In May 1999, Dr. G. Douglas Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) down as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for malpractice, fraud, and false imprisonment. The fraud finding required that the errors in the diagnosis were intentional.
Masters was accused of improper prescribing and referred to the Florida Physician Health Program (PHP). The PHP Director, a recovering alcoholic, gave him two choices-either lose your license or be evaluated at one of our assessment centers. Believing he would have an objective evaluation that would clear him, Masters chose the latter. His assessment resulted in a diagnosis of “alcohol dependence” and he was required to enroll in the Talbott Recovery Program where he was released 4 months later and forced to sign a 5-year monitoring contract with the Florida PHP.
But Masters was not an alcoholic. According to his attorney, Eric. S. Block,
“No one ever accused him of having a problem with alcohol. Not his friends, not his wife, not his seven children, not his fellow doctors, not his employees, not his employers, No one.
The type of treatment given Dr.Masters had been previously implicated in the suicides of at least 25 doctors at one of Talbott’s facilities. Neither the exposure of these suicides nor the associated lawsuits resulted in any changes in treatment protocol. Dr. Master’s successful lawsuit didn’t either.
Changes were made; not to the treatment protocol but to the medical record. In order to prevent future malpractice suits for intentional fraud and false imprisonment they would make certain the medical records supported the diagnosis using a variety of tactics including cherry picking, suppression of specific information and deliberate avoidance of key facts, unprovable and un-disprovable statements, and a lot of illogical incomprehensible jabber all designed to make the data fit the diagnosis.
And in the year 2015 a doctor is required to be evaluated at a facility exactly like this There is no choice. They simply stacked the deck and tightened the noose.
Neuropsychological Misconduct –Making the Data fit the Diagnosis Part 1: Denial
“To further complicate matters, many evaluation/treatment centers are dependent on state PHP referrals for their financial viability. Because of this if, in its referral of a physician, the PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnoses and recommendations in a way that will support the PHP’s impression of the physician.” -John Knight and J. Wesley Boyd. in “Ethical and Managerial Considerations Regarding State Physician Health Programs,” Journal of Addiction Medicine 2012

Dr. Stephen Snook, PhD
To “consciously tailor a diagnosis” is fraud. To consciously tailor” recommendations (which would logically be an inpatient admission as I doubt the recommendations for a “problematic” physician would be send him home!) is the political abuse of psychiatry.
In 2008 I was asked to have an evaluation at Talbott by the Massachusetts PHP. Like Masters I expected a fair evaluation. The evaluation was because of a positive urinalysis for the metabolite of a medication I was taking and there were no other issues. I brought with me a letter from the manufacturer of the medication I was taking stating that it was manufactured from the substance found in my urine. In addition I had two forensic toxicology tests done (fingernail and hair) by an independent lab. My work performance and bedside manner had always been rated as superb. In my 13 years at Harvard Medical School and 10 at Massachusetts General Hospital I had never had or even been threatened with malpractice. And if you talked to any of my supervisors, coworkers, nurses, students or patients they would have nothing negative to say.
But the folks at Talbott did not contact any of my supervisors, coworkers, nurses, students or patients. They only spoke with PHS. When I arrived at Talbott for the four day evaluation almost the entire first day was spent trolling my bank accounts, credit-limit, and retirement fund to see how much I could pay for up to 3-months of inpatient treatment. They even asked me if I had anyone I could borrow up to $80,000.00 for the cash only “PHP-approved” facility. I next met with the Medical Director Dr. Paul Earley who told me my future was in his hands and I was in denial. He told me I would never practice medicine again if I did not accept treatment. I refused. Any attempts at communication or questions were met with thought stopping memes and gibberish. Simple questions were deflected with “you need a check up from the neck up” and “your best thinking got you here.” I then had a neuropsychological exam done by Dr. Stephen Snook that included the MMPI and an IQ test. At the end of the four day evaluation I met with the assessment team who told me that the neuropsychological tests revealed “denial” and “cognitive impairment,” that I could not safely practice medicine and that I needed up to three months of treatment. I looked at the evaluation which appeared to be a template for confirmatory distortion. Most of it was subjective psychobabble I could not disprove but I did notice one-big red flag I could. I had done some work with the MMPI in college. Basing my diagnosis of denial on the MMPI Dr. Snook’s interpretation was as follows:
The MMPI-2 and the MCMI-III were completed as self-report measures of psychological functioning and personality characteristics. An analysis of his response style to this inventory showed that he understood the items, but responded in a rather guarded and cautious manner. His pattern of responding is typical of an individual who may be seen as making a naïve and unsophisticated attempt to appear in a positive light. There may be a pattern of minimizing and denying even common human faults. Such a pattern of responding is not unusual in such an assessment, but may reflect a person who is not particularly insightful in terms of his won feelings and behavior. Additionally, such patterns of responding are also seen in individuals who are particularly moral or religious. Due to the level of defensiveness noted on the resulting profile, a degree of caution is warranted in interpreting these results.
The Minnesota Multi-phasic Personality Inventory
In 1942, Hathaway and Mckinley published the original Minnesota Multi-phasic Personality Inventory (MMPI). It is the most widely used psychological test in the world and has been translated into 150 languages.1. It is also the most extensively researched psychological test in history.2
Since its publication it has been revised only once and this revision is referred to as the MMPI-2.
The MMPI-2 is an objectively interpreted personality instrument with empirically validated scales. A high score on a particular clinical scale is associated with certain behavioral characteristics. These scale “meanings” are objectively applied to the test taker.
People taking the MMPI-2 are asked to give one of three responses to each of 567 items: true, false, or cannot say. The responses are scored on seven validity scales and a variety of clinical scales. The test is then scored by transforming raw scores into uniform T scores with a mean of 50 and a standard deviation of 10.
The MMPI has diagnostic value as its findings can help confirm or refute the diagnostic judgments drawn from other information obtained from the patient’s history.
The MMPI-2 is easy to score by counting item responses for each scale and recording them on a profile sheet or by using a computerized scoring program. The objective scoring procedures for the MMPI-2 assure reliability in the processing of the individual responses.
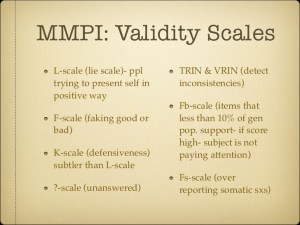
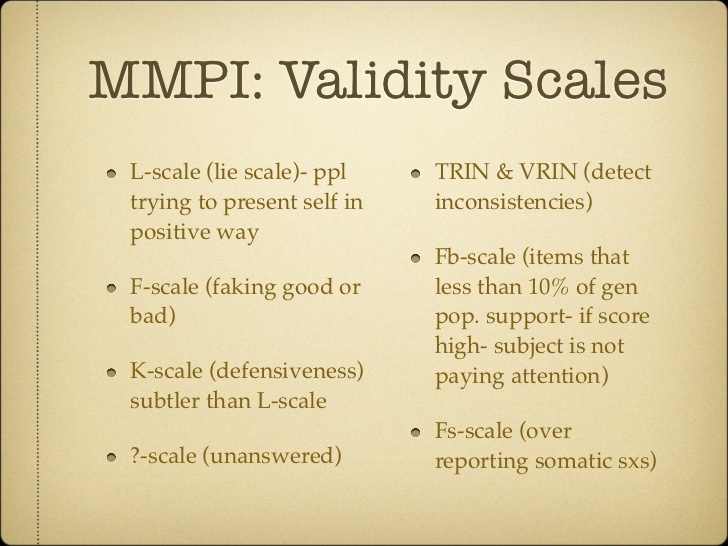
The MMPI consists of Validity Scales and Content (Basic) Scales. The creators of the MMPI were aware of the fakability of a verbal inventory and they attempted to develop several validity indicators. These are internal measures that would point to the individual who was not responding honestly.3
Although the scoring is objective, the interpretation is not. In practice clinicians generally select specific interpretations from already published possible interpretations, such as those found in an MMPI-2 handbook or a computerized report. Commercially available tests, well written manuals, and dozens of research studies facilitate but do not ensure proper and responsible test use.
According to The Handbook of Psychological Assessment,4the L (Lie Scale):
…consists of 15 items that indicate the extent to which a client is attempting to describe himself or herself in an unrealistically positive manner. Thus, high scorers describe themselves in an overly positive and idealized manner. The items consist of descriptions of relatively minor flaws to which most people are willing to admit.”
“If the clients score is considered high, it may indicate the person is describing himself or herself in an overly favorable light. This may result from conscious deception or, alternatively, from an unrealistic view of himself or herself.”
Examples of these questions include:
I do not always tell the truth
I do not like everyone I know
I would rather win than lose a game
In Psychological Assessment with the MMPI-25, it is noted that the L scale, when elevated, “reflects naïve or obvious attempts by a person to look unusually virtuous, culturally conservative, overly conscientious, and above moral reproach,” and adds that “L scale scores above a T score of 65 are unusual except in persons…or are in situations…that prompt them to present themselves in their ‘best light’.”
In Forensic Uses of Clinical Assessment Instruments,6 Archer notes that high scorers on the L-scale “present in an unusually virtuous manner and deny personal flaws that most people would be willing to admit.”
In Psychometrics :An Introduction 7 it is stated that the L-scale consists of 15 items that describe “minor flaws and weaknesses to which most people are willing to admit” and is “intended to reflect a respondent’s attempt to present an overly positive impression.”
The Psychologists’ Desk Reference8 notes indicate that individuals who score high on this scale are “presenting an overly favorable picture of themselves.”
The K scale (Correction Scale) also measures defensives and guardedness. It evaluates some of the same behavior as the L scale but much more subtly.9
The original purpose of this scale was to identify “defensiveness against psychological weakness and…a defensiveness that verges upon deliberate distortion in the direction of making a more ‘normal’ appearance.”3
To evaluate the K scale properly the specific population must be noted. In a college population a T-score on this scale between 50 and 65 is typical on the MMPI-2.9 People scoring in this range are indicating that their lives are satisfactory, that they are basically competent, and that they can manage their lives. When T = 65 or above these people are indicating “not only that they are competent people and can manage their own lives, but also that they are a bit cautious about revealing themselves. Such scores are usually obtained when a person is defensive, and/or when the test administrator does not fully explain the reason for the test.”9
Raw Scores show Dr. Snook fabricated interpretation out of whole cloth Elevated L-scale > 65 Mine = 49
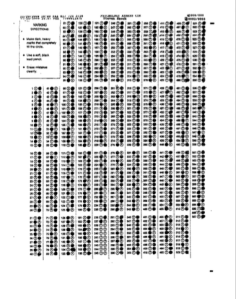
When I got back to Boston I asked MGH neuropsychologist Dr. Lauren Pollak to contact Dr. Snooks office under the guise of continuity of care. She requested that the MMPI raw data and my score sheet be sent to her. As they usually refuse to send records and labs to doctors we waited until he was out of town. The raw data confirmed what I suspected—Dr Snook made up the interpretation to make it look as if I was in denial (elevated L-scale, “reluctant to admit to even common faults”, “unsophisticated attempt to appear in positive light.” All of my validity scales were within normal limits. My L-scale T score was 49 but he wrote his assessment as if it were 65!
The scoring sheet that I filled out in March of 2008 with a #2 pencil can be seen Here. The scoring sheet showed all of my MMPI validity test T-scores within normal limits. Moreover, Dr Snook’s raw data showed that he scored the test correctly. The scoring sheet was then run independently through the MGH Neuropsychology Departments computer and showed exactly the same thing. So there was no error in scoring. An error in scoring could be understandable. People make mistakes. But this was intentional and undeniable.
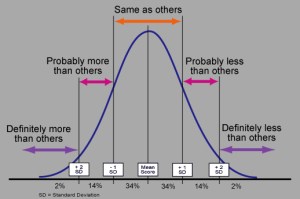
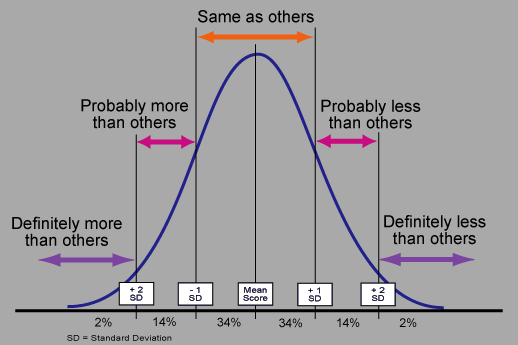
Both the original scoring sheet and his raw data show a T score of 49 on the L-scale which is normal any way you slice it. 49 is at the pinnacle of the bell shaped curve when looking at standard deviations.
This is not misinterpretation. This is not a close call. There is no controversy, ambiguity, alternative explanation, difference of opinion, or lack of clarity. MY SCORE COULD NOT BE MORE NORMAL. IT IS THE DEFINITION OF NORMAL.
There is also no defense of this as it was not a transcription error, a mathematical error, oversight, or forgetting to carry the 1 when adding. This was not a misplaced decimal or a misapplication of a fraction. There is no excuse, no rationalization, and no reason behind this.
MMPI scoring is standardized and objective. There is an MMPI manual that explains how the test is scored. It explains T-scores, standard deviations, percentiles; and what these mean and how to interpret them.
An error of quantification is understandable. An error of qualitative interpretation from quantitative data is not.
As a clinical neuropsychologist Dr Snook knows this.
Confirmatory Distortion
“Confirmatory distortion” is the process by which an evaluator, motivated by the desire to bolster a favored hypothesis, intentionally engages in selective reporting or skewed interpretations of data thereby producing a distorted picture. It is an “indisputable conscious endeavor to find and report information that is supportive of one’s favored hypothesis.10
In other words it is a conscious decision and not an unconscious bias..
I requested Talbot and Dr. Snook address the fraud and rewrite the interpretation and recommendations. I then complained to PHS not knowing at the time that they were the ones who requested it. The requests were ignored.
I then filed a complaint with the Georgia Psychological Association. They confirmed the fraud and forced Dr. Snook to correct the test. Below is his apology. An apology received only because his back was to the wall. “Profound apologies”–Give me a break. There would not be one if the Georgia Psychological Association did not force him to.
I have since spoken to a couple dozen doctors who have the same template on their evaluations. An elevated L-scale would be unusual in any doctor even if he were an alcoholic or addict. It is only the very naïve and unsophisticated who would think they can show themselves in a positive light by answering questions of obvious attempt such as “I never lie.” And if a class action lawsuit comes about this is one of the items that could be used to prove the systemic fraud. Obtain the score sheets from the facilities on anyone with this same interpretation and it will most likely show fabrication in the same manner.
Next up is the cognitive impairment piece. Just like the MMPI they manipulate the IQ tests to show cognitive impairment by shaving off points in the executive function subcategories.
Snook is one cog in this system of fraud. He and others like him should have their licenses revoked permanently. There is no excuse. How many careers have ended because of his contribution to this scam? How many have died?
As always with my posts, if he cares to contest it and can disprove the fraud I’ll take the post down. As with all the others they can’t. If they could’ve they would’ve.
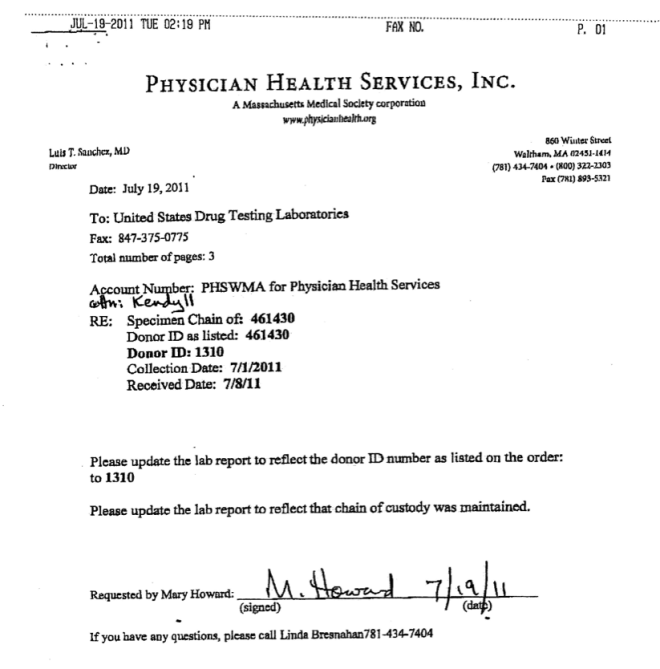
And this is the reason I was targeted by Linda Bresnahan. Upset that I got one of their own in trouble she threatened retribution. “You won’t be a doctor in five years” she said. “Dead, relapsed or in jail I don’t care.” “Dead?” I said.
“Either that or you’ll wish you were”. And when Drs. John Knight and J. Wesley Boyd were removed from PHS and were no longer there to protect me she made good on her threat. She and Luis Sanchez fabricated an alcohol test in retribution for calling out one of their own.
- Butcher JN, Williams CL. Essentials of MMPI-2 and MMPI-A Interpretation. 2nd Edition ed: University of Minnesota Press; 2000.
- Butcher JN, Rouse SV. Personality: individual differences and clinical assessment. Annu Rev Psychol. 1996;47:87-111.
- Levitt EE, Gotts EE. The clinical application of MMPI special scales. 2nd ed. Hillsdale, N.J.: L. Erlbaum Associates; 1995.
- Groth-Marnat G. Handbook of psychological assessment. 4th edition. ed. New York: J. Wiley; 2003.
- Friedman AF, Lewak R, Nichols DS, Webb JM. Psychological assessment with the MMPI-2. Mahwah, N.J: L. Erlbaum Associates; 2001.
- Archer RP. Forensic uses of clinical assessment instruments. Mahwah, N.J.: Lawrence Erlbaum Associates, Publishers; 2006.
- Furr RM, Bacharach VR. Psychometrics : an introduction. Los Angeles: Sage Publications; 2008.
- Koocher GP, Norcross JC, Hill SS. Psychologists’ desk reference. New York: Oxford University Press; 1998.
- Duckworth JC, Anderson WP. MMPI & MMPI-2 : interpretation manual for counselors and clinicians. 4th ed. Bristol, Pa.: Accelerated Development; 1995.
- Rogers R. Forensic use and abuse of psychological tests: multiscale inventories. J Psychiatr Pract. Jul 2003;9(4):316-320.
MMPI-2
GENERAL CONSIDERATIONS
Level Uniform T-Score Percentile Equivalent
Extremely High 85-90 >99.8->99.9
Very High 75-80 98->99
High 65-70 92-96
Moderately High 55-60 73-85
Average 45-50 34-55
Moderately Low 35-40 4-15
Very Low 30 <1
MMPI-2 Manual Elevation Levels:
o Very High ≥ 76
o High 66-75
o Moderate 56-65
o Modal/Average 41-55
o Low ≤ 40
3,4,5,6,9,0 = character scales; 1,2,7,8 = symptom scales
Acute: Elevated symptom scales, high F (out of ordinary distress), low K (feel
helpless in dealing with increased stress)
Chronic: Lack of elevation on symptoms scales (or 1-8 > 2-7), moderately low K
(T= 45-55), lower F (T<60)
VALIDITY SCALES
Interrelationships of Scales:
o Hi F, Lo L & K: Client is admitting to personal and emotional problems, may be
asking for help, unsure of abilities to deal w/ problems, good tx prognosis
o Hi L & K, Lo F: Client is attempting to deny problems and feelings, underreporting
of problems, attempt to present self in most positive light, most likely using primitive
defenses, problems usually chronic and therefore may be built into personality,
adequate social adjustment to see world as either good or bad
o L < F < K: Appropriate resources to deal w/ problems and not experiencing much














 Trust
Trust











 The Plan to… Require Doctors to Drug-Test all Patients
The Plan to… Require Doctors to Drug-Test all Patients