 “One of the saddest lessons of history is this: If we’ve been bamboozled long enough, we tend to reject any evidence of the bamboozle. We’re no longer interested in finding out the truth. The bamboozle has captured us. It’s simply too painful to acknowledge, even to ourselves, that we’ve been taken. Once you give a charlatan power over you, you almost never get it back.”
“One of the saddest lessons of history is this: If we’ve been bamboozled long enough, we tend to reject any evidence of the bamboozle. We’re no longer interested in finding out the truth. The bamboozle has captured us. It’s simply too painful to acknowledge, even to ourselves, that we’ve been taken. Once you give a charlatan power over you, you almost never get it back.”
― Carl Sagan, The Demon-Haunted World: Science as a Candle in the Dark
Carl Sagan devised a toolkit for nonsense-busting and critical thinking, which includes these nine rules:
- Wherever possible there must be independent confirmation of the “facts.”
- Encourage substantive debate on the evidence by knowledgeable proponents of all points of view.
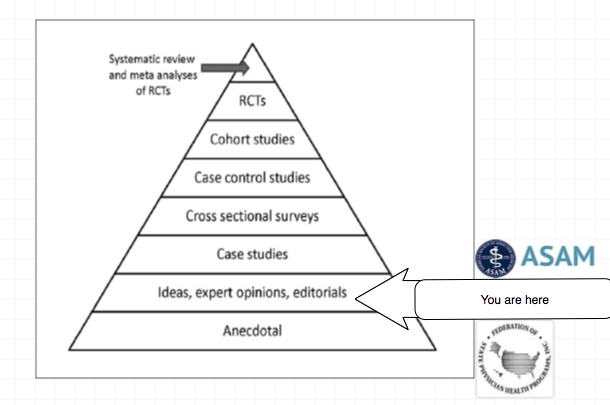
- Arguments from authority carry little weight — “authorities” have made mistakes in the past. They will do so again in the future. Perhaps a better way to say it is that in science there are no authorities; at most, there are experts.
- Spin more than one hypothesis. If there’s something to be explained, think of all the different ways in which it could be explained. Then think of tests by which you might systematically disprove each of the alternatives. What survives, the hypothesis that resists disproof in this Darwinian selection among “multiple working hypotheses,” has a much better chance of being the right answer than if you had simply run with the first idea that caught your fancy.
Try not to get overly attached to a hypothesis just because it’s yours. It’s only a way station in the pursuit of knowledge. Ask yourself why you like the idea. Compare it fairly with the alternatives. See if you can find reasons for rejecting it. If you don’t, others will.
- Quantify. If whatever it is you’re explaining has some measure, some numerical quantity attached to it, you’ll be much better able to discriminate among competing hypotheses. What is vague and qualitative is open to many explanations. Of course there are truths to be sought in the many qualitative issues we are obliged to confront, but finding them is more challenging.
- If there’s a chain of argument, every link in the chain must work (including the premise) — not just most of them.
- Occam’s Razor. This convenient rule-of-thumb urges us when faced with two hypotheses that explain the data equally well to choose the simpler.
- Always ask whether the hypothesis can be, at least in principle, falsified. Propositions that are untestable, unfalsifiable are not worth much. Consider the grand idea that our Universe and everything in it is just an elementary particle — an electron, say — in a much bigger Cosmos. But if we can never acquire information from outside our Universe, is not the idea incapable of disproof? You must be able to check assertions out. Inveterate skeptics must be given the chance to follow your reasoning, to duplicate your experiments and see if they get the same result.



A November 2014 Viewpoint article in the Journal of the American Medical Association entitled Addiction Medicine: Birth of a new Discipline describes the need for “integration of addiction specialty physicians throughout the health care system” and how they plan to accomplish this. Citing the 2012 “National Survey on Drug Use and Health” findings that only 11% of Americans in need of treatment recevied it, the authors conclude that the number of addiction psychiatry diplomates (1139) is not meeting the country’s “overwhelming need for addiction specialists. To close this “addiction treatment gap” they propose “greatly expanding addiction physician specialists to include physicians from internal medicine and other specialties.”
Lax Standards
The American Society of Addiction Medicine (ASAM) only requires that you complete a residency — any residency, even dermatology or surgery — plus one year of work in the field and then 50 hours of “education.” I took the test in 2010 and passed by a large margin without any preparation.

Remarkably, I received my “diploma” in the mail without every meeting or speaking with anyone. I simply paid the fee and took the test at one of the local testing centers. This is concerning as my prior board certifications required accredited residency and training programs and were dependent on not only successfully completing those programs academically but on the reports of my superiors documentation of my character and integrity. 
With these lax standards, the ASAM have been able to create a legion of board certified addictions specialists – outnumbering psychiatrists in the field by 3 to 1.
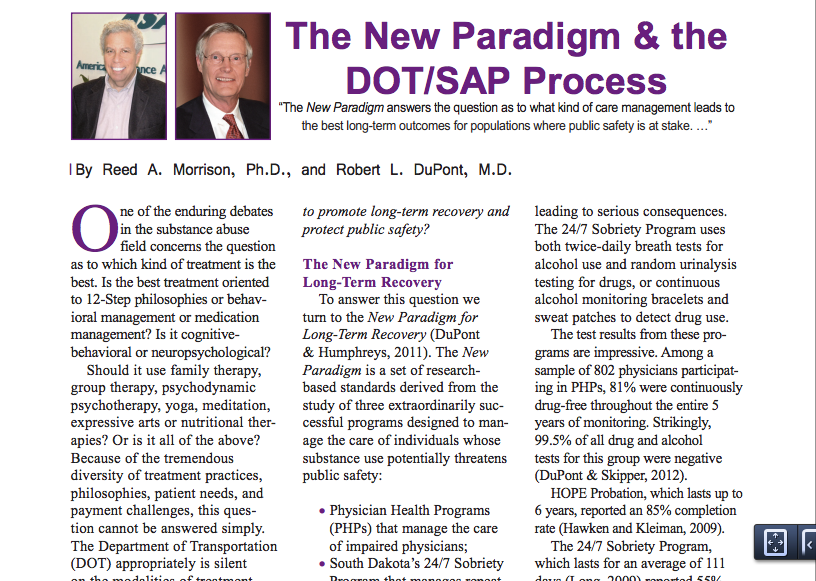
Takeover of state Physician Health Programs (PHPs)
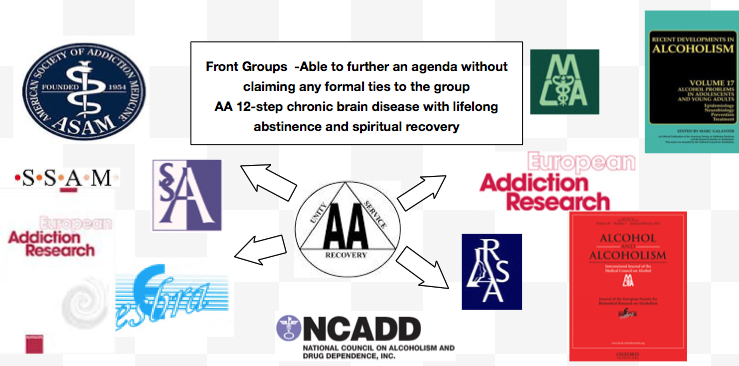
These ASAM “addiction experts” have become so numerous they have been able to take over almost all the state Physician Health Programs (PHPs). Their national association—the Federation of State Physician Health Programs (FSPHP)–has a stated goal of universal acceptance of the 12-step doctrine: lifelong abstinence, and spiritual recovery as the one and only treatment, as spelled out in the “PHP Blueprint.”
Very much like Straight, Inc in the 70s and 80s, they have cast a wide net with doctors to ensnare them in an endless loop of drug testing and rehab—whether the tests are fabricated or not. The doctors will enjoy no sympathy from the public, and complaining about it is deemed a sign of your “disease.” Furthermore, ASAM recommends that physicians only be referred to “PHP approved” facilities.
The medical directors of these facilities can all be found on this list of ”Like-Minded Docs.” Surprisingly, many Like-Minded Docs were former addicts and alcoholics, some even with criminal backgrounds. There are felons and even double-felons on the list.
It’s a rehab shell game. Heads I win tails you lose.
And the program is expanding. The organization that oversees the licensing for all medical doctors, the Federation of State Medical Boards, adopted a new policy and approved the concept of “potentially impairing illness” and the Orwellian notion of “relapse without use.”
Signals for “impairment can be as benign as not having “complete accurate, and up-to-date patient medical records” according to Physician Health Services, the Massachusetts PHP. Despite the overwhelming amount of paperwork physicians now have, incomplete or illegible records could be construed as a red flag, since as Associate Direct of PHS Judith Eaton notes “when something so necessary is not getting done, it is prudent to explore what else might be going on.” The question is, who is next?”
Not Just For Doctors, But for Everyone
Most of us are unaware of this quiet operation to police and punish our private choices. This is the New Inquisition: a move to expand this program to virtually all professions, all Americans. They want to replace the system currently being used in pilots, bus drivers, and Federal Employees with “comprehensive drug and alcohol testing” that consists of the Laboratory Developed Tests (LDTs) they introduced. Their goal is 24/7 sobriety with complete abstinence, and zero tolerance using tests of unverified validity and unknown reliability.
And they have an implementation plan. The American Society of Addiction Medicine (ASAM), bolstered by billions of dollars from forced rehab and mandatory drug testing, has a long reach and powerful political friends. ASAM plans to force your physicians to collect your urine in the name of preventive care.
That’s right, that free preventive care you’re getting under Obamacare might soon come packaged with drug screening, as outlined in the ASAM White Paper on Drug Testing. . Drug testing, they say, is “vastly underutilized” throughout healthcare. The White Paper—which is well worth reading—describes the use of drug testing “within the practice of medicine and, beyond that, broadly within American Society.”
No matter your profession, if you come for a check up, you may be unwittingly looped into being referred for “assessment” and “treatment” in a “PHP-approved” facility, where to get free, among other things, you will have to admit you are powerless and surrender to God.
If we don’t start pushing back now, soon there will be mandatory drug testing for every citizen.. A good case can be made for forced drug testing for virtually every profession –a few well-placed opeds in The New York Times and pretty soon we’ll begin to think it’s reasonable to test teachers, food handlers, you name it. They are even recruiting pediatricians to test children. And in the new system they will not have to change your test from “forensic” to “clinical.” A doctor-patient relationship renders the test “clinical” and by having doctors collect these specimens and calling the consequences “treatment” they can successfully use these unverified and unregulated tests introduced and marketed through a loophole into mainstream medical practice through a loophole.
One of the major goals of ASAM is recognition by the American Board of Medical Specialties. Should this occur it will inevitably lead to the end of Addiction Psychiatry and, by outnumbering them 3:1 it will be enveloped into the all encompassing field of “addiction medicine.” “Who needs two specialties?” they will argue, especially since most medical experts have accepted that addiction is a chronic relapsing “brain” disease.
And this legion of “authority” will infest our hospitals and mainstream medicine where they will join hospital formulary, ethics, research and other committees where they will be able to outnumber and outvote those of open mind and critical thought just as they did in the PHP system and the field of medicine will then be subverted to the guiding philosophy of the “impaired physicians movement.”
Addiction is a serious problem and those afflicted with it need proper assessment, diagnosis and treatment. This illegitimate and irrational authority does not provide that. Having had a disease does not confer authority status–I have asthma but that does not make me an expert in reactive airway disease. Neither does interest in something, no matter how sincere, make one an expert. I’ve had a sincere interest in science since I was a child but did not claim to be an expert in science when I was 7 because I was a member of Sir Isaac Newton’s Scientific Club. Aside from the $2200 I had to pay and sitting through the exam gaining ABAM certification was not all that different. This is not “expertise.”
Prior to accepting “addiction medicine” as an ABMS approved specialty their research, tenets and basic principles of should be subjected to critical reasoning and academic analysis of the Cochrane caliber to see if they are actually valid. This includes their claims of remarkable success in treatment and the non-FdA approved laboratory developed tests (LDTs) that they introduce.d. The authorities and experts involved in promoting the ideology, testing and treatment should be subject to and Institute of Medicine (IOM) conflict of interest analysis. Who is profiting? And all of the statements, claims and suppositions regarding addiction and the guiding philosophy of the group should be subjected to Carl Sagan’s Baloney Detection kit. If this were done the results would be failure on all three counts. False premises lead to false constructs.

One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model.
The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the LDT drug and alcohol testing and 12-step assessment and treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.