State Physician Health Programs -coercion, control and abuse.
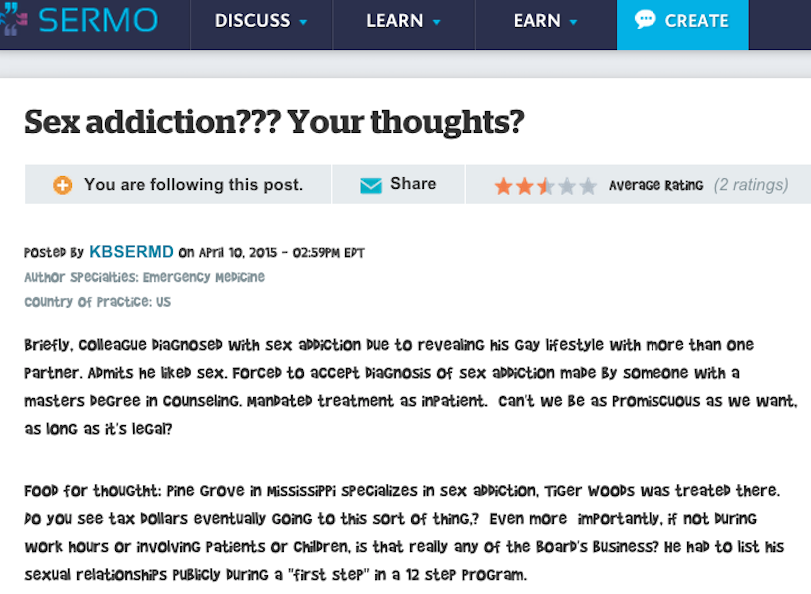
This anecdote concerning a gay doctor’s revelation he liked his non monogamous lifestyle leading to a forced acceptance of a “sex addiction” diagnosis, mandatory inpatient treatment and indoctrination into 12-step recovery was just posted on the physician social network SERMO. If the pattern looks familiar it is.
Physician Health Programs (PHPs) are non-profit NGOs that exist in every state ostensibly to help impaired doctors and protect the public from harm. PHPs have no regulation or oversight and have essentially removed all accountability. Under the ruse of protecting a doctors anonymity and providing confidentiality they have built barriers of opacity. Most doctors are unaware how they work unless they become involved with them and they are not on the radar of the public at large–they need to be.
Organized under the Federation of State Physician Health Programs, (FSPHP), state medical boards have abdicated their responsibility and consider them expert authority on all things related to physician health–a logical fallacy that has placed illegitimate and irrational authority in professional control of medicine once again proving that knowledge isn’t power and ignorance often reigns.
PHPs encourage confidential referrals for “warning signs” such as those on the list below from the Massachusetts PHP, PHS, Inc. and guarantee the reporters anonymity. All semblance of due process has been removed. Medical boards have given state PHPS complete and absolute managerial control over assessment, treatment and monitoring. PHPs are not healthcare providers but monitoring agencies. If a PHP recommends an “assessment” of a reported doctor there is no choice in the matter. No allowances for a second opinion, outside support or appeal exist.
This doctor was apparently reported to his state PHP because a patient thought she smelled alcohol on his breath. As it turned out, the accusation was bogus but by being honest and forthcoming about his sexual orientation in the interview the PHP mandated an “assessment.” for unrelated issues. A not uncommon scenario as reports of behavioral issues often end up with hair tests for alcohol and other substances resulting in mandated assessments for “substance use disorder” followed by a five-year monitoring contract with the PHP and weekly urine tests.
The PHP provides a list of three or four facilities drawn from the same pool of “PHP-approved” assessment and treatment centers. However, an audit of the N.C. PHP found no written objective criteria or quantitative measurements existed on how these assessment and treatment centers are “approved” by the PHP. The common denominator seems to be that these facilities are (1) 12-step ASAM directed, and (2) willing to “tailor” an assessment to support a predetermined diagnosis. It is, in fact, a rigged game. Unfortunately the medical boards have been duped into mandating assessments at these centers under threat of loss of medical license and specifically exclude non “PHP-approved” assessments.
This scaffold is also the unspoken and hushed major contributor to physician suicide—It is the elephant in the room no one speaks of out of fear of being targeted. Doctors who really need help for mental health, substance abuse or other issues are afraid to get it for fear of being reported to the PHP. Those already monitored are subject to all sorts of psychological, financial and emotional abuse.
The Federation of State Physician Health Programs (FSPHP) has a relationship with Pine Grove. It is one of the “PHP-approved” facilities and two of their staff, Phillip Hemphill, PhD and James C. “Jes” Montgomery, MD are are listed as Program Faculty at the FSPHP annual educational conference and business meeting on April 24-27, 2015 in Fort Worth Texas.

Political Abuse of Psychiatry
Political abuse of psychiatry is the “misuse of psychiatric diagnosis, detention and treatment for the purposes of obstructing the fundamental human rights of certain groups and individuals in a society. The coercive use of psychiatry represents a violation of basic human rights in all Cultures.
What has occurred in the medical profession is no different from China or the Soviet Union under totalitarian rule where dissent is disapproved, often punished, and those perceived as threats to the existing system can be effectively “neutralized with trumped up psychiatric illness” and by this stigmatization reputations were ruined, power was diminished, and voices were hushed.

Political abuse of psychiatry involves the deliberate action of diagnosing someone with a mental condition they do not have as a means of repression or control and if you do not believe it is occurring right here today then take a look here and here to see how they are colluding with commercial drug testing companies to engage in forensic fraud and the assessment and the treatment centers to fabricate data to support non-existent diagnoses.
“Sex Addiction” used as a tool to Discriminate
There has been a lot of “chatter” in PHP circles concerning “sex addiction” and I knew they had been aligning themselves and setting up specialized programs at certain facilities. It seemed unusual as many of the key players who erected and run this scaffold have themselves been involved in sexual misconduct. 

One of the architects of the current system, Dr. Robert Walzer, M.D., J.D. who was instrumental in tinkering with administrative and medical practice laws to remove the due process and appeal rights of doctors surrendered his license in 2001 due to inappropriate sexual relationships with patients. He was the co-author of the current physician health program paradigm.
Dr. Margaret bean-Byog, M.D, Chairman of the credentialing  committee for the first certification exam and ASAM president surrendered her medical license after being accused of sexually abusing one of her patients, a Harvard medical student who subsequently died by suicide.
committee for the first certification exam and ASAM president surrendered her medical license after being accused of sexually abusing one of her patients, a Harvard medical student who subsequently died by suicide.
 And the FSPHP seems to treat doctors involved in sexually related misconduct in a favorable light. Take for instance, Dr. James Peak, M.D., a child psychiatrist who was sent to prison on a federal child pornography conviction taken under the wing of the Montana PHP. After “proving” he only ‘”looked” at pornography of young boys but never abused any using a polygraph “lie-detector” test his license was reinstated in no time at all. His treatment includes going to one AA meeting and one 12-step sex addict meeting per week. My guess is they need more staff at the PHP or one of the assessment centers.
And the FSPHP seems to treat doctors involved in sexually related misconduct in a favorable light. Take for instance, Dr. James Peak, M.D., a child psychiatrist who was sent to prison on a federal child pornography conviction taken under the wing of the Montana PHP. After “proving” he only ‘”looked” at pornography of young boys but never abused any using a polygraph “lie-detector” test his license was reinstated in no time at all. His treatment includes going to one AA meeting and one 12-step sex addict meeting per week. My guess is they need more staff at the PHP or one of the assessment centers.
I had been wondering what the motivation was behind this focus on “sex addiction” and my suspicions seem to be correct.
I have since heard of a second case of a gay doctor being forced into his state Physician Health Program (PHP) in Alabama.
Once under the control of the PHP most doctors are afraid to come forward because of the “swift and certain” consequences imposed on them. All they have to do is say the doctor was “noncompliant” to the medical board and it is over. They lose their license and there is not a thing they can do about. it. I have heard from doctors in multiple states going to law enforcement, the Attorney General, the media and the ACLU only to have the door slammed in their faces. Myself included. .
The coercion, control, ethics, and civil and human rights violations remain hidden. The crimes remain hidden. So too will this.
It appears the FSPHP is following the same pattern they have with the “impaired” and “disruptive” physicians–to discriminate. The targeting of gay, lesbian or transgender doctors for what they do in their private lives is predictable. It is an inevitable part of this well oiled slope of coercion, control, obedience and abuse.
The import of this can not be overestimated.
References:
Position Statement on Political Abuse of Psychiatry. Paper presented at: Global Initiative on Psychiatry2005.Birley JL.
Political abuse of psychiatry. Acta psychiatrica Scandinavica. Supplementum. 2000;399:13-15.






 The Elephant in the room is the state Physician Health Programs organized under the FSPHP. Nothing has changed–they have only grown more powerful and opaque and removed themselves from accountability and culpability. Moreover, they are expanding to other fields. Just ask the airline pilots. They eventually want to expand to
The Elephant in the room is the state Physician Health Programs organized under the FSPHP. Nothing has changed–they have only grown more powerful and opaque and removed themselves from accountability and culpability. Moreover, they are expanding to other fields. Just ask the airline pilots. They eventually want to expand to