Many say a controversial program designed to help doctors with mental health issues is out of control, destroying careers and causing some doctors to commit suicide.

Author: Investigative Reporter: PJ Randhawa, Erin Richey
Dr. Gary Hammen admits that he was tired on the job.
In 2017, he had a newborn at home and a packed schedule as an anesthesiology resident, on top of a sleep disorder stemming from an injury he got serving our country as a soldier overseas.
But to him, the questions his supervisors asked crossed a line.
“They asked me, is this a drug problem? Are you sure you’re not using drugs?” he recalled. “I was floored.”
The questions came after months of exhaustion for Hammen.
Hammen says repeated, 24-hour shifts were taking their toll on his mental and physical health. Most weeks, he worked more than ninety hours and slept no more than four hours a night.
More than a year earlier, he met with his supervisors to tell them about his sleep disability, and offer them schedule recommendations from his sleep doctor.
He says supervisors promised, but failed to make any accommodation to his schedule or his sleep disability.
Weeks after his supervisors asked him about drugs, he got a call that made him think they didn’t believe him.
An organization called a Missouri Physician’s Health Program wanted him to fly to an addiction recovery center in another state, to be checked out.
Hammen couldn’t believe what was happening. “I had a bad feeling about it,” he said. “The whole thing just felt wrong.”
But he had no choice; colleagues warned him that if he didn’t follow the PHP’s requirements, he could lose his license and his career.
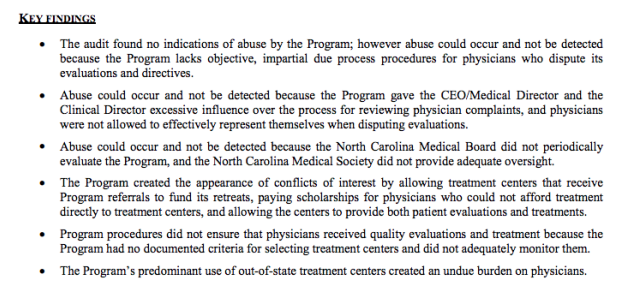
PHPs, or Physician’s Health Programs, are meant to help doctors with addiction or other psychological problems. But some, including Hammen, claim that doctors are sometimes falsely accused and getting help that they don’t need. They say the result drains their savings, endangers their licenses, and has even led some young doctors to take their own lives.
Nearly every state has a PHP. Some states have more than one. They started in the 1980s, often with closeties to the state’s medical boards or hospital associations. Medical industry professionals told 5 On Your Side’s I-Team that now big money is involved, and the lack of regulation turned a well-meaning measure into something that doctors fear even when they need help.
Dr. Wes Boyd of Harvard University is one of the skeptics. He used to work for a state PHP. Now he and others have raised concerns about these programs in the American Medical Association’s Journal of Ethics and in other respected publications.
“The physician is basically at the mercy of the PHP,” said Boyd. “There is no one outside the program looking at them, monitoring their practices and making sure that they’re really acting in a benevolent way.”
Boyd told us that when a PHP gets a tip about a supposed problem doctor, there is usually no way for the physician to appeal or dispute it. Instead, he or she must go to a “preferred” treatment center for evaluation. That center has complete authority to decide which doctors need treatment and how much.
Hammen made the flight to a treatment center, where evaluators made an unusual diagnosis. They said he had “provisional alcohol disorder,” something Hammen never heard of before.
“They hadn’t even talked to my wife to see if I drink. Most people wouldn’t make that sort of diagnosis without talking to some sort of outside person beside the patient,” said Hammen.
That diagnosis, Hammen thought, came from the fact that he told evaluators he and his wife shared a bottle of wine over the course of several dinners that week. It’s the only thing listed in the part of his evaluation describing his alcohol use.
Many of the treatment centers that PHPs refer doctors to are for-profit and specialize in addiction, even though doctors enter PHP monitoring because of stress and depression as well.
The I Team found many of the “preferred” treatment centers also donate money to the PHP trade organization: the Federation of State Physician Health Programs (FSPHP). Newsletters on the FSPHP website show several treatment centers are donors and exhibitors at FSPHP events.
Boyd told the I-Team that the bottom line motivates the centers to push doctors into treatment regardless of whether it’s really needed.
“Even in cases where there was no substance dependence, these centers come back and say, ‘You need to stay for 30 or 90 days of treatment,’” he said. “It is very hard not to think that financial motivations were behind the misdiagnoses.”
That can mean weeks of being unable to work, attending a treatment center that might not even offer services that doctors really need, with no way to get a second opinion or to choose their own care.
Even doctors who need help find the system difficult to navigate, with a high price to them and their community. Karen Miday once hoped that her son would get to help the community as a Cancer Specialist, but now he’ll never get that chance.
The words he left behind in a suicide note are so painful that she never took it out of the police department’s evidence envelope. But she read them to KSDK’s PJ Randhawa to show what he was feeling at the end of his life.
“That ‘I love you’ line stays with me,” she said.
“This is just the end of the line for my particular train,” Dr. Greg Miday wrote. “Earth wasn’t a great place for me.”
Dr. Greg Miday was 29 years old when he finished his residency in St. Louis in 2012. Friends and colleagues described him as bright, talented, and gentle. Under the surface, he also battled a drinking problem.
Miday’s last phone call was to the Missouri PHP. Karen Miday believes they had a chance to help him.
“I think all they needed to do was say, get yourself to a place of safety, you know, we’re behind you. That was all they needed to do,” she said.
Dr. Miday had been to one of the program’s approved out-of-state treatment centers before, where he followed the PHP’s requirements exactly. Then, just as he was about to start a new fellowship, he had a relapse.
Karen told the I-Team that he knew he needed help, but he also didn’t want to lose his new job. He suggested to the PHP that he could go to the outpatient program at a recovery center in St. Louis. This would let him keep his job and get treatment.
When Dr. Miday called the Missouri PHP, they said he must go to one of their “preferred” centers outside of the state. If he didn’t, the organization said, they would report Dr. Miday to the medical board.
“I think he thought there was no way out,” Karen said. “They have dual agency. It’s like being a policeman and a therapist at the same time.”
The list of approved facilities for Missouri physicians to get treatment includes just one in the state of Missouri. The nearest out-of-state option is in Lawrence, Kan.
“There’s no legitimate reason why they should have that handful of centers around the country that they prefer to use,” said Boyd.
“You start thinking after a while if there’s some diagnosing for dollars going on because now it’s not just substance use disorders, but now the “disruptive physician” and they’re talking about aging physicians,” said Miday.
Many doctors told the I-Team that the same lack of options that Dr. Miday felt is the reason that they fear contacting their local PHP when they really need help. That could put you at risk.
“If they’re afraid to ask for help, the chance that you’re going to get a doctor who shouldn’t be taking care of patients that day, goes up. And you won’t even be able to know what the chances that that’ll happen. Because nobody will say anything,” said Hammen.
The I-Team reached out to the Missouri Physician’s Health Program with questions, and even went to the home of program director Bob Bondurant, RN, to ask them. He declined to talk about the doctors’ concerns, as did the Missouri Medical Association, and the Missouri Board of Healing Arts.
The National Federation of State PHPs declined to answer any of our specific questions about how their programs work. Instead, they issued this statement:
“Physician Health Programs (PHPs) across the United States and Canada provide physicians and other health care professionals a resource to ensure they are healthy, can practice their craft and at the same time ensure public safety. Today’s physicians often suffer from stress and burnout. A smaller number develop substance use disorders and depression. We are a ready resource to physicians with such untreated conditions who would otherwise be at risk to the public an/or face loss of licensure by their state medical board. PHPs lessen the significant barriers that stand in the way of physicians asking for help.
Treatment is necessarily different for those in safety-sensitive professions, such as pilots and physicians; PHPs help physicians access care specifically designed to their needs. Our goal is to restore physicians’ lives and safely return them to patient care. Research as shown that the PHP care model has unmatched long-term consequences for substance use disorders. Additional research demonstrates successful graduates of PHP’s have a lower risk of malpractice.”
“There’s no legitimate reason why they should have that handful of centers around the country that they prefer to use,” said Boyd.
“You start thinking after a while if there’s some diagnosing for dollars going on because now it’s not just substance use disorders, but now the “disruptive physician” and they’re talking about aging physicians,” said Miday.
Many doctors told the I-Team that the same lack of options that Dr. Miday felt is the reason that they fear contacting their local PHP when they really need help. That could put you at risk.
“If they’re afraid to ask for help, the chance that you’re going to get a doctor who shouldn’t be taking care of patients that day, goes up. And you won’t even be able to know what the chances that that’ll happen. Because nobody will say anything,” said Hammen.
The I-Team reached out to the Missouri Physician’s Health Program with questions, and even went to the home of program director Bob Bondurant, RN, to ask them. He declined to talk about the doctors’ concerns, as did the Missouri Medical Association, and the Missouri Board of Healing Arts.
The National Federation of State PHPs declined to answer any of our specific questions about how their programs work. Instead, they issued this statement:
“Physician Health Programs (PHPs) across the United States and Canada provide physicians and other health care professionals a resource to ensure they are healthy, can practice their craft and at the same time ensure public safety. Today’s physicians often suffer from stress and burnout. A smaller number develop substance use disorders and depression. We are a ready resource to physicians with such untreated conditions who would otherwise be at risk to the public an/or face loss of licensure by their state medical board. PHPs lessen the significant barriers that stand in the way of physicians asking for help.
Treatment is necessarily different for those in safety-sensitive professions, such as pilots and physicians; PHPs help physicians access care specifically designed to their needs. Our goal is to restore physicians’ lives and safely return them to patient care. Research as shown that the PHP care model has unmatched long-term consequences for substance use disorders. Additional research demonstrates successful graduates of PHP’s have a lower risk of malpractice.”





 The excerpt above is taken from the 2006
The excerpt above is taken from the 2006 











 and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability. PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.
PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.