 Employee Assistance Programs (EAPs)
Employee Assistance Programs (EAPs)
Employee assistance programs (EAPs) evolved from the “industrial” or “occupational” alcohol programs (OAPs) of the 1940s that were developed by companies to address alcohol abuse and its impact on the workplace. The first of these programs was developed by Dupont de Nemours and Company from 1941-1944 followed by Kodak in 1945 (Royce and Scratchley, 1989). These programs were typically staffed by a recovering alcoholic employee working in cooperation with corporate medical departments or a union health clinic and the sole referral source was to the recently formed self-help group Alcoholics Anonymous (AA). The primary intervention was to “confront the alcoholic’s job performance decline and denial using possible job loss as leverage toward seeking help.”
 With time these programs broadened to include other issues that could potentially impact job performance. Worker Assistance Programs (WAPs) emerged in the 1950s when companies such as Consolidated Edison, Standard Oil of New Jersey, and American Cyanamid extended their alcoholism programs to also address mental health issues in their employees (Roman, 1981; Steele, 1995).
With time these programs broadened to include other issues that could potentially impact job performance. Worker Assistance Programs (WAPs) emerged in the 1950s when companies such as Consolidated Edison, Standard Oil of New Jersey, and American Cyanamid extended their alcoholism programs to also address mental health issues in their employees (Roman, 1981; Steele, 1995).
In the 1970s EAP-related legislation was passed and this markedly increased the number of these workplace programs. The Hughes Act ( Public Law 91-616 ) established the National Institute of Alcohol Abuse and Alcoholism (NIAAA) as part of the United States Department of Health and Human Services (USDHHS) and these organizations subsequently developed guidelines applicable to both the public and private sectors. Public Law 92-255 mandated their existence at all federal agencies and military institutions and in 1972 the Hughes Act was amended to also include drug abuse (Public Law 92-255 ). The amendment also required USDHHS Guidelines serve as the model for all federal programs. On September 15, 1986 President Ronald Reagan signed Executive Order 12564 stating a desired goal of achieving a Drug-Free Federal Workplace. This use of drug testing by governmental agencies then led to an increase in drug-testing by private employers and by 1986 more than a quarter of Fortune 500 companies were drug-testing job applicants
 Another significant development was the formation of private EAP firms that began to offer EAP services and drug-testing via contracts with employers. One such example is Bensinger, DuPont & Associates (BDA) which was founded in 1982 by former DEA Chief Peter Bensinger and National Institute on Drug Abuse (NIDA) founding director Robert Dupont. BDA became the sixth largest employee assistance program (EAP) provider in the United States and provided workplace drug testing and other services to some 10-million employees of companies such as Kraft Foods, American Airlines, Johnson & Johnson and the Federal Aviation Administration (FAA). On December 1, 2015 Bensinger, DuPont & Associates was acquired by the Canadian firm of Mourneau Sheppel which employs 4000 plus individuals and has approximately 20,000 clients ranging from small businesses to some of the largest corporations in North America.
Another significant development was the formation of private EAP firms that began to offer EAP services and drug-testing via contracts with employers. One such example is Bensinger, DuPont & Associates (BDA) which was founded in 1982 by former DEA Chief Peter Bensinger and National Institute on Drug Abuse (NIDA) founding director Robert Dupont. BDA became the sixth largest employee assistance program (EAP) provider in the United States and provided workplace drug testing and other services to some 10-million employees of companies such as Kraft Foods, American Airlines, Johnson & Johnson and the Federal Aviation Administration (FAA). On December 1, 2015 Bensinger, DuPont & Associates was acquired by the Canadian firm of Mourneau Sheppel which employs 4000 plus individuals and has approximately 20,000 clients ranging from small businesses to some of the largest corporations in North America.
The company now known as BDA Moreau Sheppel represents the largest employee assistance program (EAP) provider in the entire world.

Ethical Considerations in Workplace Drug-Testing and EAP Management
EAPs can be managed internally by staff employees of a company or organization who contract with outside vendors for drug-testing or externally by an EAP provider such as BDA Moreau Sheppel. The primary goal is to address an employees problem (such as a substance abuse or mental health issue) before that given problem impacts job performance. In this way EAPs are viewed as mutually beneficial; they provide timely help to an employee experiencing a problem in addressing that problem and at the same time potentially avert absenteeism, poor work performance, accidents and termination of a valuable employee. They are designed to help both the employee and the employer in a “win-win” situation. The goals, therefore, should be identical. The goals should be convergent.
Although many of these programs offer mental health counseling and other such services, the core function of EAPs does not include diagnosis or treatment but to facilitate and ascertain diagnosis and treatment. Those referred to EAPs (either through self-referral or by someone else) are assessed and referred to outside sources, either individual practitioners or institutional agencies, that have expertise and experience in assessing and diagnosing the presenting problem. It is the EAP’s function to oversee and make sure that the presenting problem is not only properly assessed, addressed, diagnosed and treated (if indicated) but that the presenting problem remains managed and under control. This requires a period of monitoring or oversight to provide reassurance; progress reports from supervisors, compliance reports from treatment providers, and periodic drug and alcohol testing (if the problem involved substance use) are all part and parcel of a typical EAP.
EAPs have two primary business relationships: 1) a network of individuals and/or programs to which they refer individuals for assessment and treatment, and 2) laboratories capable of performing drug and alcohol testing. The integrity of an EAP is therefore dependent on the integrity and quality of its referral sources and laboratory operations. Those assessing, testing and treating must have education, experience and expertise in assessing, testing and treating the problems presented to them. They must be valid and reliable and it goes without saying that any and all assessment, testing and treatment must be objective, honest and without any conflicts-of-interest.
 This topic is addressed in the book Employee Assistance Programs: What Works and what Doesn’t by Lawrence Mannion in which he discusses the notion of “control” in the context of managed mental health care. For those wishing to control any direction, entity or circumstances pertaining to these types of services Mannion states:
This topic is addressed in the book Employee Assistance Programs: What Works and what Doesn’t by Lawrence Mannion in which he discusses the notion of “control” in the context of managed mental health care. For those wishing to control any direction, entity or circumstances pertaining to these types of services Mannion states:
“..if the ends or purposes of those doing the controlling are in accord with the ends or purposes intrinsic or inherent in the thing being managed there is no conflict.”(page 133).
A 2001 study that looked at EAP professionals perceptions of ethical issues related to their business practices found that 22% of those surveyed identified “referrals” and “ownership structures” as among the most important and critical ethical issues facing the industry (Sharar, White, and Funk, 2001). Many of the respondents expressed concerns that the organizations owning and operating EAPs expected them to generate treatment revenue via a pattern of preferential referral to specific programs or practitioners and were concerned that this financial conflict-of-interest undermined the fundamental obligation of providing “neutral” and “objective” assessments to individuals with problems. To prevent the appearance of unethical conduct the recommendation below were made.
-Fully disclosing (to both employer and client) any affiliations with proposed referral options;
.-Offering an “objective” presentation of more than one referral option to the client;
-Providing clinical justification that the referral is in the best interests of the client;
-Refusing to accept any direct gain or financial remuneration for referring clients;
-Instituting a peer review program to monitor and evaluate the quality and appropriateness of referrals; and
-Developing a utilization/service summary report for employers containing detailed information on patterns of referral for continuing care and treatment.
In 1998 the American Medical Associations Council on Ethical Affairs suggested that incentive programs should be based on quality (rather than quantity) of services or referrals and that linking financial incentives to individual treatment decisions should be avoided (AMA, 1988). In summary any and all referrals need to be objective, honest and fair. They need to be reliable and valid. So too does any and all drug-testing. Most employee drug-testing follows a standardized protocol. Although errors do occur, the procedures followed by the vast majority of employee assistance program providers aim to minimize error. Most programs were implemented and evolved in collaboration with unions or other groups working on behalf of the best interests of the employee.
When drug testing initially entered the workplace many issues had to be worked out. Those in favor of drug-testing insisted that they had the right to demand a drug-free workplace and pointed to decreased productivity, increased accidents and absenteeism as potential consequences of drug abuse. Opponents challenged the constitutionality and reliability of drug-testing and also emphasized the necessity of distinguishing work life from private life. If a person smoked a joint on the weekend, they reasoned, it is no concern of management so long as they performed competently come Monday. Many in the medical community dismissed mandatory drug testing at the time as “chemical McCarthyism.” Nevertheless, drug-testing for better or for worse did enter the workplace. Most of these programs were implemented with the oversight and collaboration of unions or some other group advocating for the rights and interests of those being tested. Procedures and protocols were discussed, deliberated and had to be agreed on before implementation. In his 1984 book Designing Employee Assistance Programs, David Masi emphasizes the need for the close involvement of unions in workplace drug-testing and other EAP services in order to “protect employee rights”as well as the employers responsibilities in doing so (Masi, 1984). Most programs simply followed the already established Federal Workplace Drug Testing Guidelines and this is still the case for most EAPs today. The Mandatory Guidelines for Federal Workplace Drug-Testing Programs provide strict procedure and protocols specifically designed to protect the rights of those being tested. The Department of Transportation (DOT), United States Nuclear Regulatory Commission, and many other safety-sensitive organizations follow these stringent guidelines which include only using certified labs, strict chain-of-custody procedures and Medical Review Officer (MRO) assessment of all positive tests to rule out alternative explanations or “innocent-positives” (such as a prescribed drug). It is also the job of the MRO to verify that strict chain-of-custody was maintained from the collection of the sample to its final analysis. Additionally, only FDA approved drug-testing methods are utilized. This strict protocol assures a high level of validity and reliability (although mistakes can and do occur) to reduce the risk of someone being falsely labeled as a drug or alcohol user. False-positive-tests are absolutely unacceptable as the results of a positive drug-test can be grave, far-reaching and sometimes even permanent.

Physician Health Programs (PHPs)
Physician health programs (PHPs) are basically just employee assistance programs (EAPs) for doctors. They evolved from 1970’s “impaired physicians programs” much like EAPs evolved from the occupational alcohol programs (OAPs) of the 1940s. These programs were designed to both help sick doctors and protect the public in the same manner EAPs were designed to help sick employees and protect a company. The mechanics and mentality should be exactly the same. If the PHP feels a doctor is in need of an assessment he or she is then referred to an outside facility for evaluation (and treatment if that is indicated and in this system “treatment” is virtually guaranteed. The PHP then monitors the doctor for a period of time (typically five-years) to make sure that the problem remains under control. Monitoring inevitably includes at least weekly abstinence based substance abuse testing (including alcohol) using non-FDA approved laboratory developed tests (LDTs) no matter what the presenting problem. As with EAPs, one can self-refer to these programs or be referred by someone else and the latter can be done anonymously and with guaranteed confidentiality for the referrer.
In the context of PHPs being EAPs for doctors, the Federation of State Physician Health Programs (FSPHP) functions in the same manner as an EAP provider. The FSPHP s a non-profit corporation formed in 1990 to promote best-practices in state PHPs and influence policy. This EAP for doctors is being called the “PHP-blueprint”.
Although this model of EAP management is currently just being used on doctors, nurses, and other health care professionals; parts of the criminal justice system; and some areas of the airline industry, the grand plan is to move this model of care to other populations. Moving the “PHP-blueprint” to other occupations and populations is what is being deemed the “New Paradigm.”
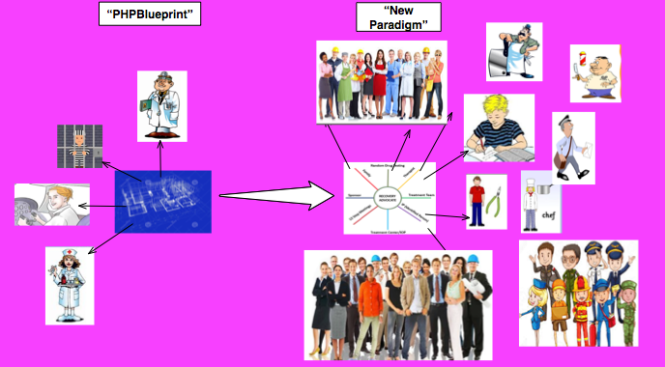
The “PHP-blueprint” and the “New Paradigm”
The American Society of Addiction Medicine (ASAM) White Paper on Drug Testing describes the current practice of drug-testing in various contexts and explains how physicians and other healthcare providers can “use drug-testing to discourage non-medical drug use and ‘diversion’ of controlled substances” to “encourage appropriate entry into addiction treatment,” identify relapse and “improve outcomes of addiction treatment” through the use of “long-term post treatment monitoring.” The paper proposes random mandatory drug-testing by medical professionals (pediatricians to obstetricians to geriatricians) using not only urine but blood, oral fluid (saliva), hair, nails, sweat and breath.”
 The White Paper’s writing Committee Chair, Dr. Robert Dupont, described this “New Paradigm” in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) in 2012 and claimed this model “sets the standard for effective use of drug testing” (Dupont, Drug Testing and the Future of American Drug Policy 2012) Dupont then proposed the “PHP-blueprint” be expanded to other workplace populations, healthcare students and schools. His audience, the Drug and Alcohol Testing Industry Association (DATIA) represents more than 1,200 companies involved in the drug and alcohol testing industry for profit and even employs their own DC-based lobbying firm, Washington Policy Associates.
The White Paper’s writing Committee Chair, Dr. Robert Dupont, described this “New Paradigm” in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) in 2012 and claimed this model “sets the standard for effective use of drug testing” (Dupont, Drug Testing and the Future of American Drug Policy 2012) Dupont then proposed the “PHP-blueprint” be expanded to other workplace populations, healthcare students and schools. His audience, the Drug and Alcohol Testing Industry Association (DATIA) represents more than 1,200 companies involved in the drug and alcohol testing industry for profit and even employs their own DC-based lobbying firm, Washington Policy Associates.
In a 2012 article entitled “Six lessons from state physician health programs to promote long-term recovery” Dupont and co-author Dr. Greg Skipper describe the need to”reach more of the 1.5 million Americans who annually enter substance abuse treatment stating that:
“This model of care management for substance use disorders has been pioneered by a small and innovative group of the nation’s physicians in their determination to help other physicians save their careers and families while also protecting their patients from the harmful consequences of continued substance abuse. In fulfilling the professional admonition “physician: first heal thyself,” these physicians have created a model with wide applicability and great promise.” (Dupont, R., Skipper, G. 2012)
 These six lessons are:
These six lessons are:
(1) zero tolerance for any use of alcohol and other drugs;
(2) thorough evaluation and patient-focused care;
(3) prolonged, frequent random testing for both alcohol and other drugs;
(4) effective use of leverage;
(5) defining and managing relapses; and
(6) the goal of lifelong recovery rooted in the 12-Step fellowships.
 The “PHP-blueprint” is being promoted as “Gold standard” and a “New Paradigm” of recovery. In other words it is being proposed that the model of care management currently being used on doctors and managed by the FSPHP replace your current EAP. And like a faulty smoke-detector or a misfired Epipen you won’t realize or possibly even care about it until it happens.
The “PHP-blueprint” is being promoted as “Gold standard” and a “New Paradigm” of recovery. In other words it is being proposed that the model of care management currently being used on doctors and managed by the FSPHP replace your current EAP. And like a faulty smoke-detector or a misfired Epipen you won’t realize or possibly even care about it until it happens.
The question for us, then, is this:
Are the ends or purposes of those managing physician health programs the same as or in accordance with those being managed by these programs?
Moreover, will the ends and purposes of the physician health model of care be in accordance with the ends and purposes of those who will potentially be managed by this model of care in the “New Paradigm?
The answer to the first question is a resounding “NO.” Complaints of coercion, abuse and other misconduct and fraud are rampant. Doctors are, in fact, being diagnosed with substance use disorder and other problems when they do not meet the diagnostic criteria for substance use disorder or other problems and being forced into unnecessary and unneeded treatment while those who do have substance use disorders and mental illness are being provided cookie-cutter treatment that is often inappropriate and inadequate treatment. Why? The money of course. Do the homework and follow the money.
It is necessary that we conform our thinking and behavior to objective reality rather than an illusion and the version of the physician health model being put forth by those promoting the “PHP-blueprint” and the “New Paradigm”is at marked variance to those being managed by the model and for further reading start with the following:
- British Medical Journal feature “Physician health programs under fire” by Jeanne Lenzer
- The “PHP-Blueprint”–A Trojan Horse for Profit and Wider Social Control: Watching helplessly, as Cassandra did, while the soldiers emerge and wreak their predicted havoc.
- “New Paradigm” is a business model not a medical model
- Physician Suicide and “Physician Wellness” –Time to start talking about the elephant in the room!
In Employee Assistance Programs: What Works and what Doesn’t, Mannion states:
“We need to spend less time making hyperbolic statements about change and entertaining grandiose ideas about strategic alliances and more time developing criteria or standards to determine what does and what does not belong under the canopy of employee assistance. More specifically what is that principle or principles on the basis of which we can develop a criterion or criteria to determine those activities that could legitimately come under the heading of employee assistance?” (page 165-166)
.
REFERENCES
American Medical Association, Council on Ethical and Judicial Affairs. Reports on Ethics in ManagedCare.Chicago, Ill.: American Medical Association Press, 1998
Dupont, R and G. Skipper “Six Lessons from State Physician Health Programs to Promote Long Term Recovery” Journal of Psychoactive Drugs 44 (1) 2012 (72-78)
Dupont, R. “Drug Testing and the Future of American Drug Policy” Presentation at the DATIA Annual Conference. San Antonio, Texas. April 19, 2012.
Jett K. Employee Assistance Programs–Government’s Role in an Expanding Field. In: Mecca AM, ed. Prevention 2000–A Public/Private Partnership: CHRF:69-81.
Manion, L. “Employee Assistance Programs: What Works and What Doesn’t” Praeger, Westport, CT. 2004
Massi, D. Designing Employee Assistance Programs. American Management Associations, New York, NY 1984
Roman P. From Employee Alcoholism to Employee Assistance. Journal of studies on alcohol. 1981;42(3):244-272.
Royce JE, Scratchley D. Alcoholism and Other Drug Problems: A Revised Edition of Alcohol Problems and Alcoholism. New York, NY: Simon & Schuster, Inc.; 1989.
Sharar D, W White, and R. Funk. “Business ethics and employee assistance/managed behavioral healthcare: A national survey of issues and challenges.” Journal of Behavioral Health Services and Research (submitted for peer review and publication April 2001).
Sharar, D., and W. White “Referrals and Ownership Structures: The first of two articles on the need for a revised ethic in employee assistance considers whether ownership structures can improperly influence EAP professionals.”
Steele P, Trice H. A History of Job Based Alcoholism Programs: 1955-1972. Journal of Drug Issues. 1995;19:511-532.
The New Paradigm for Recovery Making Recovery-and Not Relapse-the Expected Outcome of Addiction Treatment. Washington, D.C. March 2014 2014.
Making some serious gains. Let’s not lose the momentum. Please donate to my Gofundme here






















 also follow their own
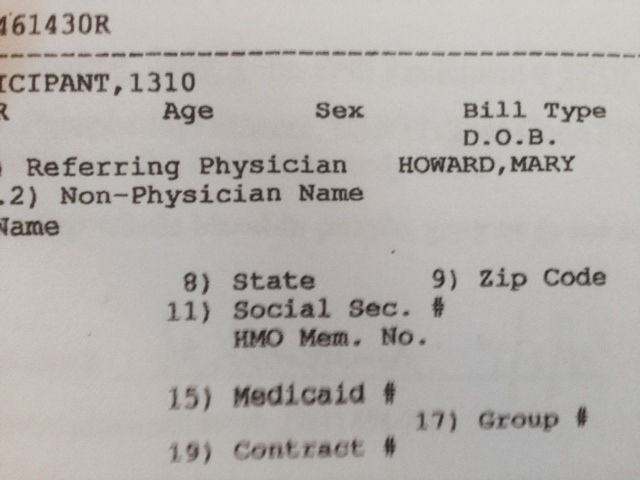
also follow their own  Both the donor ID # and chain of custody are listed as 461430.
Both the donor ID # and chain of custody are listed as 461430.





















 The majority of doctors are of good heart and sound mind. Most doctors strive to do the right thing and the correct thing to the best of their capabilities in any given circumstance. Most doctors by nature are intelligent, inquisitive and caring. Their actions are not driven by self-interest or greed but by thoughtful reasoning and moral compass. As in any population, of course, vast differences exist in individual characteristics including intellectual acumen, empathy and common sense. Those bereft of moral compass and the intolerant and prejudiced walk among us in all professions. Medicine is no exception. The simple truth to the matter is overwhelming majority of people are good people. They are honest, have integrity and are guided by conscience. Most police officers are not trigger-happy racists. Most Catholic priests do not have an affinity for alter-boys. And most doctors do not hand out opiates like halloween candy. What we hear about are the exceptions not the rule.
The majority of doctors are of good heart and sound mind. Most doctors strive to do the right thing and the correct thing to the best of their capabilities in any given circumstance. Most doctors by nature are intelligent, inquisitive and caring. Their actions are not driven by self-interest or greed but by thoughtful reasoning and moral compass. As in any population, of course, vast differences exist in individual characteristics including intellectual acumen, empathy and common sense. Those bereft of moral compass and the intolerant and prejudiced walk among us in all professions. Medicine is no exception. The simple truth to the matter is overwhelming majority of people are good people. They are honest, have integrity and are guided by conscience. Most police officers are not trigger-happy racists. Most Catholic priests do not have an affinity for alter-boys. And most doctors do not hand out opiates like halloween candy. What we hear about are the exceptions not the rule. What might Nash think of a population in which this minority of deviants was not punished for their actions but instead given “treatment” in a communal area where they were able to interact with others of the same constitution ? What do you think Nash might say if individually and collectively this same population was put in a position of power over others but without any oversight, regulation or accountability? A disequilibrium would inevitably ensue with grave complications to the rest.
What might Nash think of a population in which this minority of deviants was not punished for their actions but instead given “treatment” in a communal area where they were able to interact with others of the same constitution ? What do you think Nash might say if individually and collectively this same population was put in a position of power over others but without any oversight, regulation or accountability? A disequilibrium would inevitably ensue with grave complications to the rest. Coraline is a children’s novella written by the British author Neil Garman in 2002. It has been compared to Lewis Carroll’s Alice’s Adventures in Wonderland and adapted into a film in 2009. Coraline is a little girl who moves into a new house with her parents. She is constantly bored and unhappy her parents do not give her the attention she wants and while exploring the house she finds a door that leads to an alternate version of her reality where her parents are fun and attentive and everything seems wonderful but things get creepy very quickly. Her parents look like her parents but instead of their eyes they have shiny black buttons and she soon finds herself in a horrific and dark place that looks like reality but slightly off and terribly ominous and threatening. Such is the case with the medical profession today. Somewhere along the line it took a nasty left turn and although looks the same its slightly off nature has become threatening and crippling to many. An erosion in the hierarchy has occurred and much of the practice and policy pushed by the self-interest groups to regulators and administrators is not only bad, it is absurd.
Coraline is a children’s novella written by the British author Neil Garman in 2002. It has been compared to Lewis Carroll’s Alice’s Adventures in Wonderland and adapted into a film in 2009. Coraline is a little girl who moves into a new house with her parents. She is constantly bored and unhappy her parents do not give her the attention she wants and while exploring the house she finds a door that leads to an alternate version of her reality where her parents are fun and attentive and everything seems wonderful but things get creepy very quickly. Her parents look like her parents but instead of their eyes they have shiny black buttons and she soon finds herself in a horrific and dark place that looks like reality but slightly off and terribly ominous and threatening. Such is the case with the medical profession today. Somewhere along the line it took a nasty left turn and although looks the same its slightly off nature has become threatening and crippling to many. An erosion in the hierarchy has occurred and much of the practice and policy pushed by the self-interest groups to regulators and administrators is not only bad, it is absurd. My hero’s in medicine both historically and personally have always been the maverick’s -those doctors with superlative and almost preternatural clinical acumen who can make the right diagnosis when no one else could or have made daring and unprecedented contributions to the field.
My hero’s in medicine both historically and personally have always been the maverick’s -those doctors with superlative and almost preternatural clinical acumen who can make the right diagnosis when no one else could or have made daring and unprecedented contributions to the field.
 Authority needs to be grounded in wisdom and guided by ethical principles and codes of conduct.
Authority needs to be grounded in wisdom and guided by ethical principles and codes of conduct. 



 The
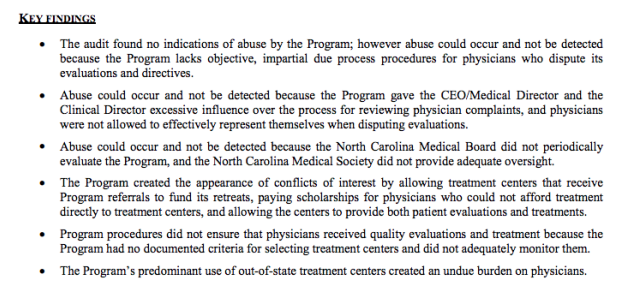
The  The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.  “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
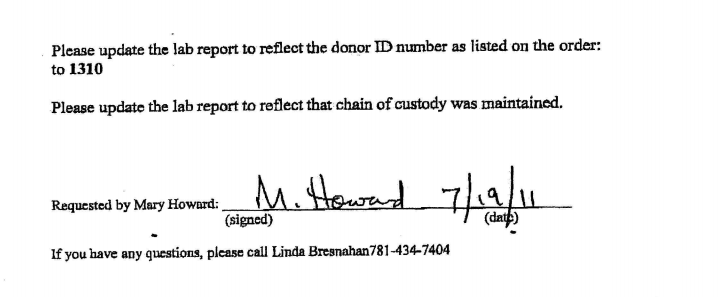
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.” Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
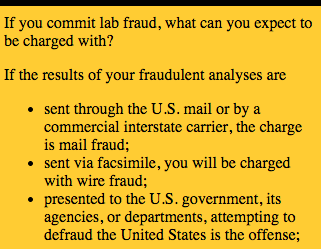
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal. What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (
What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (  It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry. Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
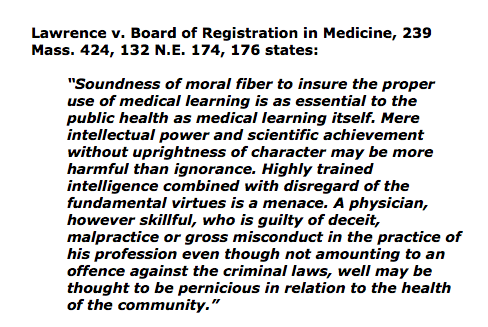
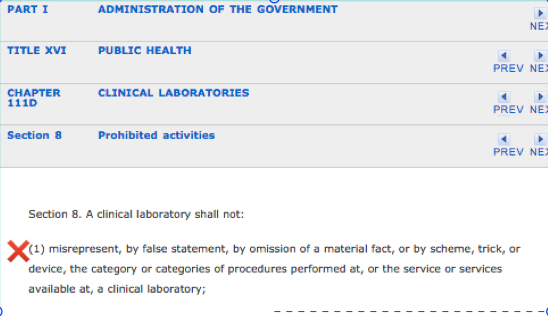
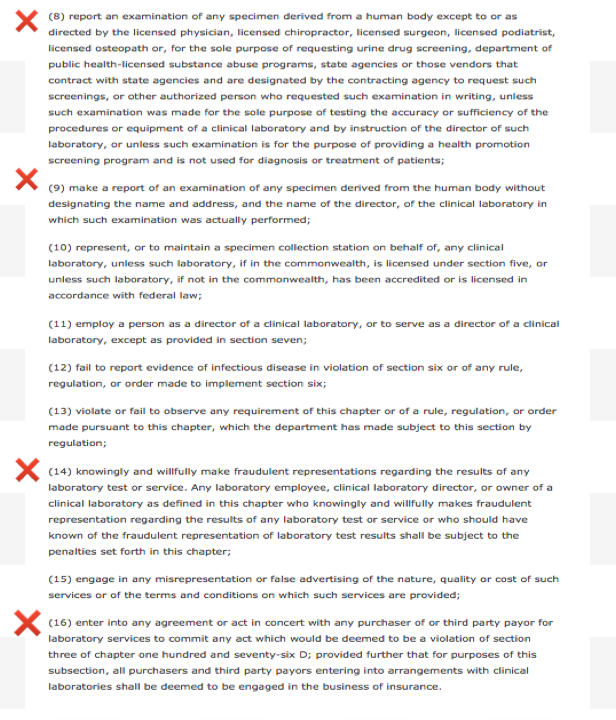
 board’s position on the fraudulent practice of medicine is quite clear.
board’s position on the fraudulent practice of medicine is quite clear.



























































 It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong.
It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong. 


 Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition.
Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition. Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add:
Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add: In her
In her 
 In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.
In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.

 As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.








{kind=link}
{kind=link}