is occurring and In order to save American Medicine the problem needs to be clearly recognized or we will become a profession that is essentially defined by the impaired physicians movement.
“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.” Father Cornelius Loos ( 1592 )
How Impaired Physicians Can be Helped–Medscape Business of Medicine Article Published February 24, 2015. Click on image to access
How can impaired Physicians be helped?
1. Impairment among physicians is growing: Why?
Answer: It is not. State Physician Health Programs (PHPs) are “diagnosing” impairment when there is no impairment. They are pathologizing the normal and expanding in scope to increase the grand scale of the hunt.
2. What’s the Prognosis for Impaired Physicians?
Answer: Not Good. Those who need help (the truly impaired) are afraid to get help for fear of being monitored by their state PHP while many of those ensnared by PHPs are not impaired. There is absolutely no oversight, regulation or accountability. This needs to be evaluated in the context of physician suicide. The system is one of institutional injustice and abuse of power.
3. Is your knowledge of physician impairment up-to-date?
Answer: No. This will only occur after an evidence-based Cochrane type review separates information from misinformation; An objective non-biased investigation by outside actors identifying any conflicts-of-interest, misconduct or lack of evidence-base in the current system and separating the art and science of the medical profession from the politicalization and exploitation of the medical profession.
As Drs. John Knight and J. Wesley Boyd note in Ethical and Managerial Considerations Regarding State Physician Health Programs, published in the Journal of the American Society of Addiction Medicine, this is what is known as “tailoring a diagnosis”–a euphemism for the political abuse of psychiatry. According to the Global Initiative on Psychiatry “Political abuse of psychiatry refers to the misuse of psychiatric diagnosis, treatment and detention for the purposes of obstructing the fundamental human rights of certain individuals and groups in a given society.” The shoe fits here. In fact it fits very well.
The Global Initiative on Psychiatry opposes the Political_Abuse_of_Psychiatry wherever it may occur and “supports those psychiatrists and psychiatric organizations that pressure the offending states to discontinue the practice and lobby vigorously those organizations which are wavering. The main way for individuals and organizations to work is through diplomatic channels. It is necessary to expose the practice and to embarrass countries that are at fault by expelling them from organizations such as the World Psychiatric Association. This can only be ensured by properly organized open investigation of psychiatric practice and interviews with the alleged victims”
Political abuse of psychiatry in the profession of medicine needs to be treated in the same way.
An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
In evaluating a physician for “impairment” or being “disruptive” the Physician Health Programs (PHPs) under the Federation of State Physician Health Programs (FSPHP) are not gathering data to form a hypothesis. They are making data fit a hypothesis that arrived at the out-of-state “PHP-approved” assessment center well before the alleged miscreant doctor.
With guilt assumed from the start, no due process, no appeal, and no way out physicians are being bullied, demoralized, and dehumanized to the point of hopelessness, helplessness and despair.
This needs to end now.
Medicine is predicated on competence, good-faith, and integrity.
Medical ethics necessitates beneficence, respect, and autonomy.
The scaffold erected here is designed for coercion and control.
Exposure, transparency, and accountability are urgent.
Blind-faith and unquestioning allegiance to expert authority deflects scrutiny and analysis. Few red flags are raised as this type of moral preening promotes misguided plausibility and complacency in the belief that these are indeed experts with good intentions. This needs to be addressed.
But if you look at any of the current “moral panics” that are being used to suggest random suspicion-less drug testing of doctors or promoting the Physician Health Programs as successful and replicable models, you will inevitably find a doctor on this list behind it. It is a given.
And the invitation goes out to Seppala to debate this in a public forum on a level playing field. Not gonna happen because it would be impossible for him to address and answer the questions rationally, directly and with any tiny scrap of evidence based data.
“Few, no matter how desperate, seek help of their own accord.” says Dr. Marv Seppala, M.D., Chief Medical Officer at Hazelden, one of the “PHP-approved” drug and alcohol assessment and treatment centers located in Center City, Minnesota. “Physicians are intelligent and skilled at hiding their addictions.”
“They’re often described as the best workers in the hospital,” he says. “They’ll overwork to compensate for other ways in which they may be falling short, and to protect their supply. They’ll sign up for extra call and show up for rounds they don’t have to do.”
In reality this is ludicrous–knee slapping absurd. If the results of this authoritative opinion were not so dire these statements would, in fact, be comical. Such is not the case, however, and opinions like Seppala’s have been taken at face value and, as a result, the aftermath has…
To have striven, to have made an effort, to have been true to certain ideals — this alone is worth the struggle. We are here to add what we can to, not to get what we can from, life. – William Osler
Diagnostic Medicine
Diagnostic medicine is the process of identifying the condition or disease that a patient has and ruling out conditions or diseases the patient does not have through assessment of the patient’s signs, symptoms, and results of various diagnostic tests.
Diagnostic Test Accuracy
Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
If a test’s results do not differ between alternative states of health, then the test has insignificant accuracy; if the results do not overlap with other states of health then the test has perfect accuracy. Most tests accuracies fall between these two extremes.
The intrinsic accuracy of a test is measured by comparing the test results to the “true condition status.”
‘True condition status” refers to one of two mutually exclusive states. Either acondition is present or it is absent.
We determine true condition status by means of a “gold standard” which is a source of information completely different from the test under evaluation which tells us the true condition status of the patient.
Say we want to develop a new rapid test for detecting strep throat. Strep throat is caused by the Streptococcus bacteria. Although more common in children and adolescents it can occur in people of all ages. Strep throat is one of many possible causes of sore throat and pharyngitis. It is contagious and can cause complications such as rheumatic and scarlet fever. Treatment with antibiotics can shorten the course of the disease and reduce the risk of complications.
A throat culture is obtained by swabbing the patient’s throat with a cotton swab. The sample is then sent to the lab where it is cultured. If strep is present it will grow on the culture and look as below. The bacteria either grows on the culture or it doesn’t. A throat culture is the “gold standard” for diagnosing strep throat. The problem is it may take two days to get back.
Sensitivity and Specificity
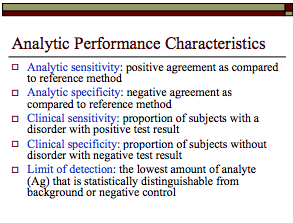
The two most important measures of diagnostic test accuracy are sensitivityand specificity.
The probability that a test will be positive in someone with the condition = Sensitivity
The Probability that a test will be negative in someone without the condition = Specificity
For diagnosing strep throat we want our test to be as close as possible to the gold standard in terms of both sensitivity and specificity.
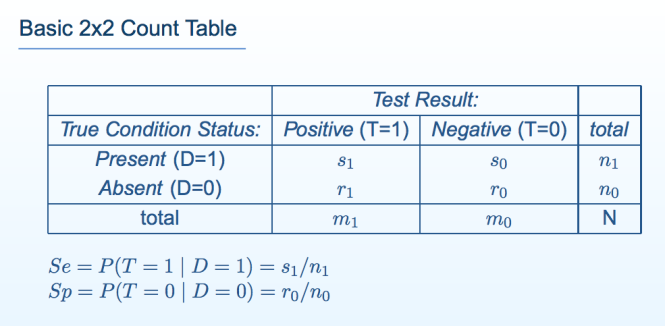
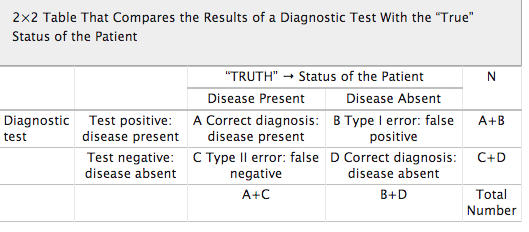
Sensitivity and specificity can be illustrated by a table with two rows and two columns. This simple Decision Matrixwhere the rows summarize the data according to the true condition status of the patients and the columns summarize the test results. This table is called a “count table” because it indicates the numbers of patients in various categories. The total number of patients with and without the condition is, respectively n\ and n0; the total number of patients with the condition who test positive and negative is respectively s\ and s0; and the total number of patients without the condition who test positive and negative is respectively r\ and ro.
The total number of patients in the study group N, is equal to N = si+so+rx+ro, or N = n\ + no·
The true condition status is symbolized by the variable D, where D = 1 if the condition is present and D= 0 if the condition is absent.
Test results indicating the condition is present are called positive; those indicating the condition is absent are called negative.
Test results are symbolized by the variable T, where T =1 denotes positive test results and T= 0 denotes negative test results.
The sensitivity (Se) of a test is its ability to detect the condition when it is present.
We write sensitivity as Se = P(T = 1 | D = 1), which is read:
“sensitivity (Se) is the probability (P) that the test result is positive (T = 1), given that the condition is present (D = 1).”
Among the n\ patients with the condition, s\ test positive; thus, Se = s\/n\.
The specificity (Sp) of a test is its ability to exclude the condition in patients without the condition.
We write specificity as Sp — P(T = 0 | D — 0), which is read:
“specificity (Sp) is the probability (P) that the test result is negative (T = 0), given that the condition is absent (D = 0).”
Among no patients without the condition, ro test negative; thus, Sp — TQ/UQ
False Negative and False Positive Tests
There are consequences associated with all test results.
False Negative Tests: If a test falsely indicates the absence of a condition in someone who truly has it then treatment can be delayed or not provided.
The consequences of a false negative strep test depend on what we do with it. Serious consequences can arise if we use our new strep test as the sole basis for subsequent decision making. Putting complete trust in the negative test result would lead to no antibiotic treatment provided to a patient with Strep and can lead to continued illness, spread of the disease and complications that would not have occurred if antibiotics were provided. The patient could potentially get rheumatic or scarlet fever.
If the new test is negative but a culture was drawn the false results could delay treatment by a couple days or so but treatment is nevertheless provided. The consequences are likely to be minimal. It is highly unlikely a patient would get rheumatic or scarlet fever as, although a little later, they are still being treated with the proper antibiotics.
False Positive Tests: If a test falsely indicates the presence of a condition in someone who does not truly have it then unnecessary tests and treatments can occur. Incorrect treatment and false labeling of patients can also occur.
In the case of a false positive strep test, a patient may undergo a course of antibiotics when they do not need them. Although the patient may suffer side-effects from the antibiotics the severity and duration of any of these consequences are minimal.
The importance of a Diagnostic Accuracy in testing is directly proportional to the tests potential to cause patient consequences and harm.
Diagnostic Medicine uses a patient’s signs, symptoms and the results of various diagnostic tests to arrive at a diagnosis.
In diagnosing strep throat a good clinician will take into account a number of variables in consideration of a differential diagnosis and base testing and treatment on the preponderance of information supporting or opposing the diagnosis.
For strep throat using the new test in addition to a throat culture, history and careful physical exam and basing the decision to prescribe antibiotics on clinical acumen based on the overall picture is the best approach. The test can be considered a piece of the puzzle but does not define it. Therefore the risk of a false positive or false negative is minimal as it is just one data point.
Diagnostic accuracy is necessary if a test is being used as the basis for further tests and treatment. If a test is being used as the sole basis for further tests and treatment it needs to be accurate. If the results of a test can cause significant patient harm or death then it needs to be either 100% accurate or combined with other highly accurate tests to confirm the diagnosis.
The specificity of a test is particularly important as a false positive can result in unneeded interventions and treatment. Stand-alone tests used in diagnosis and treatment need to be both sensitive and specific. Diagnostic accuracy is a product of consequences of false-negative and false positive tests.
Diagnostic Research Methodology
Research to discover the accuracy of a diagnostic test should be straightforward; administer the test to a group of people and see if it works.
The test being tested is the “index test”. Results of the index test are compared with the results of a “gold standard” reference test.
The research question is, “How accurately do index test results predict the (true, gold standard) reference test results?”
Diagnostic test accuracy studies require a sample of subjects who have been given the test under evaluation, some form of scoring of the tests findings and a reference or “gold standard” to which the test findings are compared. Examples include autopsy reports, surgery findings and pathology results from biopsy findings.
The gold standard for a patient’s true disease status may not always be available. A brain biopsy could be considered a gold standard for diagnosing Alzheimer’s disease but is neither practical nor humane.
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool is a set of fourteen questions that investigate the methodologic quality of scientific studies that quantify diagnostic test performance.
The questions identify research methodologies known to bias the accuracies research discovers.
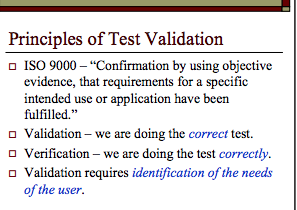
Multiple factors need to be considered in evaluating the diagnostic accuracy of a test including diagnostic validation and verification. Is the test testing what it is supposed to be testing for and are we doing it correctly?
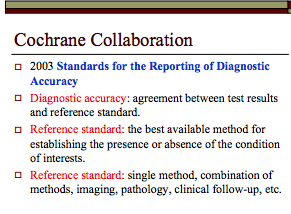
Diagnostic accuracy of a test necessitates a reference standard, The reference standard can be the best available method for establishing the presence or absence of a condition (such as the throat culture for strep throat) or a combination of methods (imaging, neuropsychological testing, clinical exam, etc. in Alzheimer’s disease.
Any test that is going to be used as a basis for decisions that impact other human beings needs to be validated before it is introduced on the market. The literature needs to be reviewed critically and trials must be designed using objective evidence that validates the test is testing for what it purports to be and verifies the correct methodology of the test. Verification that the test is being collected, handled, stored, transported and processed correctly is requisite.
Cutoff levels, , cross-reactivity and myriad other issues need to be worked out prior to bringing a diagnostic test to market.
The reliability, validity and accuracy of drug test results needs to be known prior to using a test. Specificity and sensitivity must be known prior to using a test on any population.
This should go without saying as to do anything else would be irresponsible and careless.
References
Evidence-based medicine, systematic reviews, and guidelines in interventional pain management: part 7: systematic reviews and meta-analyses of diagnostic accuracy studies Pain Physician 2009, 12(6):929-963. PubMed Abstract | Publisher Full Text
Jaeschke R, Guyatt G, Lijmer J: Diagnostic tests. In Users’ guides to the medical literature: a manual for evidence-based clinical practice. Edited by Guyatt G, Rennie D. AMA Press; 2002:121-140.
Streiner DL: Diagnosing tests: using and misusing diagnostic and screening tests.J Pers Assess 2003, 81(3):209-219. PubMed Abstract | Publisher Full Text
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J: The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003., 3(25) http://www.biomedcentral.com/1471-2288/3/25webcite
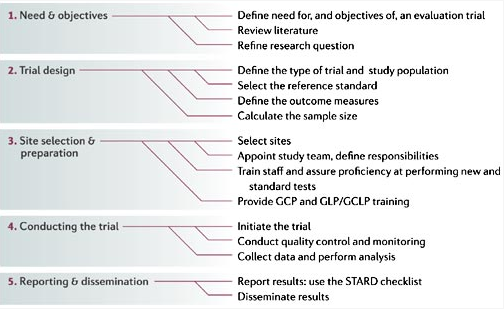
GCP, good clinical practice; GCLP, good clinical laboratory practice; GLP, good laboratory practice; STARD, standards for reporting of diagnostic accuracy. See Section III, 2.13 From Nature Reviews Microbiology 4, S20–S32 (1 December 2006) | doi:10.1038/nrmicro1570
The 12-red flags below are very applicable to American Society of Addiction Medicine (ASAM) related consensus and public policy. When viewed through this lens the science and research all falls apart.
(1) When different claims get bundled together.
(2) When ad hominem attacks against dissenters predominate.
(3) When scientists are pressured to toe the party line.
(4) When publishing and peer review in the discipline is cliquish.
(5) When dissenting opinions are excluded from the relevant peer-reviewed literature not because of weak evidence or bad arguments but as part of a strategy to marginalize dissent.
(6) When the actual peer-reviewed literature is misrepresented.
(7) When consensus is declared hurriedly or before it even exists.
(8) When the subject matter seems, by its nature, to resist consensus.
(9) When “scientists say” or “science says” is a common locution.
(10) When it is being used to justify dramatic political or economic policies.
(11) When the “consensus” is maintained by an army of water-carrying journalists who defend it with uncritical and partisan zeal, and seem intent on helping certain scientists with their messaging rather than reporting on the field as objectively as possible.
(12) When we keep being told that there’s a scientific consensus.
Up until the birth of the EtG, tests used for forensic drug and alcohol monitoring had to go through the arduous, expensive and necessary FDA approval process. The LDT pathway was designed to develop simple tests with little risk that have low market potential (i;e. the cost of the normal FDA approval process would prohibit them from coming to market). The LDT pathway was designed to improve patient care in the diagnosis and treatment of patients. It was not designed for forensic tests. LDT approval does not require in vivo testing. It is essentially an honor system and to develop an LDT it is not even necessary to prove that the test is actually testing what it is purportedly testing for (validity).
So with little to no evidence base an ASAM/FSPHP physician introduced the EtG, had it developed and marketed as a LDT in collusion with unscrupulous labs, and then began using it on physicians being monitored by State PHPs. This then spread to other monitoring organizations in which there was a large power-differential between those ordering the tests and those being tested (criminal-justice, other professional monitoring programs). These biomarkers have never been used in Federal Drug Testing, SAMHSA approved, DOT, and other organizations where unions or other organizations are present and looking out for the best interests of those being tested.
The validity and reliability of opinions lie in their underlying methodology and evidence base. Reliance on the personal authority of any expert or group of experts is the fallacy of appeal to authority.
I have asthma but that does not make me a Pulmonologist. That addiction “specialist” diagnosing and treating you may have 5 years prior been a proctologist; and maybe not even a very good one at that.
Somewhere there may be doctor with no post-graduate training in surgery wielding a scalpel and calling himself an expert surgeon, but it is difficult to imagine that he is a very good one.
“How to Position Yourself as an EXPERT, Make More Money and Help More People, by Becoming a Published Author – Even if You Don’t Know Where to Start!” Think about it – if you need to see a chiropractor, for example, would you rather see a general chiropractor, or one who has positioned … http://leighstjohn.com/free-educational-webinar-how-to-position-yourself-as-an-expert/
The ASAM plans to introduce non-FDA approved “forensic” Laboratory Developed Tests (LDTs) into mainstream healthcare via a loophole. This same group introduced most of these tests through a loophole and now they want to drug-and alcohol TEST EVERYBODY including STUDENTS AND KIDS through another loophole! These tests are of unknown reliability and accuracy. The LDT pathway does not even require proof that the test is even valid (i.e. that the test is actually testing for the substance it claims to be testing) but with no FDA oversight or regulation the labs can claim anything they want in marketing it and they do.
If a doctor collects a test on a “patient” the test is rendered “clinical” rather than “forensic” and by deeming this drug-testing “clinical” rather than “forensic” they can then call the consequences of a positive test “treatment” rather than “punishment. ” It is via this loophole they plan to introduce and unleash the panoply of junk-science tests currently being used on other groups who have no say in the matter (probationers, parolees, private professional monitoring groups, etc. ) onto the general population at large. A boon for the Drug and Alcohol Testing Industry Association and the assessment and treatment industry but a bane to the rest of society. And to prevent this from happening more people need to be talking about this.
The goal of the ASAM has always been to get the medical establishment to accept 12-step spiritual recovery.
AMSA evolved into the ASAM
According to the American Society of Addiction Medicine The ASAM Principles of Addiction Medicineis the “go-to textbook in the specialty of addiction medicine” and:
The 4th Edition of The ASAM Principles of Addiction Medicine contains an entire section entitled “Mutual Help, Twelve Step, and Other Recovery Programs” containing three chapters entitled “Twelve Step Programs in Recovery,”1 “Recent Research into Twelve Step Programs”2 and “Spirituality in the Recovery Process.”3
Despite the all-encompassing title of this 31-page section (pages 911-942) no “other recovery programs” are described. In fact, no other programs bar 12-step ideology are even mentioned.
I have read through each chapter word-for-word three times just to be sure; and although the chronic relapsing brain disease model of addiction requiring lifelong abstinence and spiritual recovery is described, trumpeted and proselytized in great detail, not one other model of addiction is even named.
As with anything I write I encourage you to fact-check this. My goal here is to present my opinions with facts and evidence that can be checked and verified. Point out any errors of fact and I will promptly remove and correct them.
If a Cardiology textbook had a section entitled “Cholesterol, Statins and other Lipid Lowering Agents” with three chapters that only described Lipitor it would be correctly lambasted from every angle by the entire field of medicine as soon as it hit the shelves.
The lack of evidence-base and conflicts-of-interest would be recognized and dealt with immediately and when it was realized that many of the authors not only profited from, but based their very own cardiac health on Lipitor they would rightly be held accountable. Such is not the case in Addiction Medicine.
The validity and reliability of opinions lie in their underlying methodology and evidence base. Reliance on the personal authority of any expert or group of experts is the fallacy of appeal to authority.
An appeal to Authority is a fallacy with the following form:
Person A is (claimed to be) an authority on subject S.
Person A makes claim C about subject S.
Therefore, C is true
The fallacy is committed when the person (or group) in question is not a legitimate authority on the subject. If person A is not qualified to make reliable claims about subject S then the argument will be fallacious. Since this sort of reasoning is fallacious only when the person is not a legitimate authority it is necessary that acceptable standards be set and the following standards are widely accepted.
The person has sufficient expertise in the subject matter in question.
The claim being made by the person is within her area(s) of expertise.
There is an adequate degree of agreement among the other experts in the subject in question.
The person in question is not significantly biased.
The area of expertise is a legitimate area or discipline
With the exception of number 5 the ASAM fails on all counts, but policy makers, members of the press, politicians and others have been successfully bamboozled into believing the ASAM are indeed “experts” in Addiction Medicine. Over the years, the American Society of Addiction Medicine has continued to promote the AA position that alcoholism (and by inference any other addiction) is an illness which only a “spiritual experience will conquer.” All addictions are believed by ASAM to be caused by a lifelong chronic relapsing brain disorder that can only be treated by complete abstinence from all mood-altering substances (with the apparent exceptions of tobacco and caffeine interestingly) and the vast majority of ASAM doctors believe that the only effective treatment for addiction must include surrendering one’s “will and life over to the care of God.”
Because addiction is defined as a disease, addicts must be “treated” (often coerced) and “cured” (which is defined as remaining abstinent).
The medical profession needs to reexamine its role in Addiction Medicine.
Confusing ideological opinions with professional knowledge is unacceptable. Presenting it as textbook science is not only dangerous but fosters negligence, abuse of power, self-interest and prejudice on the part of the medical community with respect to the treatment of all patients.
To be clear, just as Lipitor may be the best treatment for some individuals with elevated cholesterol, AA and 12-step may be the best treatment for some individuals with addiction and substance use disorders. If it works for them, then more power to them. I have no problem with that.
What I do have a problem with is imposing and mandating any treatment on others.
Under a dictatorship everything else becomes subordinated to the guiding philosophy of the dictatorship. Corresponding doctrine replaces professional guidelines, standards of care, and evidence based medicine. And unfortunately in the case of Addiction Medicine the guiding philosophy often trumps autonomy and ethics.
Inherent in the current chronic brain disease model of addiction is the importance of external control over individuals. Political correctness and the oversimplified medicalization of addiction is allowing it. Demanding scientific literacy and discriminating good science from bad science would prohibit what is occurring and In order to save American Medicine this problem needs to be clearly recognized. Otherwise we will become a profession that is essentially defined by the false dichotomies and grand illusions defined by the impaired physicians movement.
Schulz JE, Williams V. Twelve Step Programs in Recovery. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. Baltimore: Lippincott Williams & Wilkens; 2009:911-922.
McCrady BS, Tonigan GS. Recent Research into Twelve Step Programs. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed: Lippincott Williams & Wilkens; 2009:923-937.
Galanter M. Spirituality in the Recovery Process. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed. Baltimore: Lippincott Williams & Wilkens; 2009:939-942.
Please donate to Disruptedphysician.com here to keep this blog running. It is expiring in 21 days and any contribution would be appreciated. We are making significant gains with articles such as Physician Health Programs Under Fire . These issues may seem small in the current turbulence, a small whirlpool in a maelstrom, but in reality they have enormous implications for all of us. Please help out if you can-ML




























 Wanted!–a Few Statisticians, Biostatisticians and Epidemiologists who want to make a difference in Medicine, Society and our Future
Wanted!–a Few Statisticians, Biostatisticians and Epidemiologists who want to make a difference in Medicine, Society and our Future