

Originally posted on Article 8:Antitrust litigation hasn’t disappeared, but rather changed its focus. Instead of targeting the great railroad empires of the late 19th century, today’s antitrust efforts focus on more minute industries, like dentistry. In October, the Supreme Court heard arguments for North Carolina State Board of Dental Examiners v. Federal Trade Commission, in which…
corruption

Medical Urban Legend–The Legacy of the 4 MDs and why B.S. Needs to be Identified from the Get-Go!

“Because I can Biotches! That’s right..because I can!”
According to G. Douglas Talbott, rehabilitation programs that evaluate and treat the rest of the population for substance abuse issues are incapable of doing so in doctors as they are unlike any other inhabitants of our society. Physicians are unique. Unique because of their incredibly high denial”, and this genetically inherent denial is part of what he calls the “four MDs.” Used to justify the thrice lengthier length of stay in physicians the “four-MDs” are as follows: “M-Deity”, “Massive Denial” “Militant Defensiveness” and “More Drugs.”
He states that “Impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.”
Now some doctors are arrogant undisciplined egotists but narcissistic personalities exist in any profession and expanding traits that may apply to a small percentage of doctors to include all doctors as a universal truth contradicts reality. Applying a stereotypical paternalistic length of treatment in doctors three times as long as non-doctors to force a “one-size” fits all treatment on them has no evidence base.
 This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.
This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.Physicians are unique only insofar as the unique elements required of the profession to become and be a physician such as going to medical school and completing the required board examinations.
Any and all doctors referred to a PHP for assessment will spend at least 3 months in treatment if the facility feels it is indicated. It is inevitable. No one has challenged a patently absurd generalization that has absolutely no evidence base or plausible scientific or medical explanation. Of course those sentenced to the 3 or more months have complained but by that time they are de-legitimized and stigmatized. No one to complain to. After all, these are just redeemed altruistic non-profit good guys protecting the public and helping colleagues forge a path to salvation!
All the ASAM/FSPHP quacks have to do at that point to deflect legitimate concerns is point out the one doing the complaining is an “addict” who is “in denial” and it is part of his “disease.” The mere accusation of substance abuse is used to disregard the claims of the accused.
Authoritative opinion entrenched. Someone should have called B.S. long ago. But no one did and if they had we would not be in the current situation which is only going to go from bad to worse as the ASAM plan for universal contingency-management and urine usury unfolds-–A “golden age.” And the 4MDs Talbott attributes to doctors are all wrong. There is only one MD and it is “medical license.” On second thought that may not be entirely true. “More money” may be another. And I am not talking about a doctor’s income. I am referring to insurance and the specter of depleting home and hearth. Fiscal annihilation. Your license or your life. And the only true and plausible answer that Talbott could give to justify the lengthy stay is “Because I can biotches!” And “contingency-management” sounds better than extortion doesn’t it? And using your medical license as “leverage” sounds a helluva lot better than holding it for ransom.

The ‘A’ Word: Are Doctors Arrogant?
Leslie Kane
June 17, 2014
Good Doctors Have Some Bad MomentsDoctors’ personalities have become a hot topic, not only because warmth and pleasantness count toward patient satisfaction, but also because positive patient interactions have a role in better outcomes.Physicians’ personalities are under the microscope as patients post reviews of doctors on numerous Websites. In some reviews, the word “arrogant” has shown up. But calling doctors arrogant is nothing new.Are there really so many arrogant doctors? No doubt, some physicians deserve the label, but it seems to be a stereotype that has blossomed and taken on its own life.”Arrogance among doctors is not the norm”, says Marion Stuart, PhD, co-author of The 15 Minute Hour: Therapeutic Talk in Primary Care, and Professor Emeritus in the Department of Family Medicine at UMDNJ-Robert Wood Johnson Medical School. “Someone who has done the hard work and has gone into medicine because they care about people, and are interested in helping peoples’ lives and making the world a better place, is not going to be arrogant.”So how did the arrogant doctor epithet arise?In the past, doctors were considered authorities who told compliant patients what to do and treated them with a paternalistic attitude. Some doctors may retain those behaviors today.Another possibility is overgeneralizing. A patient sees a doctor who has a difficult personality and assumes that the trait is more widespread within the profession than it really is.Arrogance or Self-confidence?
Leslie Kane
June 17, 2014
Good Doctors Have Some Bad MomentsDoctors’ personalities have become a hot topic, not only because warmth and pleasantness count toward patient satisfaction, but also because positive patient interactions have a role in better outcomes.Physicians’ personalities are under the microscope as patients post reviews of doctors on numerous Websites. In some reviews, the word “arrogant” has shown up. But calling doctors arrogant is nothing new.Are there really so many arrogant doctors? No doubt, some physicians deserve the label, but it seems to be a stereotype that has blossomed and taken on its own life.”Arrogance among doctors is not the norm”, says Marion Stuart, PhD, co-author of The 15 Minute Hour: Therapeutic Talk in Primary Care, and Professor Emeritus in the Department of Family Medicine at UMDNJ-Robert Wood Johnson Medical School. “Someone who has done the hard work and has gone into medicine because they care about people, and are interested in helping peoples’ lives and making the world a better place, is not going to be arrogant.”So how did the arrogant doctor epithet arise?In the past, doctors were considered authorities who told compliant patients what to do and treated them with a paternalistic attitude. Some doctors may retain those behaviors today.Another possibility is overgeneralizing. A patient sees a doctor who has a difficult personality and assumes that the trait is more widespread within the profession than it really is.Arrogance or Self-confidence?
“Arrogance is totally different from self-confidence,” says Dr. Stuart. “When you’re confident, that’s your assessment of your own competence. You have the experience and the wisdom, you know what you can do, and your confidence says that. It’s your relationship to yourself and your own expertise,” she says.
Arrogance is a different ballgame. “This has to do with your judging that other people are inferior,” she says. “It has more to do with not seeing other people as being up to your standards.”
Could the confidence that comes with being accomplished and successful make someone arrogant? Typically no, says Dr. Stuart. The trait of arrogance develops or resides within a person at a much earlier stage, arising from one of two paths:
“I am indeed better.” Someone who has always lived a privileged life, feels entitled to all of the finer things, or has always been looked up to may take it as a given that he or she is better than others. “People who had a sheltered, protected existence with no perception of what the real world is like for other people may consider themselves an elite group, entitled to feel superior,” says Dr. Stuart.
“I made it, so why can’t you?” By contrast, a person who was deprived as a child and worked very hard to pull himself up by the bootstraps may then look down on others who don’t have the same perseverance or initiative to take charge of their life and create similar success.
Doctors Are Harried and Pressured; Patients Are More Demanding
Some doctors have admitted that at times it’s hard to maintain their patience, and frustration triggers a snappish response. Throw into the mix the fact that doctors may have less time to see each patient and answer questions, and you have the ingredients for a negative interaction.
“I’ve had eight years of medical education and I’ve been trying to get my patient to make healthy lifestyle changes, and he comes in with a page ripped out of a tabloid, convinced that the information is right…there’s a limit to how much time I can spend ‘educating’ or convincing them that their ‘cure’ has no scientific basis,” one physician told me.
People have come to expect the stance of “the customer is always right” and get annoyed if doctors don’t accede to all of their requests. But because of new medical practice guidelines, a doctor may not readily give the patient the test or medication they ask for. “Now, with healthcare insurers and companies setting limits on doctors, many times the patient feels that the doctor is not so much on their side, and this could be perceived as arrogant,” says Dr. Stuart.
Is There an Outbreak of Rudeness?
Barry Silverman, MD, a cardiologist and coauthor with pediatrician Saul Adler, MD, of Your Doctors’ Manners Matter: Better Health Through Civility in the Doctor’s Office and in the Hospital, says, “While most doctors are appreciated and respected by their patients, there’s a general perception that professionalism has declined.
“Patients are often more informed, ask detailed questions, and demand a high level of service, while demands on the doctor’s time increase and reimbursements fall,” says Dr. Silverman. “What patients interpret as arrogance is many times a rushed and harried doctor, not an uncaring one. Medicine can be mentally and physically exhausting, but the bottom line is that the doctor must listen and communicate with the patient to deliver quality medical care.”
Still, remaining pleasant and calm is easier for some doctors than for others. There’s no uniform physician personality; many doctors have a natural “people person” inclination, while others are more stoic.
Are doctors expected to smile and be nice in every circumstance, no matter what?
“Professionalism is not about putting on a happy face or being someone you are not; it is about providing quality care for the patient,” says Dr. Adler. “Patients are more informed and have access to more information than ever before. Much of that information is incorrect and sometimes harmful. That means that part of the professional duty is to teach as well as treat.
“Patients understand that doctors have significant restraints on their time, and it is not unreasonable for doctors to use preprinted written materials, educational resources outside the doctor’s personal office, and honest and informative Websites,” says Dr. Adler. “However, under no circumstances should the doctor be rude or abrupt; a smile and kind, considerate behavior is always appropriate.”
It would be naive to say that there aren’t arrogant doctors. But there are far more doctors trying to do their best for patients and relate to them.
Medscape Business of Medicine © 2014 WebMD, LLC
[
Share this:

The Problems with Recognizing Problems as Problems: Medication Records, Firefighter Arsonists and Machiavellian Sociopaths
Pharmacard: A Prescription Drug Monitoring System Designed to Record Drug Histories and Reduce the Incidence of “Drug Misadventuring.”
As a medical student in 1990 I saw a 79 year old woman in the emergency room with intractable nausea and vomiting. Earlier that week she had seen her primary care physician for nausea and a mild cough. Diagnosed with bronchitis, she was given a prescription for erythromycin. Her husband brought in her medications including digoxin which can cause nausea
when blood levels are too high. A markedly high level came back on the blood draw indicating digitalis toxicity. I spoke to her primary care physician who was unaware of her digoxin prescription; completely clueless that she was prescribed the foxglove plant extract by a cardiologist for an irregular heart beat.

Digitalis was first described by William Withering in 1785 for heart conditions and this is considered the beginning of modern therapeutics. Sometime after erythromycin became available in 1952 it was discovered that taking the two drugs together increased digoxin levels. This simplest type of drug interaction is called interference and occurs when one drug either accelerates of slows down the metabolism or excretion of the other.
Based on the progression of symptoms her husband reported and the elevated levels on admission this woman undoubtedly had elevated digitalis levels when she was seen by her doctor earlier in the week. Unaware of the digitalis he inadvertently worsened her condition by giving her a medication that elevated her levels even further. She was lucky.
 The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).
The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).Digitalis toxicity in those who die outside of the hospital often goes unrecognized as most are elderly and assumed to have died from age related causes.
Seeing several more cases of drug related problems caused by ignorance of current medications and lack of communication prompted an interest in drug misadventures. I also became interested in developing a computerized up to date and accurate record accessible by all health care providers in real time , a closed loop system of “portable” information easily transferred among all health care providers be they primary doctors, pharmacists or emergency room personnel.
Research pharmacologist Dr. Edward Gallaher and I brainstormed over ideas and eventually came up with a computer program using WORM (write-once-read-many) optical technology used in compact disc systems. much like a CD-R but without the spinning disc. The credit-card sized disk could store up to two megabytes of data on an optical layer that could be written once and never changed. An optical card-reader interfaced with any IBM compatible PC. The plan was to place card readers at pharmacies, medical offices and emergency rooms. We called it Pharmacard.

Pharmacard System Developed. ASTI Connections. Vol 4. Eugene, OR: Advanced Science and Technology Institute; 1992.

Although computerized medical records existed in 1992 they were predominantly stand alone with many just replicating the paper record without word search capability. Moreover these programs did not communicate with one another so no information portability existed between the entities involved. Communication of information from pharmacy to doctors to emergency room was not an option. The system was fragmented and the search for information long.
But drug mishaps were a real problem. As with digoxin they could be fatal. Multiple reports of drug induced morbidity and mortality were found in literature searches. An obvious problem existed. . Many were drug interactions such as that with digitalis and erythromycin. From my viewpoint the need for addressing the problems caused by inadequate and and incomplete records was not only self-evident but a priority. Solutions however were few. “Brown-bag” sessions in which patients bring in a paper bag containing all of their meds were held periodically. Little booklets titled “patient medication records” were given to patients to update and record their new and current prescriptions.
 In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.An available baseline EKG was decided based on its presence making it much easier to detect a problem by looking for differences. A baseline EKG would conceivably facilitate the timing and accuracy of diagnosis. In addition it would save money because without a comparison the default is admission.
We then applied for multiple research grants for funding to do a pilot study. All were rejected and contained comments suggesting we pitch our wares to the computer people not the medical people-this is computer science not medical science.
We received very little interest at an AMA poster presentation in Washington D.C. Few people would even read the poster with most taking a quick glance and redirecting straight ahead as if they were avoiding a street-corner pollster. Those who did read it were either non-plussed, perplexed or cynical.
A research psychopharmacologist M.D.,PhD from France asked permission to give me some advice. He then told me it would not work. He said the idea was great, it would work as intended and probably help prevent drug related problems. But that did not matter because no one
gets it yet.”
gets it yet.”
Aside from a handful of people intimately involved in the research most everyone else finds this useless as do most people at the conference. This means nothing to them.
 They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.In 1999 the Institute of Medicine published To Err is Human: Building a Safer Health Care System placing patient safety high on the nation’s health care agenda. Medical errors, adverse drug reactions and interactions were deemed a big problem. Identifying ways to keep track of medications became a priority and multiple business ventures popped up and got their hats in the ring. Suddenly everyone not only recognized the problem but imparted the sense they knew it all along. Seven years had gone by and our project had then fallen by the wayside. In addition our optical platform was obsolete.
As with firefighter arson this illustrates the most crucial step in addressing a problem is admitting the problem exists. Firefighter arson had been documented for over a century but not properly addressed. The extent of the problem was not publicly recognized until a Special Report: Firefighter Arson was done by the Department of Homeland Security, the United States Fire Administration and the National Fire Data Center in 2003. The most crucial step was admitting the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
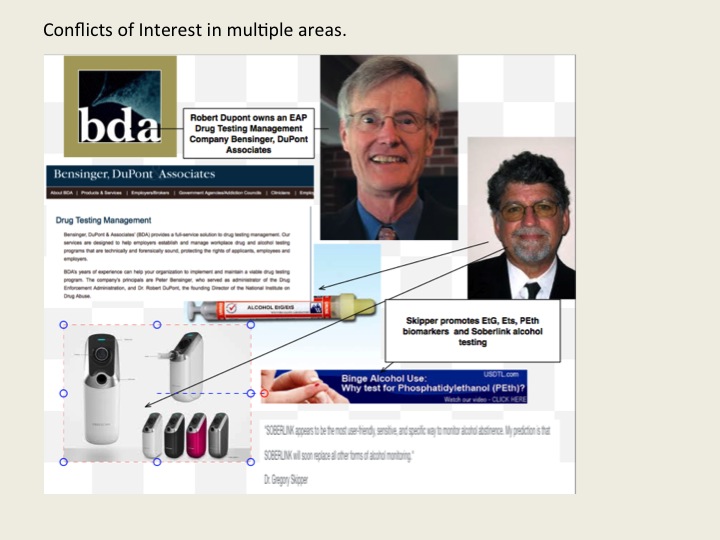
 The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.
The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.Skipper’s introduction of junk science drug and alcohol testing and use of cutoff points he pulls out of a hat and then moves upward as the problems are exposed is shameful. The fact that he unleashed this on other doctors knowing full well what would happen in a zero tolerance program needs to be revealed.
My survey is revealing many suicides as a direct result of these tests, including those of medical students and residents. And most of those who have died were not even remotely addicts or alcoholics. They were reported anonymously, given one of these tests and asked to be evaluated at a “PHP-approved” assessment center where a diagnosis was confirmed followed by 3-4 months of inpatient treatment. I am finding out most of the doctors referred to PHPs do not have any problems but the PHPs and their affiliates are giving false diagnoses, false drug testing and using threats to control them and there is little they can do about it. Skipper’s complete lack of empathy for his victims as he continues to put coins in his purse is abhorrent. Meanwhile the death count continues to rise.


Share this:

An Open Letter to Senator Elizabeth Warren Regarding Laboratory Developed Tests, Physician Health Programs and Institutional Injustice

I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.

Share this:

Press Release | Forensic Science Misconduct: A Dark and Cautionary Tale | @csidds
Press Release | Forensic Science Misconduct: A Dark and Cautionary Tale | @csidds.

Originally posted on FORENSICS in FOCUS @ CSIDDS | News and Trends:

Don’t expect a “whodunnit” version of CSI victories in this Op-ed blog article about a darker side of the forensic sciences. It is from an author with ample forensic credentials and experience from both within and outside criminal courts of the US. The article has topics ranging from the continued use of outdated or grossly over hyped “CSI” methods, ethical and moral failures in some forensic groups, to the criminal courts inability to understand much of anything about what is “real ” versus self-serving personal opinion called “science.” A measure of proof confirming these systemic problems is the article’s presenting a glimpse into the multi-million dollar costs to taxpayers for damages won by those wrongfully convicted with the help of court-qualified forensic testimony. Some optimism about better scientific scrutiny is presented but the institutional inertia resisting legitimate change in some forensic organizations, government agencies, and criminal justice institutions is still…
View original 56 more words
Share this:

Bent Science and Bad Medicine: The Medical Profession, Moral Entrepreneurship and Social Control

 The Medical Profession, Moral Entrepreneurship, and Social Control
The Medical Profession, Moral Entrepreneurship, and Social Control
Sociologist Stanley Cohen used the term “”moral panic” to characterize the amplification of deviance by the media, the public, and agents of social control.1 Labeled as being outside the central core values of consensual society, the deviants in the designated group are perceived as posing a threat to both the values of society and society itself. Belief in the seriousness of the situation justifies intolerance and unfair treatment of the accused. The evidentiary standard is lowered.
Howard Becker describes the role of “moral entrepreneurs,” who crusade for making and enforcing rules that benefit their own interests by bringing them to the attention of the public and those in positions of power and authority under the guise of righting a society evil. 2
And according to cultural theorist Stuart Hall, the media obtain their information from the primary definers of social…
View original post 2,654 more words
Share this:

Backfire Step 1: Expose the Injustice–Forensic Fraud being committed by PHPs in Collusion with Corrupt Labs

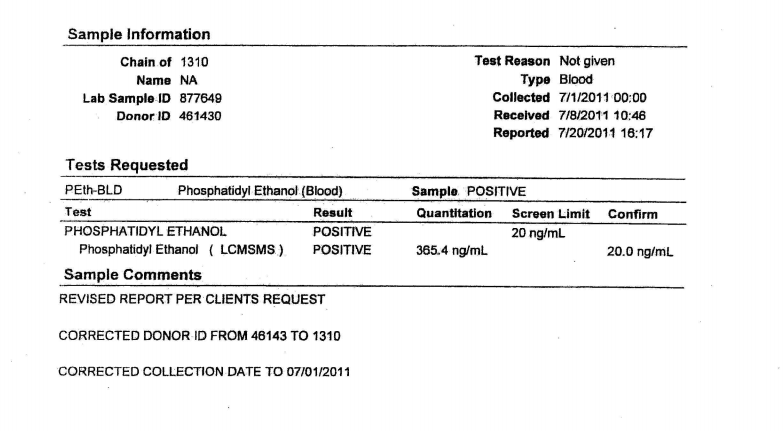
I will be putting up a survey shortly and want to hear your stories. One of the recurrent themes I keep hearing from those victimized by PHPs is falsified drug and alcohol tests. Attached is an example of what they are capable of.

Quote by Dr. Greg Skipper, MD, FASAM, FSPHP
Remember, this group has essentially removed themselves from accountability in drug and alcohol testing via the use of Laboratory Developed Tests (LDTs), a loophole which avoids FDA approval and oversight. Whereas most drug testing is transparent and held accountable, the PHPs use testing that is opaque, unregulated and accountable to no one. Accountability demands both the provision of information and justification for ones actions. PHPs block both. While most drug-testing requires the immediate provision of information if the test is questioned (as it should be), PHPs have put forth the logical fallacy that doctors have some sort of inherent expertise in toxicology and pharmacology and can “figure out” how to circumvent the testing process if they were to get copies of their lab results. They block this provision of information. And even if this information is ultimately provided, as seen below, no outside organizations exist to hold them to account. They do not have to justify their actions to anyone. No safeguards exist to assure integrity and honesty of the sample. No safeguards exist to assure the integrity and honesty of those ordering the sample either.
The documents below show forensic fraud. This is undeniable and indefensible. It does not take a toxicologist or Medical Review Officer to understand what “chain-of-custody” is and that “updating” one constitutes misconduct, fraud and (as seen here) criminal activity. These documents were obtained 5 months after a falsified test was ordered by Linda Bresnahan, Director of Operations at Physician Health Services, Inc. (PHS, inc.) the Massachusetts PHP via fax no less. The blood test was drawn on July 1, 2011. On July 19th, 2011 Ms Bresnahan requests (through the PHP secretary Mary Howard) that an already positive test for the alcohol biomarker phosphatidylethanol be “updated” with ID # 1310 and a “chain-of-custody. (which is an oxymoron-a “chain-of-custody” by definition cannot be “updated.” Unveleivably the lab does it without hesitation or any apparent compunction. The documents speak for themselves. ID # 1310 just happens to be my ID number. When I complained that no one ever accused me of ever having an alcohol problem she replied:
“You have an Irish last name-good luck finding anyone who will believe you!”
For a more detailed analysis see here, here and here. And where was the Medical Review Officer during all of this? Good question and one he will not answer! And no one else is holding him to account. This needs to change.











A

B

C




1. Supression of Dissent: Basic Information
2. The keys to backfire
• “Reveal: expose the injustice, challenge cover-up
• Redeem: validate the target, challenge devaluation
• Reframe: emphasize the injustice, counter reinterpretation
• Redirect: mobilize support, be wary of official channels• Resist: stand up to intimidation and bribery”
via Helpful resources for those abused and afraid — via www.bmartin.cc .
- Backfire Basics: http://www.bmartin.cc/pubs/bf/bfbasics.pdf
- More materials on Backfire: http://www.bmartin.cc/pubs/backfire.html
Share this:

American Doctors Are Killing Themselves and No One Is Talking About It–By Gabrielle Glaser via the Daily Beast
 Via the Daily Beast: http://www.thedailybeast.com/articles/2015/03/23/american-doctors-are-killing-themselves-and-no-one-is-talking-about-it.html
Via the Daily Beast: http://www.thedailybeast.com/articles/2015/03/23/american-doctors-are-killing-themselves-and-no-one-is-talking-about-it.html

Excerpt:
“Doctors who acknowledge problems with substances or mental health are typically referred to a physicians health program, or PHP. These organizations evaluate, monitor, and treat physicians. Established initially in the 1970s, PHPs, which exist in almost every state, were intended to divert physicians suffering from alcohol or drug problems from censure from their state medical boards. PHPs are incorporated as nonprofits and have autonomy from the boards. But some PHPs breach confidentiality if they fear a doctor is a danger to the public. And some state medical boards also fund their PHPs. Since the boards hold the keys to licensure, many say this is a conflict of interest.
There are growing concerns about whether PHPs have the right approach to the job. They typically send doctors to rehab programs rooted in the faith-and-abstinence principles of Alcoholics Anonymous. While AA’s 12 steps might work for some with alcohol-use disorders, critics say most PHP recommendations are ill suited for patients with mental health problems.
J. Wesley Boyd, a Harvard psychiatrist who left his post as assistant director of the Massachusetts PHP over a disagreement about practices there, says PHPs routinely intimidate their clients. In an article he co-wrote for the Journal of Addictions Medicine in 2012, Boyd noted that many doctors who seek or are referred by colleagues for treatment are mandated to attend pre-selected rehabilitation facilities for 60 to 90 days. Afterward, they must agree to monitoring and drug testing, typically at their own cost. When doctors resist PHP recommendations, they risk losing their livelihood and their licenses.”
For full article see: http://www.thedailybeast.com/articles/2015/03/23/american-doctors-are-killing-themselves-and-no-one-is-talking-about-it.html
Share this:

When Dentists Go Too Far: North Carolina Board of Dental Examiners v. Federal Trade Commission
The recent strike down of anticompetitive regulation in N.C. dental case opens the door to antitrust litigation against other state Regulatory Agencies such as Medical Boards.
The Federation of State Physician Health Programs has set up a “hidden” system of coercion and control using various methods (policy and moral entrepreneurship, changes in state medical practice acts and administrative procedure, misuse of health law, etc.) to create a system that lacks oversight and regulation. As a power unto themselves they are accountable to no one.
Although originally funded by medical societies and staffed by volunteer doctors in order to help sick colleagues and protect the public, any system can be subverted for profit and power, and these programs have been taken over by groups representing the multi-billion dollar drug and alcohol testing, assessment and treatment industry and become reservoirs of bad medicine and fraud. All manner of abuse can be hidden under a veil of benevolence. Although most are afraid to speak publicly under fear of punishment and retaliation (“swift and certain” consequences, summary suspension) I have herd from many many doctors in multiple states. Their stories are all the same.
In addition to misconduct related to the non-FDA laboratory developed tests (they themselves introduced into the market using a loophole that bypasses FDA approval) there are reports of coercion into unneeded evaluation and treatment at a couple dozen or so “PHP-approved” facilities under threat of loss of licensure.
Reports to a state PHP can be done anonymously with confidentiality guaranteed to the reporter. Any report will result in a meeting with the state PHP and if they feel a licensee is in need of an assessment they require it be done at a “PHP-approved” assessment center.
As non-profit tax exempt corporations, PHPs do not provide clinical assessments. They can only recommend assessments. State Regulatory Agencies (Medical Boards, Nursing Boards, etc.) have accepted the PHPs requirements of limiting assessments to those approved by the PHP. In fact many states mandate assessments to solely “PHP-approved” assessment centers under threat of summary suspension of a professional license.
An Audit of the North Carolina PHP by State Auditor Beth Woods, however, found financial conflicts-of-interest in the use of these predominantly out-of-state assessment facilities to which the N.C. PHP was referring and the state Medical Board was requiring. Woods requested the qualitative indicators and quantitative measures used to “approve” these assessment centers from the N.C. PHP but they were unable to produce any documentation showing any quality indicators or objective criteria existed! The best response they could come up with was “informal” methods and “reputation.” The full audit can be seen here.
Imagine if the FDA gave this reply if asked to provide the criteria used to “approve” medications or medical devices in the “FDA-approval” process!
Making matters even worse, the Medical Director of the N.C. PHP, Dr. Warren Pendergast was serving as President of their national organization, the FSPHP at the time of the audit.
The simple fact is no criteria exist.
A recent class action lawsuit in Eastern Michigan found this same pattern of referral to out-of-state assessment and treatment centers ( Marworth, Talbott, Hazelden. Promises,etc.)
State referrals to “PHP-approved” facilities has become a matter of public policy. Both the American Society of Addiction Medicine and the Federation of State Medical Boards have issued public policy statements stating that only “PHP-approved” centers be utilized by Regulatory Agencies in the assessment and treatment of their licensees. Moreover, these policies specifically exclude “non-PHP-approved facilities and often involve a limited time-frame. No choice, no appeal and no bartering. Do it. Do it now and if you don’t suffer the consequences.
These public policy statements can be seen in the 2011 ASAM “Public Policy Statement on Coordination between Treatment Providers, Professionals Health Programs and Regulatory Agencies” and the 2011 FSMB “updated Policy on Physician Impairment.” Many state Regulatory Agencies have strictly adhered to these policy recommendations.
What this means is that states are mandating evaluations at “PHP-approved” facilities even though there is no documentable or plausible reason for doing so. No measurable criteria exist as to how the list of “approved” facilities were “approved” yet they have “cornered the market,” removed choice and created an imposed monopoly under threat of loss of professional licensure.
In reality no official “PHP-approved” list exists. Neither does any objective published criteria for approving them. At the same time state Regulatory Agencies and Boards are forcing evaluations on licensed professionals at these couple-dozen or so facilities. They are excluding patient autonomy and choice violating the fundamental freedoms of the individual and informed consent.
All semblance of due process has been removed. If a plausible reason existed (i.e. they met some minimum standard of credentialing, quality or patient outcome) for referring to a proscribed list of assessment centers it could be arguably justified. Without such criteria, and in light of the economic and ideological conflicts of interest involved, it is patently unjustifiable.
Even more disturbing is, as Drs. John Knight and J. Wesley Boyd (who collectively have more than 20 years experience as Associate Directors at the Massachusetts PHP, PHS, Inc.) pointed out in their 2012 paper published in the Journal of the American Society of Addiction Medicine, many of these facilities are willing to “tailor” the diagnosis and recommendations of an evaluation to fit the wishes of the PHP. “Tailoring” an assessment and recommendations to anything other than what the true data show is healthcare fraud. It is, in fact, the political abuse of psychiatry.
PHPs started out as “Physicians Health Programs” but many are transitioning to “Professionals Health Programs” to widen the net. For example in Michigan and Florida the state PHP covers all health care practitioners from Acupuncturists to Veterinarians. PHPs have also entered non -healthcare employee assistance programs (EAPs) such as the aviation industry and the grand plan is expansion to non-healthcare professions. They are doing this by claiming remarkable success rates and brandishing themselves as the “gold-standard” of substance abuse treatment. Interestingly, the same individuals claiming how successful PHP programs are are the same individuals profiting from the drug and alcohol testing they introduced. Anyone with any sort of license is at risk.
So whether you cut hair, teach, take care of patients or even drive a car they could be coming after you next and they don’t have to convince you of the validity and reliability of their services–they only need to convince those who regulate your license and, as we have seen, they are very accomplished at persuasion in this department.
And that is why we need more state audits of PHPs and Medical Boards. The starting point is simple. Request from the state PHP and Board a list of “PHP-approved” facilities and the criteria by which they were approved. What should be a simple reply will undoubtedly not be as they will not be able to provide either.

Antitrust litigation hasn’t disappeared, but rather changed its focus. Instead of targeting the great railroad empires of the late 19th century, today’s antitrust efforts focus on more minute industries, like dentistry.
View original post 2,385 more words
Share this:

An Open Letter to Senator Elizabeth Warren Regarding Laboratory Developed Tests, Physician Health Programs and Institutional Injustice
—There is no place in science for consensus or opinion, only evidence.-Claude Bernard
Dear Senator Warren,
Thank you for your reply regarding laboratory developed tests (LDTs) and the need for regulatory oversight. As you mention, LDTs are developed without FDA approval—a pathway in which is not even necessary to prove validity of a test (that it is actually testing what it claims to be testing for) to bring it to market. With no FDA oversight or regulation a commercial lab can claim any validity they want in marketing these tests. The regulation debate has focused on the reliability and validity of a number of clinical tests marketed with unverified claims of accuracy such as prenatal screening and Lyme disease and this lack of oversight is a direct threat to patient safety.
I am sure you would agree with me that the importance of tests diagnostic accuracy is directly proportional to that tests potential to cause patient harm if reported inaccurately.
Sensitivity and specificity are important components of any diagnostic test because there are consequences associated with both false-positive and false negative results.
A test falsely indicating the absence of a condition in someone who truly has it can delay or prevent needed treatment wile a test falsely indicating the presence of a condition in someone who does not truly have it can result in unnecessary testing and treatment.
Incorrect treatment and false labeling of patients can also occur. Therefore diagnostic accuracy is paramount if a test is being used as the basis for further tests and treatment. Any test being used as a basis for further tests or treatment needs to be accurate. It needs to be reliable and valid. Moreover, if the consequences of a test can result in significant patient harm (such as unneeded chemotherapy) it needs to be either 100% accurate or be combined with other tests to confirm the true diagnosis.
“Forensic” vs. “Clinical” Laboratory Testing
“Forensic” testing differs from “clinical” testing because of the consequences and the process is tightly controlled because false-positive results are unacceptable as the consequences can be grave, far-reaching and even permanent.
Forensic testing demands special handling and safeguards to protect the donor such as validated tests, certified labs, strict chain-of-custody procedures and MRO (Medical Review Officer) review. These safeguards of quality control assure the validity and integrity of the specimen. The LDT pathway was not designed for forensic tests.
Forensic Laboratory Developed Tests (LDTs)
Paradoxically, laboratory developed tests with the potential to cause life-changing and possibly irreparable harm have been absent from the regulatory debate; LDT drug and alcohol tests used for “forensic” monitoring purposes.
A panoply of tests using urine, blood, hair, fingernails breath and saliva have been developed and brought to market since 2003 when the first one was introduced by Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, who “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.” 1
Developed as an LDT, Skipper and NMS then claimed the alcohol biomarker (which was discovered in the 1950s) “appeared to be 100 percent specific” in detecting covert use of alcohol based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male. 2 With this “evidence-base” and a not yet published paper in the pipeline,3 Skipper then pitched the test to the Federation of State Medical Boards (FSMB) as an accurate and reliable tool detect covert alcohol use in health care professionals.
Policy Entrepreneurship
In “Agendas, Alternatives, and Public Policies,”4 John W. Kingdon describes the problem, policy and political streams involved in public policy making. When these three streams come together a specific problem becomes important on the agenda, policies matching the problem get attention, and then policy change becomes possible.
Kingdon also describes “policy entrepreneurs’ who use their knowledge of the process to further their own policy ends. They ‘lie in wait… with their solutions at hand, waiting for problems to float by to which they can attach their solutions, waiting for a development in the political stream they can use to their advantage.”4
And due to a perfect confluence of streams ( Institute of Medicine report that 44,000 people die each year due to medical error,5 media reports of “impaired physicians,” the the war-on-drugs, etc.) the FSMB was swayed into accepting not just the validity but the necessity of using an alcohol biomarker of unknown reliability and validity on doctors referred to or monitored by state Physician Health Programs (PHPs) .
As the national organization that gives guidance to state medical boards through public policy development and recommendations, the individual state medical boards adopted use of the test without critical appraisal and no meaningful opposition.
Shortly after its founding in 1912, the FSMB began publishing a journal called the Quarterly of the Federation of State Boards of the United States. Now known as the Journal of Medical Regulation, the publication has archived all issues with full articles dating back to 1967 and, as the official journal of the national organization involved in medical licensing and regulation this facilitates an unskewed and impartial examination of how and when specific issues and problems were presented and who presented them and, in doing so, the “policy entrepreneurship” Kingdon describes can be seen quite clearly. For example a 1995 issue containing articles written by the program directors of PHPs in 8 different states contains an FSMB editorial acknowledging the reported 90% success rate claimed of these programs (in part attributed to the 90-day inpatient treatment programs) that concludes:
“Cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” 6
No one bothered to examine the methodology of these reports to discern the validity of the claims and it is this acceptance of faith without objective assessment that has allowed the passage of flawed public policy in medical regulation.
Nowhere is “policy entrepreneurship” more glaringly displayed as it is in a 2004 issue promoting the use of EtG in monitoring doctors as under the same cover is an article identifying both the need7 for such a test and an article providing the solution.8
“Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs,” a survey of state Physician Health Programs (PHPs) concludes that “surreptitious alcohol use” is a significant concern” for PHPs, there is no current “best method” for detection, but a promising new test with “exceptional specificity (100 percent) and sensitivity” in detecting small amounts of alcohol for up to 18 hours has recently become available.7
This same issue contains an article authored by Skipper about a new marker “not detectable unless alcohol has been consumed” recently introduced in the United States and now commercially available.”8
Notably absent from both of these articles is Skipper’s role in the commercial availability of the test. This conflict-of-interest is nowhere mentioned in this display of “creating a market then filling it.”
This “regulatory sanctification” of the test implied its tacit approval by the medical profession (i.e. “if they are using it on doctors it must be valid”) and facilitated its marketing to other monitoring agencies (nurses, airline pilots) as well as Courts and Probation Departments where those doing the monitoring had absolute power while those being monitored had no voice.
In Bending Science: How Special Interests Corrupt Public Health Research9, Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using carefully crafted distorted or “bent” science to influence legal, regulatory and public health policy. The authors describe how those making these decisions often assume the information that reaches them has been sufficiently vetted by the scientific community as it flows through a pipeline of rigorous peer-review and professional oversight and that the final product that exits the pipeline is unbiased and produced in accordance with the norms and procedures of science.
McGarity and Wagner note the serious and sometimes horrific consequences of bent science and provide examples involving Tobacco and Big Pharma . The authors call for:
“..immediate action to reduce the role that bent science plays in regulatory and judicial decision making” and the need for the scientific community to be involved in “designing and implementing reform.”
“Shedding even a little light on how advocates bend policy -relevant science could go a long way toward remedying these problems. Indeed, precisely because the advocates have overtaken the law in this area, heightened attention to the social costs of bending science could itself precipitate significant change.”
In the case of EtG this shedding of light is not very hard as no “carefully crafted” studies bending science were used to sway opinion. None existed. The only items in the pipeline were directly related to Skipper. If anyone dare to look, the Emperor has no clothes.
Lack of Answerability and Accountability
There are difficulties in challenging bent science including a general lack of recognition of the problem and an absence of counter-studies to oppose deliberately manufactured ends-oriented research. This has proven true with the myriad LDTs introduced into the marketplace as no counter-forces or competing economic interests producing counter-studies exist.
Multiple lawsuits, including a class-action, have been decided in favor of the labs who have taken a stand-your-ground approach supported by a body of industry-related “research” they or their affiliates produced to support the validity and reliability of the tests.
Those affected by these tests either have no power or have had their power removed. Most do not have the resources to mount a defense let alone produce counter-studies questioning the reliability and validity of the tests.
Most employee drug testing follows Department of Health and Human Services (DHHS) guidelines using FDA-approved tests that have specific cutoff levels defining a positive-result in an effort to eliminate false-positive results.10 Procedural safeguards are in place in these programs to protect the donor. Forensic testing programs using LDTs provide no such safeguards as the testing is unregulated and there is no oversight from outside actors.
Unlike clinical LDTs “forensic” LDTs are even exempt from CLIA oversight. The only avenue for complaint is through the College of American Pathologists (CAP) and, as an accrediting agency, they can only address problems by ensuring compliance with CAP guidelines. If an investigation concludes lab error or misconduct CAP can mandate the lab correct the test result and come into compliance with their guidelines under threat of loss of accreditation but no other consequences exist. Accountability has been removed yet the consequences to those harmed by these are significant and without remedy.
State Physician Health Programs
As is the case with the LDTs they introduced, Physician Health Programs have no oversight or regulation. A 2013 Audit of the North Carolina PHP 11 prompted by complaints from doctors and performed by State Auditor Beth Woods found absolutely no oversight of the program by either the state medical board or medical society and that “abuse could occur without being detected.”
The Audit also found that doctors were predominantly referred to the same “PHP-approved” out-of-state facilities to which they in part attribute their high success rates in treatment. Interestingly the PHP could not identify what quality indicators or quantitative measurements were used by the PHP to “approve” the “PHP-approved” facilities.
In January of 2015 a Federal class action lawsuit was filed in the Eastern District of Michigan against the state PHP program and found health care providers were subject to the same referral system using these out-of-state facilities. The suit alleges constitutional violations related to the forced medical treatment of health care professionals and the “callous and reckless termination of professional licenses without due process.” 12
As with North Carolina, the Michigan PHP will be unable to provide what quality indicators and quantitative measurements are being used to “qualify” and “approve these facilities. None exist. The sole indicators for approving these assessment centers are ideological and economic. In fact, the medical directors of most, if not all, of these facilities can be seen on this list of “like-minded docs.”
You once said “People feel like the system is rigged against them. And here’s the painful part: they’re right. The system is rigged.”
As the Michigan lawsuit notes: “Unfortunately, a once well-meaning program has turned into a highly punitive and involuntary program where health professionals are forced into extensive and unnecessary substance abuse/dependence treatment under the threat of the arbitrary application of pre-hearing deprivations.”
This has become the rule not the exception. The Federation of State Physician Health Programs (FSPHP), the same group to which Dr. Skipper belongs, has systematically taken over these programs state by state by removing competent and caring doctors not agreeing with the groupthink and silenced them under threat of litigation if they violate their confidentiality agreements and “peer review” statutes.
The same system of coercion, control and abuse exists in Massachusetts. In the past week alone I have heard from a medical student, a resident and two doctors who complained of misconduct misconduct involving fraudulent testing and falsified diagnoses.
In “Ethical and Managerial Considerations Regarding State Physician Health Programs,” published in the Journal of Addiction Medicine in 2012, Drs. John Knight, M.D. and J. Wesley Boyd, M.D., PhD who collectively have more than 20 years experience with the Massachusetts Physician Health Program (PHP) state that:
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”13
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 13
They recommend the relationship between PHP’s and the evaluation and treatment centers and licensing boards be transparent and that national standards be developed “that can be debated by all physicians, not just those who work within PHPs.”13
Accountability, or answerability, is necessary to prevent corruption. This requires both the provision of information and justification for actions. What was done and why? Accountability also requires that consequences be imposed on those who engage in misconduct.
In discussing the financial conflicts-of-interest between PHPs and “PHP-approved” assessment centers Knight and Boyd state:
“..if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.”
To “consciously tailor a diagnosis” is fraud. It is political abuse of psychiatry. And it is not only the assessment and treatment centers willing to “tailor” a diagnosis; so too are the labs involved.
Physician Suicide
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.
The Massachusetts Medical Society and Massachusetts DPH claim no oversight of the Massachusetts PHP, PHS.inc. The Massachusetts Board of Registration in Medicine (BORM) will not address ethical or even criminal complaints about the doctors involved in the PHP and there is good evidence that some members of the BORM are in fact complicit in unethical and even criminal behavior. As the Massachusetts AGO represents the BORM they defer issues back to them and dig no deeper.
Drs. Knight and Boyd have suggested State Audits and we are hoping that MA State Auditor Suzanne Bump will investigate the MA PHP and the Board of Registration in Medicine’s Physician Health and Compliance Unit shortly.
One major problem is that barriers have been put in place to prevent information from getting to the right people.
The majority of people at medical societies, boards, departments of public health and other organizations are individuals of integrity and honesty but the system has been erected so that valid complaints are deflected, delayed, dismissed or otherwise tabled by sympathizers, apologists and those complicity. The criminal activity the Massachusetts PHP is engaging in is undeniable and indefensible but who is going to hold them to account?
It is going to take a while to reform this system of institutional abuse and it has to be done state by state. Please take a look at the facts and documentary evidence and help me hold them accountable. This needs to be exposed, acknowledged and addressed. Doctors are dying from this system of institutional abuse. It is a public health emergency no one is talking about. Yet those behind the PHP programs are claiming this system of coercion, abuse and control is the “gold standard” of addiction treatment and, using another loophole, they want to expand this system to mainstream healthcare.
Sincerely,
Michael L. Langan, M.D.
- Skipper G. Exploring the Reliability, Frequency, and Methods of Drug Testing: What is Enough to Ensure Compliance?: Alcohol Markers and Devices. 2013; http://www.fsphp.org/Skipper, Exploring the Reliability Frequency and Methods 2 Presentation.pdf.
- Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcoholism, clinical and experimental research. Mar 2003;27(3):471-476.
- Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
- Kingdon JW. Agendas, alternatives, and public policies. Updated 2nd ed. Boston: Longman; 2011.
- Leape LL. Institute of Medicine medical error figures are not exaggerated. JAMA : the journal of the American Medical Association. Jul 5 2000;284(1):95-97.
- Schneidman B. The Philosophy of Rehabilitation for Impaired Physicians. The Federal Bulletin: The Journal of Medical Licensure and Discipline. 1995;82(3):125-127.
- Jansen M, Bell LB, Sucher MA, Stoehr JD. Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs. Journal of Medical Licensure and Discipline. 2004;90(2):8-13
- Skipper G, Weinmann W, Wurst F. Ethylglucuronide (EtG): A New Marker to Detect Alcohol Use in Recovering Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):14-17.
- McGarity TO, Wagner WE. Bending Science: How Special Interests Corrupt Public Health Research. Cambridge, MA: Harvard University Press; 2008.
- US Department of Health and Human Services. Mandatory guidelines and proposed revisions to mandatory guidelines for federal workplace drug testing programs: notices. Federal Register. April 13, 2004;69(71):19659-19660.
- Wood B. State of North Carolina Performance Audit North Carolina Physicians Health Program. . http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf. Accessed March 17, 2015.
- U.S. District Court Eastern District of Michigan, Case No: 2:15-cv-10337-AJT-RSW (2015). Carole Lucas, R.N., Tara Vialpandno, R.N., Scott Sanders, R.N., Kelly Schultz, P.A., and all other similarly situated health professionals v. Michigan Department of Licensing and Regulatory Affairs, Carole Engel, J.D.Former Director of Michigan Bureau of Health Professions, Ulliance, Inc. (State Contractor), Carolyn Batchelor (HPRP Contract Administrator), Stephen Batchelor (HPRP Contract Administrator), and Nikki Jones, LMSW. Filed January 30, 2015.
- Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.




