

Originally posted on Article 8:Antitrust litigation hasn’t disappeared, but rather changed its focus. Instead of targeting the great railroad empires of the late 19th century, today’s antitrust efforts focus on more minute industries, like dentistry. In October, the Supreme Court heard arguments for North Carolina State Board of Dental Examiners v. Federal Trade Commission, in which…
“Physician Health”

Competent, Ethical and Fair Legal Representation for Doctors —A Possible New Niche area for Lawyers.
Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.– Father Cornelius Loos (1592) “PHP-Approved Attorneys” My survey has revealed an additional factor stacking the deck and removing accountability from […]
Share this:

Competent, Ethical and Fair Legal Representation for Doctors —A Possible New Niche area for Lawyers.
Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.– Father Cornelius Loos (1592)

“PHP-Approved Attorneys”
My survey has revealed an additional factor stacking the deck and removing accountability from PHPs. The attorneys ostensibly representing doctors are also part of the racket.
A doctor referred to a PHP will be given a list of 3 or 4 attorneys by the PHP who are “experienced in working with the medical board.” What they do not tell you is that theses attorneys are hand-picked or cultivated to abide by the rules dictated by the PHP.
They will not “bite the hand that feeds” and any procedural, ethical or criminal misconduct by the PHP will not be addressed. Laboratory fraud, false diagnoses, and Establishment Clause violations are off limits.
The primary purpose of these attorneys is to enforce payment for laboratory fees and demand compliance with whatever the PHP demands. Their primary purpose is to keep doctors powerless under the PHP and prevent misconduct, including crimes, from being discovered.
The attorney pool is currently over-served by those serving two clients and most of those outside simply do not know enough about the “physician health” legal issues related to doctors. When they appear before the board it is as if they are a deer in the headlights. It is a new terrain where all due process and familiar protocol have been removed. Of course this was all facilitated by changes in administrative and medical practice acts orchestrated by the physician health movement “in the interests of protecting the public. This must be recognized and addressed.
Skilled negotiators and lawyers with administrative law experience would do well to consider representation for doctors before medical boards regarding “physician health” matters.
It is not that esoteric, complicated or difficult. As with the rest of the population, most have just not critically analyzed the issues behind the curtain.



Share this:

Physician Suicide, Organizational Justice and the “Cry of pain” Model: Hopelessness, Helplessness and Defeat

According to Talbott, “impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.” “Terminal uniqueness “ is a phrase Talbott uses to describe doctors’ tendency to think they can heal themselves. “M-Deity” refers to doctors “being trained to think they’re God,” an unfounded generalization considering the vast diversity of individuals that make up our profession. This attitude, according to some critics, stems from the personal histories of the treatment staff, including Talbott, who are recovering alcoholics and addicts themselves. One such critic was Assistant Surgeon General under C. Everett Koop John C. Duffy who said that Ridgeview suffered from a “boot-camp mentality” toward physicians under their care and “assume every physician suffering from substance abuse is the same lying, stealing, cheating, manipulating individual they were when they had the illness. Certainly some physicians are manipulative, but it’s naïve to label all physicians with these problems.”

They can be a terror to your mind and show you how to hold your tongue
They got mystery written all over their forehead
They kill babies in the crib and say only the good die young
They don’t believe in mercy
Judgement on them is something that you’ll never see
They can exalt you up or bring you down main route
Turn you into anything that they want you to be–Bob Dylan, Foot of Pride

Although no reliable statistics yet exist, anecdotal reports suggest a marked rise in physician suicide in recent years. From the reports I am receiving it is a lot more than the oft cited “medical school class” of 400 per year.
This necessitates an evaluation of predisposing risk factors such as substance abuse and depression, but also requires a critical examination of what external forces may be involved in the descent from suicidal ideation to suicidal…
View original post 4,152 more words
Share this:

When Dentists Go Too Far: North Carolina Board of Dental Examiners v. Federal Trade Commission
The recent strike down of anticompetitive regulation in N.C. dental case opens the door to antitrust litigation against other state Regulatory Agencies such as Medical Boards.
The Federation of State Physician Health Programs has set up a “hidden” system of coercion and control using various methods (policy and moral entrepreneurship, changes in state medical practice acts and administrative procedure, misuse of health law, etc.) to create a system that lacks oversight and regulation. As a power unto themselves they are accountable to no one.
Although originally funded by medical societies and staffed by volunteer doctors in order to help sick colleagues and protect the public, any system can be subverted for profit and power, and these programs have been taken over by groups representing the multi-billion dollar drug and alcohol testing, assessment and treatment industry and become reservoirs of bad medicine and fraud. All manner of abuse can be hidden under a veil of benevolence. Although most are afraid to speak publicly under fear of punishment and retaliation (“swift and certain” consequences, summary suspension) I have herd from many many doctors in multiple states. Their stories are all the same.
In addition to misconduct related to the non-FDA laboratory developed tests (they themselves introduced into the market using a loophole that bypasses FDA approval) there are reports of coercion into unneeded evaluation and treatment at a couple dozen or so “PHP-approved” facilities under threat of loss of licensure.
Reports to a state PHP can be done anonymously with confidentiality guaranteed to the reporter. Any report will result in a meeting with the state PHP and if they feel a licensee is in need of an assessment they require it be done at a “PHP-approved” assessment center.
As non-profit tax exempt corporations, PHPs do not provide clinical assessments. They can only recommend assessments. State Regulatory Agencies (Medical Boards, Nursing Boards, etc.) have accepted the PHPs requirements of limiting assessments to those approved by the PHP. In fact many states mandate assessments to solely “PHP-approved” assessment centers under threat of summary suspension of a professional license.
An Audit of the North Carolina PHP by State Auditor Beth Woods, however, found financial conflicts-of-interest in the use of these predominantly out-of-state assessment facilities to which the N.C. PHP was referring and the state Medical Board was requiring. Woods requested the qualitative indicators and quantitative measures used to “approve” these assessment centers from the N.C. PHP but they were unable to produce any documentation showing any quality indicators or objective criteria existed! The best response they could come up with was “informal” methods and “reputation.” The full audit can be seen here.
Imagine if the FDA gave this reply if asked to provide the criteria used to “approve” medications or medical devices in the “FDA-approval” process!
Making matters even worse, the Medical Director of the N.C. PHP, Dr. Warren Pendergast was serving as President of their national organization, the FSPHP at the time of the audit.
The simple fact is no criteria exist.
A recent class action lawsuit in Eastern Michigan found this same pattern of referral to out-of-state assessment and treatment centers ( Marworth, Talbott, Hazelden. Promises,etc.)
State referrals to “PHP-approved” facilities has become a matter of public policy. Both the American Society of Addiction Medicine and the Federation of State Medical Boards have issued public policy statements stating that only “PHP-approved” centers be utilized by Regulatory Agencies in the assessment and treatment of their licensees. Moreover, these policies specifically exclude “non-PHP-approved facilities and often involve a limited time-frame. No choice, no appeal and no bartering. Do it. Do it now and if you don’t suffer the consequences.
These public policy statements can be seen in the 2011 ASAM “Public Policy Statement on Coordination between Treatment Providers, Professionals Health Programs and Regulatory Agencies” and the 2011 FSMB “updated Policy on Physician Impairment.” Many state Regulatory Agencies have strictly adhered to these policy recommendations.
What this means is that states are mandating evaluations at “PHP-approved” facilities even though there is no documentable or plausible reason for doing so. No measurable criteria exist as to how the list of “approved” facilities were “approved” yet they have “cornered the market,” removed choice and created an imposed monopoly under threat of loss of professional licensure.
In reality no official “PHP-approved” list exists. Neither does any objective published criteria for approving them. At the same time state Regulatory Agencies and Boards are forcing evaluations on licensed professionals at these couple-dozen or so facilities. They are excluding patient autonomy and choice violating the fundamental freedoms of the individual and informed consent.
All semblance of due process has been removed. If a plausible reason existed (i.e. they met some minimum standard of credentialing, quality or patient outcome) for referring to a proscribed list of assessment centers it could be arguably justified. Without such criteria, and in light of the economic and ideological conflicts of interest involved, it is patently unjustifiable.
Even more disturbing is, as Drs. John Knight and J. Wesley Boyd (who collectively have more than 20 years experience as Associate Directors at the Massachusetts PHP, PHS, Inc.) pointed out in their 2012 paper published in the Journal of the American Society of Addiction Medicine, many of these facilities are willing to “tailor” the diagnosis and recommendations of an evaluation to fit the wishes of the PHP. “Tailoring” an assessment and recommendations to anything other than what the true data show is healthcare fraud. It is, in fact, the political abuse of psychiatry.
PHPs started out as “Physicians Health Programs” but many are transitioning to “Professionals Health Programs” to widen the net. For example in Michigan and Florida the state PHP covers all health care practitioners from Acupuncturists to Veterinarians. PHPs have also entered non -healthcare employee assistance programs (EAPs) such as the aviation industry and the grand plan is expansion to non-healthcare professions. They are doing this by claiming remarkable success rates and brandishing themselves as the “gold-standard” of substance abuse treatment. Interestingly, the same individuals claiming how successful PHP programs are are the same individuals profiting from the drug and alcohol testing they introduced. Anyone with any sort of license is at risk.
So whether you cut hair, teach, take care of patients or even drive a car they could be coming after you next and they don’t have to convince you of the validity and reliability of their services–they only need to convince those who regulate your license and, as we have seen, they are very accomplished at persuasion in this department.
And that is why we need more state audits of PHPs and Medical Boards. The starting point is simple. Request from the state PHP and Board a list of “PHP-approved” facilities and the criteria by which they were approved. What should be a simple reply will undoubtedly not be as they will not be able to provide either.

Antitrust litigation hasn’t disappeared, but rather changed its focus. Instead of targeting the great railroad empires of the late 19th century, today’s antitrust efforts focus on more minute industries, like dentistry.
View original post 2,385 more words
Share this:

Class Action Suit Filed Against Michigan PHP Alleging Constitutional Violations Related to Involuntary Treatment
 A Federal class action lawsuit has been filed in the Eastern District of Michigan against the state PHP program alleging constitutional violations related to the forced medical treatment of health care professionals involved in the State’s “Professionals Health Program” (PHP) and the “callous and reckless termination of professional licenses without due process.” According to the complaint:
A Federal class action lawsuit has been filed in the Eastern District of Michigan against the state PHP program alleging constitutional violations related to the forced medical treatment of health care professionals involved in the State’s “Professionals Health Program” (PHP) and the “callous and reckless termination of professional licenses without due process.” According to the complaint:
“The Health Professional Recovery Program (HPRP) was established by the Michigan Legislature as a confidential, non-disciplinary approach to support recovery from substance use or mental health disorders. The program was designed to encourage impaired health professionals to seek a recovery program before their impairment harms a patient or damages their careers through disciplinary action. Unfortunately, a once well-meaning program, HPRP, has turned into a highly punitive and involuntary program where health professionals are forced into extensive and unnecessary substance abuse/dependence treatment under the threat of the arbitrary application of pre-hearing deprivations (Summary Suspension) by LARA.filed in the the State of Michigan and a private contractor (Ulliance, Inc. of Troy, Michigan) engaged in a conspiracy to violate the civil rights of Michigan health professionals by involuntarily subjecting them to excessive and unnecessary treatment for substance abuse and suspending their licenses if they do not comply.”
As is the case with most PHPs across the country taken over by the FSPHP the mechanics and mentality are the same. Referrals can be made anonymously by “colleagues, partners, hospital administrations, patients, family members, or the State” to the PHP for any health professional (from acupuncturist to veterinarian) exhibiting “potential signs of impairment”
The HPRP website states the names of those reporting are kept confidential “unless testimony is needed at a later disciplinary hearing.”
 After initial intake with HPRP, the licensee is referred to a “qualified evaluator” and “If the evaluation indicates a substance use and/or mental health disorder that represent a possible impairment” the HPRP makes referrals for treatment services to an “approved provider.
After initial intake with HPRP, the licensee is referred to a “qualified evaluator” and “If the evaluation indicates a substance use and/or mental health disorder that represent a possible impairment” the HPRP makes referrals for treatment services to an “approved provider.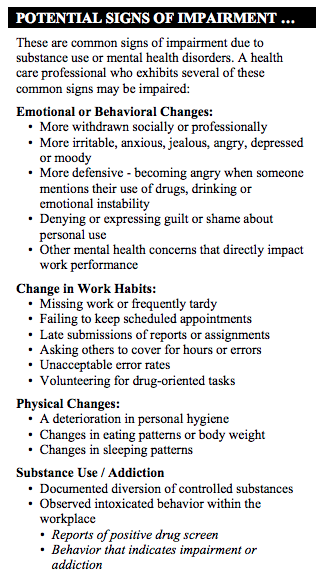
The “qualified evaluators” and “approved providers” are undoubtedly the same out-of-state facilities North Carolina state Auditor Beth Woods found her state program was referring to in her audit of the N.C. PHP under the undefinable justification they were “PHP-approved.”
As with North Carolina, the Michigan PHP will be unable to provide what quality indicators and quantitative measurements are being used to “qualify” and “approve these facilities. None exist as the common denominators in these “PHP-approved” and state mandated assessment and treatment centers are ideological and economic.
The medical directors of almost if not all of them can be seen on this list of “like-minded docs.” The conflicts-of-interest and intertwined relationships among this group is staggering.
The philosophy of Like-Minded Docs is the following:
“We believe that evidence from extensive, well-designed studies demonstrates the great benefits of Twelve-Step recovery modalities including Twelve Step Facilitation in promoting long-term recovery. Further, Twelve-Step modalities are compatible with other treatment strategies including medication-management. We believe that Addiction specialists need to facilitate a path for our patients toward the best possible state of wellness and recovery as they receive treatment for this chronic disease. We believe a well-rounded educational and clinical preparation for physicians choosing to practice addiction medicine or addiction psychiatry requires a comprehensive exposure to the psychosocial and spiritual modalities of treatment as well as the neurobiological and psychopharmacological modalities.”
This connection needs to be made by both North Carolina and Michigan as the state is mandating treatment not only to assessment and treatment centers with economic conflicts of interest but with ideological ones as well. Health care practitioners are being forced into evaluations exclusively at 12-step facilities and excluding non-12 step assessment and treatment centers. This is a clear violation of the Establishment Clause of the 1st Amendment.
The complaint goes on to state the HPRP:
“has expanded its role to include making treatment decisions in place of the opinions of qualified providers. Licensees are subjected to intake evaluations by a pre-selected cadre of providers who profit from the enrollment of HPRP members. This process culminates in a large number of health professionals receiving a “Monitoring Agreement” which is essentially a nonnegotiable contract for treatment selected by HPRP. While HPRP’s contract with the State requires that treatment be selected by an approved provider and that it be tailored in scope and length to meet the individual licensee’s needs, licensees generally receive the same across-the-board treatment mandates regardless of their diagnosis or condition. Further, treatment providers are not permitted to recommend the specific treatment rendered and HPRP has a policy that only HPRP can set the terms of the treatment required in the contract. Failure to “voluntarily” submit to unnecessary and costly HPRP treatment results in automatic summary suspension..”
“Facing the threat of summary suspension in the event of non-compliance, licensed health professionals are induced into a contract as a punitive tool of BHCS and are often required to refrain from working without prior approval, refrain from taking prescription drugs prescribed by treating physicians, and sign broad waivers allowing HPRP to disclose their private health information to employers, the State of Michigan, and/or treating physicians.”
“Every licensee in the State of Michigan who has received a summary suspension, as a result of HPRP non-compliance, has had their private health data transmitted to the BHCS for use during administrative proceedings. In short, the mandatory requirements of HPRP, coupled with the threat of summary suspension, make involvement in HPRP an involuntary program circumventing the due process rights of licensees referred to the program. The involuntary nature of HPRP policies and procedures as outlined above and the unanimous application of suspension procedures upon HPRP case closure are clear violations of Procedural Due Process under the Fourteenth Amendment.”
This is exactly the same system of institutional injustice seen at Ridgeview under G. Douglas Talbott. Multiple physician suicides were attributed to these same abuses–involuntary forced treatment under extortion of loss of licensure. It is time this elephant in the room be addressed in terms of the marked increased in suicide we are seeing now.
http://www.chapmanlawgroup.com/hprp-class-action/
Health Professionals File Class Action Against HPRP
Feb 28th, 2015 // Blog
Jurisdiction: U.S. District Court for the Eastern District of Michigan
Subject: Plaintiff’s filed a class action lawsuit on behalf of Michigan health care professionals, alleging constitutional violations related to the forced medical treatment of health care professionals involved in the State’s substance abuse monitoring program (HPRP) and the callous and reckless termination of professional licenses without due process by HPRP and the Bureau of Healthcare Services.
Three Michigan health professionals filed a federal class action for due process violations arising out of execution of a State substance abuse monitoring program known as the Health Professionals Recovery Program. According to the class action lawsuit filed today in the Eastern District of Michigan, the State of Michigan and a private contractor (Ulliance, Inc. of Troy, Michigan) engaged in a conspiracy to violate the civil rights of Michigan health professionals by involuntarily subjecting them to excessive and unnecessary treatment for substance abuse and suspending their licenses if they do not comply.
HPRP, intended as a voluntary treatment program by the legislature, has become a highly punitive and involuntary tool designed to circumvent due process, the complaint states. However, according to the complaint, Carole Engle, the Former Director of the Bureau of Healthcare Services, implemented a policy that any person who does not voluntarily submit to this unnecessary treatment would be immediately suspended without a hearing and prevented from practicing as a health professional. Carole Engle recently resigned her position after Governor Snyder refused to renew her contract with the State of Michigan. It is unclear whether her recent resignation is related to the recently filed class action.
The controversial treatment program has generated a significant amount of criticism in recent years from Michigan health professionals who have called for a class action in an effort to stop HPRP’s abuse of their broad sweeping power. For years, HPRP subjected nurses to three years of intense addiction treatment sometimes on the basis of an anonymous tip.
“We turned to the courts for fairness because HPRP’s mandate of unnecessary treatment has ruined countless lives. My life has been ripped apart by HPRP despite the fact that two evaluators determined that I do not need treatment. I am only one of hundreds who have had to choose between suspension of my license and tens of thousands of dollars worth of treatment that was unnecessary – I just couldn’t afford it, and now I can no longer practice as a nurse” said Carol Lucas, a registered nurse and a Plaintiff in the class action.
Chapman Law Group, a Michigan health care law firm, filed the complaint on behalf of three named Plaintiffs, each of whom fell victim to HPRP’s demand that they submit to unnecessary treatment or have their license suspended. The class includes Michigan health professionals who are or were participants in the Health Professionals Recovery Program during the period from January 1, 2011 to present.
The complaint and amended complaint can be seen below:
Share this:

The Aging Physician—Goodbye Dr. Welby!

As a specialist in geriatric medicine I have experience in taking care of a number of doctors who were referred to me for suspected memory problems. Still operating and teaching residents in his 70s, my first was a well-respected surgeon, a pioneer or Maverick who had made advances in his particular subspecialty. Known for his detailed knowledge of the history of medicine and sharp clinical acumen, he had not seemed himself for a while. His colleagues noted he appeared slower, fatigued and forgetful at times (not remembering his keys, having trouble finding the right word). An internist friend and co-worker who knew him for 50 years curb-sided me and asked if I would see him. He did not have a primary care physician or even seen a doctor professionally for decades (a common phenomenon in this age cohort of doctors).
I met him the next week and he readily admitted to having difficulty concentrating and having trouble with his short term memory. On taking his history he told me of his life and career which started as an intern in Boston in 1942 and he was on duty the night 492 people were killed in the Cocoanut Grove fire with many of the victims transported to his hospital. “I can see every detail as if it were yesterday–beautiful young women wearing fashionable dresses and gowns and young men in formal evening wear who looked as if they were sleeping but were dead.”
“Gastric reflux ” was the only medical problem he reported, adding it was well controlled for the better part of a decade with anti-reflux medications from the office sample closet. I tested his memory with several cognitive scales which showed some mild deficits in short-term memory and sent him to a neuropsychologist for more comprehensive testing. His physical examination, including a comprehensive neurological exam was normal. I ordered the usual lab work up for dementia to look for possible metabolic causes and his B12 level returned markedly low–a result of his long-term use of proton pump inhibitors. He was given an intramuscular injection and started on high doses of oral B12. As one of the “reversible’ causes of dementia he was back to his usual sprightly self several months later.
Another, a 70 old psychiatrist still teaching medical students and residents had asked a third-year psychiatric resident out on a date on two separate occasions. She reported him to administration on the second request. When I asked him about the incident he replied he didn’t see what was wrong with what he did and it was being blown out of proportion. “She’s in her 20’s” I said to which he replied “Well I’m only 36.” Still giving lectures to first year medical students without error or pause from knowledge he learned long ago, he could not identify a pencil or a watch when I pointed to them and asked what there were. He knew neither the month, season or year. After an MRI and neuropsychological testing he was given a diagnosis of probable Alzheimers disease. He had no spouse or children and his work was his life. After that he became profoundly depressed and six months later was dead.
Another elderly doctor, an internist, had a fairly sudden sudden onset of memory problems and symptoms of delirium. It turned out he was having trouble sleeping and his cardiologist prescribed him Dalmane, a benzodiazepine similar to Valium (medications that have a whole host of adverse effects in older patients including memory problems and falls). But valium has a half-life of hours whereas Dalmane has a half life of days. The medication was stopped and he was back to normal after a few days.
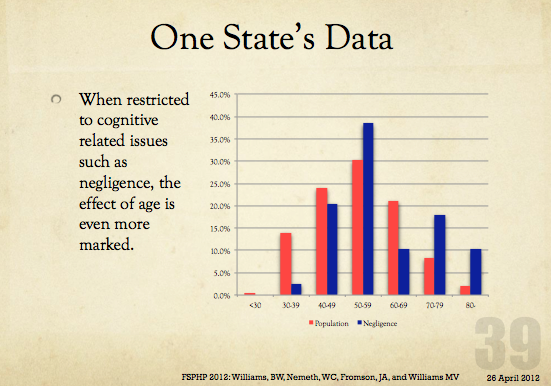
Aging is associated with an increased decline in many areas including cognition, motor-skills, muscle strength, and vision that can individually or cumulatively create risk to the person or others in a variety of situations (driving, living situation, occupation).
With advancing age comes advancing risk and the recognition and vigilance of others is often necessary for intervention. If the risk is recognized the problem can be addressed by the appropriate healthcare providers and specialists.
Doctors are not immune from cognitive impairment or dementia and the perspicacity of others is necessary should this occur.
Recognition and awareness are important. So too is an assessment by a qualified physician Board Certified in Neurology, Geriatrics or Geriatric Psychiatry who has education and experience in the diagnosis and treatment of memory disorders.
Recognition, Insight and Education Essential
In 2009 Dr. Ralph Blasier, M.D, J.D., published an article in the Journal Clinical Orthopaedics and Related Research entitled “The Problem of the Aging Surgeon: When Surgeon Age Becomes a Surgical Risk Factor” discussing the ability of older physicians to practice medicine safely and effectively.
His primary message is that a decline in physical and cognitive abilities is associated with the aging process and that these issues are especially pertinent to the field of medicine.
An area little researched, Blasier gives anecdotal examples such as a surgeon in his late 80s who had to regularly depend on younger colleagues to finish his operations. He concludes that these anecdotal examples suggest many surgeons lack insight into the degradation of their own skills and suggests recognition, insight, and education can help facilitate retirement of the aging surgeon before a decline in competency and skill creates a problem.
The awareness, education and insight of others is necessary to identify age associated illness in doctors who can then be referred to the proper specialists for evaluation. And although no evidence base exists, anecdotal reports such as these caused some groups to see an opportunity to increase the grand scale of the hunt.
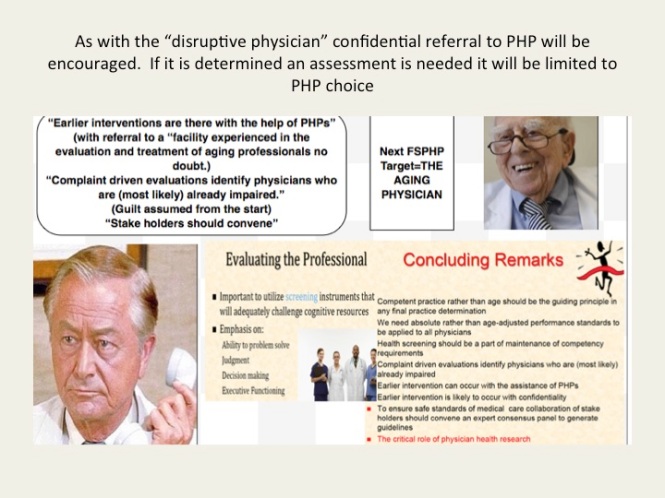
Aging Physicians Next Target of Physician Health Programs
As with the “impaired” and “disruptive” physician, the “physician health and wellness movement” organized as the Federation of State Physician Health Programs (FSPHP) is linking the “aging” physician with threats to patient safety and hospital liability. “Experts say doing nothing could result in lawsuits, higher liability insurance rates, ruined reputations for practices and all involved, and even possible losses of practices and the licenses of non-reporting physicians.”
And if you look at the articles and presentations aimed at the administrative, regulatory, and legal arenas of medicine it appears a new moral panic is percolating in the “physician wellness” cauldron.
Labelling a group dangerous and creating fear in those responsible for that group is an effective means to sway policy and opinion.
With absolutely no evidence base these groups have acted as “moral entrepreneurs ” and used this same methodology to successfully change policy and regulation in the medical profession and advance their goals. The methodology is to
1. Label a group and link that group to danger
2. Offer to assist in identifying and eliminating that danger
3. Corner the market and control all aspects including assessment, testing and monitoring by swaying those in authority to make it public policy and regulation. 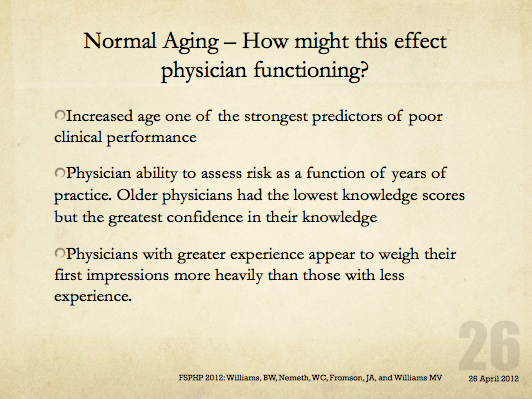
The methodology is not new–witches are real, witches are dangerous and witches need to be identified and exterminated at all costs. Convince the authorities to assist you in protecting the public from harm and advance the greater good
In this manner the FSPHP has convinced state medical boards to adopt and enforce policies that have incrementally and systematically increased their autonomy, scope and power since they first cultivated a relationship with the Federation of State Medical Boards (FSMB). This occurred in 1995 when they took an uninvited seat at the table of power by offering a non-disciplinary “safe harbor” as an alternative to discipline for doctors impaired by drugs or alcohol.
Since then they have increased their scope from the “impaired” to the “disruptive” to everything else. Arising from the “impaired physicians movement” as “addiction specialists” these doctors whose specialty of addiction is not even recognized by the American Board of Medical Specialties have now become the “experts” in all matters related to physician health. Jacks of all trades covering neurology, psychiatry, geriatrics, and occupational medicine.
A 2011 updated FSMB Policy on Physician Impairment states that Medical Boards should recognize the state Physician Heath Program (PHP) as their experts in all matters relating to licensed professionals with “potentially impairing illness,” and these include those potentially impairing maladies that increase as we age.
They are also using “everyone else does it why don’t we?” logical fallacy. According to a Washington Post article “other professions are subject to age-related regulations. For example, airline pilots must undergo regular health screenings staring at age 40 and must retire at age 65. FBI agents must retire at age 57.”
Proposing drug testing in doctors a JAMA article uses this same logic stating when sentinel events occur in the airline, nuclear power and railway industry the get drug tested. However all of these industries use FDA approved tests, certified labs, strict chain-of-custody and MRO review in their drug testing. One of the authors of the JAMA paper, Dr. Greg Skipper, introduced the non-FDA approved and unvalidated Laboratory Developed Tests currently used in PHPs such as EtG. He claims no conflicts-of-interest. Comparing drug testing to industries that use the highest quality of testing and safeguards to protect the donor from false-positives to the junk science used in PHPs is comparing apples to oranges. Which one do you think they’s be using in the random drug testing of doctors?
Furthermore, airline pilots, railway engineers and nuclear power plant employees have a choice of assessment and treatment centers should they get a positive test. Doctors do not. They are mandated to “PHP-approved” facilities. This is enforced by state medical boards as they adhere to an ASAM Public Policy Statement recommending only “PHP approved” treatment centers be used for assessment and treatment and a recent audit found the PHP in North Carolina could not provide any measurable indices or qualitative indicators of how an assessment center is stamped “approved.” The best they could come up with is “reputation” and other ‘informal sources. What the audit missed is all of the 19 out-of-state “PHP-approved” centers Medical Directors can be found on this list.
And what will happen with the “aging physician” is the same. Doctors will be forced into “assessments” at “PHP-approved” facilities where they will be misdiagnosed, over-diagnosed and forced into monitoring contracts under threat of loss of licensure. Goodbye Dr. Welby!




Share this:

The Elephant in the Room: Physician Suicide and Physician Health Programs
The Elephant in the Room: Physician Suicide and Physician Health Programs.
Accountability is rooted in organizational purpose and public trust. Unfortunately, humanitarian ideals have been trampled by the imposition of corporate front groups who advance hidden agendas under guises of science and scholarship and patinas of benevolence. Rife with conflicts of interest, these groups obfuscate, mislead and exploit us to further an underlying political and corporate agenda. Healthcare and medicine has been infiltrated by various groups that pose a serious threat to both the humanitarian and evidence based aspects.


Share this:

Bent Science and Bad Medicine: The Medical Profession, Moral Entrepreneurship and Social Control

 The Medical Profession, Moral Entrepreneurship, and Social Control
The Medical Profession, Moral Entrepreneurship, and Social Control
Sociologist Stanley Cohen used the term “”moral panic” to characterize the amplification of deviance by the media, the public, and agents of social control.1 Labeled as being outside the central core values of consensual society, the deviants in the designated group are perceived as posing a threat to both the values of society and society itself. Belief in the seriousness of the situation justifies intolerance and unfair treatment of the accused. The evidentiary standard is lowered.
Howard Becker describes the role of “moral entrepreneurs,” who crusade for making and enforcing rules that benefit their own interests by bringing them to the attention of the public and those in positions of power and authority under the guise of righting a society evil. 2
And according to cultural theorist Stuart Hall, the media obtain their information from the primary definers of social reality in authoritative positions and amplify the perceived threat to the existing social order. The authorities then act to eliminate the threat.3 The dominant ideas or ideologies are reproduced by relying on the opinions of the defining authority and then spread through the media. The communal good has been assailed.
As a society governed by organizations, associations, institutions and regulatory bodies, the medical profession is not immune to “moral panics.” A threat to patient care or the values of the profession can be identified and amplified. A buildup of public concern fueled by media attention ensues creating a need for governing bodies to act. Medical Professionalism and the Public Health has been assailed.
Unbeknownst to the general public and most members of the medical profession at large, certain groups have gained tremendous sway within medical society. Through moral entrepreneurship they have gained authority and become the primary definers of the governance of the medical profession and the social control of doctors. To benefit their own interests they have fostered and fueled “moral panics” and “moral crusades. ” Exhorting authorities to fight these threats by any means necessary they have successfully made and enforced rules and regulations and introduced new definitions and tools with no meaningful resistance or opposition.
The Inquisition did not have to convince individual citizens or the general public of their beliefs to advance an agenda; just Ecclesiastical and Political Authority. Similarly, the “impaired physicians movement” did not have to convince individual doctors or the medical profession of their beliefs to further a self-serving agenda; just regulatory and administrative authority.
Addiction Medicine Monopoly, False Authority and Conflicts of Interest
The “impaired physicians movement” can be defined as a group of physicians with alcohol and substance abuse problems who, having found sobriety through 12-step spirituality, banded together to promote the ideology behind their personal “recovery” to other doctors and the medical community at large. In the 1980s the movement gained momentum and as their numbers grew began calling themselves specialists in “addiction medicine.” The American Society of Addiction Medicine (ASAM) is not a true specialty, but a Self-Designated-Practice-Specialty, which simply means that is what they are calling themselves. It reflects neither knowledge nor expertise.. “Board certification” by the American Board of Addiction Medicine (ABAM) is not recognized by the American Board of Medical Specialties (ABMS).
ABAM certification requires only a medical degree, a valid license to practice medicine, and completion of residency training in ANY specialty. Addiction Psychiatry, a subspecialty of psychiatry under the American Board of Neurology and Psychiatry is the only specialty recognized by the ABMS. and their specialty society is the American Academy of Addiction Psychiatry.
The ASAM is schooled in just one one uncompromising model of addiction with the majority attributing their very own sobriety to that model–the chronic relapsing “brain disease” with lifelong abstinence and 12-step spiritual recovery model. As the “voice of addiction medicine,” the ASAM has nevertheless defined the dominant treatment paradigm in the United States. ASAM doctors outnumber addiction psychiatrists by 4:1 and the movement is well funded. Because addiction is defined as a “disease”, addicts must be “treated” (more often coercive than voluntary), and “cured” (defined as abstinent). The billion dollar assessment and treatment industry and the drug and alcohol testing industry lucratively profits from this model which has grown to monopolize addiction treatment in the United States.
The goal of the ABAM Foundation is to “gain recognition of Addiction Medicine as a medical specialty by the American Board of Medical Specialties (ABMS).” A monopoly defined by self-appointed experts without recognized specialty training will soon likely Robber baron their way to being accepted as a true specialty.
Physician Health Programs, Regulatory Agencies, and Treatment Centers
Physician Health Programs (PHPs) meet with, assess, and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Unless being monitored by one, PHP practices are unknown to most physicians and operate outside the scrutiny of the medical community. Initially funded by State Medical Societies and staffed by volunteer physicians, PHPs served the dual function of helping sick doctors and protecting the public.
As the populations of ASAM physicians proliferated in the 1980s, many joined their state Physician Health Programs. PHP doctors who did not agree with the ASAM groupthink were gradually removed and they organized under the Federation of State Physician Health Programs (FSPHP). Other ASAM physicians found employment at treatment centers as staff physicians and medical directors.
The FSPHP cultivated a relationship with the Federation of State Medical Boards (FSMB) and the state PHPs formed alliances with their state medical boards. Promoting themselves as offering “treatment” rather than”punishment” they offered an alternative to disciplinary action. They then began promoting their successful outcomes in rehabilitating “impaired physicians”, and this history can be seen by examining the archives of the Journal of Medical Regulation and similar publications. In 1995 the Washington PHP claimed a success rate of 95.4%, Tennessee claimed 93% and Alabama 90%.
Part of this success was attributed to the specialized treatment centers for doctors directed by their ASAM colleagues such as Ridgeview Institute in Atlanta created by G. Douglas Talbott. Talbott, who helped organize and serve as past president of the ASAM claimed a 92.3 percent recovery rate. He also put forth a Medical Urban Legend–the proposition that doctors were a different species, separate from the rest of society, who needed special treatment three times longer than anyone else. Amazingly, this dicto simpliciter argument that can, in fact, be refuted simply by pointing it out was allowed to enter regulatory medicine unopposed. Simply because, sadly, no one ever pointed out the logical fallacy. It is now entrenched. Three months or more of treatment is standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value.
Physicians are unique only insofar as the unique elements required of the profession to become and be a physician such as going to medical school and completing the required board examinations. That’s it. I implore anyone to put forth any sound argument based on science and evidence that justifies a thrice lengthy stay in medical professionals. Not gonna happen. Thought stopping memes and logical fallacy is the best they have to offer. And, unfortunately this type of rabbling gibberish cuts the mustard in the regulatory medicine venue. A “low-bar” evidentiary standard is not the problem. If you look at the documentary evidence from a medico-historical perspective there never was a bar. The FSMB has essentially given the impaired physicians movement carte blanche authority and unrestrained managerial prerogative. A bar never even existed. It’s a laissez-faire Lord of the Flies free-for-all. The logical fallacy of appeal to authority–illegitimate and irrational authority. Bamboozled by smoke and mirrors.
A 1995 issue of the FSMB publication The Federal Bulletin: The Journal of Medical Licensure and Discipline contains reports on eight separate state PHPs. The “almost 90% success rate” was applauded by the editor, who added “cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” And more recent reports suggest PHPs reduce malpractice claims. They are now being promoted as a replicable model to be used in other populations.
The problem is no one bothered to examine the methodology to discern the validity of these claims. There has been no critical analysis or Cochrane type review of any of these studies which are invariably small, methodologically flawed, and biased.
The FSMB has accepted them as expert authority and their authoritative opinion as fact. It is this acceptance of faith without objective assessment that has allowed the ASAM and FSPH to advance their agenda. By confusing ideological opinion with professional knowledge, the FSMB and state Medical Boards have acted as willing gulls each step of the way. No counter-forces existed. And they still don’t. Junk science and unvalidated neuropsychological testing is used by these groups unconstrained and willfully. There is no regulation, oversight, or accountability. They are using polygraph testing (despite the AMA’s previous public policy statement deeming it junk) to both condemn “disruptive” surgeons and deem convicted pedophiles fit to return to work. They have introduced junk-science in drug and alcohol testing and unvalidated “neuropsychological” testing to detect “character-defects” by getting regulatory agencies to accept the validity of these tests not by the Scientific Method or Evidence Based Research but by (to coin a term) “Regulatory Sanctification”
To paraphrase one FSPHP member, “Who needs evidence-based medicine when the boards have already accepted these tests as valid?” Who indeed?
The ideological bias and financial conflicts of interest between PHPs and the treatment centers was also not recognized. It still isn’t. The spotlights are apparently all on Big Pharma in this regard. Some sunlight needs to be exposed in the direction of the billion dollar drug and alcohol testing and assessment industry as well.
Doctors were held at Ridgeview three times longer than the rest of the population (and at three times the cost) under threat of loss of licensure. Although there is no evidence base or plausible explanation why an entire profession would have a three-times longer length of stay than the rest of the population this continues to be the reality. There is no choice.
in 2011 The ASAM issued a Public Policy Statement on coordination between PHPs, regulatory agencies, and treatment providers recommending that only “PHP approved” treatment centers be used in the assessment and treatment of doctors. It specifically excludes non “PHP -recognized” facilities. And what defines a “PHP approved” treatment center? In addition to finding essentially no oversight by the state medical society and medical board, a recent audit of the North Carolina PHP found financial conflicts of interest and no documented criteria for selecting the out of state treatment centers they used. The common denominator the audit missed was that the 19 “PHP-approved” centers were all ASAM facilities just like Ridgeview whose medical directors can be seen on this list.
The appeal to authority logical fallacy has enabled the FSPHP to become the expert authority on physician impairment through the eyes of the medical boards. It has also allowed them to increase their scope.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that:
“Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with ‘potentially impairing illness.'”
According to the FSPHP, physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years.”
The policy extends PHP authority to cover physical illnesses affecting cognitive, motor, or perceptive skills, disruptive physician behavior, and “process addiction” (compulsive gambling, compulsive spending, video gaming, and “workaholism”). It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A A language –stinking thinking.” AA language has entered the Medical Profession and no one even blinked. It will get worse.
The ASAM has monopolized addiction treatment in the United States. It has imposed it on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. It selects who will be monitored and dictates every aspect of what that entails. It is a, in fact, a rigged game.
Inherent in this model is the importance of external control. It gives them power to exert control over the individual regardless of whether they need to be treated.
By bamboozling regulatory medicine this was accomplished. And the maintenance of this relationship is necessary as this presentation by an FSPHP physician warns, “guard this relationship jealously.”

Moral Panics and Moral Crusades
By introducing and fueling moral panics the ASAM/FSPHP political apparatus has been able to expand in both scope and power.
The Medscape article “Drug Abuse Among Doctors: Easy, Tempting, and Not Uncommon” published in the “Business of Medicine” section in January 2014 is characteristic example of the authoritative opinion, propaganda, and misinformation spun to maintain a pervasive climate of fear. Proof by anecdote. Physicians are “5 times as likely as the general public to misuse prescription drugs” according to Lisa Merlo, PhD. “Given the epidemic of prescription addiction sweeping the nation, that’s a grim statistic.”
Described as a “researcher at the University of Florida’s Center for Addiction Research and Education,” Merlo’s research involving 55 doctors being monitored by their state Physician Health Program published in the Journal of Addiction Medicine in October 2013 found “most physicians who abuse prescription drugs” do so to “relieve stress and physical or emotional pain.” Nowhere is it mentioned on Medscape that Merlo is the Director of Research for the Florida state PHP Professionals Research Network. Physician access to medications through prescriptions, “networks of professional contacts, and proximity to hospital and clinic supplies” gives them “rare access to powerful, highly sought-after drugs” says Marvin D. Seppala, chief medical officer at Hazelden. This access “sets them apart” and “not only foment a problem” but”perpetuate it” says Seppala. “Access “becomes an addict’s top priority” and they “will do everything in their power to ensure it continues.”
“They’re often described as the best workers in the hospital,” he says. “They’ll overwork to compensate for other ways in which they may be falling short, and to protect their supply. They’ll sign up for extra call and show up for rounds they don’t have to do.”-Dr. Marvin D. Seppala
Physicians are intelligent and skilled at hiding their addictions, he says. Few, no matter how desperate, seek help of their own accord.” In reality this is absurd. And if you look at any of the current “moral panics” that are being used to suggest random suspicion-less drug testing of all doctors or promoting the Physician Health Programs as the “New Paradigm” you will inevitably find a doctor, just like Marv Seppala who is on this list as an author or interviewee. It is a given.
The terms “impaired physician” and the “disruptive physician” are used as labels of deviancy. As deviants who allegedly threaten the very core of medicine (patient care) and the business of medicine (profit) they must be stopped at all costs. Belief in the seriousness of the situation justifies intolerance and unfair treatment. The evidentiary standard is lowered. Aided by a “conspiracy of silence” among doctors in which impaired colleagues are not reported necessitates identification of them by any means necessary. Increase the grand scale of the hunt.
In this way these front-groups have successfully acted as moral entrepreneurs to make and enforce rules and put forth new definitions and mandates that serve their own interests. A retrospective non -blinded non-randomized cohort study with serious underlying methodological errors involving 904 physicians being monitored by PHPs is now being used to “set the standard for recovery.”

Across the Country doctors are going to the media, law enforcement, the AGO, and the ACLU only to be turned a deaf ear. Many consider this a “parochial” issue best handled by the medical community. Doctors reporting crimes are turned back over to the very perpetrators of the crimes. The Medical Societies and professional organizations contribute to the problem by willful ignorance. Accusations are used to disregard the claims of the accused. It is a system of institutional injustice that is driving many doctors to suicide. Hopeless, helpless, and feeling entrapped many are taking this route. And no one is talking about it. This cannot be avoided any longer.
The next target is the “aging physician.” And as they have done with the “impaired” and “disruptive” physician” the FSPHP and their affiliates are setting the stage for another “moral crusade.”
- Cohen S. Folk Devils and Moral Panics: The Creatio of the Mods and Rockers (New Edition). Oxford, U.K.: Martin Robertson; 1980.
- Becker H. Outsiders: Studies in the Sociology of Deviance. New York: Free Press; 1963.
- Hall SC, Critcher C, Jefferson T, Clark J, Roberts B. Policing the Crisis: Mugging, the State, and Law and Order. London: Macmillan; 1978.

Share this:

Integrity and Accountability—Going on two months and no winners stepping forward. Defend the MRO Procedurally, Ethically or Legally and you win all the prizes

As the Medical Review Officer (MRO) for the Massachusetts state Physician Health Program (PHP), Physician Health Services, Inc. (PHS, inc.), Dr. Wayne Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody in any and all drug and alcohol testing is intact before reporting a test as positive.

Note Dr Gavryck is: 1. Certified by ASAM; 2. A .Certified Medical Review Officer (MRO) who “serves PHS in this capacity.” Although Dr. Gavryck serves PHS I would beg to differ on the MRO function. Accessed from PHS Website 1/15/2015 http://www.massmed.org/Physician_Health_Services/About/PHS_Associate_Directors/#.VM1dZlXF-hY
Dr. Gavryck evidently did not do that here. In fact for more than a year he helped cover up an alcohol test that was intentionally fabricated at the behest of PHS Director of Operations Linda Bresnahan (who told me when I confronted her with the fact that I have never had or ever even been suspected of having an alcohol problem “you have an Irish last name–good luck finding anyone who will believe you!”
It took a formal complaint with the College of American Pathologists to get the truth out. The whole fiasco can be seen here and here.
What Gavryck and his co-conspirators did is egregious and ethically reprehensible. It shows a complete lack of moral compass and personal integrity. What was done from collection to report to coverup and everything in-between is indefensible on all levels (procedurally, ethically, and legally).
The documentary evidence shows with clarity that this was not accident or oversight. It was intentional and purposeful misconduct. I think everyone would agree that there should be zero-tolerance for forensic fraud in positions of power. Any person of honor and civility would agree.
Transparency, regulation, and accountability are necessary for these groups. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. I’ll erase my blog and vanish into the woodwork. But If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Sanchez and Bresnahan (much like Annie Dookhan) he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths.
Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
It is people just like this who are killing physicians across the country. The body count is vast and multiple. And those who are caught doing dirty deeds such as this need to be held accountable.
Please help me get this exposed, corrected, and rectified. The doctors of Massachusetts and the doctors of this entire country deserve better than this.

The MRO Code of Ethics–Seems like Dr. Gavryck’s breaking them in sequential order!

