Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Although he specifies the numerical percentage “in physicians at 7.9%,”3 he avoids the use of numbers (14.6%) in the general population. He instead uses the qualifier “somewhat less.” Why is this?
My guess is because it understates the statistical fact that the prevalence found by Kessler in the general population was almost twice that found by Hughes in physicians.
You see, “Somewhat less” is a “detensifier.” It creates an impression of a small disparity between doctors and the general population.
In propaganda this is what is known as a “weasel phrase.” Weasel phrases are used to obfuscate the truth. Weasel phrases mislead those either without the time, or without the sense to see or look any deeper. The problem is it works.
“Methodologic differences may account for this difference,” Earley states, as the Hughes study “surveyed 9, 600 physicians by mail” and “relied on honest and denial-free reports by the physicians; the Kessler study utilized face-to-face interviews with trained interviewers.”1
This is an example of language framing. Language framing uses words and phrases to direct attention to a point of view to advance a vested interest.
In this case the use of the phrase “honest and denial free” in the context of physician reporting imparts associative meaning to the reader.
As denial is a recurring motif and cardinal attribute of physician addiction according to the paradigm, the connotation is that the reports by physicians may have been influenced by dishonesty and denial while face-to-face interviews done by “trained” interviewers were not.
“Framing” is another propaganda technique designed to tell the audience how to interpret the information given through context. The message here is that the somewhat less lifetime prevalence of substance abuse and addiction in physicians found by anonymous mail survey may be underreported as a result of both methodology and denial.
But in actual fact there is a large body of research regarding “social desirability bias” that shows the converse to be true.
One of the most consistent findings of studies of this kind is that socially desirable responding is significantly more likely with face-to-face administered data collection compared with self-administered anonymous modes.4-6
Tourangeau et al. reviewed seven studies comparing self-reports of drug use in surveys conducted in different modes. For each estimate obtained in the studies they calculated the ratio of drug use reported in self-reported surveys to the corresponding estimates in interviewer administered surveys and found that 57 of 63 different comparisons showed higher levels of reporting of drug use in the self-reported mode.7
The principal cause of social desirability bias is the level of perceived anonymity of the reporting situation.7
Evidence-based research does not support Earley’s claim that methodological differences in study design explain the difference in reported lifetime prevalence of substance abuse or addiction between physicians and the general population in these two studies.
Evidence based research would, in fact, make the findings more robust.
Moreover, I find it hard to comprehend the psychodynamics, motivation, and logic of denial and dishonesty in influencing an anonymous survey. So too would anyone else who dare peer beneath the veil. It is, in fact, a Potemkin village. In reality the emperor has no clothes.
Earley PE. Physician Health Programs and Addiction among Physicians. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed. Baltimore: Lippincott Williams & Wilkens; 2009:531-547.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Sudman S, Bradburn NM. Response effects in surveys: A review and synthesis. Chicago: Aldine Publishing; 1974.
Tourangeau R, Smith TW. Collecting sensitive information with different modes of data collection. In: Couper MP, Baker RP, Bethlehem J, et al., eds. Computer assisted survey information collection. New York: John Wiley & Sons, Inc.; 1998.
Dillman DA. Mail and telephone surveys: The total design method. New York: Wiley-Interscience; 1978.
Tourangeau R, Rips LJ, Rasinski KA. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000.
American Society of Addiction Medicine: Patient Placement Criteria. Chevy Chase, MD: American Society of Addiction Medicine; 2000.
Merlo LJ, Gold MS. Successful Treatment of Physicians With Addictions: Addiction Impairs More Physicians Than Any Other Disease. Psychiatric Times. 2009;26(9):1-8.
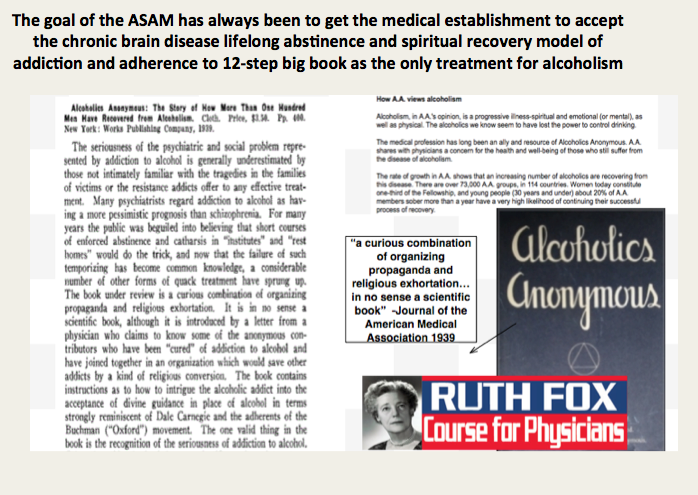
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
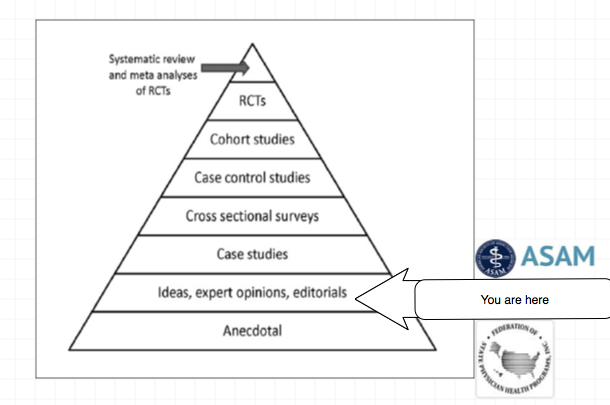
In order to comprehend the current plight of the medical profession and the dark clouds that lie ahead it is necessary to understand the history of the “impaired physician movement” and the American Society of Addiction Medicine (ASAM).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”1
The impaired physician movement emphasizes disease and therapy rather than discipline and punishment and believes that addiction is a chronic relapsing brain disease requiring lifelong abstinence and 12-step spiritual recovery. The drug or alcohol abuser or addict is a person lacking adequate internal controls over his or her behavior; for his own protection as well as the protection of society external restraints are required including involuntary treatment.
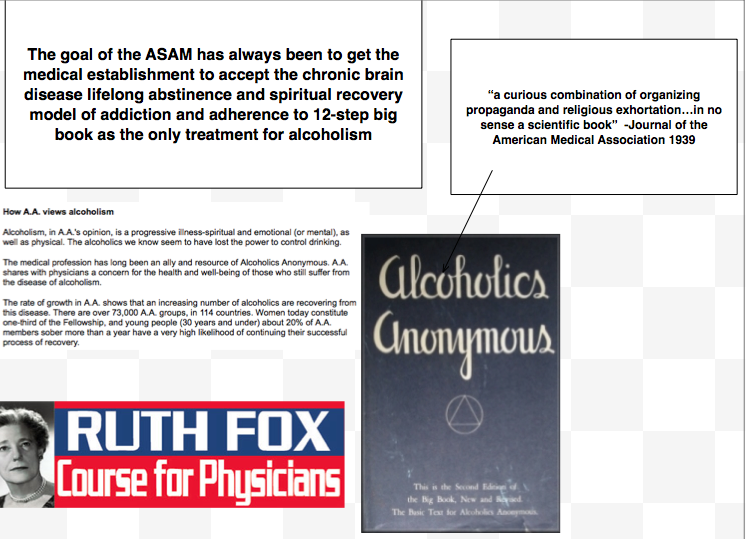
The American Society of Addiction Medicine (ASAM) can trace its roots to the 1954 founding of the New York City Medical Society on Alcoholism (NYCMSA) by Ruth Fox, M.D whose husband died from alcoholism.
Finding that alcoholics in her psychoanalytic practice did not recover when she used conventional analytic approaches, she taught her patients about alcoholism as a disease and introduced “them to AA meetings held in her living room.”2
A number of physicians in the New York Medical Society were themselves recovering alcoholics who turned to Alcoholics Anonymous for care.3
The society, numbering about 100 members, established itself as a national organization in 1967, the American Medical Society on Alcoholism (AMSA).3
The group promoted the concept of alcoholism as a chronic relapsing disease requiring lifelong spiritual recovery through the 12-steps of AA.
In 1973 AMSA became a component of the National Council on Alcoholism (NCA), now the National Council on Alcoholism and Drug Dependence (NCADD) in a medical advisory capacity until 1983.
“Abstinence from alcohol is necessary for recovery from the disease of alcoholism” became the first AMSA Position Statement in 1974.2
In 1985 ASAM’s first certification exam was announced. According to Dr. Bean-Bayog, chair of the Credentialing Committee:
“A lot of people in the alcoholism field have long wanted physicians in the field to have a high level of skills and scientific credibility and for this body of knowledge to be accredited.”2
And in 1986 662 physicians took the first ASAM Certification Exam.
By 1988 membership was over 2,800 with 1,275 of these physicians “certified” as:
“having demonstrated knowledge and expertise in alcoholism and other drug dependencies commensurate with the standards set forth by the society.”4
“While certification does not certify clinical skill or competence,” the Board explained, “it does identify physicians who have demonstrated knowledge in diagnosis and treatment of alcoholism and other drug dependencies.”5
Somehow, I don’t think this is quite what they had in mind!
Achieving “recognized board status for chemical dependence” and fellowships in “chemical dependency” are among the five-year objectives identified by the group. These are to come to fruition by “careful discussion, deliberation, and consultation” to “determine its form and structure and how best to bring it about.”5
The formation of ASAM State Chapters begins with California, Florida, Georgia, and Maryland submitting requests.6
In 1988 the AMA House of Delegates votes to admit ASAM to the House. According to ASAM News this “legitimizes the society within the halls of organized medicine.”2
In 1989 the organization changes its name to the American Society of Addiction Medicine (ASAM).2
Since 1990, physicians have been able to list addiction medicine as a self-designated area of practice using the specialty code “ADM.”
By 1993 ASAM has a membership of 3,500 with a total of 2,619 certifications in Addiction Medicine.
The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”7
Ninety physicians become Fellows of the American Society of Addiction Medicine (FASAM) in 1996 “to recognize substantial and lasting contributions to the Society and the field of addiction medicine.”8
Among the honorees are Robert DuPont, G. Douglas Talbott, Paul Earley, and Mel Pohl. In addition to at least five consecutive years of membership and certification by the Society, Fellows must have “taken a leadership role in ASAM through committee service, or have been an officer of a state chapter, and they must have made and continue to make significant contributions to the addictions field.”8
The American Board of Addiction Medicine (ABAM) is formed in 2007 as a non-profit 501(C)(6) organization “following conferences of committees appointed by the American Society of Addiction Medicine” to “examine and certify Diplomats.”9
In 2009 National Institute on Drug Abuse (NIDA) Director Nora Volkow, M.D., gives the keynote address at the first ABAM board certification diploma ceremony.10
According to an article in Addiction Professional “Board certification is the highest level of practice recognition given to physicians.”
“A Physician membership society such as ASAM, however, cannot confer ‘Board Certification,’ ” but a“ “Medical Board such as ABAM has a separate and distinct purpose and mission: to promote and improve the quality of medical care through establishing and maintaining standards and procedures for credentialing and re-credentialing medical specialties.”
The majority of ASAM physicians meet these requirements by “working in a chemical dependency treatment facility, taking continuing medical education courses in addiction, or participating in research.”11
“In the United States accredited residency programs in addiction exist only for psychiatrists specializing in addiction psychiatry; nonpsychiatrists seeking training in addiction medicine can train in nonaccredited ‘fellowships,’ or can receive training in some ADP programs, only to not be granted a certificate of completion of accredited training.”11
Specialty recognition by the American Board of Medical Specialties, fifty Addiction Medicine Fellowship training programs and a National Center for Physician Training in Addiction Medicine are listed as future initiatives of the ABAM Foundation in 2014.
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers, and consumers of health care products, and the general public’12
In this they have succeeded.
And in the year 2014 G.V. Stimson’s characterization of the “impaired physician movement” remains as accurate and apt as it was in 1985. But the “number of evangelical recovered alcoholic and addict physicians” has increased dramatically (outnumbering Addiction Psychiatry by 4:1) and their involvement in “ medical society and treatment programs” has been realized and enforced through the state Physician Health Programs and their “PHP-approved’ assessment and treatment centers.
Their“ability to make authoritative pronouncements on physician impairment…based on their own claim to insider’s knowledge” has become public policy and sanctified by Regulatory Medicine -essentially the Word of the Lord.
And the 1953 Alcoholics Anonymous prophecy that “With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world” is also coming to pass.
Stimson GV. Recent developments in professional control: the impaired physician movement in the USA. Sociology of health & illness. Jul 1985;7(2):141-166.
Four Decades of ASAM. ASAM News. March-April 1994, 1994.
Freed CR. Addiction medicine and addiction psychiatry in America: Commonalities in the medical treatment of addiction. Contemporary Drug Problems. 2010;37(1):139-163.
. American Medical Society on Alcoholism & Other Drug Dependencies Newsletter. Vol III. New York, NY: AMSAODD; 1988:12.
Ursery S. $1.3M verdict coaxes a deal for doctor’s coerced rehab. Fulton County Daily Report. May 12, 1999b 1999.
. AMSAODD News. Vol III. New York, NY: American Medical Society on Alcoholism & Other Drug Dependencies; 1988.
Membership Campaign Update. ASAM News. Vol VIII: American Society of Addiction Medicine; 1993:11.
. ASAM News. Vol 12. Chevy Chase, MD: American Society of Addiction Medicine; 1997:20.
Tontchev GV, Housel TR, Callahan JF, Kunz KB, Miller MM, Blondell RD. Specialized training on addictions for physicians in the United States. Substance abuse : official publication of the Association for Medical Education and Research in Substance Abuse. Apr 2011;32(2):84-92.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.” The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical Society updated its mission to read:
“The purposes of the Massachusetts Medical Society shall be to do all things as may be necessary and appropriate to advance medical knowledge, to develop and maintain the highest professional and ethical standards of medical practice and health care, and to promote medical institutions formed on liberal principles for the health, benefit and welfare of citizens of the commonwealth.”
With a foundation and history built and based on of scholarship and critical thought we need to support the highest levels of science, fact, intelligence and reason. Stupidity tries but it should not rein. Before the Boston Society for the Diffusion of Useful Knowledge in 1842, Dr. Oliver Wendell Holmes delivered two long lectures entitled “Homeopathy and Its Kindred Delusions.” He characterized one of its popular practitioners, Dr. Robert Wesselhoeft, as one of those:
“Emperics [quacks], ignorant barbers, and men of that sort…who announce themselves ready to relinquish all the accumulated treasure of our art, to trifle with life upon the strength of these fantastic theories.” That “pretended science” as Holmes called it, was “a mingled mass of perverse ingenuity, of tinsel erudition, of imbecile credulity, and artful misrepresentation, too often mingled in practice…with heartless and shameless imposition.”
And Holmes words are as apt and appropriate today as they were in mid 19th Century Boston! Probably more so.
History has recurrently proved that false constructs and groundless concepts allow for endless error.
The Massachusetts Medical Society needs to come to the realization that Physician Health Services is engaging in procedural, ethical and legal breaches. The evidence is clear that past medical director Dr. Luis Sanchez and Director of operations Linda Bresnahan are engaging in not only unethical but criminal activity within the walls of the MMS. Egregious misconduct including forensic fraud and political abuse of psychiatry can be seen in detail here, here and here.This is not a matter of opinion but a matter of fact. It has been ascertained by outside agencies and can also be confirmed by two former associate directors at PHS. What more does the MMS need? This type of misconduct can have grave and far reaching consequences for referred doctors and needs to be addressed urgently with precise, firm methods. To ignore the problem or suggest that it does not exist will only cause more damage.The majority of Massachusetts Medical Society members are honest, thoughtful and responsible. Most are unaware of the ethical and criminal allegations concerning PHS.. It is time they become aware as sunshine is the best disinfectant. As the most crucial step in solving a problem is admitting it exists I am requesting this be ascertained or refuted based on the documents and examined procedurally, ethically and legally. If there is no problem then the MMS should have no problem supporting or justifying the actions of Dr. Luis Sanchez, Dr. Wayne Gavryck and Linda Bresnahan. If the MMS cannot justify, support or defend these actions then it must be concluded that these individuals have violated professional protocol,, professional and community ethics and the law. And if that is the case it is the responsibility of the MMS to admit the problem exists, define it and address it. It is the responsibility of the MMS to facilitate exposure and that those engaged in wrongdoing be held appropriately accountable for their actions. I am sure no one at the MMS would disagree that forensic fraud be met with Zero-tolerance. The criminal and ethical violations shown here do not comport with any codes of conduct including those of the medical society. Those engaging in forensic fraud must be removed.
Good leadership requires correct moral and ethical behavior of both the individual and the organization. . Integrity is necessary for establishing relationships of trust. It requires a true heart and an honest soul. People of integrity instinctively do the “right thing” in any and all circumstances. Adherence to ethical codes of the profession is a universal obligation. It excludes all exceptions. Without ethical integrity, falsity will flourish.
The documentary evidence here shows fraud. It is intentional. All parties involved knew what they were doing, knew it was wrong but did it anyway. The schism between pious rhetoric and reality is wide.
One measure of integrity is truthfulness to words and deeds. These people claim professionalism, ethics and integrity. The documents show a reality of hypocrisy and sanctimony. But the hypocrisy seen here is also a danger because the careers and lives of doctors in Massachusetts are in these peoples hands.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.”The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical…
The article below was published in the now defunct magazine Gray Areas almost twenty years ago. (Vol. 4, No. 1, Spring 1995 pp. 75-77). Antipolygraph.og founder George Maschke noted in 2008 that article “makes a good introduction to the pseudoscience of polygraphy” and “the criticisms of polygraphy remain valid today.” They still do.
The Art of Deception: Polygraph Lie Detection
By Michael Lawrence Langan, M.D.
I’d swear to it on my very soul, If I lie, may I fall down cold.”
– Rubin and Cherise
(Hunter/Garcia)
The accuracy of polygraphic lie detection is slightly above chance. Nevertheless, State and local police departments and law enforcement agencies across the United States are devoted proponents of this unscientific and specious device. In addition, the American public seems to lend an implicit credence to the “lie detector” as evinced by its ubiquitous use on television crime shows and in “whodunit” literature. It is given overt attributions of credibility on tabloid type talk shows and news shows. For example, in the highly publicized case of Tonya Harding a reporter stated, not with removed objectivity but with sardonic grin and mocking emphasis, that the accused had failed two polygraph tests. The implied assumption is that if the person has failed the polygraph test, then therefore he or she is guilty regardless of other evidence. Bottom line. Culpa ex machina. End of story.
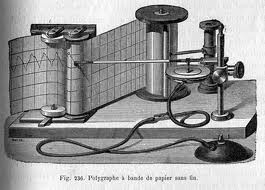
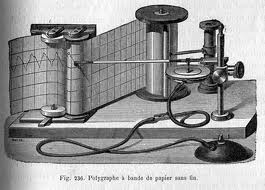
Lie detection by the polygraph is based on the premise that the act of telling a lie causes specific, universal, and reproducible physiological responses as manifested by the autonomic nervous system. (Saxe, 1991) These physiological responses, which are largely outside the influence of voluntary control, are then measured by the polygraph instrument. The polygraph itself is simplistic in design. It consists of several devices which are attached to the subject to record blood pressure, pulse, respiration, and galvanic skin response (which is related to perspiration). The results are then recorded on a moving paper by a “kymograph.” Hence any change of one of the autonomic nervous system variables will be recorded on the paper as a change from baseline. The polygraph examiner then interprets the tracing. A characteristic change from baseline on a relevant question is interpreted as a lie.
In fact, the polygraph test does measure autonomic nervous system activity. The role of the autonomic nervous system with its sympathetic and parasympathetic branches is well defined within the field of medicine, and was well described by the French physician Claude Bernard over a century ago. The primary role of the autonomic nervous system is to maintain bodily homeostasis to allow the individual to exist in a changing environment.
Simplistically described, the autonomic nervous system is a part of the peripheral nervous system which consists of a variety of outgoing nerve pathways that regulate important physiological functions generally outside of voluntary and conscious control. Thus, respiration, body temperature, heart rate, digestion, sweating, and blood pressure are all, partly or entirely, regulated by the autonomic nervous system. It is divided into sympathetic and parasympathetic branches which have contrasting functions in terms of effect. The sympathetic branch increases heart rate, respiratory rate, blood pressure, and perspiration. It is active at all times but varies with the constantly changing environment, and is especially active during rage or fright and prepares the body for the so called “fight or flight” phenomenon. Many of these reactions are caused by the release of epinephrine. The parasympathetic nervous system, on the other hand, is primarily involved with conservation and restoration. It is the sympathetic branch of the autonomic nervous system that the polygraph measures in terms of its activity. Thus, from a medical perspective it is entirely valid that the polygraph will accurately measure sympathetic nervous system activity with its instrumentation.
The false assumption of the polygraph test is that dishonesty is the sole cause of sympathetic arousal during a polygraph examination. Deception is a cognitive phenomenon that cannot be measured. Indeed, throughout the entire history of medicine there has not been a single scientific study that demonstrated evidence that a cognitive phenomenon (such as love, hatred, truth, altruism, jealousy) could be measured. Since, in the complex realm of truth and deception, there is no known physiological response that correlates with lying, then there is no validity to the test. Although the act of lying can elicit fear and anxiety via the sympathetic nervous system, so can multiple other confounding and complex emotional factors including stress, embarrassment, anger, and fear. “Deception itself cannot be measured directly.” (Steinbrook, 1992) In addition, each individual differs in autonomic lability. Some people stay calm with a gun at their head. While others get autonomically excited, with heart thumping and palms sweating at simply shaking someone’s hand.
In reality, the examination itself is inherently designed to elicit fear and anxiety. It is an interrogation. If this fear and anxiety are recorded on a relevant question, then you have failed that question according to the polygraph “experts.”
The polygraph technique begins with a pre-test. After a sixth-grade level lecture on the nervous system and a proclamation of the test’s infallibility, the examiner will go over all of the questions that have been formulated.
These questions consist of control questions, relevant questions, and irrelevant questions. The subject will then be attached to the polygraph equipment and the formal testing begins.
The most crucial questions on the polygraph examination, or “Control Question Test,” are the control questions and relevant questions. The control questions are garnered from the suspect by asking him an innocuous question which could not be truthfully denied. For example, “Have you ever thought of hurting someone?” or “Have you ever lied to anyone?” The responses to the control questions will elicit some degree of autonomic activity which can then serve as a baseline for which to compare subsequent questions. The relevant questions pertain to the actual investigation at hand. The magnitude of responses to relevant questions and control questions as compared with the irrelevant questions is then interpreted, in a non-blinded manner, by the examiner. The assumption is, that if you are prevaricating, the relevant questions will cause a greater response than the control questions. So if the question “Have you ever been late for an appointment?” (control question) elicits less of an emotive response on the polygraph equipment than “Did you murder and rape your girlfriend?” (relevant question) you have failed the test. And, according to the American Polygraph Association (APA) you are lying. Assuming the subject is innocent, it is fairly obvious that he would respond with more emotional autonomic activity to a question regarding a recently deceased loved one than he would an inquiry about punctuality. Obvious to everyone, that is, but the APA.
The APA is a professional organization for polygraph examiners who have complete faith in the accuracy of the test. They have their own trade journalPolygraph in which they report scientifically worthless studies and brandish anecdotes of the wonders of their trade. The majority of these members can pride themselves on completing a 6 week to 6 month post- high school training course in the art of polygraphy. They have no formal training in medicine, psychology, physiology, or behavior; the very disciplines on which the testing is based. The majority of them cater to the legal system wherein their economic livelihood depends.
Since they are primarily paid to identify guilty suspects, motivational factors may play a part in their eagerness to find the guilty suspect. (Kleinmuntz, 1987)
The accuracy of any test is determined by that test’s sensitivity (ability to find a positive) and specificity (ability to find a negative). A polygraph examiner will ardently tell you that the exam has somewhere in the neighborhood of a 95% sensitivity rate. This means that if 100 guilty suspects are given a polygraph exam, 95 of them will be detected through the test. Only five of the 100 will be a false negative and not be detected by this miraculous method. Likewise they will claim a similar specificity rate, and state that if you are telling the truth then you have almost a 100% chance of being cleared by the test. John Reid, the inventor of the Control Question Test claimed 99% accuracy. (Reid and Inbau, 1977)
This is clearly not accurate. The polygraph was not subjected to much critical and scientific investigation until the last two decades. (Saxe, et al., 1983) Since this time there have been a number of studies of sound scientific design and methodology which clearly refute the high specificity and sensitivity that polygraph advocates claim. These studies have appeared in reputable peer-reviewed journals and not trade publications. Horvath, for example, reported a sensitivity of 76 percent and a specificity of 52 percent. (Horvath, 1977) This means that out of 100 liars 76 of them will be detected by the polygraph. What is astonishing though is the specificity of 52 percent. This means that out of 100 people who are not lying, 52 will be identified as telling the truth while 48 of the honest individuals will be branded as liars. The odds are similar to that of a coin toss which would have a specificity of 50 percent. Barland and Raskin’s study actually demonstrated a specificity of 45%. Worse than a coin toss. (Barland and Raskin, 1976) Multiple other studies have shown similar results. (Brett, et al., 1986, Kleinmuntz and Szucko, 1984, Lykken, 1984).
The polygraph examiner likens his “skill” to that of the radiologist reading a chest X-Ray or a cardiologist interpreting an EKG. (Barefoot, 1974) This analogy is not only ridiculous but, in fact, if a medical test had a similar sensitivity and specificity to that of the polygraph examination it would simply not be used in the field of medicine. They will cite the fact that the polygraph has been used in the United States for greater than 70 years as if longevity is directly related to validity. They will state that they have personally administered hundreds or thousands of these tests, and have almost never been wrong, as if total number of tests given constitutes accuracy.
They are so convinced of the accuracy of the polygraph that they regard opponents of polygraphy as communists and do-nothing professors. (Arther, 1986) It doesn’t occur to them that someone with a Ph.D. and years of research experience, in the very subjects they ignorantly dabble in, may know something more than they do.
It is astounding that the criminal justice system has institutionalized and perpetuated a so called “technology” that lacks scientific evidence and is in fact rejected by the scientific community. It is as ludicrous as procuring the so called “love meter” machine from the amusement park which measures galvanic skin response and placing it in the courtroom. But in a backward legal system which has been known to use psychics to help with unsolved murders and has allowed the mentally retarded to serve as jurors, it is not entirely surprising.
The tool is useful to them, however, in that 25 to 50 percent of examinees will, under the tense psychological pressure of the exam, confess to the misdeed at hand. (Lykken, 1981, Lykken, 1991) Persuaded that they have been proven dishonest by “scientific” means they give up hope. It is usual for the polygraph examiner to interrogate the subject who has failed the test. They will state that there is no way now to deny the objective guilt demonstrated by this impartial and unbiased scientific device, and that the only available option is to confess.
The assessment by the polygrapher is genuinely convincing because, sadly, he believes it himself. Thus the instrument is clearly useful as a confession inducing device. One wonders, over the past 70 years, how many false confessions have been obtained in this way from innocent persons.
In summary, the polygraph is a ludicrous implementation of pseudo-science at its worst. The members of the APA are non-scientists practicing science, and the consequences are often dire. Lykken reports the cases of three men who were convicted of murder largely due to the polygraph examiner’s testimony that in their “expert opinion” they had failed the test. All three were subsequently found to be innocent. (Lykken, 1991) Polygraph examiners ignore such cases or rationalize that they are due to the rare incompetence of some examiners.
The continued use of polygraphic lie detection has the potential to cause much harm to those who are judged dishonest by its results. The specificity and sensitivity are not dissimilar to that of a coin toss. Innocent suspects have about a 50/50 chance. One failure is all it takes to ruin your life. Since the 1923 Federal Court decision of Frye vs United States (293 F 1013 [DC Cir 1923]), polygraph evidence has not been admissible in federal court cases because there was deemed a lack of scientific validity to the test. This travesty however is still used widely by the state court system. Furedy characterizes the continued use of polygraphy as a serious “social disease.” (Furedy, 1987) State laws regarding abuse of the polygraph must change, and it is time for the medical and scientific communities to educate lawmakers and policy makers about the true validity of this perversion of science. It must be forever banished to the same realm of parapsychology as the Ouija Board, phrenology, and palmistry. The relatively conservative American Medical Association’s Council on Scientific Affairs recommended that the polygraph not be used in pre-employment screening and security clearance. (Council on Scientific Affairs, 1986) It is time to extend this recommendation across the board, and put the greater than 3000 anachronistic polygraph examiners in the United States out of business.
Meanwhile, if you are asked to take a polygraph test–don’t do it. Those involved in the criminal justice system, including lawyers, are largely uneducated in the realm of scientific scrutiny and experimental methodology.
They may not separate science and pseudo-science, and erroneously believe that the polygraph is an accurate scientific instrument. Their interactions are with polygraph examiners who proselytize its use, and they have little or no interaction with scientists, psychologists, and physicians who refute its use. Refuse to take the test and educate them. Cite the Frye doctrine, go to the medical library, copy the scientific articles which belie its validity, and present them to whomever requested you to take the test. State that the principles and assumptions underlying polygraphy are not supported by our understanding of psychology, neurology, and physiology. Then put the burden of proof on their heads. Tell them to present you with scientific evidence that corroborates the validity of the test. There is simply no rational basis for a machine to detect liars.
References
Arther RO. 1986. The polygraph’s enemies: An update. Journal of Polygraph Science. 20: 133-136.
Barefoot J. 1974. The Polygraph Story. Cluett Peabody and Co., New York.
Barland, G, Raskin D. 1976. Validity and reliability of polygraph examinations of criminal suspects (Report 76-1, Contract 75 NI-99-0001).
Brett AS, Phillips M, Beary JF. 1986. Predictive power of the polygraph: Can the “lie detector” really detect liars? The Lancet. 1: 544-547.
Council on Scientific Affairs. 1986. Polygraph. Journal of the American Medical Association. 256: 1172-1175.
Furedy JJ. 1987. Evaluating polygraphy from a psychophysiological perspective: a specific-effects analysis. Pavlovian Journal of Biological Sciences.22: 145-151.
Horvath F. 1977. The effect of selected variables on interpretation of polygraph records. Journal of Applied Psychology. 62: 127-136.
Kleinmuntz B. 1987. The predictive power of the polygraph: The lies lie detectors tell. Journal of the American Medical Association. 257: 189-190.
Kleinmuntz B, Szucko J. 1984. A field study of the fallibility of polygraphic lie detection. Nature. 308: 449-450.
Lykken D. 1984. Polygraph Interrogation. Nature. 307: 681-684.
Lykken DT. 1981. A tremor in the blood: Uses and abuses of the lie detector. McGraw-Hill, New York.
Lykken DT. 1991. Why (some) Americans believe in the lie detector while others believe in the guilty knowledge test. Integrative Physiological and Behavioral Science. 26: 214-222.
Reid JE, Inbau FE. 1977. Truth and deception: The polygraph (“lie detector”) technique. Williams & Wilkins, Baltimore.
Saxe L. 1991. Science and the CQT polygraph: A theoretical critique. Integrative Physiological and Behavioral Science. 26: 223-231.
Saxe L, Dougherty D, Crosse T. 1983. Scientific validity of polygraph testing: a research review and evaluation. Conference: OTA-TM. U.S. Congress Office of Technology Assessment.
Steinbrook R. 1992. The polygraph test – A flawed diagnostic method. The New England Journal of Medicine. 327: 122-123.
The article below was published in the now defunct magazine Gray Areas almost twenty years ago. (Vol. 4, No. 1, Spring 1995 pp. 75-77). Antipolygraph.og founder George Maschke noted in 2008 that article “makes a good introduction to the pseudoscience of polygraphy” and “the criticisms of polygraphy remain valid today.” They remain valid in 2014.
The Art of Deception: Polygraph Lie Detection
By Michael Lawrence Langan, M.D.
I’d swear to it on my very soul, If I lie, may I fall down cold.”
– Rubin and Cherise
(Hunter/Garcia)
The accuracy of polygraphic lie detection is slightly above chance. Nevertheless, State and local police departments and law enforcement agencies across the United States are devoted proponents of this unscientific and specious device. In addition, the American public seems to lend an implicit credence to the “lie detector” as evinced by its ubiquitous use on television crime shows and…
It is only a few public policy steps and minor changes in state regulatory statutes before what is described in the ASAM White Paper on Drug Testing comes to fruition. Before we know it the Drug and Alcohol Testing Industries “New Paradigm” as described here by Robert Dupont will be ushered in. From the ASAM white Paper:
“THIS WHITE PAPER ENCOURAGES WIDER AND “SMARTER” USE OF DRUG TESTING WITHIN THE PRACTICE OF MEDICINE AND, BEYOND THAT,BROADLY WITHIN AMERICAN SOCIETY. SMARTER DRUG TESTING MEANS INCREASED USE OF RANDOM TESTING* RATHER THAN THE MORE COMMON SCHEDULED TESTING,* AND IT MEANS TESTING NOT ONLY URINE BUT ALSO OTHER MATRICES SUCH AS BLOOD, ORAL FLUID (SALIVA), HAIR, NAILS, SWEAT AND BREATH WHEN THOSE MATRICES MATCH THE INTENDED ASSESSMENT PROCESS. IN ADDITION, SMARTER TESTING MEANS TESTING BASED UPON CLINICAL INDICATION FOR A BROAD AND ROTATING PANEL OF DRUGS RATHER THAN ONLY TESTING FOR THE TRADITIONAL FIVE-DRUG PANEL.”
Backed by the multi-billion dollar drug and alcohol testing, assessment and treatment industry the public policy positions of the American Society of Addiction Medicine (ASAM) have invariably passed. There has been little if any meaningful opposition.
To prevent this future drug testing dystopia, that includes testing schoolchildren, we need to take a step back and analyze the reliability and credibility of the “evidence-base” behind these multiple non-FDA approved (Introduced as Laboratory Developed Tests (LDTs) to bypass FDA approval) “forensic” drug and alcohol tests and testing devices (The alcohol biomarkers EtG, EtS, PEth; SCRAM (Subcutaneous Remote Alcohol Monitoring Bracelet);CDPB (Cellular Digital Photo Breathalyzer); and Hair Testing- Psychemedics, etc.) the ASAM proposes be used on the population at large. These tests include nail, hair, saliva, breath, blood and urine and they plan on utilizing the Medical Profession as a urine collection agency by calling this testing a “medical evaluation” rather than “monitoring” for drug and alcohol use. This change in semantics enables them to bypass the usual forensic drug testing protocol (that includes strict chain-of-custody collection and MRO review) designed to minimize false-positives because the results of erroneous test can be grave and far reaching. According to the ASAM white paper the “clinical” collection of specimens as is good enough as the results of a positive test will result in “treatment” rather than “punishment.”
Amazingly, there has been no Academic review of these tests, let alone a Cochrane type critical analysis. It is essentially untapped territory. In addition there has been no Institute of Medicine type Conflict of Interest Analysis.
And that is why I am asking for help from statisticians, biostatisticians and epidemiologists. The task would entail a review of the literature prior to the introduction of these tests for evidence base of forensic applicability (there essentially is none) and a review of the literature peri-and post marketing of these devices to assess the reliability and credibility of the underlying methodology and ascertain the evidence-base. The goal would be publication in both academic journals and presentation to the general public through media publication with the assistance of investigative journalists and other writers. The goal is to get the truth out about these tests and allow both the medial profession and public at large to awaken to the menace this represents.
I can’t pay you but you would be combating injustice, corruption and dishonesty. You would be doing your part in helping the Medical Profession, honest and decent doctors, our country and perhaps our future.


 Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
























 Circa 1995
Circa 1995