

Forget what you see
Some things they just change invisibly–Elliott Smith

Physician Impairment
The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence, published by the American Medical Association’s (AMA) Council on Mental Health in The Journal of the American Medical Association in 1973,1 recommended that physicians do a better job of helping colleagues impaired by mental illness, alcoholism or drug dependence. The AMA defined an “impaired physician” as “a physician who is unable to practice medicine with reasonable skill and safety to patients because of mental illness or excessive use or abuse of drugs, including alcohol.”
Recognition of physician impairment in the 1970s by both the medical community and the general public led to the development of “impaired physician” programs with the purpose of both helping impaired doctors and protecting the public from them.
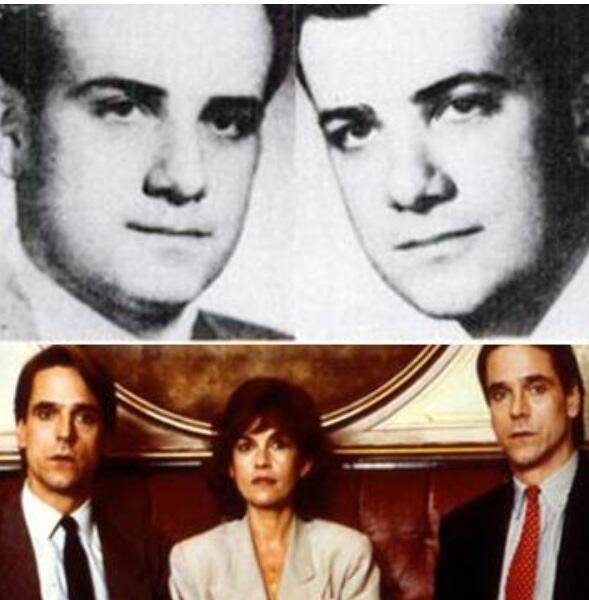
 The 1975 media coverage of the deaths of Drs. Stewart and Cyril Marcus brought the problem of impaired physicians into the public eye.
The 1975 media coverage of the deaths of Drs. Stewart and Cyril Marcus brought the problem of impaired physicians into the public eye.  Leading experts in the field of Infertility Medicine, the twin gynecologists were found dead in their Upper East Side apartment from drug withdrawal that New York Hospital was aware of but did nothing about. Performing surgery with trembling hands and barely able to stand, an investigation revealed that nothing had been done to help the Marcus brothers with their addiction or protect patients. They were 45 –years old.
Leading experts in the field of Infertility Medicine, the twin gynecologists were found dead in their Upper East Side apartment from drug withdrawal that New York Hospital was aware of but did nothing about. Performing surgery with trembling hands and barely able to stand, an investigation revealed that nothing had been done to help the Marcus brothers with their addiction or protect patients. They were 45 –years old.
Although the New York State Medical Society had set up its own voluntary program for impaired physicians three years earlier, the Marcus case prompted the state legislature to pass a law that doctors had to report any colleague suspected of misconduct to the state medical board and those who didn’t would face misconduct charges themselves.
Physician Health Programs
Physician health programs (PHPs) existed in almost every state by 1980. Often staffed by volunteer physicians and funded by State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referral.
As an alternative to discipline the introduction of PHPs created a perception of medical boards as “enforcers” whose job was to sanction and discipline whereas PHPs were perceived as “rehabilitators” whose job was to help sick physicians recover. One of many false dichotomies this group uses and it is perhaps this perceived benevolence that created an absence of the need to guard.
Employee Assistance Programs for Doctors
Physician Health Programs (PHPs) are the equivalent of Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess, and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems.
Most EAPs, however, were developed with the collaboration of workers unions or some other group supporting the rights and best interests of the employees. PHPs were created and evolved without any oversight or regulation.
The American Society of Addiction Medicine can trace its roots to the 1954 founding of theNew York City Medical Society on Alcoholism (NYCMSA) by Ruth Fox, M.D whose husband died from alcoholism.
The society, numbering about 100 members, established itself as a national organization in1967, the American Medical Society on Alcoholism (AMSA).
By 1970 membership was nearly 500.
In 1973 AMSA became a component of the National Council on Alcoholism (NCA) in a medical advisory capacity until 1983.
But by the mid 1980’s ASAM’s membership became so large that they no longer needed to remain under the NCADD umbrella.
In 1985 ASAM’s first certification exam was announced. According to Dr. Bean-Bayog, chair of the Credentialing Committee, “a lot of people in the alcoholism field have long wanted physicians in the field to have a high level of skills and scientific credibility and for this body of knowledge to be accredited.”2 And in 1986 662 physicians took the first ASAM Certification Exam.

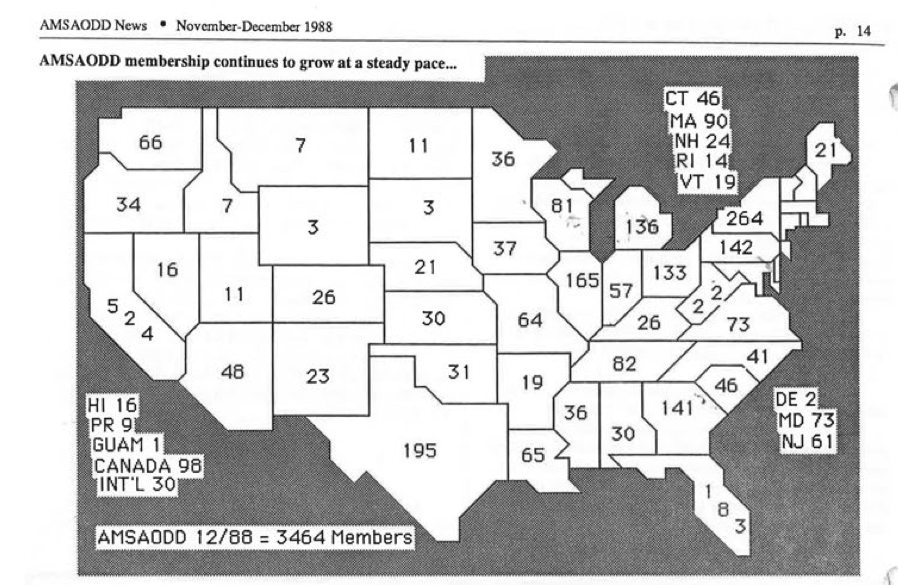
By 1988 membership was over 2,800 with 1,275 of these physicians “certified” as “having demonstrated knowledge and expertise in alcoholism and other drug dependencies commensurate with the standards set forth by the society.”3 “The formation of State Chapters began with California, Florida, Georgia, and Maryland submitting requests.4
In 1988 the AMA House of Delegates voted to admit ASAM to the House. According to ASAM News this “legitimizes the society within the halls of organized medicine.”2
By 1993 ASAM had a membership of 3,500 with a total of 2,619 certifications in Addiction Medicine. The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”5
certifications in Addiction Medicine. The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”5
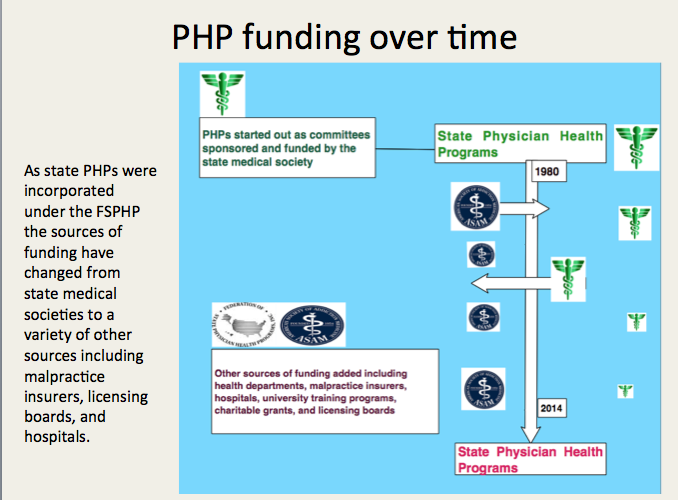
Many of these physicians joined state PHPs and over time have taken over under the umbrella of the FSPHP.
Others became medical directors of treatment centers such as Hazelden, Marworth and Talbott.
- The sick physician. Impairment by psychiatric disorders, including alcoholism and drug dependence. JAMA : the journal of the American Medical Association. Feb 5 1973;223(6):684-687.
- Four Decades of ASAM. ASAM News. March-April 1994, 1994.
- . American Medical Society on Alcoholism & Other Drug Dependencies Newsletter. Vol III. New York, NY: AMSAODD; 1988:12.
- . AMSAODD News. Vol III. New York, NY: American Medical Society on Alcoholism & Other Drug Dependencies; 1988.
- Membership Campaign Update. ASAM News. Vol VIII: American Society of Addiction Medicine; 1993:11.



