Pharmacard: A Prescription Drug Monitoring System Designed to Record Drug Histories and Reduce the Incidence of “Drug Misadventuring.”
As a medical student in 1990 I saw a 79 year old woman in the emergency room with intractable nausea and vomiting. Earlier that week she had seen her primary care physician for nausea and a mild cough. Diagnosed with bronchitis, she was given a prescription for erythromycin. Her husband brought in her medications including digoxin which can cause nausea
when blood levels are too high. A markedly high level came back on the blood draw indicating digitalis toxicity. I spoke to her primary care physician who was unaware of her digoxin prescription; completely clueless that she was prescribed the foxglove plant extract by a cardiologist for an irregular heart beat.

Digitalis was first described by William Withering in 1785 for heart conditions and this is considered the beginning of modern therapeutics. Sometime after erythromycin became available in 1952 it was discovered that taking the two drugs together increased digoxin levels. This simplest type of drug interaction is called interference and occurs when one drug either accelerates of slows down the metabolism or excretion of the other.
Based on the progression of symptoms her husband reported and the elevated levels on admission this woman undoubtedly had elevated digitalis levels when she was seen by her doctor earlier in the week. Unaware of the digitalis he inadvertently worsened her condition by giving her a medication that elevated her levels even further. She was lucky.
 The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).
The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).Digitalis toxicity in those who die outside of the hospital often goes unrecognized as most are elderly and assumed to have died from age related causes.
Seeing several more cases of drug related problems caused by ignorance of current medications and lack of communication prompted an interest in drug misadventures. I also became interested in developing a computerized up to date and accurate record accessible by all health care providers in real time , a closed loop system of “portable” information easily transferred among all health care providers be they primary doctors, pharmacists or emergency room personnel.
Research pharmacologist Dr. Edward Gallaher and I brainstormed over ideas and eventually came up with a computer program using WORM (write-once-read-many) optical technology used in compact disc systems. much like a CD-R but without the spinning disc. The credit-card sized disk could store up to two megabytes of data on an optical layer that could be written once and never changed. An optical card-reader interfaced with any IBM compatible PC. The plan was to place card readers at pharmacies, medical offices and emergency rooms. We called it Pharmacard.

Pharmacard System Developed. ASTI Connections. Vol 4. Eugene, OR: Advanced Science and Technology Institute; 1992.

Although computerized medical records existed in 1992 they were predominantly stand alone with many just replicating the paper record without word search capability. Moreover these programs did not communicate with one another so no information portability existed between the entities involved. Communication of information from pharmacy to doctors to emergency room was not an option. The system was fragmented and the search for information long.
But drug mishaps were a real problem. As with digoxin they could be fatal. Multiple reports of drug induced morbidity and mortality were found in literature searches. An obvious problem existed. . Many were drug interactions such as that with digitalis and erythromycin. From my viewpoint the need for addressing the problems caused by inadequate and and incomplete records was not only self-evident but a priority. Solutions however were few. “Brown-bag” sessions in which patients bring in a paper bag containing all of their meds were held periodically. Little booklets titled “patient medication records” were given to patients to update and record their new and current prescriptions.
 In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.An available baseline EKG was decided based on its presence making it much easier to detect a problem by looking for differences. A baseline EKG would conceivably facilitate the timing and accuracy of diagnosis. In addition it would save money because without a comparison the default is admission.
We then applied for multiple research grants for funding to do a pilot study. All were rejected and contained comments suggesting we pitch our wares to the computer people not the medical people-this is computer science not medical science.
We received very little interest at an AMA poster presentation in Washington D.C. Few people would even read the poster with most taking a quick glance and redirecting straight ahead as if they were avoiding a street-corner pollster. Those who did read it were either non-plussed, perplexed or cynical.
A research psychopharmacologist M.D.,PhD from France asked permission to give me some advice. He then told me it would not work. He said the idea was great, it would work as intended and probably help prevent drug related problems. But that did not matter because no one
gets it yet.”
gets it yet.”
Aside from a handful of people intimately involved in the research most everyone else finds this useless as do most people at the conference. This means nothing to them.
 They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.In 1999 the Institute of Medicine published To Err is Human: Building a Safer Health Care System placing patient safety high on the nation’s health care agenda. Medical errors, adverse drug reactions and interactions were deemed a big problem. Identifying ways to keep track of medications became a priority and multiple business ventures popped up and got their hats in the ring. Suddenly everyone not only recognized the problem but imparted the sense they knew it all along. Seven years had gone by and our project had then fallen by the wayside. In addition our optical platform was obsolete.
As with firefighter arson this illustrates the most crucial step in addressing a problem is admitting the problem exists. Firefighter arson had been documented for over a century but not properly addressed. The extent of the problem was not publicly recognized until a Special Report: Firefighter Arson was done by the Department of Homeland Security, the United States Fire Administration and the National Fire Data Center in 2003. The most crucial step was admitting the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
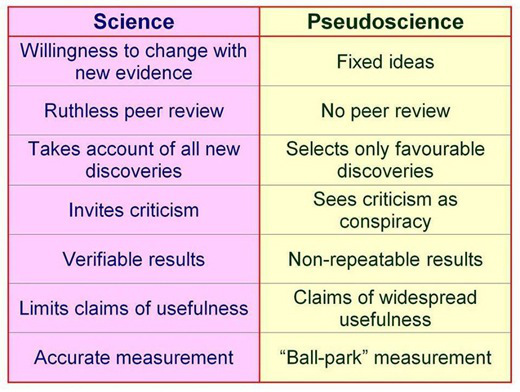
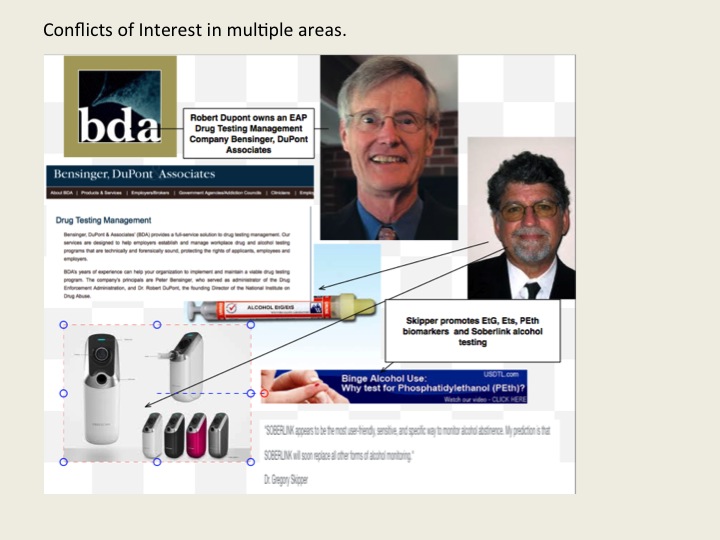
 The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.
The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.Skipper’s introduction of junk science drug and alcohol testing and use of cutoff points he pulls out of a hat and then moves upward as the problems are exposed is shameful. The fact that he unleashed this on other doctors knowing full well what would happen in a zero tolerance program needs to be revealed.
My survey is revealing many suicides as a direct result of these tests, including those of medical students and residents. And most of those who have died were not even remotely addicts or alcoholics. They were reported anonymously, given one of these tests and asked to be evaluated at a “PHP-approved” assessment center where a diagnosis was confirmed followed by 3-4 months of inpatient treatment. I am finding out most of the doctors referred to PHPs do not have any problems but the PHPs and their affiliates are giving false diagnoses, false drug testing and using threats to control them and there is little they can do about it. Skipper’s complete lack of empathy for his victims as he continues to put coins in his purse is abhorrent. Meanwhile the death count continues to rise.




 Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.
Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.