Are Physician Health Programs (PHPs) above the law?
Unable to get law enforcement to take cognizance of reported abuse, many doctors I have spoken with believe that the actors involved are impervious to criminal liability. Complaints of fabrication and fraud involving PHPs and their affiliates to the police, the Attorney General and other law enforcement agencies have been given no credence, tabled or dismissed with little investigation.
Believing these agencies are deliberately ignoring credible complaints and the documentary evidence placed before them, some have concluded that state PHPs have been given the power to commit crimes with impunity and immunity.
PHPs are not above the law. It is by removing themselves from and blocking the usual routes of accountability and absolute operational control of the testing, assessment and treatment process that has enabled misconduct to remain hidden, unrecognized or excused. The crimes exist but they remain undetected, unnoticed and unpunished.
Removing Accountability
The essence of accountability is answerability which means having the obligation to answer questions regarding decisions and actions. This requires the transmission of information when it is requested. The accountable actor provides the information to the overseeing actors in a transparent manner.
Accountability also requires explanation and justification for the information provided. What was done and why? Standards, rules, regulations, codes, laws and other benchmarks are then applied by the overseeing actor to determine if the information provided was appropriate or inappropriate.
The availability and application of sanctions for illegal or inappropriate actions uncovered through answerability is also a necessary component of accountability. This is necessary to impose restraint on authority and power. Lack of enforcement of sanctions contribute to the creation of a culture of impunity.
The usual mechanisms that exist to impose restraint and create incentives for appropriate behavior and actions are absent. No outside oversight exists to limit their power or subject them to a set of rules. No regulation exists to curb abuse.
A Culture of Impunity
The authority accorded PHPs and the power they exercise exist in a culture of impunity.
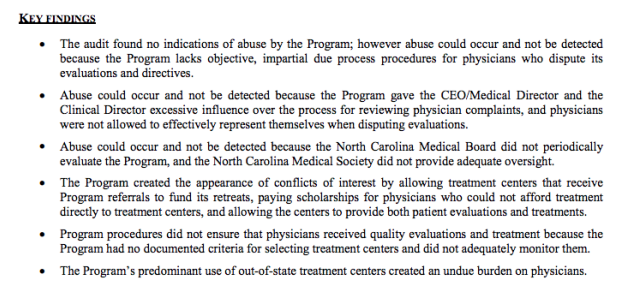
No indications of abuse were found, a point brandished by the PHP as redeeming and proving no abuse was occurring. In actual fact it is an ominous finding that also relates to their apparent ability to violate the law.
The audit found no indications of abuse but that abuse could occur and not be detected because of an absence of due process for the complainant, excessive control of the complaint process by the PHP and absence of oversight by either the medical board or medical society. What this means is that a doctor with no power is making a complaint against an unsupervised agency with enough power to influence the investigation of a complaint against itself. The reason no indications of abuse were found is because the system is specifically designed to hide abuse. That is the intent.
Absence of transparency, regulation and oversight coupled with control of information enables both censorship and doctoring of records. Strict Confidentiality is enforced by HIPAA, peer review protection, and drug and alcohol confidentiality law.
PHPs are able to suppress and conceal criminal activity but they are also able to manufacture information designed to hide misconduct.
The North Carolina Audit found no objective selection criteria for the out of state assessment and treatment centers because none exist other than ideological mindset and monetary gain. The same facilities are used by most state PHPS. They are, in fact, mandated as they are the “PHP-preferred” facilities.
In 2011 The American Society of Addiction Medicine (ASAM) issued a public policy statement on coordination between PHPs, regulatory agencies, and treatment providers. recommending only “PHP-approved” treatment centers be used and the statement specifically excludes ‘non-PHP” recognized facilities.
What the Audit diid not discover is the medical directors of all of the “PHP-approved” facilities can all be seen on this list of Like-Minded Docs.It is a rigged game Every aspect of drug-testing, assessment and treatment is kept hidden and secret and within control of the PHP.
It is a rigged game in which they have removed themselves from all aspects of accountability. They have, in effect, manufactured a culture of impunity at our expense.
Count De Monet: I have come on the most urgent of business. It is said that the people are revolting!
King Louis: You said it; they stink on ice.
Count de Monet: Gerald! Gerald: Count da Money! Count de Monet: de Monet… Monet! Say it! Monet! Gerald and Count de Monet: Moonnet, Moonnet, Moonnet Gerald, Count de Monet, Bearnaise: Mooonnnet! Count de Monet: Perfect, don’t forget! Give it to me again! Monet. Gerald and Bernaise: Monet.
Impoverished Paris Street Merchant: Rats, rats for sale. Get your rats. Good for rat stew, rat soup, rat pies, or the ever-popular ratatouille.
Other Street Merchant: Nothing, I have absolutely nothing for sale!
These ASAM “addiction experts” have become so numerous they have been able to take over almost all the state Physician Health Programs (PHPs). Their national association—the Federation of State Physician Health Programs (FSPHP)–has a stated goal of universal acceptance of the 12-step doctrine: lifelong abstinence, and spiritual recovery as the one and only treatment, as spelled out in the “PHP Blueprint.”
Very much like Straight, Inc in the 70s and 80s, they have cast a wide net with doctors to ensnare them in an endless loop of drug testing and rehab—whether the tests are fabricated or not. The doctors will enjoy no sympathy from the public, and complaining about it is deemed a sign of your “disease.” Furthermore, ASAM recommends that physicians only be referred to “PHP approved” facilities.
The medical directors of these facilities can all be found on this list of ”Like-Minded Docs.” Surprisingly, many Like-Minded Docs were former addicts and alcoholics, some even with criminal backgrounds. There are felons and even double-felons on the list.
Forget what you see Some things they just change invisibly–Elliott Smith
Physician Impairment
The Sick Physician: Impairment by Psychiatric Disorders, Including Alcoholism and Drug Dependence, published by the American Medical Association’s (AMA) Council on Mental Health in The Journal of the American Medical Association in 1973,1 recommended that physicians do a better job of helping colleagues impaired by mental illness, alcoholism or drug dependence. The AMA defined an “impaired physician” as “a physician who is unable to practice medicine with reasonable skill and safety to patients because of mental illness or excessive use or abuse of drugs, including alcohol.”
Recognition of physician impairment in the 1970s by both the medical community and the general public led to the development of “impaired physician” programs with the purpose of both helping impaired doctors and protecting the public from them.
The 1975 media coverage of the deaths of Drs. Stewart and…
In his book “Fire Lover: A True Story,” Joseph Wamnaugh profiles Fire Captain and Senior Arson Investigator for the Glendale California Fire Department John Orr. Known for his uncanny instincts in solving arson cases, Orr often astounded other investigators with his seemingly brilliant deductions in determining the causes of incendiary crime.
As it turns out, neither instinct nor brilliance played any role. Orr solved many of these cases by first-hand knowledge. He actually started many of the infernos he fought. Burning down businesses and homes for over a decade, investigators suspect Orr may have intentionally set as many as 2000 fires.
John Orr
One involved a large Pasadena hardware store that killed four people including a 3-year old toddler and his grandmother. Orr is now serving a life-sentence at Lompoc Penitentiary. Details of his arsonist acts are described in chilling detail in his own book, “Points of Origin…playing with fire.”
These cases have generally been attributed to “bad apples,” and prevention has hence been focused on identification by screening of candidates in the same manner as police departments–methods that may successfully identify and weed out criminals turned cops but not cops turned criminals.
This type of screening is unlikely to isolate those with inverted perceptions of morality for whom the normal rules do not apply. There is no test to identify individuals joining the police force “who might get so caught up in making things right or getting their guy that they would push procedural, legal or ethical boundaries.” There is no test that would have identified John Orr.
The 1991 film Backdraft illustrates this type of warped morality in portraying a firefighter turned arsonist who attempts to make a moral political statement about the dangers of reducing firefighter staffing by setting a series of explosive fires to prove the social value of firefighters. Hinds-Aldrich describes an ends-justifies-the-means occupational overzealousness in which these individuals in their efforts to do what they think is right take matters into their own hands and begin freelancing.
Occupational socialization and commitment go awry and firefighter arsonists may attempt to downplay their acts and believe the risks are manageable or even justified and necessary. They may believe they are truly providing the community a valuable service by eliminating dilapidated and crime-ridden properties-noble corruption all done for the greater good.
In a large number of cases studied by Hinds-Aldrich, at least two firefighters at the same department were involved in the fire-setting. They worked together. In Louisiana, authorities discovered that several firefighters from two rural districts were setting dozens of fires each year, mostly grassland but eventually buildings.
The majority of firefighters are individuals of integrity, good-heart and moral compass. But an estimated 100 firefighters are arrested for arson each year. Many others have avoided detection due to a confluence of factors. Hinds-Aldrich notes some have even returned to work as firefighters at a later date. Some have been let go by their department without formal investigation under the rationalization that the threat was removed. The desire to keep this behind closed-doors is understandable as the arsonist, as a firefighter, puts a stain on a noble profession. How many of these returned to their old habits is unknown. Historically no methods have been in place to detect, investigate and hold accountable those who are engaging in behavior that is the antithesis of their public responsibility and trust.
But this behavior has consequences that are sometimes grave and permanent. As Wamnaugh notes: “The damage they do in one fire can be enormous. I mean it can be a calamity, just one crime.”
Backdraft was loosely based on firefighter Ray Norton Jr who was in 1985 was convicted of conspiring with seven other “sparkies” to set 219 blazes in and around Boston during a 14-month arson spree. The group was motivated by the mistaken belief that the fires would force local governments to hire more firefighters after widespread layoffs in the 1980s. The group started with trash bins and vacant buildings but this soon escalated to burned houses, churches, factories, restaurants, a Marine Corps barracks and the Massachusetts Fire Academy. More than 300 people were injured and $22 million in property was destroyed. This illustrates the concept of so called “noble corruption” and the power of “groupthink.”
What are the motivational factors involve? Some experts previously hypothesized arsonist firefighters may have been motivated by situational factors, boredom or wanting to participate in the job they were tasked with doing –putting out fires. Others have theorized that becoming a firefighter was a direct consequence of being a firebug; a deliberate volitional choice similar to a foot fetishist becoming a shoe salesman.
This seems plausible on the surface. It makes sense in the same vein of logic as Willie Sutton’s explanation as to why he robbed banks–“that’s where the money is.” If firefighter arsonists are the product of a pyromaniacs wish fulfillment in choosing a vocation that supports and a fire fetish then screening to identify this pathology makes perfect sense. Identify and remove the threat before the damage occurs. If Florsheims wanted to extirpate all foot fetishists a screening system identifying any unusual proclivity for toes could be developed. The underlying reliability and validity of that screen, however, depends on multiple factors including the truthfulness of the potential shoe salesman. It’s much more complicated. It is a safe assumption that selling shoes does not create a fetish for feet. Some foot fetishists become shoe salesmen but I would guess few shoe salesmen become foot fetishists.
In the case of arsonist firefighters evidence suggests that it is much more complicated. Arsonist firefighters are not the simple product of a firebug choosing a vocation that provides an increased incidence of engaging in and a closer proximity to their avocation. Joining the profession does not appear to be deliberate machination to acquire an unmolested backstage pass to start fires. The personality profiles of firefighters who engage in arson seems to involve an interplay between insecurity and power. Therefore the usual screening procedures are ineffective as this type of personality predisposes these individuals to evolve into arsonists over time. It is an evolution fostered by the reinforcement of power and control. Such was the case with Orr.
According to Joseph Waughnaugh: “It’s power and control. They’ve not only created a living thing, they’ve created a living thing that is the object of massive attention.”
One of the primary motives for firefighters who commit arson was found to be the desire to be seen as a hero. Those with deep-seated insecurities and feelings of powerlessness, such as Orr, are provided with a feeling of empowerment over society. These individuals are suddenly given attention, recognition and validity they never had. Retaliation for some grievance, real or imagined, may also sometimes play a role.
“They may be the first to call in a fire, the first on the scene, and one of the most eager, excited, and enthusiastic members of the response team. Their main reason for lighting the fire is so they can appear as a hero, either by being the first to spot the flames, or by rescuing people and saving property. Extreme cases of firefighter arson involve fires set in occupied structures. When a firefighter sets fire to an occupied structure, the potential for being a life-saving hero is even greater. In North Carolina, one firefighter would set fire to an occupied house, and then return to the scene and rescue the family. His need for excitement, being worshiped, and getting attention predominated over any concern about the terrible danger to which he exposed the occupants”
Some researchers believe that firefighter arsonists undergo a mental process referred to as RPM: the arsonist rationalizes the crime, projects blame, and minimizes the consequences.
The impact of firefighter arson can be severe. People die or are seriously injured, including fellow firefighters. Homes are destroyed. An arsonist from within the fire department can disgrace the whole department, and his actions diminish public trust. Several states that have experienced the crime of firefighter arson have developed new legislation that directly impacts the prosecution of firefighters accused of arson.
The most crucial step was admitting that the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
Physician Wellness Suicides and Medical Review Officer Forensic Fraud
Multiple parallels exist between firefighter arsonists and physician wellness experts. Misuse of entrusted power occurs when those who have been given authority to carry out expected goals instead use their position and power to benefit themselves and others close to them. Abuse of power is particularly egregious when that person is doing the opposite of what he or she is supposed to do.
The firefighter who commits arson is an example of this phenomenon. So too would be a program that ostensibly promotes the health of doctors but is in reality driving them to suicide or a Medical Review Officer (MRO) ( whose sole job is to prevent the donor of a drug or alcohol test from being falsely accused of drug or alcohol use) falsely accuse a donor of drug or alcohol use by engaging in fraud.
Some of the same psychodynamics and sociocultural factors are probably involved. A disproportionate number of arsonist firefighters are volunteer firefighters (75%) who offered to help fight fires and ended up doing the opposite.. A large majority of physician wellness experts were doctors who had had their licenses revoked and were only able to practice medicine again by becoming “addiction medicine” specialists and offering to help other doctors. As a result these programs self-select for doctors who did something severe enough to lose their licenses and getting their licenses back does not necessarily mean they have changed. Many used the “salvation” card to get their licenses back. “I’ve changed.” “I want to help others.” “I’ve been redeemed.”
Designed with the dual purpose of helping sick doctors and protecting the public, many of the current state Physician Health Programs (PHPs) do neither. Paradoxically they have become reservoirs of bad medicine and institutional injustice. Part of the problem is the PHPs have removed themselves from answerability and accountability. Accountability necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable. As we have seen, much of this is by intentional design. PHPs have no oversight or outside regulation. No avenue exists to file a complaint let alone investigate one. In addition those who do file complaints are targeted for retaliation and retribution via “swift and certain consequences” that can be irreversible. Because of this, few ensnared by these programs speak out and those outside dare not speak up out of fear of being targeted themselves. This provides the necessary secrecy and silence they need in order to operate.
As with firefighter arson, few people are pointing their fingers at PHPs and claiming any problems with them. Any suggestion of misconduct or wrongdoing is inevitably ignored, delayed, blocked, rationalized or justified.
Most worrisome is the fact that outside agencies who should and could be doing something about ethical violations, procedural irregularities and even crimes are doing nothing. As a result inverted systems of morality involving procedural, ethical and criminal violations against doctors are able to not only exist but thrive.
This needs to change. Everyone in the medical profession must be and should be prepared to admit that there are ethical, procedural and legal breaches being committed by State PHPs and that precise, firm methods are needed to combat the situation. To ignore the problem or suggest that it doesn’t exist will only increase the damage caused by the impaired physician movement as well as destroy the morale of good and honest doctors. We must talk to all doctors about forensic fraud, neuropsychological fraud and physician suicide. We must investigate, charge and convict the perpetrators of these crimes. No exceptions. The most crucial step in exposing firefighter arsonist was admitting the problem exists. The most crucial step in exposing physician wellness corruption is admitting the problem exists. Although we have made some gains this has not yet happened.
Defend the Medical Review Officer (MRO)
It is now over five months and no one has been able to procedurally, ethically or legally justify the actions of Dr. Wayne Gavryck and the Massachusetts PHP, Physician Health Services, Inc. I had previously offered 100 volumes of the Classics in Medicine Library to anyone who could do so. (see prior blog below). No one has.
Therefore I am going to lower the bar and increase the prizes. If anyone can think of anything that would hypothetically justify the actions of Gavryck and PHS procedurally, ethically or legally then they win my complete collection of the Classics in Medicine Library. On top of that I will add my collection of Cocoanut Grove artifacts as seen below. Just one will do.
Cocoanut Grove Artifacts including menu, wine list, and matchbook
The Cocoanut Grove was a popular nightclub and restaurant lo located at 17 Piedmont Street in Downtown Boston. On Saturday November 28, 1942 it was the scene of a tragic and deadly fire that killed 492 people and injured many more. Fourteen hospitals received the injured and the dead: Beth Israel, Boston City, Cambridge (MT Auburn St.), Cambridge City, Carney, Chelsea Naval, Faulkner,
Massachusetts General, Massachusetts Memorial, Peter Bent Brigham, St. Elizabeth’s, St. Margaret’s, and U.S. Marine. Boston City Hospital took the majority of patients (134) and Massachusetts General Hospital took 39.
Boston City Hospital merged with the Boston University Medical Center Hospital and unfortunately the majority of its records and archives have been lost. Fortunately, we know more about the practices and techniques used at Mass General as a result their excellent archives and due to the June, 1943Annals of Surgery, which was dedicated to the Symposium on the Management of the Cocoanut Grove Burns at the MGH.
While innovations in burn treatment were a major focus, burns were not the only medical problem. Upon arrival at the hospitals, it was obvious that a large number of patients had severe respiratory distress. Some patients showed evidence of obstruction to the air passages. Non-burn specialists were quickly called to the scene to perform laryngoscopes, tracheal suction and tracheotomies. Such a large number of respiratory patients at one time enabled doctors and researchers to better understand the impact of various treatments, leading to many advances in the field.
As the Medical Review Officer (MRO) for the Massachusetts state Physician Health Program (PHP), Physician Health Services, Inc. (PHS, inc.), Dr. Wayne Gavryck’s responsibility is an important one. His job is to verify that the chain-of-custody in any and all drug and alcohol testing is intact before reporting a test as positive.
Dr. Gavryck evidently did not do that here. In fact for more than a year he helped cover up an alcohol test that was intentionally fabricated at the behest of PHS Director of Operations Linda Bresnahan (who told me when I confronted her with the fact that I have never had or ever even been suspected of having an alcohol problem “you have an Irish last name–good luck finding anyone who will believe you!”
It took a formal complaint with the College of American Pathologists to get the truth out. The whole fiasco can be seen here and here.
What Gavryck and his co-conspirators did is egregious and ethically reprehensible. It shows a complete lack of moral compass and personal integrity. What was done from collection to report to coverup and everything in-between is indefensible on all levels (procedurally, ethically, and legally).
The documentary evidence shows with clarity that this was not accident or oversight. It was intentional and purposeful misconduct. I think everyone would agree that there should be zero-tolerance for forensic fraud in positions of power. Any person of honor and civility would agree.
Transparency, regulation, and accountability are necessary for these groups. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. I’ll erase my blog and vanish into the woodwork. But If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Sanchez and Bresnahan (much like Annie Dookhan) he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths.
Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
It is people just like this who are killing physicians across the country. The body count is vast and multiple. And those who are caught doing dirty deeds such as this need to be held accountable.
Please help me get this exposed, corrected, and rectified. The doctors of Massachusetts and the doctors of this entire country deserve better than this.
Integrity and Accountability—Defend the MRO Procedurally, Ethically or Legally and win 100 Volumes of the Classics in Medicine Library and Salk and Sabin Autographs!
“The incompetent or unprincipled physician, licensed to practice medicine by a too complaisant State, is the greatest menace to scientific medicine – as great a menace as all the cultists put together.” —Dr. Morris Fishbein (The Medical Follies. New York: Boni Liverlight, 1925 p. 71)
“There is no place in science for consensus or opinion, only evidence” —Claude Bernard
Sabin, Salk and the Classics in Medicine Library
Polio is nearly a thing of the past thanks to to Dr. Jonas Salk and Albert Sabin. In 1952 Salk discovered and developed the first successful vaccine for polio and combined with Albert Sabin’s 1961 oral vaccination the duo effectively obliterated the contagious polio virus. Once a deadly threat to our country and future there were 93,000 cases of polio reported in the U.S. Between 1952 and 1953 alone. But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
full body respirator or “iron lung” needed to treat patients whose respiratory muscles became paralyzed by polio
October 23, 2014 was the centenary of Jonas Salk’s birth and in honor of his 100th birthday I am sponsoring a contest to win framed autographs of both Jonas Salk andAlbert Sabin as seen above. In addition, you will receive 100 volumes of the Classics in Medicine Library published by Gryphon Editions whose “mission is the preservation of the literary and intellectual heritage of the noble professions that we serve”
These are exact facsimiles of the original classics bound in leather and include works by William Osler, Harvey Cushing and Paul Dudley White.
Background
According to British sociologist G. V. Stimson the “impaired physician movement” is characterized by a “number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by involvement in medical society and treatment programs.” Their “authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
In this regard Dr. Wayne Gavryck, M.D. is a prototypical example.
An ex-alcoholic with a history of malpractice, Gavryck quit drinking through Alcoholics Anonymous, became “board certified” in “Addiction Medicine” and became involved with the Massachusetts PHP, Physician Health Services, Inc. (PHS) where he has been an Associate Director since 1988. He serves as their Medical Review Officer (MRO).
The “impaired physician movement” has gained tremendous sway through the American Society of Addiction Medicine and the Federation of State Physician Health Programs. The ASAM is not a valid medical specialty but a “special interest group” that represents the chronic relapsing brain disease with lifelong abstinence and 12-step recovery model of addiction and the companies that profit from it financially ( drug and alcohol testing labs, 12-step inpatient assessment and treatment centers) and politically (Drug War advocates, Anti -Medical Marijuana advocates). The impaired physician movement gained a seat at the table of power in medicine by bamboozling regulatory and administrative medicine. This illegitimate and irrational authority is in charge of almost every state PHP in the United States. ASAM physicians joined their state PHPs, gained power, and then removed those who did not agree with the groupthink and doublethink. Blind obedience and control are favored over fairness, truth and evidence-base. As with other states under the FSPHP, blindly obedient doctors are kept on while those who question the science and ethics of the groupthink are removed. The PHP-Drug Testing Laboratory and “PHP approved” assessment and treatment center industrial complex requires a Medical Review Officer of blind faith who places the goals of the FSPHP above all other considerations including the Hippocratic Oath. The system requires doctors who are willing to participate in “moral disengagement” of wrongdoing including professional, ethical and legal violations. To erect this scaffold they have put in place barriers to exposure and accountability. By declaring themselves “experts” they have used logical fallacy to temporize deflect and otherwise stifle accountability. With no oversight or regulation they are, in fact, accountable to no one. The appeal to authority and esoteric knowledge is an effective means of extinguishing valid concerns. Complacent that this is a group of benevolent organizational purpose those who should know better and could do something about it rationalize their apathy and indifference. A necessary step in exposing and addressing this problem is imposing accountability. If an organization is able to engage in conduct that is the antithesis of accepted professional guidelines and standards of care, in violation of professional and societal mores and codes-of-conduct and is illegal then there is a systemic problem. This problem can fortuitously be addressed by examining standards of care, conduct and criminal codes for breaches. If a breach is found then it needs to be explained and justified. One of the tactics of the FSPHP is to deflect criticism under the logical fallacy of appeal to authority. We are the experts. We know better. That is where it usually ends. But accountability requires both the provision of information and justification of actions. My hypothesis is that this group is committing fraud, violating ethics and flouting the law in an irrefutable manner. If this is not true then my hypothesis should be able to be refuted. It cannot. And for that reason I am putting my money where my mouth is.
Accountability
In all fairness, If Gavryck can justify his actions either procedurally, ethically or legally and back it up by any written protocol, guideline or standard then he wins and I will refrain from any more criticisms. In addition I will hand deliver to him the Salk and Sabin autographs and 100 volumes of the classics in medicine, apologize and remove this entire blog.
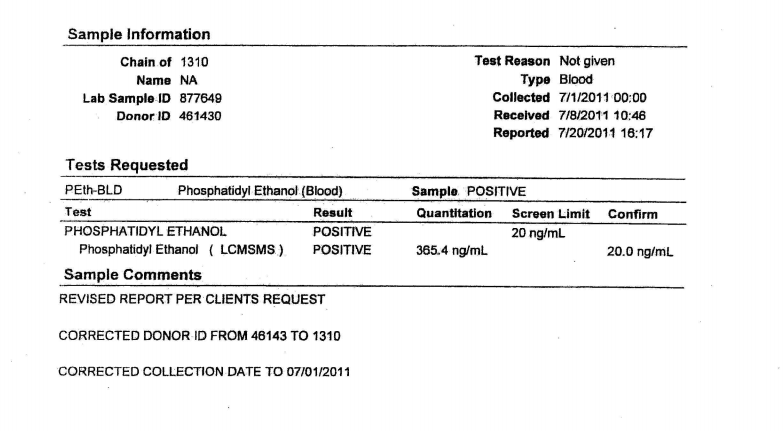
Accountability requires both the provision of information and justification of actions. One way of examining this is to look at the body professional and ethical standards and state and federal law. The FSPHP has blocked the provision of information regarding drug-testing. Although it has taken over three years I have obtained the all of the information pertaining to a July 1, 2011 test that should have immediately been rejected by the MRO. It is an invalid test.
Dr. Gavryck violated every conceivable procedural guideline and standard-of-care there is for an MRO, the Medical Review Officer Certification Council’s Codes of Ethical Conduct and both State and Federal Law. This can be ascertained by looking at the documentation. I have done this and found hundreds of documents that support the accusation that as an MRO Wayne Gavryck breached protocol, engaged in unethical behavior and broke the law. Prove me otherwise with just one credible source and the prizes are yours.
Contest Rules
Your job is to review the documentary evidence and records from PHS, Quest Diagnostics and USDTL and assess the actions and decisions made by the MRO)
If you can show that these decisions were the result of legitimate reasoning based on published guidelines or protocol, ethically defensible or did not break any laws and cite one credible source that concurs with this point of view then you have won.
If you can show that these decisions were the product of legitimate and thoughtful reasoning in accordance with established guideline, ethical codes then I will hand-deliver the items to you.
If you can justify, support or defend the actions of the Medical Review Officer (MRO):
Procedurally;
Ethically;
or Legally;
You win all of the prizes! Simple as that!
In fact, If you can support just one of these the entire lot is yours.
If you can show Dr. Gavryck did not breach any and all published Standards-of-Care andProfessional Protocols and Guidelines regarding drugs-of-abuse testing, OR that he did not violate any and all Codes of Conduct and Ethical Guidelines of the Medical Profession from Hippocrates to the American Medical Association OR that he did not violate multiple State and Federal Laws you win Salk and Sabin autographs and all of the books.
All of the documents and details regarding the forensic fraud, concealment, coverup and deliberate misrepresentation to a state agency under color of law can be seen here:
To Review: Any and all drug testing requires chain-of-custody. “Forensic” drug testing differs from “clinical”drug testing because the consequences of a falsely positive test can be grave and far reaching. Because the results of a positive test can result in the loss of rights and liberties of the person taking the test it is essential that it be done correctly. False-positive tests are unacceptable so strict chain-of-custody procedure and MRO review assure specimen integrity. This provides accountability and the custody
The custody-and-control form records chain-of-custody and is given the status of a legal document as it has the ability to invalidate a test that lacks complete information. The job of the MRO is to invalidate specimens without intact chain-of-custody.
The MRO job is fairly simple. If a lab reports a positive test for any substance the MRO must check that the signatures, dates, times and other information on the custody-and-control form are correct and per protocol. Chain-of-custody must be accurate and complete. The MRO looks for “fatal flaws” on the chain-of-custody form. If a “fatal flaw is present then the test is invalidated and the test is not reported as “positive” but “invalid.”
The sole job of the MRO is to ensure that the drug testing process and chain-of-custody procedure is followed to the letter. The MRO reviews the Custody and Control form for accuracy and completeness. The MRO also rules out any other possible explanations for a positive test (such as legitimately prescribed medications). Only then is a test reported as positive.
“the sole responsibility of the MRO is to”ensure that his or her involvement in the review and interpretation of results is consistent with the regulations and will be forensically and scientifically supportable.”
Corruption is misuse of entrusted power. It occurs when those who have been given authority to carry out expected goals instead use their position and power to benefit themselves and others close to them. Abuse of power is particularly egregious when that person is doing the opposite of what he or she is supposed to do.
Accountability is necessary to prevent corruption and necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable.
Although Gavryck may serve PHS, it is not in the capacity of a certified medical review officer; by my count the documentary evidence alone shows that he violated four of the seven Medical Review Officer Certification Council Codes of Ethical Conduct. In addition to violating the MRO Ethical Conduct he violated every other code I can think of from the Hippocratic Oath to the AMA Code of Ethics. and everything in between.
As the MRO for PHS Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody of the sample was intact before reporting a test as positive.
This is indefensible on all levels (procedurally, ethically, and legally). The documents show with clarity that this was not accident or oversight, but intentional and purposeful misconduct
There should be zero-tolerance for forensic fraud of this sort. Those of integrity and moral compass would agree. Transparency, regulation, and accountability are necessary. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Linda Bresnahan, much like Annie Dookhan, he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths. Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
Please help me get this exposed, corrected, and rectified. The physicians of Massachusetts deserve better than this.
Don’t expect a “whodunnit” version of CSI victories in this Op-ed blog article about a darker side of the forensic sciences. It is from an author with ample forensic credentials and experience from both within and outside criminal courts of the US. The article has topics ranging from the continued use of outdated or grossly over hyped “CSI” methods, ethical and moral failures in some forensic groups, to the criminal courts inability to understand much of anything about what is “real ” versus self-serving personal opinion called “science.” A measure of proof confirming these systemic problems is the article’s presenting a glimpse into the multi-million dollar costs to taxpayers for damages won by those wrongfully convicted with the help of court-qualified forensic testimony. Some optimism about better scientific scrutiny is presented but the institutional inertia resisting legitimate change in some forensic organizations, government agencies, and criminal justice institutions is still…
The Medical Profession, Moral Entrepreneurship, and Social Control
Sociologist Stanley Cohen used the term “”moral panic” to characterize the amplification of deviance by the media, the public, and agents of social control.1 Labeled as being outside the central core values of consensual society, the deviants in the designated group are perceived as posing a threat to both the values of society and society itself. Belief in the seriousness of the situation justifies intolerance and unfair treatment of the accused. The evidentiary standard is lowered.
Howard Becker describes the role of “moral entrepreneurs,” who crusade for making and enforcing rules that benefit their own interests by bringing them to the attention of the public and those in positions of power and authority under the guise of righting a society evil. 2
And according to cultural theorist Stuart Hall, the media obtain their information from the primary definers of social…
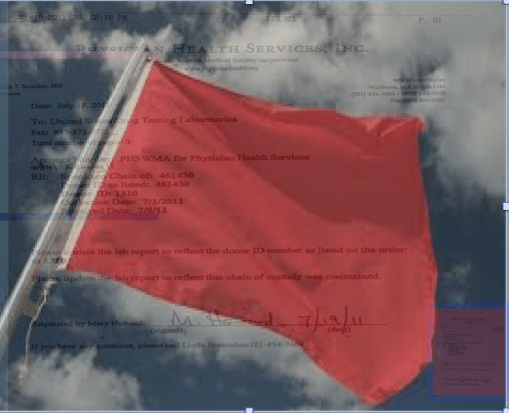
I will be putting up a survey shortly and want to hear your stories. One of the recurrent themes I keep hearing from those victimized by PHPs is falsified drug and alcohol tests. Attached is an example of what they are capable of.
Quote by Dr. Greg Skipper, MD, FASAM, FSPHP
Remember, this group has essentially removed themselves from accountability in drug and alcohol testing via the use of Laboratory Developed Tests (LDTs), a loophole which avoids FDA approval and oversight. Whereas most drug testing is transparent and held accountable, the PHPs use testing that is opaque, unregulated and accountable to no one. Accountability demands both the provision of information and justification for ones actions. PHPs block both. While most drug-testing requires the immediate provision of information if the test is questioned (as it should be), PHPs have put forth the logical fallacy that doctors have some sort of inherent expertise in toxicology and pharmacology and can “figure out” how to circumvent the testing process if they were to get copies of their lab results. They block this provision of information. And even if this information is ultimately provided, as seen below, no outside organizations exist to hold them to account. They do not have to justify their actions to anyone. No safeguards exist to assure integrity and honesty of the sample. No safeguards exist to assure the integrity and honesty of those ordering the sample either.
The documents below show forensic fraud. This is undeniable and indefensible. It does not take a toxicologist or Medical Review Officer to understand what “chain-of-custody” is and that “updating” one constitutes misconduct, fraud and (as seen here) criminal activity. These documents were obtained 5 months after a falsified test was ordered by Linda Bresnahan, Director of Operations at Physician Health Services, Inc. (PHS, inc.) the Massachusetts PHP via fax no less. The blood test was drawn on July 1, 2011. On July 19th, 2011 Ms Bresnahan requests (through the PHP secretary Mary Howard) that an already positive test for the alcohol biomarker phosphatidylethanol be “updated” with ID # 1310 and a “chain-of-custody. (which is an oxymoron-a “chain-of-custody” by definition cannot be “updated.” Unveleivably the lab does it without hesitation or any apparent compunction. The documents speak for themselves. ID # 1310 just happens to be my ID number. When I complained that no one ever accused me of ever having an alcohol problem she replied:
For a more detailed analysis see here,here and here. And where was the Medical Review Officer during all of this? Good question and one he will not answer! And no one else is holding him to account. This needs to change.
A
B
C
1. Supression of Dissent: Basic Information
2. The keys to backfire
• “Reveal: expose the injustice, challenge cover-up
• Redeem: validate the target, challenge devaluation
• Reframe: emphasize the injustice, counter reinterpretation
• Redirect: mobilize support, be wary of official channels• Resist: stand up to intimidation and bribery”
—There is no place in science for consensus or opinion, only evidence.-Claude Bernard
Dear Senator Warren,
Thank you for your reply regarding laboratory developed tests (LDTs) and the need for regulatory oversight. As you mention, LDTs are developed without FDA approval—a pathway in which is not even necessary to prove validity of a test (that it is actually testing what it claims to be testing for) to bring it to market. With no FDA oversight or regulation a commercial lab can claim any validity they want in marketing these tests. The regulation debate has focused on the reliability and validity of a number of clinical tests marketed with unverified claims of accuracy such as prenatal screening and Lyme disease and this lack of oversight is a direct threat to patient safety.
I am sure you would agree with me that the importance of tests diagnostic accuracy is directly proportional to that tests potential to cause patient harm if reported inaccurately.
Sensitivity and specificity are important components of any diagnostic test because there are consequences associated with both false-positive and false negative results.
A test falsely indicating the absence of a condition in someone who truly has it can delay or prevent needed treatment wile a test falsely indicating the presence of a condition in someone who does not truly have it can result in unnecessary testing and treatment.
Incorrect treatment and false labeling of patients can also occur. Therefore diagnostic accuracy is paramount if a test is being used as the basis for further tests and treatment. Any test being used as a basis for further tests or treatment needs to be accurate. It needs to be reliable and valid. Moreover, if the consequences of a test can result in significant patient harm (such as unneeded chemotherapy) it needs to be either 100% accurate or be combined with other tests to confirm the true diagnosis.
“Forensic” vs. “Clinical” Laboratory Testing
“Forensic” testing differs from “clinical” testing because of the consequences and the process is tightly controlled because false-positive results are unacceptable as the consequences can be grave, far-reaching and even permanent.
Forensic testing demands special handling and safeguards to protect the donor such as validated tests, certified labs, strict chain-of-custody procedures and MRO (Medical Review Officer) review. These safeguards of quality control assure the validity and integrity of the specimen. The LDT pathway was not designed for forensic tests.
A panoply of tests using urine, blood, hair, fingernails breath and saliva have been developed and brought to market since 2003 when the first one was introduced by Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, who “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.” 1
Developed as an LDT, Skipper and NMS then claimed the alcohol biomarker (which was discovered in the 1950s) “appeared to be 100 percent specific” in detecting covert use of alcohol based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male. 2 With this “evidence-base” and a not yet published paper in the pipeline,3 Skipper then pitched the test to the Federation of State Medical Boards (FSMB) as an accurate and reliable tool detect covert alcohol use in health care professionals.
Policy Entrepreneurship
In “Agendas, Alternatives, and Public Policies,”4 John W. Kingdon describes the problem, policy and political streams involved in public policy making. When these three streams come together a specific problem becomes important on the agenda, policies matching the problem get attention, and then policy change becomes possible.
Kingdon also describes “policy entrepreneurs’ who use their knowledge of the process to further their own policy ends. They ‘lie in wait… with their solutions at hand, waiting for problems to float by to which they can attach their solutions, waiting for a development in the political stream they can use to their advantage.”4
And due to a perfect confluence of streams ( Institute of Medicine report that 44,000 people die each year due to medical error,5 media reports of “impaired physicians,” the the war-on-drugs, etc.) the FSMB was swayed into accepting not just the validity but the necessity of using an alcohol biomarker of unknown reliability and validity on doctors referred to or monitored by state Physician Health Programs (PHPs) .
As the national organization that gives guidance to state medical boards through public policy development and recommendations, the individual state medical boards adopted use of the test without critical appraisal and no meaningful opposition.
Shortly after its founding in 1912, the FSMB began publishing a journal called the Quarterly of the Federation of State Boards of the United States. Now known as the Journal of Medical Regulation, the publication has archived all issues with full articles dating back to 1967 and, as the official journal of the national organization involved in medical licensing and regulation this facilitates an unskewed and impartial examination of how and when specific issues and problems were presented and who presented them and, in doing so, the “policy entrepreneurship” Kingdon describes can be seen quite clearly. For example a 1995 issue containing articles written by the program directors of PHPs in 8 different states contains an FSMB editorial acknowledging the reported 90% success rate claimed of these programs (in part attributed to the 90-day inpatient treatment programs) that concludes:
“Cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” 6
No one bothered to examine the methodology of these reports to discern the validity of the claims and it is this acceptance of faith without objective assessment that has allowed the passage of flawed public policy in medical regulation.
Nowhere is “policy entrepreneurship” more glaringly displayed as it is in a 2004 issue promoting the use of EtG in monitoring doctors as under the same cover is an article identifying both the need7 for such a test and an article providing the solution.8
“Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs,” a survey of state Physician Health Programs (PHPs) concludes that “surreptitious alcohol use” is a significant concern” for PHPs, there is no current “best method” for detection, but a promising new test with “exceptional specificity (100 percent) and sensitivity” in detecting small amounts of alcohol for up to 18 hours has recently become available.7
This same issue contains an article authored by Skipper about a new marker “not detectable unless alcohol has been consumed” recently introduced in the United States and now commercially available.”8
Notably absent from both of these articles is Skipper’s role in the commercial availability of the test. This conflict-of-interest is nowhere mentioned in this display of “creating a market then filling it.”
This “regulatory sanctification” of the test implied its tacit approval by the medical profession (i.e. “if they are using it on doctors it must be valid”) and facilitated its marketing to other monitoring agencies (nurses, airline pilots) as well as Courts and Probation Departments where those doing the monitoring had absolute power while those being monitored had no voice.
In Bending Science: How Special Interests Corrupt Public Health Research9, Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using carefully crafted distorted or “bent” science to influence legal, regulatory and public health policy. The authors describe how those making these decisions often assume the information that reaches them has been sufficiently vetted by the scientific community as it flows through a pipeline of rigorous peer-review and professional oversight and that the final product that exits the pipeline is unbiased and produced in accordance with the norms and procedures of science.
McGarity and Wagner note the serious and sometimes horrific consequences of bent science and provide examples involving Tobacco and Big Pharma . The authors call for:
“..immediate action to reduce the role that bent science plays in regulatory and judicial decision making” and the need for the scientific community to be involved in “designing and implementing reform.”
“Shedding even a little light on how advocates bend policy -relevant science could go a long way toward remedying these problems. Indeed, precisely because the advocates have overtaken the law in this area, heightened attention to the social costs of bending science could itself precipitate significant change.”
In the case of EtG this shedding of light is not very hard as no “carefully crafted” studies bending science were used to sway opinion. None existed. The only items in the pipeline were directly related to Skipper. If anyone dare to look, the Emperor has no clothes.
There are difficulties in challenging bent science including a general lack of recognition of the problem and an absence of counter-studies to oppose deliberately manufactured ends-oriented research. This has proven true with the myriad LDTs introduced into the marketplace as no counter-forces or competing economic interests producing counter-studies exist.
Multiple lawsuits, including a class-action, have been decided in favor of the labs who have taken a stand-your-ground approach supported by a body of industry-related “research” they or their affiliates produced to support the validity and reliability of the tests.
Those affected by these tests either have no power or have had their power removed. Most do not have the resources to mount a defense let alone produce counter-studies questioning the reliability and validity of the tests.
Most employee drug testing follows Department of Health and Human Services (DHHS) guidelines using FDA-approved tests that have specific cutoff levels defining a positive-result in an effort to eliminate false-positive results.10 Procedural safeguards are in place in these programs to protect the donor. Forensic testing programs using LDTs provide no such safeguards as the testing is unregulated and there is no oversight from outside actors.
Unlike clinical LDTs “forensic” LDTs are even exempt from CLIA oversight. The only avenue for complaint is through the College of American Pathologists (CAP) and, as an accrediting agency, they can only address problems by ensuring compliance with CAP guidelines. If an investigation concludes lab error or misconduct CAP can mandate the lab correct the test result and come into compliance with their guidelines under threat of loss of accreditation but no other consequences exist. Accountability has been removed yet the consequences to those harmed by these are significant and without remedy.
As is the case with the LDTs they introduced, Physician Health Programs have no oversight or regulation. A 2013 Audit of the North Carolina PHP11 prompted by complaints from doctors and performed by State Auditor Beth Woods found absolutely no oversight of the program by either the state medical board or medical society and that “abuse could occur without being detected.”
The Audit also found that doctors were predominantly referred to the same “PHP-approved” out-of-state facilities to which they in part attribute their high success rates in treatment. Interestingly the PHP could not identify what quality indicators or quantitative measurements were used by the PHP to “approve” the “PHP-approved” facilities.
As with North Carolina, the Michigan PHP will be unable to provide what quality indicators and quantitative measurements are being used to “qualify” and “approve these facilities. None exist. The sole indicators for approving these assessment centers are ideological and economic. In fact, the medical directors of most, if not all, of these facilities can be seen on this list of “like-minded docs.”
As the Michigan lawsuit notes: “Unfortunately, a once well-meaning program has turned into a highly punitive and involuntary program where health professionals are forced into extensive and unnecessary substance abuse/dependence treatment under the threat of the arbitrary application of pre-hearing deprivations.”
This has become the rule not the exception. The Federation of State Physician Health Programs (FSPHP), the same group to which Dr. Skipper belongs, has systematically taken over these programs state by state by removing competent and caring doctors not agreeing with the groupthink and silenced them under threat of litigation if they violate their confidentiality agreements and “peer review” statutes.
The same system of coercion, control and abuse exists in Massachusetts. In the past week alone I have heard from a medical student, a resident and two doctors who complained of misconduct misconduct involving fraudulent testing and falsified diagnoses.
In “Ethical and Managerial Considerations Regarding State Physician Health Programs,” published in the Journal of Addiction Medicine in 2012, Drs. John Knight, M.D. and J. Wesley Boyd, M.D., PhD who collectively have more than 20 years experience with the Massachusetts Physician Health Program (PHP) state that:
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”13
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 13
They recommend the relationship between PHP’s and the evaluation and treatment centers and licensing boards be transparent and that national standards be developed “that can be debated by all physicians, not just those who work within PHPs.”13
Accountability, or answerability, is necessary to prevent corruption. This requires both the provision of information and justification for actions. What was done and why? Accountability also requires that consequences be imposed on those who engage in misconduct.
In discussing the financial conflicts-of-interest between PHPs and “PHP-approved” assessment centers Knight and Boyd state:
“..if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.”
To “consciously tailor a diagnosis” is fraud. It is political abuse of psychiatry. And it is not only the assessment and treatment centers willing to “tailor” a diagnosis; so too are the labs involved.
Physician Suicide
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.
The Massachusetts Medical Society and Massachusetts DPH claim no oversight of the Massachusetts PHP, PHS.inc. The Massachusetts Board of Registration in Medicine (BORM) will not address ethical or even criminal complaints about the doctors involved in the PHP and there is good evidence that some members of the BORM are in fact complicit in unethical and even criminal behavior. As the Massachusetts AGO represents the BORM they defer issues back to them and dig no deeper.
One major problem is that barriers have been put in place to prevent information from getting to the right people.
The majority of people at medical societies, boards, departments of public health and other organizations are individuals of integrity and honesty but the system has been erected so that valid complaints are deflected, delayed, dismissed or otherwise tabled by sympathizers, apologists and those complicity. The criminal activity the Massachusetts PHP is engaging in is undeniable and indefensible but who is going to hold them to account?
It is going to take a while to reform this system of institutional abuse and it has to be done state by state. Please take a look at the facts and documentary evidence and help me hold them accountable. This needs to be exposed, acknowledged and addressed. Doctors are dying from this system of institutional abuse. It is a public health emergency no one is talking about. Yet those behind the PHP programs are claiming this system of coercion, abuse and control is the “gold standard” of addiction treatment and, using another loophole, they want to expand this system to mainstream healthcare.
Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcoholism, clinical and experimental research. Mar 2003;27(3):471-476.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
Kingdon JW. Agendas, alternatives, and public policies. Updated 2nd ed. Boston: Longman; 2011.
Leape LL. Institute of Medicine medical error figures are not exaggerated. JAMA : the journal of the American Medical Association. Jul 5 2000;284(1):95-97.
Schneidman B. The Philosophy of Rehabilitation for Impaired Physicians. The Federal Bulletin: The Journal of Medical Licensure and Discipline. 1995;82(3):125-127.
Jansen M, Bell LB, Sucher MA, Stoehr JD. Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs. Journal of Medical Licensure and Discipline. 2004;90(2):8-13
Skipper G, Weinmann W, Wurst F. Ethylglucuronide (EtG): A New Marker to Detect Alcohol Use in Recovering Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):14-17.
McGarity TO, Wagner WE. Bending Science: How Special Interests Corrupt Public Health Research. Cambridge, MA: Harvard University Press; 2008.
US Department of Health and Human Services. Mandatory guidelines and proposed revisions to mandatory guidelines for federal workplace drug testing programs: notices. Federal Register. April 13, 2004;69(71):19659-19660.
U.S. District Court Eastern District of Michigan, Case No: 2:15-cv-10337-AJT-RSW (2015). Carole Lucas, R.N., Tara Vialpandno, R.N., Scott Sanders, R.N., Kelly Schultz, P.A., and all other similarly situated health professionals v. Michigan Department of Licensing and Regulatory Affairs, Carole Engel, J.D.Former Director of Michigan Bureau of Health Professions, Ulliance, Inc. (State Contractor), Carolyn Batchelor (HPRP Contract Administrator), Stephen Batchelor (HPRP Contract Administrator), and Nikki Jones, LMSW. Filed January 30, 2015.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
Accountability is rooted in organizational purpose and public trust. Unfortunately, humanitarian ideals have been trampled by the imposition of corporate front groups who advance hidden agendas under guises of science and scholarship and patinas of benevolence. Rife with conflicts of interest, these groups obfuscate, mislead and exploit us to further an underlying political and corporate agenda. Healthcare and medicine has been infiltrated by various groups that pose a serious threat to both the humanitarian and evidence based aspects.
The evidence that Physician Health Services, Inc. (PHS) is committing crimes has been free-floating for the past two years. It has been posted on Reddit, Twitter, Facebook, Linkedin, blogged, faxed, and phoned. The response? Absolute silence.
The procedural, ethical and criminal violations are clear and many. The incontrovertible evidence has been directly delivered to individuals who should address this but for some reason do not. This is not a matter of opinion folks but a matter of fact. Time and time again we hear of egregious misconduct hidden for decades because of cognitive dissonance and blinkered apathy.
They are engaging in criminal activity within the walls of an institution whose foundation is the antithesis of this groups actions and it must be addressed. Either support what the documents show or do something about it.
So please sign this petition and call Massachusetts State Auditor Suzanne Bump at 617-727-6200
Institutional injustice just like that being committed by Luis Sanchez, Linda Bresnahan and the corrupt MRO Wayne Gavryck is killing doctors across the country. They need to be held accountable. Help me hold them accountable.






















 But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.