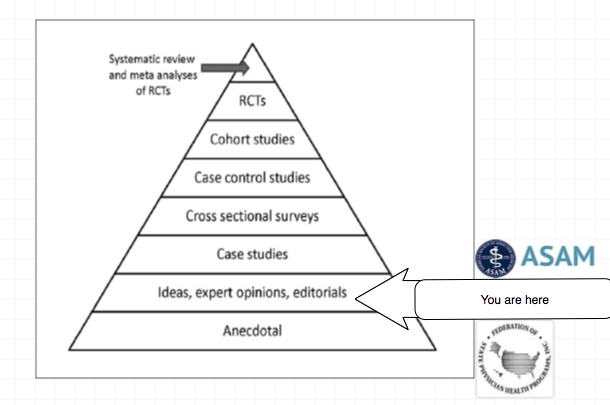
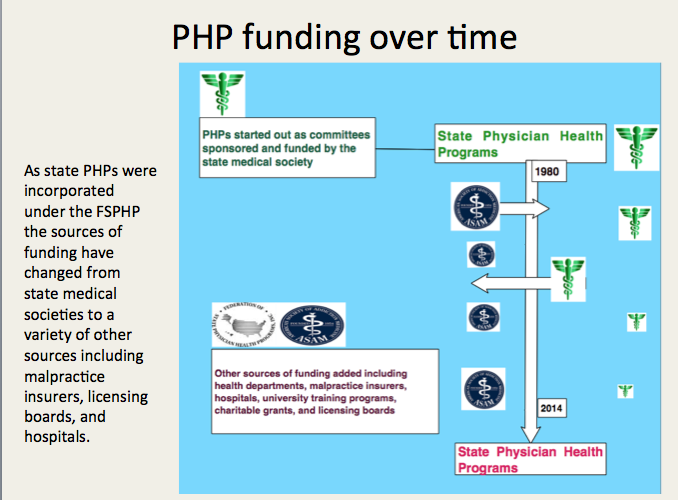
The blue slides below are from a presentation at the 2014 FSPHP spring meeting in Denver, Colorado and can be seen here. The presentation was given by past FSPHP Presidents Gary Carr, MD and Warren Prendergast, MD, West Virginia PHP Director Brad Hall, MD and Montana PHP Director Mike Ramirez, MS.
This needs to be seen as a “to-do” list.
A.A. = ASAM = FSPHP
The quote is from Alcoholics Anonymous and the full passage is as follows:
“We are convinced that a spiritual mode of living is a most powerful health restorative. We, who have recovered from serious drinking, are miracles of mental health. But we have seen remarkable transformations in our bodies. Hardly one of our crowd now shows any mark of dissipation.
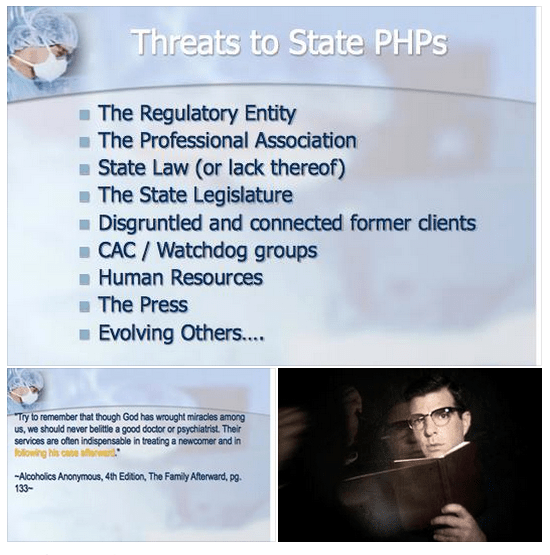
But this does not mean that we disregard human health measures. God has abundantly supplied this world with fine doctors, psychologists, and practitioners of various kinds. Do not hesitate to take your health problems to such persons. Most of them give freely of themselves, that their fellows may enjoy sound minds and bodies. Try to remember that though God has wrought miracles among us, we should never belittle a good doctor or psychiatrist. Their services are often indispensable in treating a newcomer and in following his case afterward.”–Alcoholics Anonymous, 4th Edition, The Family Afterward
Federation of State Physician Health Program (FSPHP) physicians often quote A.A. because they are defined by A.A. in both mechanics and mentality. The “impaired physician” movement began with evangelical recovered addict and alcoholic physicians whose recovery was based on 12- step spirituality. As this group molded into the American Society of Addiction Medicine (ASAM) many of them found employment at 12-step rehabilitation facilities and others joined their state Physician Health Programs and organized under the FSPHP. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insiders knowledge of recovery as brandished in this A.A. passage which I find condescending toward the medical profession and oddly narcissistic.
This special knowledge, of course, was based on the chronic relapsing brain disease model with lifelong abstinence and participation in 12-step recovery.
These “miracles of mental health” joined their state PHPs and those who did not agree with their rigid inflexible views were removed. Those with access to special secret knowledge were eventually able to outvote those with intelligence and open minds as this groupthink infested and eventually monopolized PHPs.
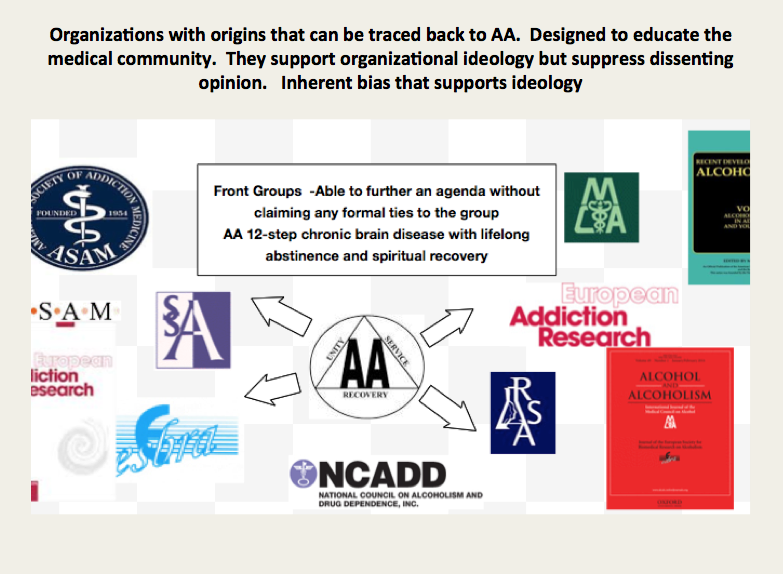
It is important to understand that the ideology of A.A. is the ideology of the ASAM is the ideology of the FSPHP
Like all “front-groups” the ASAM purports to serve one agenda while in reality serving another. The ASAM claims to be a “physician society with a focus on addiction and its treatment” According to their website their mission is to
- increase access to and improve the quality of addiction treatment;
- to educate physicians (including medical and osteopathic students), other health care providers and the public;
- to support research and prevention;
- to promote the appropriate role of the physician in the care of patients with addiction;
- and to establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers and consumers of health care services, and the general public
In order to accomplish this the American Board of Addiction Medicine certifies doctors to “provide assurance to the American public that Addiction Medicine physicians have the knowledge and skills to prevent, recognize and treat addiction.”
Ostensibly these are laudable goals that are almost universally endorsed. The perceived organizational purpose and public persona are altruistic and humanitarian. Treating addiction not only saves individual lives but improves the community. It is for the common good.
Abuse Hidden Under Benevolence and Torture as Treatment
History reveals that all manner of abuse can lie underneath a patina of benevolence. In the past few months alone we have both Bill Cosby and the British Parliamentary pedophile ring as prototypical examples. Both cases reveal a decades long coverup of allegations in which the abusers escaped little or no investigation into their alleged crimes. Abuse of power with a large gap between the power of the abuser and the powerlessness of the abused is a common denominator. If the abuser endorses our own beliefs systems it creates a discord that promotes disbelief. It does not fit. Accusations are dismissed, deflected or otherwise suppressed. Power effectively extinguishes the truth. Disbelieved and delegitimized, information is suppressed, charges are not filed and law enforcement and the media turn a blinkered eye for decades. Indifference, disbelief, rationalization and cognitive dissonance prevent exposure and accountability. Hidden in plain site the truth was there and easy to find. The problem was no one was looking. Most did not want to look.
It does not take much sleuthing to uncover what is beneath the veil of the American Society of Addiction Medicine. The history, mentality and mechanics are well documented and reveal where they came from, how they evolved and what they have planned. It is a complicated web and hard to explain but once the pieces of the puzzle are fit together it is clear. But it involves assembling a complex puzzle by finding the individual pieces scattered in disparate areas including the regulatory, clinical, administrative and professional niches of the medical profession, Alcoholics Anonymous and 12-step related organization, public policy, all levels of the political arena and other areas. Once put together the portrait is clear.
In reality the ASAM is a political action group or special interest group that is designed to cement the chronic relapsing brain disease model with lifelong abstinence and spiritual recovery as the one and only treatment for addiction. A.A. is used as the energy source of the operation. By labeling addiction a “disease” requiring “treatment” in which someone is helpless they are able to dictate all aspects by coercion and control. But in my opinion the A.A. ideology is just used as a ruse to support the multi-billion dollar drug and alcohol testing, assessment and treatment industry. The zero-tolerance mindset of the “treaters” combined with the “helplessness” of the diseased enables them to erect a revolving door of testing, assessment and treatment that provides them with both control and a steady stream of money.

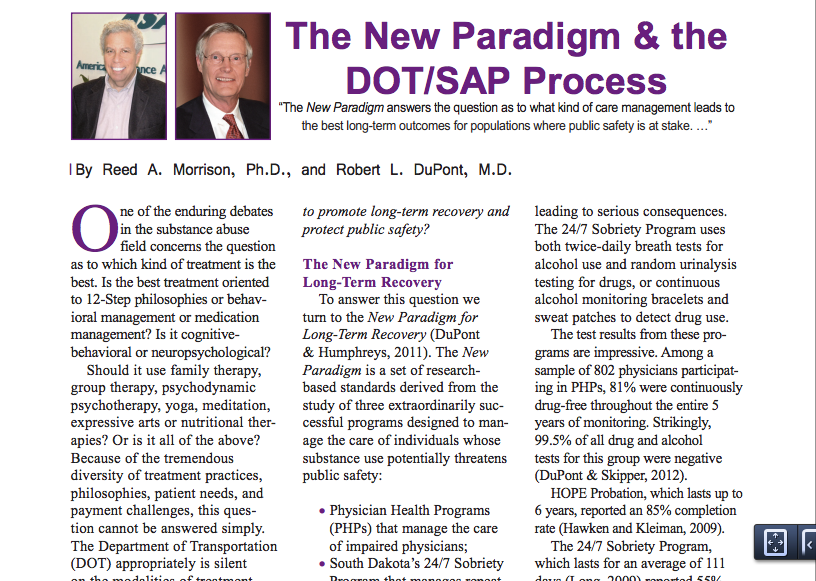
The FSPHP mandates 12-step ideology on all doctors in a zero-tolerance system of abuse and control while at the same time putting out misinformation that the PHP programs are the “new paradigm.” The page below is from the book Drug-Impaired Professionals by Robert Holman Coombs.
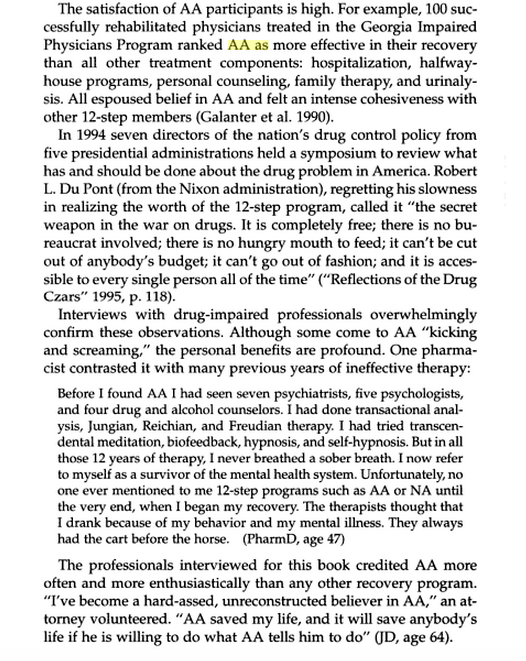
This is they type of propaganda these groups have propagated. What is described above is absurd and unrealistic but it is reported, reproduced and repeated to the point that it is accepted as the truth.
The majority of physicians referred to these programs are not even addicts. These programs of Zero-tolerance and 12-step indoctrination are based on coercion and control. They are causing many doctors to die by suicide as they are feeling hopeless, helpless and defeated. This portrayal of a group of blissful 12-stepping doctors over the moon because they found spirituality is nonsense.
But you will not find many doctors speaking out against them for fear of “contingency management.” Disagreeing or even questioning PHP practices including the validity of 12-step can literally cost you your license.
I have spoken to multiple physicians and nurses and have encouraged them to tell their stories here but they are afraid of retribution and “unintended consequences.” And who can blame them?
They can send you back to one of the “PHP-approved” facilities for “stinkin thinkin.”
Unfortunately the ASAM and FSPHP have successfully bamboozled others into believing they are true experts with noble intent. They have bamboozled the Federation of State Medical Boards (FSMB) to the point where they have gained autonomy and unrestrained managerial prerogative. They essentially use the state Boards to impose sanction on doctors who they report doctors for “noncompliance” which includes disagreeing with or questioning mandated A.A or refusing to admit you have a chronic relapsing brain disease when you in fact do not. They are in fact imposing A.A. on doctors and forcing them to accept their thinking under threat of loss of licensure. This violates the Establishment Clause and is a very serious problem that is being ignored. It is a slippery slope we are on.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness” that predates impairment often by many years.”
It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A. A. language –stinking thinking.”
The ASAM has monopolized addiction treatment in the United States. But what the FSPHP arm has done is far more sinister. A.A. has effectively taken over regulatory medicine and the private lives of doctors as a form of social control. A doctor can be referred to a PHP for virtually anything and if the PHP believes he or she is in need of an assessment it will be done by a “PHP-approved” facility which means it will be done by a 12-step facility. The PHP selects who will be monitored and dictates every aspect of what that entails and the entire process is done within the confines of A.A. ideology. It is a, in fact, a rigged game as the medical directors of the PHP approved facilities can all be seen on this list of like-minded docs who refer to theselves as “trusted servants” and “believe that evidence from extensive, well-designed studies demonstrates the great benefits of Twelve-Step recovery modalities including Twelve Step Facilitation in promoting long-term recovery.”
A.A. is imposed on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. And the bottom line is that A.A. has taken over all aspects of “physician health” and is forcing doctors to accept doctrine that is perhaps helpful to a few, useless or unneeded for many, and harmful and sometimes lethal to others. This is unacceptable and it needs to be recognized.
“New Paradigm” of Zero-Tolerance and 12-step Spirituality Based on “success” of PHP to Move to Other Occupations and Kids.
To move this “new paradigm” to other populations they had to gain control of the doctors first. They have not only created a monopoly but buffered themselves from physicians who may disagree with what they are doing to others. This current system essentially stifles them.
The power, immunity and impunity this group yields over doctors was done silently and with no opposition. It was done by sequential public-policy steps. This is why anyone interested in civil liberties and human rights should recognize the menace this presents to society. The scaffold is in place and they are just adding more nooses. Just ask the airline pilots. They plan to impose similar systems on teachers, students and athletes.
And this is all spelled out in the ASAM White Paper on Drug Testing. What people need to realize is what is described therein is just a few public policy steps away from them. The only organization they have to convince is the organization that regulates any type of professional license, employment or benefit.
Gaining regulatory sway in the medical field and control over individual doctors was necessary to move this model to other populations. It is merely a stepping stone for things to come. It is only a few public policy steps from us to you.
This impacts us all. It enables control of research, public policy and public health. It is a system that suppresses dissent and shapes conformity. The FSPHP encourages the confidential referral of outliers.
The ASAM is pro-drug war and anti-medical marijuana. This essentially silences most doctors for fear of being recognized and being brought in. I know many doctors who will not even talk about it in public.
This is fixed doctrine and will not change.
That is why the ACLU and other groups who promote civil rights, those who are against the drug war and anyone involved in Medical Marijuana need to step in. These groups need to recognize the reality of who these people are, what they have planned and understand why they need to be stopped. They are currently not even in the public eye and by outward appearances they appear to be benign. In truth they are malignant and rapidly metastasizing without any symptoms.
In Order to Stop This the Following Must be Done
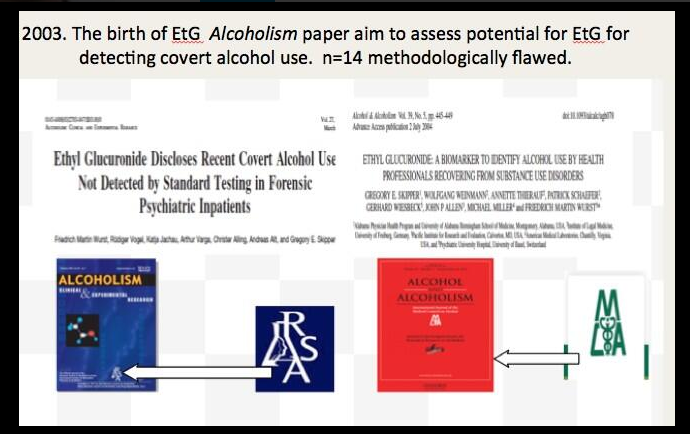
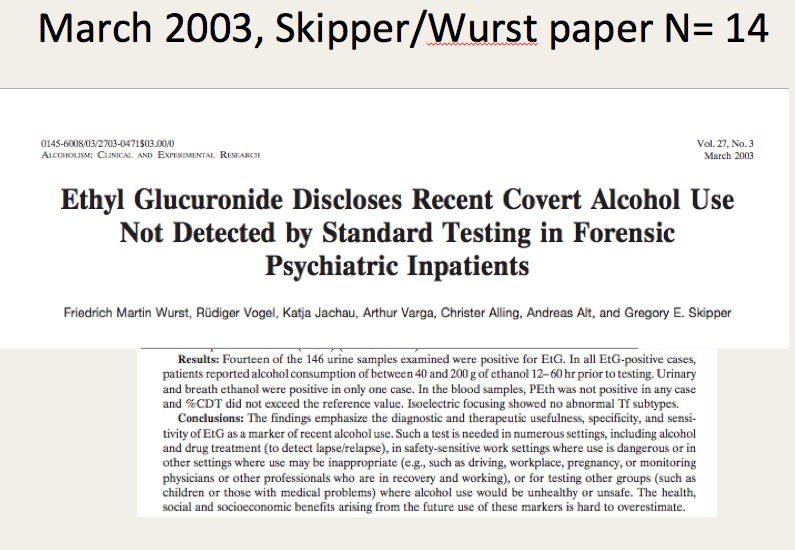
1) get a team of epidemiologists/statisticians to attack the “evidence-base” and “research” that the ASAM/FSPHP has used to support their claims (junk science, pseudoscience, success of 12-step, etc) and do a Cochrane type meta-analysis that will show there is little to no basis for it.
2) Demand accountability of the PHPs. Assign accountability to the Medical Societies and Departments of Public Health. Demand they be accountable for state-contractors with the Medical Boards (many of whom are complicit–in Massachusetts the Board of Registration in Medicine is simply an extension of the state PHP-i.e. Like-minds.
3) Demand that the criminal activity taking place within these PHPs be addressed by law enforcement.
4) Demand the Attorney General enforce the rampant Establishment Clause Violations occurring with mass 12-step coercion.
5) Identify and expose the backgrounds of many of the individuals involved including felons and double felons who reinvented themselves as “addiction medicine” doctors. Many of these individuals are repeat offenders with a history of manipulating the system who should have never had their licenses returned. In my opinion the ASAM/FSPHP/LMD rigged system is an example of corporate psychopathy. While corporate level psychopathy is estimated at around 3% the numbers here appear to be much higher if one looks at the moral disengagement, unethical decision making, lack of empathy and externalization of blame evident in their personal histories.
6) Correctly identify that this system of institutional injustice is responsible for the astronomical suicide rate in physicians. This is due to the fact that doctors who need help are not getting it for fear of being ensnared by the state PHP and those already ensnared are being subject to coercion, abuse, institutional injustice, degradation, dehumanization, delegitimization and civil and human rights abuses and that this is a public health emergency that needs to be addressed.
7) reveal the scam set up between the PHPs, rogue labs, and “PHP-preferred” assessment and treatment gulags.
8) show how this is only a few public policy steps from Doctors to Pilots to Teachers to students to kids. etc. etc.
This necessitates that we get the conversation going before it is too late.
AA and 12-step may be the best treatment for some individuals with addiction and substance use disorders. If it works for you, then more power to you. I have no problem with that.
What I do have a problem with is imposing and mandating 12-step treatment on others.
Under a dictatorship everything else becomes subordinated to the guiding philosophy of the dictatorship. Corresponding doctrine replaces professional guidelines, standards-of-care, and evidence based medicine. And unfortunately in the case of Addiction Medicine the guiding philosophy often trumps autonomy and ethics.
Inherent in the current chronic brain disease model of addiction is the importance of external control over individuals and political correctness and medicalization of addiction is allowing it. Demanding scientific literacy and discriminating good from bad science would prohibit what is occurring and In order to save American Medicine the problem needs to be clearly recognized or we will become a profession that is essentially defined by the impaired physicians movement.




 This infographic on workplace bullying was created by International Business Degree Guide to convey the message that workplace bullies not only hurt people, they can also hurt business–driving away good employees in their quest for control.
This infographic on workplace bullying was created by International Business Degree Guide to convey the message that workplace bullies not only hurt people, they can also hurt business–driving away good employees in their quest for control.



 The
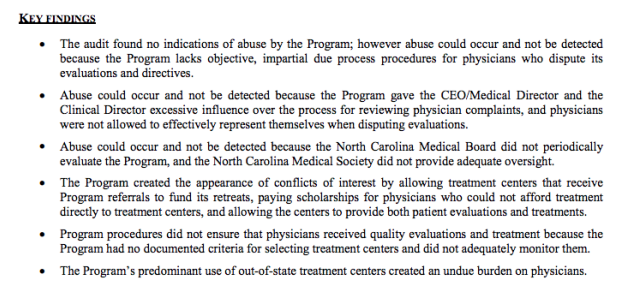
The  The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.  “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.” Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal. What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (
What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (  It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry. Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
 board’s position on the fraudulent practice of medicine is quite clear.
board’s position on the fraudulent practice of medicine is quite clear.



























































 It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong.
It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong. 


 Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition.
Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition. Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add:
Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add: In her
In her 
 Medicalization removes the constitutional safeguards of due process. The potential for abuse is especially the case in the absence of clearly articulated and openly established program policies and procedures.
Medicalization removes the constitutional safeguards of due process. The potential for abuse is especially the case in the absence of clearly articulated and openly established program policies and procedures. In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.
In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.





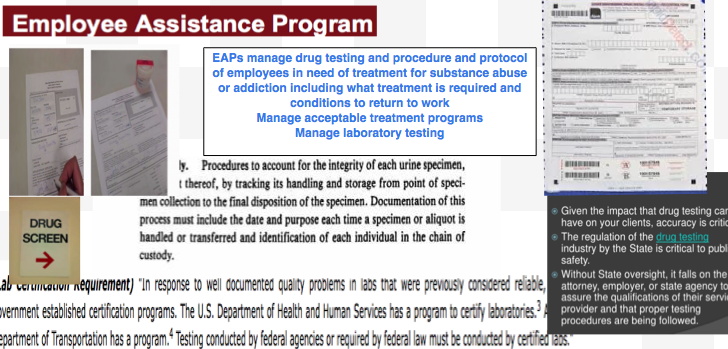
 and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability. PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.
PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.