

The methodology is not new–witches are real, witches are dangerous and witches need to be identified and exterminated at all costs. Convince the authorities to assist you in protecting the public from harm and advance the greater good
In this manner the Federation of State Physician Health Programs (FSPHP) has convinced the Federation of State Medical Boards state medical boards (FSMB) to adopt and enforce policies that have incrementally and systematically increased their own autonomy, scope and power. This began in 1995 when the FSPHP first cultivated a relationship with the FSMB and subsequently took an uninvited seat at the table of power by offering a non-disciplinary “safe harbor” as an alternative to discipline for doctors impaired by drugs or alcohol.
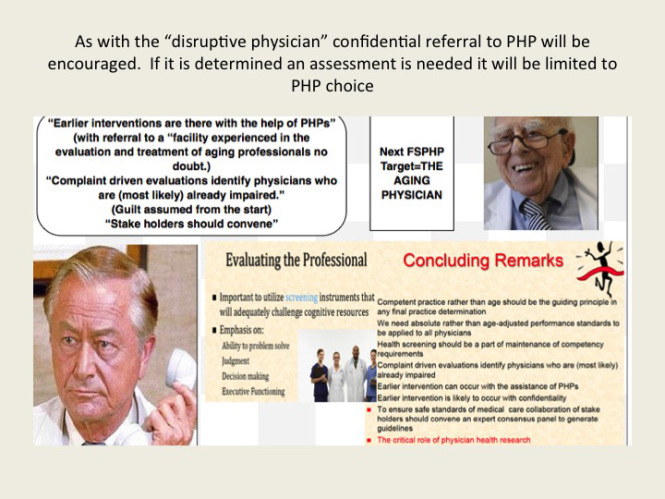
Since then they have increased their scope from the “impaired” to the “disruptive” to everything else. Arising from the “impaired physicians movement” as “addiction specialists” these doctors whose specialty of addiction is not even recognized by the American Board of Medical Specialties have now become the “experts” in all matters related to physician health. Jacks of all trades covering neurology, psychiatry, geriatrics, and occupational medicine.
A 2011 updated FSMB Policy on Physician Impairment states that Medical Boards should recognize the state Physician Heath Program (PHP) as their experts in all matters relating to licensed professionals with “potentially impairing illness,” and these include those potentially impairing maladies that increase as we age. This has gone too far. Isn’t it time we take back the profession of medicine from illegitimate and irrational authority?



As a specialist in geriatric medicine I have experience in taking care of a number of doctors who were referred to me for suspected memory problems. Still operating and teaching residents in his 70s, my first was a well-respected surgeon, a pioneer or Maverick who had made advances in his particular subspecialty. Known for his detailed knowledge of the history of medicine and sharp clinical acumen, he had not seemed himself for a while. His colleagues noted he appeared slower, fatigued and forgetful at times (not remembering his keys, having trouble finding the right word). An internist friend and co-worker who knew him for 50 years curb-sided me and asked if I would see him. He did not have a primary care physician or even seen a doctor professionally for decades (a common phenomenon in this age cohort of doctors).
I met him the next week and he readily admitted to having difficulty concentrating and having trouble with his short term…
View original post 1,533 more words


My concern with the expanding range of substance abuse / mental illness conditions that PHPs allege they are competent to assess is that there is no assurance that the PHP evaluator is in fact either appropriately trained or competent to conduct such an evaluation. Does the evaluator (and here I intentionally avoid the term “clinician”) have adequate training in conducting tests to assess cognitive decline? As they are likely going to err on the side of caution, then that means that any physician about whom a memory or competence issue has been raised and is now deemed to be present by this evaluator is liable to be mandatorily sent for an exhaustive and costly evaluation by one of their “preferred programs.” Is that an appropriate level of intervention? I doubt it.
Further, how can a PHP on the one had assert that they are qualified to conduct these assessments and then on the other hand deny that they are in fact conducting diagnostic assessments? They seem very invested in avoiding acknowledging that the evaluation that they conduct is in fact a medical / psychiatric evaluation. Is this because they want to avoid an allegation of malpractice? That’s very creative but cagey, and I believe wholly dishonest. That’s like doing camp physicals but claiming that they’re not “real” physicals because they’re just a formality required to clear a kid to go to camp.
Do they perhaps avoid taking ownership of this evaluation being a diagnostic psychiatric evaluation so as not to invoke the attention of the IRS as, it would appear, a “public charity” (as many PHPs are incorporated as) chartered to provide education and advocacy is generally not permitted to conduct clinical activities?
Or is it because their diagnostic psychiatric evaluation, which they are denying they are conducting, is actually – by nature of it being compelled by a state licensing authority – a forensic diagnostic psychiatric evaluation and this would then get into the very murky and potentially litigious area of constitutional protection against unlawful search (4th Amendment) and the laws protecting unlawful psychiatric commitment and detention and violation of one’s civil rights?
Whatever it is, I think physicians and medical societies need to demand clarification of the nature of the evaluation being conducted by that PHP – is it a medical/psychiatric evaluation? If not, what is it? If so, what is their authority and qualification to conduct such? And what protections does a physician have in agreeing to such an evaluation – e.g. assurance of due process and “medical due process;” accountability for negligence or worse for bad faith (i.e. unfair or rigged) evaluation; and accountability for conflicts of interest (i.e. via self-serving referral to pre-selected programs which are part of the PHP “preferred” network).
If the board made me see a neurologist for memory concerns, isn’t it fair that I get to see the neurologist of my choosing rather than making me go to a PHP non-clinician evaluator, demanding that I trust that this non-clinical PHP staff person can conduct a sufficiently competent and objective evaluation, at that one whose report it won’t let me see? Likewise for matters of mental illness and substance abuse. (After all, if it’s not really a clinical evaluation and the company whose staff conduct the evaluation is not a licensed medical corporation, what prevents them from allowing recent high school grad Joe Schmoe whose entire knowledge of substance abuse and mental illness comes rom his conversations with his brother who’s had depression and is also in AA to conduct the evaluation?
Please understand, this is not to say that a) there isn’t a need for evaluation and treatment of impaired docs; nor that b) there shouldn’t be PHPs. Clearly docs need evaluation and treatment for a range of conditions, and Boards have a right and a duty to ensure that practitioners are safely practicing when a concern is raised. And clearly, there is a need for an organized program to facilitate this process. The issues here are those of clarification of both the nature of the evaluation and the evaluating entity, their authority and competency to conduct the evaluation, and the assurance of legal fairness and medical honesty, objectivity and integrity. Because erroneously conducted, or worse, done in bad faith, such an evaluation can be career and life threatening to the physician subjected to it.
LikeLiked by 1 person
[…] The Aging Physician—Goodbye Dr. Welby! […]
LikeLike