

Milton Friedman (July 31, 1912 – November 16, 2006) was an American economist who received the 1976 Nobel Memorial Prize in Economic Sciences
In an article written for the March 2015 Physician Health News, the official newsletter of the Federation of State Physician Health Programs (FSPHP) President Doris Gunderson reviews the history of the organization in honor of its 25th anniversary. She writes:
“In 1990 the FSPHP was born out of a need for individual state programs to work together in discussing and promoting best practices and especially to influence national public policy.”
For the last quarter century the FSPHP has pushed a plethora of both practice and policy (legal, regulatory and healthcare) that claims to assist state physician health programs in identifying, managing and monitoring impaired physicians and protect the public from harm.It was recently suggested by the Chief Editor of American Society of Addictions Medicine (ASAM) Weekly News that this same group take the helm in influencing public policy for addiction medicine at large (i.e. not just doctors but everyone from our kids to our pregnant mothers to our elderly) on a national organizational level.
It is time we examined both the authority and the knowledge claims on which they are based.
In her rebuttal to Pauline Anderson’s August 2015 Medscape article ‘Physician Health Programs: More Harm Than Good? Gunderson dismissed criticisms as “allegations rather than facts” and “second hand anecdotes.”
In response to allegations that PHPs have no oversight Gunderson comments:
“In fact, we operate under a microscope, answering to individual practitioners, medical boards, malpractice carriers, defense attorneys, state attorneys, medical societies, hospitals, medical schools and residency training programs. We are also accountable to patient safety entities and a Board of Directors.”
The list of organizations Gunderson has to “answer” to appears to be many of the organizations and societies that physician health programs interact with. She might as well add Blockbuster for getting her videos back on time. This is not meaningful oversight. Oversight equates with accountability and that requires answerability (the provision of information) and justification for one’s actions. It also requires the presence of an outside organization truly independent of the group that is able to sanction or punish individuals for wrongdoing or misconduct. No such organization exists for state physician health programs. Period. There is no organization that exists that is able to investigate a complaint of misconduct and provide sanctions. The same applies to their primary business associates, the assessment and treatment centers (because they are private pay and out-of-pocket) and drug and alcohol testing labs (because they use non-FDA approved tests). The entire racket is unaccountable and unexamined.
Kathryn Pyne Addelson warned that what we should fear most is “unexamined” authority. “Illegitimate politicization and rampant irrationality find their most fruitful soil when our activities are mystified and protected from criticism.”
This group has been protected from criticism for the better part of a generation. They have enjoyed making authoritative pronouncements as unexamined authority. Their power depends entirely on not being questioned as what is behind the curtain is flimsy and dredged, a Potemkin village. The recent Medscape and BMJ articles are revealing that confrontation with direct and precise questions results in nothing but logical fallacy, distortions and lies. They are utterly incapable of responding with a direct and precise answer. Gunderson’s response to absent oversight is just another example of this logical fallacy and distortion. This is not how rational authority responds. This is not how legitimate authority responds. I kindly invite her to debate this. I would like a back-and-forth to clarify. It is a simple question that deserves a simple answer and I know she follows my blog as she used her own name and e-mail address.
The cumulative comments on the articles critical of these programs are revealing a system of oppressions, injustices and illusions. A more recent article on Medscape, “One-Man Fight: MD Takes on State Medical Board, PHP” reports the same pattern of coercion, absence of due process and diagnosis rigging for sham peer review that I am hearing from doctors across the country. The comments section to this article are also overwhelmingly critical of PHPs. They are pertinent, articulate and precise and missing from them is any semblance of a rebuttal by the FSPHP, their apologists or anyone else. The writing is on the wall as they say. And for that reason we call upon all those of good will in both the medical profession and the public at large to join us in this confrontation with illegitimate, irrational and immoral authority.
- Gunderson D. Message From the President Twenty-Five Years: A Remarkable Journey. Physician Health News. 2015;20(March).
- Addelson KP. The Man of Professional Wisdom. In: Fonow MM, Cook JA, eds. Beyone Methodology: Feminist Scholarship as Lived Research. Bloomington: Indiana University Press; 1991:16-35.
Federation of State Physician Health Programs



Investigative Journalists Take Note-A Spotlight Opportunity to Expose Corruption!

Physician Health Programs Under Fire (Link to BMJ article by Jeanne Lenzer)
The attached article was published in the June 30, 2016 edition of the British Medical Journal. The BMJ is one of the oldest and most respected medical publications in the wold and the Associate Editor of the BMJ Jeanne Lenzer wrote it. The article speaks for itself and it should be noted that former FSPHP president Warren Pendergast “retired”on the same day this article was published. Although the monopolistic abuses and horror stories of doctors have been percolating around medical circles they have not yet reached the mainstream media and they need to.
Physician Health Programs (PHPs) were designed to provide timely professional help to doctors who developed problems that might otherwise lead to work impairment that could cause patient harm. They are similar to employee assistance programs (EAPs) and the central purpose of an EAP is to provide timely professional aid for employees who have problems that might otherwise lead to work impairment, absenteeism or job loss.
What they have become is a multi-state criminal operation involving state PHPs, several drug testing labs and close to two dozen “PHP-approved” drug and alcohol treatment centers across the US.
Although the mechanics of EAPs and PHPs are the same the mentality is quite different. Any system can be subverted, but as cleanly-coined self-governing organizations with no oversight or regulation and started by volunteers with benevolent intentions PHPs were particularly vulnerable to exploitation. This was accomplished when some unscrupulous individuals from the “impaired physicians movement” started creeping into state PHPs. Many of the doctors who who orchestrated this system were former alcoholics or drug addicts who regained their licenses after completing treatment and were now in “recovery.” Normally that would be a good thing but many of the doctors who erected the FSPHP scaffold had long histories of manipulating the system and claiming “recovery” was their get out of jail free card. Some very bad people were able to slip through the cracks and joined their state PHPs and eventually took them over while at the same time bamboozling others into the belief they were just altruistic do-gooders who actually knew what they were talking about.
The Federation of State Physician Health Programs (FSPHP) is a monopoly power of abuse It is both an illegitimate and irrational authority that neither represents the interests of doctors nor the public. It is a false construct designed to advance the interests of the drug and alcohol testing, assessment and treatment industry.
By selling the “PHP-blueprint” to other EAPs as the “New Paradigm” they are able to sell with it the dozens of junk-science non-FDA approved drug tests that go along with it. It can be compared to the razor model — sell a razor cheaply and mark up the razor blades. Rather than making a one-time profit on the razor, you’ll make continuing profit as the customer keeps buying razor blade replacements—or the rotating panel of urine, hair, blood, and saliva testing described in the ASAM White Paper in this case.
In reality the FSPHP is a façade; a Potemkin village with a foundation of sand that brandishes “research” of little probative value and relies on unquestioned authoritative opinion and the blind faith of others. This is underscored by the comments of current FSPHP President Doris C Gunderson who told The BMJ that the federation is concerned that publicity about “a small, dissatisfied minority of physicians who were not able to achieve a successful return to their profession,” could drive doctors away from programs that are helping them.
As a false authority in power the FSPHP primarily depends on silence, secrecy and avoiding facts and critical reasoning. They do not operate visibly, predictably or understandably and refuse to provide direct simple answers to direct simple questions. The chink in their armor is confrontation with direct facts and this was seen with state Auditor Beth Wood’s Audit of the North Carolina PHP that is mentioned in the BMJ article and found to have holes “big enough to drive a truck through”.
A 2011 American Society of Addiction Medicine (ASAM) public policy statement specifically states that doctors should only be referred and assessed at “PHP-approved” centers and also excludes non “PHP-approved assessment and treatment centers. State medical boards mandate that doctors be assessed at “PHP-approved” assessment and treatment centers under threat of loss of licensure. This is under the ruse that these facilities have “special knowledge” and that doctors are unique but when Auditor Wood’s asked Warren Pendergast what criteria went into PHP approval of “PHP-approved” facilities the then President of the FSPHP could not give an answer. The best he could come up with is “word of mouth” and “reputation.” This emperor has no clothes. It is all artificiality and farce; spider thread spun out of the minds of profiteers to make the data fit the hypothesis and sell the “PHP-blueprint” and the multiple non-FDA approved drug and alcohol testing that goes along with it.
 Gunderson’s “mere fools” logical fallacy is alarming considering the complaints involve false diagnoses, overdiagnoses, diagnosis rigging, forensic fraud, coercion, control and other abuses of power. Human rights violations involving the political abuse of psychiatry need to be addressed directly.
Gunderson’s “mere fools” logical fallacy is alarming considering the complaints involve false diagnoses, overdiagnoses, diagnosis rigging, forensic fraud, coercion, control and other abuses of power. Human rights violations involving the political abuse of psychiatry need to be addressed directly.
Delegitimizing one’s opponent to avoid addressing the substance of the argument is an unacceptable response considering the gravity of the issues presented. Faith in institutions demands mass adherence to faith in that authority and the FSPHP has bamboozled their key stakeholders into blinkered head-in–the sand complacency. It is important to recognize that the unique role of discrediting opinion and dehumanizing those with one whom disagrees is not limited to totalitarian regimes and the coercive use of psychiatry represents a violation of basic human rights in all cultures.
Corruption breeds in opacity: in a crystal clear world of full information there would be no possibilities to circumvent existing rules in order to derive benefits for own pockets.

Direct challenges to the status quo are necessary. We need to critically question the validity of their research involving PHPs and the toxicology testing. A public-policy and conflict of interest analysis need to be done. The profession needs to be informed, concerned and engaged. We need to question this authority and demand direct answers.
Dissenting voices that are all too frequently met with a wall of blinkered apathy or openly dismissed or opposed by those who are unable or unwilling to look any deeper. As with the trees impeding to see the forest the FSPHP has successfully hidden themselves under authoritative pronouncements and a veneer of superficialities. So investigative journalists there is a treasure trove beneath this rock waiting to be discovered and we need to shine more light in an a dark dank area that is seldom seen.

Share this:

The Federation of State Physician Health Programs and the Dead Doctors at Ridgeview-A Harbinger of the Medical Profession’s Current Suicide Epidemic
“There is enormous inertia—a tyranny of the status quo—in private and especially governmental arrangements. Only a crisis—actual or perceived—produces real change. When that crisis occurs, the actions that are taken depend on the ideas that are lying around. That, I believe, is our basic function: to develop alternatives to existing policies, to keep them alive and available until the politically impossible becomes politically inevitable.” –Milton Friedman

“Gentlemen, it is a disagreeable custom to which one is too easily led by the harshness of the discussions, to assume evil intentions. It is necessary to be gracious as to intentions; one should believe them good, and apparently they are; but we do not have to be gracious at all to inconsistent logic or to absurd reasoning. Bad logicians have committed more involuntary crimes than bad men have done intentionally.”–Pierre S. du Pont (September 25, 1790)
“It is easier to believe a lie one has heard a hundred times than a truth one has never heard before.” –Robert S. Lynd
Ridgeview Institute was a drug and alcohol treatment program for “impaired physicians” in Georgia created by G. Douglas Talbott, a former cardiologist who lost control of his drinking and recovered through the 12-steps of Alcoholics Anonymous.
Up until his death on October 18, 2014 at the age of 90, Talbott owned and directed a number of treatment facilities for impaired professionals, most recently the Talbott Recovery Campus in Atlanta, one of the preferred referrals for physicians ordered into evaluation and treatment by licensing boards today.
G. Douglas Talbott is a prototypical example of an “impaired physician movement” physician–in fact in many ways he may be considered the”godfather” of the current organization. He helped organize and serve as past president of the American Society of Addiction Medicine (ASAM) and was a formative figure in the American Medical Association’s (AMA’s) Impaired Physician Program.

G. Douglas Talbott (center), with sons Mark (left) and Dave (right). (image: Ham Biggar)
The cost of a 28-day program for nonprofessionals at Ridgeview in 1987 was $10,000 while the cost was “higher for those going through impaired-health professionals program,” which lasted months rather than 28 days.1
In 1975 after creating the DeKalb County Impaired Physicians Committee for the Medical Association of Georgia, Talbott founded the Georgia Disabled Doctors Program for the assessment and treatment of physicians. Founded in part because “traditional one-month treatment programs are inadequate for disabled doctors,” and they required longer treatment to recover from addiction and substance abuse. According to Talbott, rehabilitation programs that evaluate and treat the rest of the population for substance abuse issues are incapable of doing so in doctors as they are unlike any other of the inhabitants of our society. Physicians are unique. Unique because of their incredibly high denial”, and he includes this in what he calls the “Four MDs,” “M-Deity”, “Massive Denial” “Militant Defensiveness” and “More Drugs.”2 And these factors set doctors apart from the rest.
According to Talbott, “impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.” “Terminal uniqueness “ is a phrase Talbott uses to describe doctors’ tendency to think they can heal themselves.
“M-Deity” refers to doctors “being trained to think they’re God;”3 blinded by an overblown sense of self-importance and thinking that they are invincible-an unfounded generalization considering the vast diversity of individuals that make up our profession. Although this type of personality does exist in medicine, it is a small minority -just one of many opinions with little probative value offered as factual expertise by the impaired physician movement and now sealed in stone.

Former Assistant Surgeon General (Ret) Admiral (Ret) John C. Duffy
This attitude, according to some critics, stems from the personal histories of the treatment staff, including Talbott, who are recovering alcoholics and addicts themselves. One such critic was Assistant Surgeon General under C. Everett Koop John C. Duffy who said that Ridgeview suffered from a “boot-camp mentality” toward physicians under their care and “assume every physician suffering from substance abuse is the same lying, stealing, cheating, manipulating individual they were when they had the illness. Certainly some physicians are manipulative, but it’s naïve to label all physicians with these problems.”1

LeClair Bissell
American Society of Addiction Medicine (ASAM) President (1981-1983) LeClair Bissell was also highly critical of Talbott’s approach. Bissell, co-author of the first textbook of ethics for addiction professionals4 when asked if there was any justification to the claim that doctors are sicker than other people and more vulnerable to addiction replied:
“Well, based on my treatment experience, I think they are less sick and much easier to treat than many other groups. I think one reason for that is that in order to become a physician…one has to have jumped over a great many hurdles. One must pass the exams, survive the screening tests and the interviews, be able to organize oneself well enough to do examinations and so on, and be observed by a good many colleagues along the way. Therefore I think the more grossly psychotic, or sicker, are frequently screened out along the way. The ones we get in treatment are usually people who are less brain-damaged, are still quite capable of learning, are reasonably bright. Not only that, but they are quite well motivated in most cases to hang on to their licenses, the threat of the loss of which is frequently what puts them in treatment in the first place. So are they hard to treat? No! Are they easy patients? Yes! Are they more likely to be addicted than other groups? We don’t know.”5“I’m not much for the bullying that goes along with some of these programs,” Bissell commented to the Atlanta Journal and Constitution in 1987.3
The constitution did a series of reports after five inpatients died by suicide during a four-year period at Ridgeview.6 In addition there were at least 20 more who had killed themselves over the preceding 12 years after leaving the treatment center.1
Bissell, the recipient of the 1997 Elizabeth Blackwell Award for outstanding contributions to the cause of women and medicine remarked: “When you’ve got them by the license, that’s pretty strong leverage. You shouldn’t have to pound on them so much. You could be asking for trouble.”3
According to Bissell: “There’s a lot of debate in the field over whether treatment imposed by threats is worthwhile…To a large degree a person has to seek the treatment on his own accord before it will work for him.”3
A jury awarded $1.3 million to the widow of one of the deceased physicians against Ridgeview,7 and other lawsuits initiated on behalf of suicides were settled out of court.6
The Constitution reported that doctors entered the program under threats of loss of licensure “even when they would prefer treatment that is cheaper and closer to home.” 8 The paper also noted that Ridgeview “enjoys unparalleled connections with many local and state medical societies that work with troubled doctors,” “licensing boards often seek recommendations from such groups in devising an approved treatment plan,” and those in charge are often “physicians who themselves have successfully completed Ridgeview’s program.”8
In 1997 William L. White interviewed Bissell whom he called “one of the pioneers in the treatment of impaired professionals.” The interview was not published until after her death in 2008 per her request. Noting that her book Alcoholism in the Professions9 “remains one of the classics in the field”, White asked her when those in the field began to see physicians and other professionals as a special treatment population; to which she replied:
“When they started making money in alcoholism. As soon as insurance started covering treatment, suddenly you heard that residential treatment was necessary for almost everybody. And since alcoholic docs had tons of money compared to the rest of the public, they not only needed residential treatment, they needed residential treatment in a special treatment facility for many months as opposed to the shorter periods of time that other people needed.”10
Talbott claimed a “92.3 percent recovery rate according to information compiled from a five-year follow-up survey based on complete abstinence and other treatment.”11 A 1995 issue of The Federal Bulletin: The Journal of Medical Licensure and Discipline, published by the Federation of State Medical Boards, contains articles outlining impaired physician programs in 8 separate states. Although these articles were little more than descriptive puff-pieces written by the state PHP program directors and included no described study-design or methodology the Editor notes a success rate of about 90% in these programs and others like them 12 and concludes:
“cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” 12No one bothered to examine the methodology to discern the validity of these claims and it is this acceptance of faith without objective assessment that has allowed the impaired physician movement through the ASAM and FSPH to advance their agenda; confusing ideological opinions with professional knowledge.
“There is nothing special about a doctor’s alcoholism,” said Bissel
“These special facilities will tell you that they come up with really wonderful recovery rates. They do. And the reason they do is that any time you can grab a professional person by the license and compel him or her into treatment and force them to cooperate with that treatment and then monitor them for years, you’ll get good outcomes—in the high 80s or low 90s in recovery rates—no matter what else you do.”10 “The ones I think are really the best ones were not specialized. There were other well-known specialty clinics that claimed all the docs they treated got well, which is sheer rot. They harmed a great many people, keeping them for long, unnecessary treatments and seeing to it that they hit their financial bottom for sure: kids being yanked out of college, being forced to sell homes to pay for treatment, and otherwise being blackmailed on the grounds that your husband has a fatal disease. It’s ugly.”10Stanton Peele’s “In the Belly of the American Society of Addiction Medicine Beast” describes the coercion, bullying, threats and indoctrination that are standard operating procedure in Talbott’s facilities.13 Uncooperative patients, “and this covers a range of sins of commission or omission including offering one’s opinion about one’s treatment,” are “threatened with expulsion and with not being certified-or advocated for with their Boards.”13
The cornerstone of treatment is 12-step spiritual recovery. All new patients are indoctrinated into A.A. and coerced to confess they are addicts or alcoholics. Failure to participate in A.A. and 12-step spirituality means expulsion from the program with the anticipated result being loss of one’s medical license.
In May 1999 Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for fraud, malpractice, and the novel claim of false imprisonment.14
The fraud finding required a finding that errors in the diagnosis were intentional. Masters, who was accused of overprescribing narcotics to his patients was told by the director of the Florida PHP that he could either surrender his medical license until the allegations were disproved or submit to a four-day evaluation.
Masters agreed to the latter, thinking he would have an objective and fair evaluation. He was instead diagnosed as “alcohol dependent” and coerced into “treatment under threat of loss of his medical license. Staff would routinely threaten to report any doctor who questioned any aspect of their diagnosis or treatment to their state medical boards “as being an impaired physician, leaving necessary treatment against medical advice,”14 the equivalent of professional suicide.
Masters, however, was not an alcoholic.
According to his attorney, Eric. S. Block, “No one ever accused him of having a problem with alcohol. Not his friends, not his wife, not his seven children, not his fellow doctors, not his employees, not his employers, No one.” 15
He was released 4 months later and forced to sign a five-year “continuing care” contract with the PHP, also under continued threat of his medical license.
Talbott faced no professional repercussions and no changes in their treatment philosophy or actions were made. They still haven’t. They have simply tightened the noose and taken steps to remove accountability.
Up until his recent death, Talbott continued to present himself and ASAM as the most qualified advocates for the assessment and treatment of medical professionals for substance abuse and addiction.16
ASAM and like-minds still do.
In most states today any physician referred for an assessment for substance abuse will be mandated to do so in a facility just like Ridgeview.
There is no choice. In mechanics and mentality, this same system of coercion, control, and indoctrination has metastasized to almost every state only more powerful and opaque in an unregulated gauntlet protected from public scrutiny, answerable and accountable to no one. Laissez faire Machiavellian egocentricity unleashed. For what they have done is taken the Ridgeview model and replicated it over time state by state and tightened the noose. By subverting the established Physician Health Programs (PHPs) started by state medical societies and staffed by volunteer physicians they eliminated those not believing in the mentality of the groupthink. They then mandated assessment and treatment of all doctors be done at a “PHP-approved” facility which means a facility identical to Ridgeview. This was done under the scaffold of the Federation of State Physician Health Programs (FSPHP). They are now in charge of all things related to physician wellness in doctors.
- Durcanin C, King M. The suicides at Ridgeview Institute: Suicides mar success at Ridgeview with troubled professionals. Atlanta Journal and Constitution. December 18, 1987, 1987: A13.
- Gonzales L. When Doctors are Addicts: For physicians getting Drugs is easy. Getting help is not. Chicago Reader. July 28, 1988, 1988.
- King M, Durcanin C. The suicides at Ridgeview Institute: A Doctor’s treatment program may be too tough, some say. Atlanta Journal and Constitution. December 18, 1987a, 1987: A12.
- Bissell L, Royce JE. Ethics for Addiction Professionals. Center City, Minnesota: Hazelden; 1987.
- Addiction Scientists from the USA: LeClair Bissell. In: Edwards G, ed. Addiction: Evolution of a Specialist Field. 1 ed: Wiley, John & Sons, Incorporated; 2002:408.
- Durcanin C. The suicides at Ridgeview Institute: Staff members didn’t believe Michigan doctor was suicidal. Atlanta Journal and Constitution. December 18, 1987, 1987: A8.
- Ricks WS. Ridgeview Institute loses $1.3 million in suit over suicide. Atlanta Journal and Constitution. October 11, 1987, 1987: A1.
- King M, Durcanin C. The suicides at Ridgeview Institute: Many drug-using doctors driven to Ridgeview by fear of losing licenses. Atlanta Journal and Constitution. December 18, 1987b, 1987: A1.
- Bissell L, Haberman PW. Alcoholism in the Professions. Oxford University Press; 1984.
- White W. Reflections of an addiction treatment pioneer. An Interview with LeClair Bissell, MD (1928-2008), conducted January 22, 1997. Posted at http://www.williamwhitepapers.com. 2011.
- Williams c. Health care field chemical dependency threat cited. The Tuscaloosa News. January 16, 1988, 1988: 16.
- Schneidman B. The Philosophy of Rehabilitation for Impaired Physicians. The Federal Bulletin: The Journal of Medical Licensure and Discipline. 1995;82(3):125-127.
- Peele S. In the Belly of the American Society of Addiction Medicine Beast. The Stanton Peele Addiction Website (accessed March 28, 2014) http://web.archive.org/web/20080514153437/http://www.peele.net/debate/talbott.html.
- Ursery S. $1.3M verdict coaxes a deal for doctor’s coerced rehab. Fulton County Daily Report. May 12, 1999b 1999.
- Ursery S. I was wrongly held in alcohol center, doctor charges. Fulton Count y Daily Report. April 27, 1999a 1999.
- Parker J. George Talbott’s Abuse of Dr. Leon Masters MD ( http://medicalwhistleblowernetwork.jigsy.com/george-talbott-s-abuse-of-leon-masters ). Medical Whistelblower Advocacy Network.
Share this:

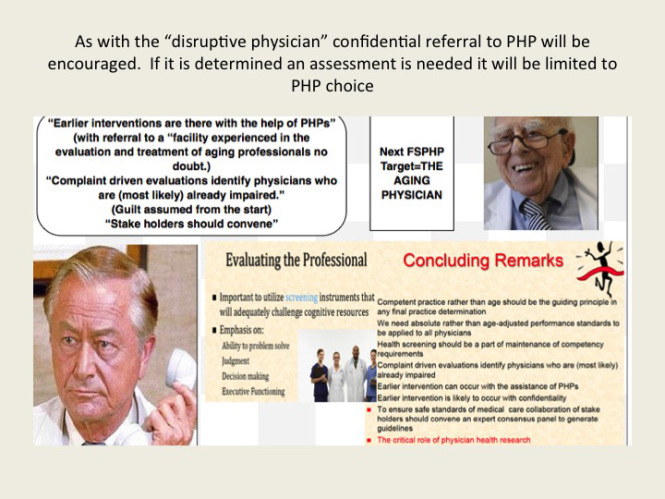
The Aging Physician—Goodbye Dr. Welby!
The methodology is not new–witches are real, witches are dangerous and witches need to be identified and exterminated at all costs. Convince the authorities to assist you in protecting the public from harm and advance the greater good
In this manner the Federation of State Physician Health Programs (FSPHP) has convinced the Federation of State Medical Boards state medical boards (FSMB) to adopt and enforce policies that have incrementally and systematically increased their own autonomy, scope and power. This began in 1995 when the FSPHP first cultivated a relationship with the FSMB and subsequently took an uninvited seat at the table of power by offering a non-disciplinary “safe harbor” as an alternative to discipline for doctors impaired by drugs or alcohol.
Since then they have increased their scope from the “impaired” to the “disruptive” to everything else. Arising from the “impaired physicians movement” as “addiction specialists” these doctors whose specialty of addiction is not even recognized by the American Board of Medical Specialties have now become the “experts” in all matters related to physician health. Jacks of all trades covering neurology, psychiatry, geriatrics, and occupational medicine.
A 2011 updated FSMB Policy on Physician Impairment states that Medical Boards should recognize the state Physician Heath Program (PHP) as their experts in all matters relating to licensed professionals with “potentially impairing illness,” and these include those potentially impairing maladies that increase as we age. This has gone too far. Isn’t it time we take back the profession of medicine from illegitimate and irrational authority?



As a specialist in geriatric medicine I have experience in taking care of a number of doctors who were referred to me for suspected memory problems. Still operating and teaching residents in his 70s, my first was a well-respected surgeon, a pioneer or Maverick who had made advances in his particular subspecialty. Known for his detailed knowledge of the history of medicine and sharp clinical acumen, he had not seemed himself for a while. His colleagues noted he appeared slower, fatigued and forgetful at times (not remembering his keys, having trouble finding the right word). An internist friend and co-worker who knew him for 50 years curb-sided me and asked if I would see him. He did not have a primary care physician or even seen a doctor professionally for decades (a common phenomenon in this age cohort of doctors).
I met him the next week and he readily admitted to having difficulty concentrating and having trouble with his short term…
View original post 1,533 more words

