Please donate to this effort below. Your contribution can and will make a difference. https://www.gofundme.com/PHPReform



Please donate to this effort below. Your contribution can and will make a difference. https://www.gofundme.com/PHPReform

Below images link to podcast.



Physician Health Programs (PHPs) now targeting medical students–More sheep for the slaughter
The attached article entitled “Medical school drug testing is a moral and scientific failure” opposes testing medical students for drugs and alcohol but things are going to get a whole lot worse.
In the past six-months I have been contacted by an increasing number of medical students searching for help after being trapped in quagmire of their state physician health program (PHP). Each of them had either been referred to a “PHP-approved” assessment center or had already had an evaluation recommending inpatient treatment.
Some of these students were subjected to non-FDA approved laboratory developed tests including hair testing for marijuana metabolites and the alcohol biomarker EtG. These typeof tests can detect substances that were used days, weeks and even months prior to testing.
Medical students and physicians are just as likely to have experimented with illicit substances in their lifetimes as their age and gender matched peers.1
Although medical students as a group drink slightly more alcohol than the general population, the pattern and prevalence of alcohol, dependence is consistent with their age mates in the general population.1 2
Like it or not recreational and experimental drug use is widespread in young adults and most of them “grow out of it” and the 21st Amendment repealed the Volstead Act in 1933. Alcohol is legal and those that can handle it have a right to a round of beers after a long day or imbibe a cocktail with a dinner date. But according to the prohibitionist profiteers and moral preeners any drug or alcohol use is a sign of “potentially impairing illness” that must be addressed and treated early to prevent an inexorable slide into a chronic relapsing brain disease and abstinence and lifelong adherence to the principles 12-step spirituality are the only way to do so.
An old joke asks “How does a doctor define an alcoholic?” Answer–“anybody who drinks more than he does.” How does a PHP define an alcoholic? Answer –anybody who walks through the front door.
In reality, a zero-tolerance paradigm utilizing this type of testing would be ruinous. With recreational and experimental drug use common in young adults a profession that refuses to accept anyone who tests positive for drugs will exclude large numbers of brilliant, talented individuals. Dismissing highly talented people in medicine for what might be a one-off recreational non problematic drug experience would retard its advance.
The use of these non-FDA approved tests of unknown validity should not be allowed to begin with but there needs to be a concerted direct attack on their use on medical students or the brain-drain on the profession will bring it back to the dark ages. The ASAM White Paper on Drug Testing proposes imposing this system with mandatory drug testing by the healthcare system from childhood to old age. College loans are proposed as “leverage” for college students in this “contingency management” paradigm so a lot of promising students could be weeded out before even applying to medical school. Forget GPA and MCATS as the primary criteria for medical school admission will be sobriety and clean urine screens..
Diagnosing disease without meeting the diagnostic criteria for that disease.
None of the students who contacted me seemed to fit the diagnostic criteria for the diagnosis given to them stories which were articulate, detailed and sincere. All cases involved either a naive mistake or isolated incident.
One student made the disastrous revelation to a PHP director who had just given a class lecture that she had smoked marijuana with her high school friends in her home state of Colorado. She was then called in by the PHP and referred for an evaluation at an out of state facility where she was diagnosed with “marijuana dependence” based on a positive low level THC metabolite on a hair follicle test. She was told she was in denial and inpatient treatment was recommended. Although she admitted to occasional weekend marijuana use there were absolutely no problems in any realm of her life. It is self-evident that impairment due to drugs or alcohol impacting someones capacity to work or function needs to be addressed but the penalty imposed on her for her private behavior was to end her career in medicine before it even started. The medical school administration mandated she either complete the treatment required by the PHP or she would not be able to enroll the following semester and not being able to come up with the up-front out-of-pocket cost for treatment she was not able to return to the medical school and has decided to pursue a different career.
Another student was anonymously reported to the PHP for smoking marijuana at a weekend party which resulted in a similar assessment and recommendation for inpatient treatment. After spending 3 months at a facility in Alabama he is now under monitoring contract with his PHP but returned to school.
Healthy student asks for help in his organizational skills–ends up with a psychiatric and substance abuse diagnosis
After reading an advertisement in the state medical society newsletter promoting work-life balance a second-year medical student contacted his state PHP to obtain advice on his problem with “procrastination.” Classes and working part time in the endocrinology lab left him with little time and he found himself slacking off on his exercise routine and burning the midnight oil before test nights. He told the PHP director about his history of depression after his father died immediately before his freshman year at college. That October he became overwhelmed with sadness and missed his dad and hometown. He sought help from the campus physician who prescribed prozac which was discontinued in a years time without return of any symptoms.
Realizing there were no classes in work-life balance but only a support group for “burnout” the student declined the PHP directors offer of an assessment of his “mental health.” Much to his surprise he was called in the following week by a medical school administrator and told that the PHP was requiring an assessment at one of two out of state “PHP-approved” assessment centers in Lawrence Kansas. He was at first confused at the nonsense he was hearing and then became indignant at the nonsensical and illogical request without rhyme or reason and the betrayal of trust and ethics. “Surely this must be a HIPPA violation.” He obtained an outside consultation from a psychiatrist and contacted the campus physician who confirmed his diagnosis was acute situational depression and bereavement but the PHP disregarded the information. He bartered for a local evaluation but this was refused. He arranged for the 96-hour assessment in Kansas. His mother paid the requisite out-of-pocket up-front $4,500.00 to the facility and she told him not to worry as his life would get back to normal after they confirmed he had no psychological problems. “Dysthymia, Major depressive disorder, severe, in remission and alcohol use disorder” were given as diagnoses. “Alcohol use disorder” was based on a hair test for EtG which was the result of his drinking an occasional beer or two with friends after school and on the weekends. He was told he may be “self-medicating” and playing “Russian roulette” given his history of depression. Recommendations included inpatient treatment followed by a “structured aftercare program” of abstinence and monitoring by for alcohol and drugs of abuse. Forced to sign a contract with the PHP he was understandably upset at the serious and unfounded sequelae that was the result of asking for help.
Another fourth-year student got into a bit of a shoving match with his buddy at the bar on a Saturday night and was reported to his PHP anonymously. He is awaiting evaluation.
This brings up another potential problem–sham peer review. As PHPs accept anonymous referrals what is in place to prevent inappropriate referrals based on removing a competitor and improving your academic standing.
A legitimately prescribed stimulant for ADHD bought a third year student into a PHP contract. He was forced to discontinue the medication prescribed by a psychiatrist specializing in childhood ADHD by a family practitioner in “recovery” from abusing intravenous fentanyl who had been monitored by the PHP himself for ten years then became medical director after getting board certified as an addiction medicine specialist.
This student got 99th percentile across the Board on his MCATs and may one day cure cancer but now faces an uncertain future as he recently got a positive EtG on a urine test and they are currently “sorting this out.”
The most bizarre story was from a student who sought help for sleep troubles after reading about the PHP as a referral source. He subsequently saw a sleep-specialist and was diagnosed with an oversized uvula which was surgically corrected. His sleep troubles improved but his troubles with the PHP remained. A triathlete and excellent student the PHP determined he had a “thought disorder” and discussions of “schizophrenia” were entertained by the PHP and they recommended an out of state evaluation at one of the three gulags used by the FSPHP for “disruptive physician” and behavioral exams–Vanderbilt, Acumen and the Professional Renewal Center. All of these facilities come with a guaranteed diagnosis. Polygraphs and unvalidated neuropsychological instruments designed to detect “character defects” cast a pretty wide net.
Question FSPHP with direct questions to undermine a “culture of professionalism.
It is important that medical school administrators refuse to engage in blind deference to the authority of the state PHP. Authority must always be questioned and to not do so is irresponsible. Unquestioning allegiance to an authority does not comport with the history of the medical profession or science. Faith in institutions demands mass adherence to faith in that authority and direct challenges to the status quo are needed to undermine that faith. They have bamboozled the medical boards into implementing bad policy, approving bad science and making bad decisions. They have duped state legal authorities into deference to their expertise and integrity under the notion that questioning these attributes undermines a culture of professionalism. Fact of the matter is they have no expertise, no integrity and no professionalism.
PHPs have been contaminated with an outside influence and support an agenda that has nothing to do with protecting the public or helping medical students. They are an illegitimate authority that has become an irrational authority and their recommendations mandate direct answers and justification.
If the PHP has concerns about a student then the first step should be to obtain an independent second opinion. PHPs discourage second these second opinions and disregard all outside expert opinion no matter how well qualified and experienced that expert is. Anyone outside this brood of addiction addicts is scoffed at as biased or unenlightened to the simplistic belief system with which they have contaminated the medical profession. Look into the assessment centers to which they are mandating referral. Ask what qualitative factors and quantitative measurements were used to approve that facility and why no one in Massachusetts has the ability come to a competent diagnosis. The yarn that doctors and medical student have an ability to dissemble and appear normal while harboring a “potentially impairing condition” is one of the medical urban legends they started. Ask to see the evidence base. There is none and it defies common sense, logic and science.
An increasingly bright light is being shed towards the malfunctions and corrupt practices of this unaccountable confederacy of “authorities” and at some point soon their jig will inevitably be up. In the interim, if you are referred to a PHP it would be a good idea obtain independent lab tests and two second opinions. Although the PHP will disregard this documentation it would be wise to obtain it to prove both your normality and the discrepancy between your independent evaluation results and the cherry-picked pulled out of a hat multiple diagnoses confabulated and misrepresented by the PHP.

Medical school drug testing is a moral and scientific failure
ANONYMOUS | EDUCATION | MAY 11, 2014
Before the 1980s, drug testing was uncommon. It was widely viewed as an invasion of privacy and an infringement on fourth amendment rights. Today, a medical student is likely to be drug tested before entering medical school, before clinical rotations, and/or before residency. If preventing drug use among medical students is the goal of these tests, they have failed miserably. Urinalysis drug tests are ineffective. But more importantly, they are immoral.
Drug tests are ineffective for two reasons. First, they basically just test for marijuana. A 10 panel urinalysis technically tests for 10 different drugs, but marijuana is one of the only drugs that can be detected for more than 30 days. Cocaine can be detected for 4 days. Amphetamine, methamphetamine, ecstasy, heroin, and codeine all can be detected in urine for only 2 days. This means that a user of drugs far more dangerous than marijuana needs to abstain for just a couple of days. Psilocybin mushrooms, as well as several other mind-altering drugs, are not tested for at all.
For a marijuana user, a drug test might seem like a nightmare. But here we arrive at the second reason why drug tests are ineffective, they are easily beaten. A marijuana user may choose to drink a lot of water before his drug test to dilute his urine. Alternatively, he may choose to use a friend’s urine who he knows does not use marijuana. Either one of these options might work. But fortunately for such a marijuana user, there is another option that is essentially risk free, synthetic urine. There are several companies that make synthetic urine capable of beating drug tests. The word on the Internet is that Quick Fix is a safe bet. I personally know some people who would agree. At just $30 for a bottle, it looks like the drug test is no match for the free market.
Do not just take my word for it though. In 2003, the University of Michigan conducted a study on the effectiveness of drug testing students. From nearly 900 schools, the study found that drug testing, whether routine, random, or based on suspicion, had no measurable effect on drug use among students. Put simply, drug testing accomplishes nothing.
The most important concern I have about drug testing medical students is a moral one. Regardless of their effectiveness, or ineffectiveness, the endgame of drug testing is to prevent drug users from becoming doctors. Users, not addicts; and there is a big difference. A marijuana user might use on weekends or at night to relax, much like an alcohol user. A marijuana addict, although rare, is the type of person who might show up to important occasions intoxicated. The statistics on marijuana addiction vary. They usually show that less than 10% of users become addicts, but they always show that alcohol users have higher rates of addiction. A urinalysis detects alcohol for no more than 12 hours after use. This means that medical students who use alcohol are more likely to be addicted, and they face basically no risk of failing a drug test.
Should we be worried about medical students being drunk in clinical settings? Of course. And we should also be worried about medical students being high in clinical settings. Intoxication could be disastrous and it needs to be prevented. The good news is that this is done naturally. It is highly unlikely to find medical students who are addicts of marijuana, alcohol, or any mind-altering drug. I believe it is safe to say that the rigor of medical school itself prevents drug addicts from becoming doctors. There are, however, drug users who will make it into medical school or other rigorous scientific careers. Actually, many of them thrive. Richard Feynman, Kary Mullis, and Francis Crick used marijuana and LSD, Carl Sagan used marijuana, and Oliver Sacks used several illicit drugs. When drug tests are required for every medical student, the casual drug user, no matter how much potential he has, is bullied for no reason. The potentially dangerous drug addict has already been weeded out long ago.
Medical school is supposed to be based on science. The science shows that drug testing does not work. If it did work, then many great scientists would have been removed from their professions. These facts alone should be enough to settle the issue, but it is important to look at two more moral objections we should all have.
First, drug tests are not free. Before entering medical school, I paid about $30 for one. This does not sound like much. But charging students even one penny is unacceptable, for there is not even a fraction of a penny in benefit from these tests. The nearest drug testing facility for me was a 20 minute drive from my house. I could have driven anywhere for 20 minutes and just handed $30 to any random person. Surely, that $30 would bring more value to society than $30 wasted on a drug test. Imagine if a police officer searched a person’s car for drugs against his will, found none, and then charged this person $30. That is the reality of drug testing.
Second, drug tests are an invasion of privacy. Medical students should not be forced to prove their innocence. This creates a guilty until proven innocent environment. It immediately creates resentment among students, and rightfully so. Furthermore, what about people with paruresis? The International Paruresis Association estimates that 7% of people suffer from this condition, also known as shy bladder. Type “paruresis drug test” into a search engine and spend some time reading through the horror stories that are shared. These people suffer from a medical condition, and of all places, their medical school is completely inconsiderate.
Drug testing is a moral and scientific failure. Medical schools should be too embarrassed to take part in such nonsense.
The author is an anonymous medical student who blogs at unchainedmedical.
TAGGED AS: MEDICAL SCHOOL


Nosce te ipsum. Nosce inimicum tuum
According to Erich Fromm rational authority is based on competence, experience, and mutual respect. Irrational authority is often disguised as benevolent paternalism and is designed to perpetuate or intensify conditions of inequality through the use or threat of force, deceptiveness, and secretiveness.
The Federation of State Physician Health Programs (FSPHP) has has operated as an unexamined authority for the past 25-years . They have pushed practice and policy unquestioned and without opposition that has gravely harmed individual doctors, the medical profession itself and the public at large. Everything they have done has been done to benefit themselves and their drug and alcohol assessment, testing and treatment affiliates in the provision of protections, power and profits.
 Examining the specific practice and policy pushed reveals a body of false-claims making designed to facilitate the systemic use of coercion and threats, remove all due process protections and fundamental rights from physicians and prevent, block and eliminate the evidence. This practice and policy collective has created a culture of impunity, immunity and deference that is able to successfully conceal ethical violations and crimes. Uncovering their wrongdoing is a nearly impenetrable gauntlet. It is a system of institutional injustice that is undoubtedly a major contributor to the suicide epidemic in the profession. They have been able to conceal the truth, avoid investigation and prevent punishment for years by removing themselves from all accountability and outside inquiry. Direct and specific questioning appears to be their Achille’s heel as the recent spat of articles critical of these programs is showing just how much of an illegitimate authority they really are.
Examining the specific practice and policy pushed reveals a body of false-claims making designed to facilitate the systemic use of coercion and threats, remove all due process protections and fundamental rights from physicians and prevent, block and eliminate the evidence. This practice and policy collective has created a culture of impunity, immunity and deference that is able to successfully conceal ethical violations and crimes. Uncovering their wrongdoing is a nearly impenetrable gauntlet. It is a system of institutional injustice that is undoubtedly a major contributor to the suicide epidemic in the profession. They have been able to conceal the truth, avoid investigation and prevent punishment for years by removing themselves from all accountability and outside inquiry. Direct and specific questioning appears to be their Achille’s heel as the recent spat of articles critical of these programs is showing just how much of an illegitimate authority they really are.
In her rebuttal to Pauline Anderson’s article “Physician Health Programs: More Harm Than Good?” FSPHP President Doris Gunderson dismissed the accusations of fraud and abuse in one fell swoop as “allegations rather than facts” and second hand anecdotes. Countering allegations of an absence of oversight and regulation she states:

“In fact, we operate under a microscope, answering to individual practitioners, medical boards, malpractice carriers, defense attorneys, state attorneys, medical societies, hospitals, medical schools and residency training programs. We are also accountable to patient safety entities and a Board of Directors.”
Untrue. Accountability demands both provision of information and justification for actions to outside entities capable of punishing misconduct. . What was done and why? No such entity exists and no pathway for appeal or grievance redressal exists either. Zero accountability. Ditto for the “PHP-approved” assessment and treatment centers. As cash only out-of-pocket facility they remove themselves from the prying eyes of insurers.
 The North Carolina PHP Audit found the past FSPHP President and NC PHP director Warren Pendergast could not identify the qualitative or quantitative indicators used for “approving” PHP-approved facilities. The best he could come up with is “reputation” and “word of mouth” yet state medical boards mandate evaluations of doctors at these facilities and specifically exclude non-“PHP-approved” facilities.This is enforced by the Federation of State Medical Boards Policy on Physician Impairment. Each state managed by the FSPHP utilizes the same dozen or so facilities and each state medical board mandates it under threat of disciplinary action. It is in fact a rigged game.
The North Carolina PHP Audit found the past FSPHP President and NC PHP director Warren Pendergast could not identify the qualitative or quantitative indicators used for “approving” PHP-approved facilities. The best he could come up with is “reputation” and “word of mouth” yet state medical boards mandate evaluations of doctors at these facilities and specifically exclude non-“PHP-approved” facilities.This is enforced by the Federation of State Medical Boards Policy on Physician Impairment. Each state managed by the FSPHP utilizes the same dozen or so facilities and each state medical board mandates it under threat of disciplinary action. It is in fact a rigged game.
Denying accusations of coercion Gunderson states in her rebuttal to Anderson’s article:
“The detractors of PHPs interviewed for the article maintain that PHPs are coercive. Yet the report fails to mention that PHPs have no authority to mandate treatment and monitoring, suspend or revoke licensure, or otherwise discipline physicians.”
 The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy. (ASAM Policy on Coordination Between Treatment Providers, Professionals Health Programs, and Regulatory Agencies).
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy. (ASAM Policy on Coordination Between Treatment Providers, Professionals Health Programs, and Regulatory Agencies).
Legitimate authority articulates ethical, evidence-based, or internally consistent arguments when challenged. Legitimate authority does not simply delegitimize one’s opponent and use logical fallacy and obfuscation to avoid addressing the substance of an argument. In her rebuttal Gunderson claims the NC Audit was favorable to them because no evidence of abuse was found. This is akin to a serial killer claiming victory because no bodies were found in his dungeon replete with torture devices and restraints. State auditor Beth Wood set this straight when she told the BMJ in Physician Health Programs Under Fire that the holes were big enough in the program “you could drive a truck through them” and it would be “difficult, if not impossible, to defend” oneself against an incorrect assessment” as no ability to “appeal a diagnosis or assessment” existed.
 “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
Multiple Barriers Removing Accountability at Multiple Levels
The inability to obtain one’s own medical records or lab reports is the first obstacle one must overcome. The second barrier is that even if documents are obtained there is no one to give them to. The third is the existence of “point people” who deflect, block and otherwise dismiss valid complaints. The only oversight provided to the involved labs is an an accreditation agency, the College of American Pathologists (CAP) They can investigate and correct but do not have the ability to sanction.
 Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
It is therefore critical it be recognized for what it shows and it is morally imperative that those involved be held to account as the documents illustrate clearly and undeniably a collusion between a state PHP and its drug testing lab to fabricate evidence. The corruption is top-down as it involves another former FSPHP President Luis Sanchez and the VP of Laboratory operations at USDTL Joseph Jones. As explicit and detailed as it is in revealing unequivocal black and white crimes it has been ignored by the usual channels.
 Research on street criminals suggests the certainty of punishment has the strongest deterrent effect (basically will I be caught) and the more people think they will be arrested for a crime the less likely they are to commit it. Criminals weigh their actions against possible gains and consequences and the risk of consequences in this system have been essentially zero. Diagnosis rigging, coercion, threats and abuse are rampant because they have no fear of punishment. The Chairman of the commission that examined the causes of the 2008 financial collapse compared the relatively small fines paid by corporations to “someone who robs a 7-Eleven, takes $1,000 and being able to settle for $25 and no admission of wrongdoing.” He added,“Will they do it again? Absolutely, because it pays.” This is like someone who robs a 7-Eleven, takes $1,000 and never gets caught so he goes to the next 7-Eleven and takes $2000 then hits as many 7-Elevens as he can for as much as he can. There is zero-accountability. No fines. No repercussions. No risk. What has happened is not only logical but inevitable. It is time to name the enemy. The enemy is not state physician health programs (PHPs) but those in charge of them. The Federation of State Physician Health Programs (FSPHP) is a heretofore unexamined authority. Current evidence is revealing the FSPHP is also an irrational authority. It is also quite easy to show by historical documentation of the policy and practice they have pushed that they are an illegitimate authority. Illegitimate authority when identified and recognized needs to be removed.
Research on street criminals suggests the certainty of punishment has the strongest deterrent effect (basically will I be caught) and the more people think they will be arrested for a crime the less likely they are to commit it. Criminals weigh their actions against possible gains and consequences and the risk of consequences in this system have been essentially zero. Diagnosis rigging, coercion, threats and abuse are rampant because they have no fear of punishment. The Chairman of the commission that examined the causes of the 2008 financial collapse compared the relatively small fines paid by corporations to “someone who robs a 7-Eleven, takes $1,000 and being able to settle for $25 and no admission of wrongdoing.” He added,“Will they do it again? Absolutely, because it pays.” This is like someone who robs a 7-Eleven, takes $1,000 and never gets caught so he goes to the next 7-Eleven and takes $2000 then hits as many 7-Elevens as he can for as much as he can. There is zero-accountability. No fines. No repercussions. No risk. What has happened is not only logical but inevitable. It is time to name the enemy. The enemy is not state physician health programs (PHPs) but those in charge of them. The Federation of State Physician Health Programs (FSPHP) is a heretofore unexamined authority. Current evidence is revealing the FSPHP is also an irrational authority. It is also quite easy to show by historical documentation of the policy and practice they have pushed that they are an illegitimate authority. Illegitimate authority when identified and recognized needs to be removed.
Nosce te ipsum. Nosce inimicum tuum. Know thyself, know thy enemy. The FSPHP is the enemy. They cannot be bargained with. They need to be removed. In the interim we need to set up advocacy and watchdog groups to help and protect those already caught in this web of manipulation, oppression and fear. Wake up, Stand up and Speak up. Silence is consent. Let’s drain this swamp in 2017.


 Link to Medscape article by Pauline Anderson Here:
Link to Medscape article by Pauline Anderson Here:
Link to illegible, post-dated and undated documents submitted as evidence and mentioned in article can be seen here> board-records-obtained-june-2016
Link to document written June 6, 2013 but date-stamped as being received in 2012 ( both by hand and apparently by the Board’s Document Imaging Unit (DIU) > Back to the Future: Massachusetts Board of Registration in Medicine


Michael Langan, MD, a Boston-based internal medicine specialist who has fought the Massachusetts Physician Health Service (PHS) and Board of Registration in Medicine for years to reinstate his license, has suffered a setback but is bolstered by a new development.
A justice of the Supreme Judicial Court of Massachusetts has denied Dr Langan’s petition to invalidate the 2013 suspension of his medical license for not meeting conditions to have his license reinstated.
However, a new law has enabled Dr Langan to access his records. According to Dr Langan, these documents show that the court did not consider key evidence in his case, as demonstrated by the fact that his hearing occurred after the date of receipt that is stamped on the documents. This may offer an opportunity to reopen his case.
The court decision, which was handed down in December by Associate Justice Geraldine Hines, states that although Dr Langan completed required psychiatric evaluations, he “did not submit a suitable worksite or substance abuse monitoring plan. In combination with his violation of the LoA [Letter of Agreement] meeting requirement, the board’s decision to affirm its prior suspension of petitioner’s license to practice medicine is supported by the record. The board’s decision to deny reinstatement in the absence of an acceptable plan is affirmed.”
“It’s unbelievable; everyone is dumbfounded,” said Dr Langan of the decision.
Dr Langan is appealing the denial of his petition, a process that will take an estimated 6 months.
He maintains that the PHS committed “forensic fraud” and concealed doing so.
“If I couldn’t win with all the direct evidence of felony crimes that you don’t need to be a lawyer to recognize, then I don’t think anyone can,” he told Medscape Medical News.
The PHS is a confidential resource for physicians and medical students seeking help for a variety of physical and behavioral health concerns, which may include difficulties with substance use.
In 2007, Dr Langan was at Massachusetts General Hospital (MGH) and Harvard University when he approached the PHS to help him with his dependence on Vicodin, an opioid analgesic.
He became dependent on Vicodin after a bout of chickenpox during residency, when he developed shingles. He stressed that there were no work-related problems associated with use of this drug.
According to Dr Langan, there were no problems until mid-2011, when a report from the US Drug Testing Laboratories found he was positive for phosphatidylethanol (PEth), a blood marker for chronic alcohol use.
The level detected was 365.4 ng/mL, which “is the equivalent of drinking a half gallon of whisky a day,” or a sign of end-stage alcoholism, said Dr Langan, who insists he has never had an alcohol problem.
“That the test was invalid at this point should have been self-evident,” said Dr Langan.
Lab Fraud?
Suspecting that there had been “lab fraud” and that he would “end up being admitted for 3 months,” Dr Langan said he requested, but was denied, an independent evaluation outside the 12-step PHP-approved list of facilities. Because his request was denied, he attended one of the approved facilities, Hazelden Addiction Treatment Center, in Minnesota, where he “was cleared.”
An independent investigation by James G. Flood, PhD, who has been chief of toxicology at MGH for nearly 30 years, concluded in a November 5, 2012, letter to Dr Langan’s lawyer “that there is a purposeful and intentional act by PHS” to show Dr Langan’s test as valid “when in reality this test was invalid and involved both fatal laboratory errors” and inadequate review of the results.
Any confirmatory, positive finding based on the July 2011 test “should be reversed, rectified and remediated,” Dr Flood writes.
Dr Flood claims the sample was directed to the wrong laboratory, where it sat for several days. The storage conditions of the sample while at that laboratory were not documented.
Following an investigation by the College of American Pathologists, in October 2012, Dr Langan’s laboratory test result was corrected from having a positive result to being an invalid test, but he said he did not learn of this change until months later.
Dr Sanchez noted that, on the basis of the revised report, “PHS will continue to disregard the July 2011 PEth test result.”
Dr Langan requested the record of the chain of custody pertaining to his testing. This document showed that the test was “not only invalid but falsely created,” said Dr Langan. He added that it included a fax from the PHS requesting that his identification number be added to an already positive test and that the chain of custody be updated.
“You can’t update a chain of custody, as it is generated in real time,” said Dr Langan. “This is forensic fraud. It clearly shows collusion between the PHS and the lab.”
In an October 2012 letter, Dr Sanchez alleged that Dr Langan did not attend required peer support group meetings, but according to Dr Langan, this claim is “without fact or support.” Dr Langan maintains that he attended all required meetings. He also maintains that the PHS actions were in “retaliation” for requesting the chain of custody record.
Massachusetts PHS Director Dr Sanchez did not respond to a request from Medscape Medical News for clarification.
“The AG’s [Attorney General’s] Office often defends state agencies in litigation and we typically do not comment on behalf of our clients, who in this case is the Board of Registration in Medicine,” Emily Snyder, deputy press secretary, Office of Massachusetts Attorney General, told Medscape Medical News in an email.
Intentional Delay?
Dr Langan alleges that the PHS “intentionally delayed” his efforts to undergo a psychiatric evaluation that was necessary to have his license reinstated. He said the PHS insisted he get this evaluation out of state, even though he suggested three Boston-area board-certified experts.
Dr Recupero’s November 2013 report determined that Dr Langan “is safe to return to the practice of medicine without further supervision,” that he “has an excellent prognosis and a very low risk of relapse,” and he “has not had an alcohol use, abuse or dependence problem.”
Many of the conflicts between the PHS and Dr Langan revolve around positive test findings, Dr Recupero notes in her letter.
Dr Langan acknowledges he used hand sanitizers in the course of his work as a physician. Owing to severe allergies, he also uses prescribed asthma inhalers, which contain alcohol as a propellant.
Dr Recupero also notes that “almost without exception,” Dr Langan’s test findings have been below the minimum level to declare a test positive and that positive findings “are not a sign of relapse.”
Dr Langan said that since it suspended his medical license, the board has “engaged in a persistent pattern of ignoring my every reasonable effort at trying to be reinstated” and has “abused the administrative law process to accomplish this.”
Medscape Medical News contacted the Massachusetts medical board as well as its counsel, Deb Stoller, but received no response.
“Close to Homeless”
A memorandum to the Supreme Judicial Court, filed May 13, 2016, proposed a settlement between Dr Langan and the board. In return for the immediate reinstatement of Dr Langan’s license, he would be monitored for a maximum of 3 months by Dr Recupero and Timothy E. Wilens, MD, codirector of the Center for Addiction Medicine at MGH.
That memorandum was accompanied by letters from Dr Recupero and Dr Wilens agreeing to the terms, but according to Dr Langan, it has been “ignored.”
“The board did not acknowledge or address the proposals in any way,” said Dr Langan.
Dr Langan maintains that he “never ever” had any patient care or malpractice problems during his 15 years at MGH. In fact, his supervisors and colleagues reported that his work performance has been “superlative” on all counts, he said.
Many in the addiction medicine and psychiatric community support Dr Langan. He has letters from high-profile physicians in the field who verify that he is safe to practice medicine.
A first petition was filed in the Supreme Court on October 22, 2014, but the judge dismissed it because it had not been filed within the required 60-day period. Dr Langan’s most recent petition was filed July 3, 2015.
The past few years, he said, have taken a toll on his family. They have lost their home and health insurance because of his inability to practice his profession.
Disheartened by this latest setback, Dr Langan is looking into the possibility of becoming licensed in another state and leaving Massachusetts.
But Dr Langan has renewed hope. Under Massachusetts’ new Public Records Reform Law, which went into effect January 1, 2017, “the board was forced to comply with my request for records within 10 days,” and has done so, he said.
According to Dr Langan, these records show some irregularities that may bolster his case.
“A letter dated December 15, 2011, introducing exculpatory evidence was date-stamped January 17, 2012, almost 1 month after the hearing where it was submitted as evidence. All of the other documents had either illegible or absent date-stamps,” he said.

Milton Friedman (July 31, 1912 – November 16, 2006) was an American economist who received the 1976 Nobel Memorial Prize in Economic Sciences
In an article written for the March 2015 Physician Health News, the official newsletter of the Federation of State Physician Health Programs (FSPHP) President Doris Gunderson reviews the history of the organization in honor of its 25th anniversary. She writes:
“In 1990 the FSPHP was born out of a need for individual state programs to work together in discussing and promoting best practices and especially to influence national public policy.”
For the last quarter century the FSPHP has pushed a plethora of both practice and policy (legal, regulatory and healthcare) that claims to assist state physician health programs in identifying, managing and monitoring impaired physicians and protect the public from harm.It was recently suggested by the Chief Editor of American Society of Addictions Medicine (ASAM) Weekly News that this same group take the helm in influencing public policy for addiction medicine at large (i.e. not just doctors but everyone from our kids to our pregnant mothers to our elderly) on a national organizational level.
It is time we examined both the authority and the knowledge claims on which they are based.
In her rebuttal to Pauline Anderson’s August 2015 Medscape article ‘Physician Health Programs: More Harm Than Good? Gunderson dismissed criticisms as “allegations rather than facts” and “second hand anecdotes.”
In response to allegations that PHPs have no oversight Gunderson comments:
“In fact, we operate under a microscope, answering to individual practitioners, medical boards, malpractice carriers, defense attorneys, state attorneys, medical societies, hospitals, medical schools and residency training programs. We are also accountable to patient safety entities and a Board of Directors.”
The list of organizations Gunderson has to “answer” to appears to be many of the organizations and societies that physician health programs interact with. She might as well add Blockbuster for getting her videos back on time. This is not meaningful oversight. Oversight equates with accountability and that requires answerability (the provision of information) and justification for one’s actions. It also requires the presence of an outside organization truly independent of the group that is able to sanction or punish individuals for wrongdoing or misconduct. No such organization exists for state physician health programs. Period. There is no organization that exists that is able to investigate a complaint of misconduct and provide sanctions. The same applies to their primary business associates, the assessment and treatment centers (because they are private pay and out-of-pocket) and drug and alcohol testing labs (because they use non-FDA approved tests). The entire racket is unaccountable and unexamined.
Kathryn Pyne Addelson warned that what we should fear most is “unexamined” authority. “Illegitimate politicization and rampant irrationality find their most fruitful soil when our activities are mystified and protected from criticism.”
This group has been protected from criticism for the better part of a generation. They have enjoyed making authoritative pronouncements as unexamined authority. Their power depends entirely on not being questioned as what is behind the curtain is flimsy and dredged, a Potemkin village. The recent Medscape and BMJ articles are revealing that confrontation with direct and precise questions results in nothing but logical fallacy, distortions and lies. They are utterly incapable of responding with a direct and precise answer. Gunderson’s response to absent oversight is just another example of this logical fallacy and distortion. This is not how rational authority responds. This is not how legitimate authority responds. I kindly invite her to debate this. I would like a back-and-forth to clarify. It is a simple question that deserves a simple answer and I know she follows my blog as she used her own name and e-mail address.
The cumulative comments on the articles critical of these programs are revealing a system of oppressions, injustices and illusions. A more recent article on Medscape, “One-Man Fight: MD Takes on State Medical Board, PHP” reports the same pattern of coercion, absence of due process and diagnosis rigging for sham peer review that I am hearing from doctors across the country. The comments section to this article are also overwhelmingly critical of PHPs. They are pertinent, articulate and precise and missing from them is any semblance of a rebuttal by the FSPHP, their apologists or anyone else. The writing is on the wall as they say. And for that reason we call upon all those of good will in both the medical profession and the public at large to join us in this confrontation with illegitimate, irrational and immoral authority.
- Gunderson D. Message From the President Twenty-Five Years: A Remarkable Journey. Physician Health News. 2015;20(March).
- Addelson KP. The Man of Professional Wisdom. In: Fonow MM, Cook JA, eds. Beyone Methodology: Feminist Scholarship as Lived Research. Bloomington: Indiana University Press; 1991:16-35.

But in this Court, what Diff’rence does appear!
For every one’s both Judge and Jury here;
Nay, and what’s worse, an Executioner.
William Congreve, The Double-dealer

Regulatory capture is a form of government failure that occurs when a regulatory agency created to act in the public interest, instead advances the commercial or political concerns of special interest groups that dominate the industry or sector it is charged with regulating and introduced in an article by George J. Stigler in 1971 entitled The Theory of Economic Regulation. The main idea of the article can be summarized in Stigler’s (1971: 3) affirmation that:
“…as a rule, regulation is acquired by the industry and is designed and operated primarily for its benefits.”
The basic hypothesis of Stigler is that an industry may use—or rather abuse—the coercive public power of the State to establish and enforce rules in order to obtain private gain.
Historians will at some point recognize 1995 as the “regulatory capture” inception point of American medicine when the Federation of State Physician Health Programs ( FSPHP ) forged a relationship with the Federation of State Medical Boards (FSMB), the national organization responsible for the licensing and discipline of doctors and memorialized in a 1995 Journal of Medical Licensure and Discipline(Vol82N3)with articles claiming high success rates in eight state PHPs.
An accompanying Editorial written by past President of the FSMB Barbara S. Schneidman, MD, MPH concluded that:
“cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.”
Roger A. Goetz of the the Florida Impaired Practitioners Program, for example reported that 84% of all referrals to the PRN “Occur prior to any violation of the Medical Practice Act or any evidence of patient harm.” Journal of Medical Licensure and Discipline(Vol82N3) As protecting the public from patient harm is the primary directive of medical boards those statistics seem pretty impressive! That the PRN prevented inevitable spirals of drug addled and besotted doctors from mayhem is questionable as how many were just like Leonard Masters? After being accused of overprescribing Goetz told Masters he could either relinquish his license or have an evaluation. Masters chose the evaluation thinking he would be returning in 4-days but was diagnosed as an alcoholic and spent 4-months. He didn’t even have a drinking problem. He successfully sued G. Douglas Talbott and the facility for false imprisonment, malpractice and fraud.

Goetz was also instrumental in promoting the chronic-relapsing brain disease model as a pathway to return revoked medical licenses. No matter how abhorrent their behavior, by misplacing blame on the “disease” doctors who should have hung up their smocks forever quickly returned to practice as they didn’t do it the drugs or alcohol did. In this manner serial sex-offenders, pedophiles, date-rapists using roofies and fiends who replaced dying cancer patients narcotics with saline and let them die in agony were quickly returned to the fold. The error in this thinking is that for the most part drugs and alcohol may induce good people to do disinhibited things or stupid things but they do not make good people do bad bad things. Empathy and moral compass are innate and the majority of doctors would not roofie drinks or take away dying patients pain meds under any influence. Unfortunately no test exists for psychopathy.
Many found employment as medical directors of these specialized programs and others became active in their states PHPs.
Since that time the FSPHP has duped the FSMB easier easier than a carney dupes a rube.
They asked the FSMB to approve public-policy to request state medical boards provide absolute deference to their state PHPs as their experts in all things related to physician health and to agree to never ever question their decision making skills regarding monitored doctors lest it “undermine a culture of professionalism” and this was agreed to.
Deference is acceptable but agreeing to blind deference and accepting the delusion of infallibility is unwise. A culture of deference is unacceptable. Lord Acton noted in a letter to a friend that the main point he was trying to get across when he wrote “Power tends to corrupt, and absolute power corrupts absolutely”was not that power corrupts powerful people but that power corrupts other people. This dynamic certainly holds here. They make allowances.
Since that time they have expanded from ‘impaired physicians” to “disruptive physicians” to the “aging physician.” They have gained power and autonomy without regulation or oversight and by removing transparency and absolutely zero accountability they have essentially run amuck.

In 1995 this was a simple but growing shakedown scheme using a medical license to extract money under the threat of its loss. The PHP refers doctor X to “PHP-approved facility” for an evaluation and the “PHP-approved” facility tells doctor X you will stay here until I say so or I tell the PHP you ain’t gettin your license back. Doctor X stays because he knows the PHP can do it as the PHP is not going to be questioned by the medical board.They refer to it as “contingency-management” but it essentially meets the criminal definition of extortion.
Business has boomed since 1995 as they introduced non-FDA approved drug and alcohol tests into the market even though they are unvalidated with very low specificity. Junk-gadgets such as the SCRAM alcohol monitoring bracelet and the Soberlink cellular photo breathalyzer have been promoted as accurate and valid. None of this has any oversight but their linkages with the drug and alcohol testing, assessment and treatment industry has become an enormous gold mine. Both the drug-testing and assessment and treatment industry are multi-billion dollar enterprises.
The FSMB even made it public policy for medical boards to provide deference to PHPs and consider them experts in all things physician health. In this manner they have introduced a panoply of junk science, brought legions of polygraph examiners out of their basements and rebranded the 360 degree personal development employee assistance tool as a bona fide diagnostic instrument used for disruptive physician evaluations. The FSMB has also accepted concocted and imaginary concepts such as “potentially impairing illness” and “relapse without use” as not only nonfictional but medically scientific truth. If they proposed tiddlywinks for assessment of the “aging” physician the FSMB would probably buy it. Is potentially potentially impairing illness next.? There has been no apparent inquiry or opposition to this.
Accountability requires both the provision of information and justification for actions and they have minimized both. Prohibiting doctors from obtaining their own assessments, medical records and drug-testing records markedly reduces risk of exposure as does prohibiting release of those records to third parties. Cash only prevents inquiry from insurers. The PHPs have no oversight or regulation. The drug and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
And with zero accountability corruption not only thrives but is inevitable. The simple extortion scheme from 1995 has now grown to around two dozen “PHP-approved” assessment and treatment centers and state boards require that only “PHP-approved” facilities be used and specifically excludes non “PHP-approved” facilities. The preferred facilities engage in “diagnosis rigging” and false diagnoses to warrant unneeded treatment. The labs such as USDTL and Quest engage in laboratory misconduct and will create a falsely positive test at client request. It is a closed system where everything is kept within the PHP circle.
And complete regulatory capture has been achieved through autonomous units within Boards that essentially serve as PHP protection units and hired guns. They protect the PHP and their friends and also act as an assassin squad to do whatever the PHP wants them to do to suspend, revoke and interfere with the medical licenses of doctors any which way they want.
In Massachusetts Policy 94-002 created Physician Health and Compliance Unit (PHCU) Board counsel as an independent unit outside the enforcement division of the Massachusetts Board of Registration in Medicine by design.
These units were created at the request of state physician health programs ostensibly to monitor the compliance of doctors under monitoring their monitoring contracts. The MA PHCU Board counsel is run by attorney Deb Stoller and also includes attorneys Robert Harvey and Tracy Ottina.
 PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also. They were set up to hold all the cards and it is a stacked deck.
PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also. They were set up to hold all the cards and it is a stacked deck.
This additional circle around the closed-loop system provides an additional layer of protection to prevent the fraud and abuse from being discovered. That the Massachusetts Board is not under any active supervision from the executive branch has been confirmed in writing to the Massachusetts Legislature by Governor Charles Baker in a letter accompanying his Bill (H.4188) which aimed to finally establish a framework for active supervision and oversight over the Board.
These units enforce PHP policy and requirements including the restriction of assessments to the out of state (“PHP-approved”) assessment and treatment centers and forbid any outside assessments. Any doctor in Massachusetts will be forced to go to Georgia, Alabama, Arkansas, Kansas or some other remote venue for an evaluation under the guise of special knowledge. Any doctor reported to the PHCU as “non-compliant” is summarily suspended. Truth and evidence are irrelevant. The opinions of all outside experts no matter how qualified or how many are not only dismissed they are patently ignored with eyes wide shut. They simply do not register anything outside the racket. They abuse administrative law procedure to dismiss, deflect and delay. Having the power to act as both a hearing-officer to accept or exclude evidence and present cases to the Board and make disciplinary recommendations provides them with absolute power to render judgment. It means they are in charge of every decision made, and they have the power to be rid of whomever they choose as judge, jury and executioner. The Board’s simply defer to PHCU Board counsel and give little thought or time to what was presented and ratify whatever is asked. They are uninformed and disengaged.
The system is almost foolproof. It is a culture of impunity and deference. To make matters worse states Attorney Generals defer to the medical-board and their physician health experts. The AGO represents the state agency and its expert in legal challenges and crimes reported by doctors are dismissed at the outset. The agency responsible for investigating rackets and laboratory and healthcare fraud as well as civil rights violations and color of law abuse is the states AGO. No one is minding the minders.
The assistant AGOs representing boards appear to use the same tactics as the PHCU Board counsel and a similar moral disengagement mentality but it is unclear what the interface is with the PHP/medical board and states AGOs. If anyone has any insight please advise as I have not figured it out. Perhaps they agreed to deference to the medical board/PHP just as the medical board agreed to deference to the PHP. Perhaps they have specific administrative attorneys who they use or even a cadre within but it is implausible that the entire AGO would be supporting the rehab racket.
But in the final analysis this has resulted in is a complete systems failure where corruption and abuse is occurring as a product of bad apples in plain view and within the walls of regulatory medicine with each agency deferring to the integrity and honesty of its predecessor. This is not good governance.
Historians will someday look back at the fall of American medicine and wonder how it was allowed to happen and link systemic as well as specific problems pervasively plaguing the profession with regulatory capture by the drug and alcohol testing, assessment and treatment industry.


Accountability, or answerability, is necessary to prevent abuse and corruption. This requires both the provision of information and justification for actions. What was done and why?
Professional guidelines and standards of care, ethical codes of conduct and the law are all objective benchmarks that can be used to assess the actions and decisions of others. In any free society this necessitates the existence of organizations of truly independent opinion capable of standing in this judgment.
State PHPs are Non-Governmental Organizations (NGOs) over which the state health department has no supervisory oversight. There is no regulation, no transparency and no accountability. There is no public scrutiny and they police themselves.
In Ethical and Managerial Considerations Regarding State Physician Health Programs Drs. John Knight and J. Wesley Boyd call for greater oversight and scrutiny of PHPs by the medical community at large. They recommended periodic auditing, national standards and regulation. They also attempted to convince the Massachusetts Medical Society to implement changes at PHS where they served as Associate Directors with over two decades of collective experience.
These efforts to promote transparency and accountability at both local and national levels, however, fell on deaf ears.
State PHPs have systematically removed those not conforming to groupthink. Threatening them with litigation if they breached “peer-review” statutes and confidentiality agreements has effectively silenced them from reporting any misconduct, abuse or even crimes they may have witnessed.
In Massachusetts John Knight was removed in 2009 and J. Wesley Boyd in 2010. In Ethical and Managerial Considerations Regarding State Physician Health Programs they comment “if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise—tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.” So too will the clinical laboratories.
How is this any different from the case of Dr. Farid Fata, the Michigan oncologist who intentionally diagnosed healthy patients with cancer so he could charge them for unneeded chemotherapy? The U.S. Attorney called it the “most egregious” case of health care fraud ever. His acts may have contributed to one patient death. The institutional injustice of the PHP system is causing countless deaths of physicians.
To consciously “tailor” a diagnosis is fraud. To tailor a diagnosis of substance use disorder or any other psychiatric diagnosis is the political abuse of psychiatry. Misrepresentation, dishonesty, deception, and distortion play no role in the Profession and Guild of Medicine. To do so violates the basic moral principles of Medical Ethics–Autonomy, Beneficence, Non-Maleficence and Justice.
The “PHP-approved” assessment and treatment centers are all staffed by doctors of “like-mind.” It is a rigged game.
An audit of the North Carolina PHP found essentially no oversight from the Medical Board or Medical Society. The audit found that “abuse could occur without being detected,” and this is by design. By removing and blocking the provision of information necessary for accountability, restricting the liberties and freedoms of physicians, and increasing their power and control they have erected a framework of hidden abuse.
The situation in North Carolina is standard operating procedure for PHPs under the Federation of State Physician Health Programs (FSPHP). It is not the exception but the rule.
While outspoken in denouncing what they regard as unethical and unprofessional behavior by other doctors, they are resistant to apply even the most minimal standards to their own activities.
To whom are the PHPs accountable? Whom do they represent? These are legitimate concerns.

Please click on the link below and complete the following survey if you have been monitored or are being monitored by a PHP.
Professional Health Program (PHP) Survey
This is a confidential survey. If you have concerns about anonymity please create an alternative alias email address (this video shows you how to create an alias G-mail address), then use the alias email address as your “name” for future correlation.



Physician Health Programs are not Above the Law
Are Physician Health Programs (PHPs) above the law?
Unable to get law enforcement to take cognizance of reported abuse, many doctors I have spoken with believe that the actors involved are impervious to criminal liability. Complaints of fabrication and fraud involving PHPs and their affiliates to the police, the Attorney General and other law enforcement agencies have been given no credence, tabled or dismissed with little investigation.
Believing these agencies are deliberately ignoring credible complaints and the documentary evidence placed before them, some have concluded that state PHPs have been given the power to commit crimes with impunity and immunity.
PHPs are not above the law. It is by removing themselves from and blocking the usual routes of accountability and absolute operational control of the testing, assessment and treatment process that has enabled misconduct to remain hidden, unrecognized or excused. The crimes exist but they remain undetected, unnoticed and unpunished.
Removing Accountability
The essence of accountability is answerability which means having the obligation to answer questions regarding decisions and actions. This requires the transmission of information when it is requested. The accountable actor provides the information to the overseeing actors in a transparent manner.
Accountability also requires explanation and justification for the information provided. What was done and why? Standards, rules, regulations, codes, laws and other benchmarks are then applied by the overseeing actor to determine if the information provided was appropriate or inappropriate.
The availability and application of sanctions for illegal or inappropriate actions uncovered through answerability is also a necessary component of accountability. This is necessary to impose restraint on authority and power. Lack of enforcement of sanctions contribute to the creation of a culture of impunity.
The usual mechanisms that exist to impose restraint and create incentives for appropriate behavior and actions are absent. No outside oversight exists to limit their power or subject them to a set of rules. No regulation exists to curb abuse.
A Culture of Impunity
The authority accorded PHPs and the power they exercise exist in a culture of impunity.
The key findings of the2014 North Carolina PHP Audit are below:.
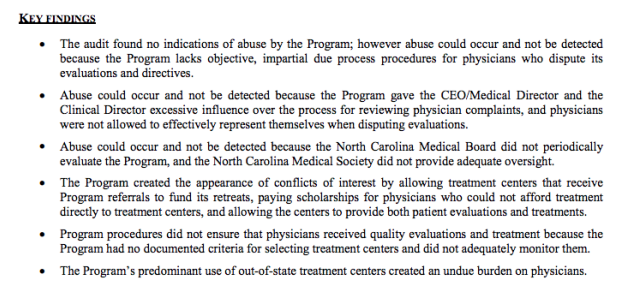
No indications of abuse were found, a point brandished by the PHP as redeeming and proving no abuse was occurring. In actual fact it is an ominous finding that also relates to their apparent ability to violate the law.
The audit found no indications of abuse but that abuse could occur and not be detected because of an absence of due process for the complainant, excessive control of the complaint process by the PHP and absence of oversight by either the medical board or medical society. What this means is that a doctor with no power is making a complaint against an unsupervised agency with enough power to influence the investigation of a complaint against itself. The reason no indications of abuse were found is because the system is specifically designed to hide abuse. That is the intent.
Absence of transparency, regulation and oversight coupled with control of information enables both censorship and doctoring of records. Strict Confidentiality is enforced by HIPAA, peer review protection, and drug and alcohol confidentiality law.
PHPs are able to suppress and conceal criminal activity but they are also able to manufacture information designed to hide misconduct.
The North Carolina Audit found no objective selection criteria for the out of state assessment and treatment centers because none exist other than ideological mindset and monetary gain. The same facilities are used by most state PHPS. They are, in fact, mandated as they are the “PHP-preferred” facilities.
In 2011 The American Society of Addiction Medicine (ASAM) issued a public policy statement on coordination between PHPs, regulatory agencies, and treatment providers. recommending only “PHP-approved” treatment centers be used and the statement specifically excludes ‘non-PHP” recognized facilities.
What the Audit diid not discover is the medical directors of all of the “PHP-approved” facilities can all be seen on this list of Like-Minded Docs. It is a rigged game Every aspect of drug-testing, assessment and treatment is kept hidden and secret and within control of the PHP.
It is a rigged game in which they have removed themselves from all aspects of accountability. They have, in effect, manufactured a culture of impunity at our expense.
“PHP-Approved Attorneys”
My survey has revealed an additional factor stacking the deck and removing accountability from PHPs. The attorneys ostensibly representing doctors are also part of the racket.
A doctor referred to a PHP will be given a list of 3 or 4 attorneys by the PHP who are “experienced in working with the medical board.” What they do not tell you is that theses attorneys are hand-picked or cultivated to abide by the rules dictated by the PHP.
They will not “bite the hand that feeds” and any procedural, ethical or criminal misconduct by the PHP will not be addressed. Laboratory fraud, false diagnoses, and Establishment Clause violations are off limits.
The primary purpose of these attorneys is to enforce payment for laboratory fees and demand compliance with whatever the PHP demands. Their primary purpose is to keep doctors powerless under the PHP and prevent misconduct, including crimes, from being discovered.
The attorney pool is currently over-served by those serving two clients and most of those outside simply do not know enough about the “physician health” legal issues related to doctors. When they appear before the board it is as if they are a deer in the headlights. It is a new terrain where all due process and familiar protocol have been removed. Of course this was all facilitated by changes in administrative and medical practice acts orchestrated by the physician health movement “in the interests of protecting the public. This must be recognized and addressed.
Skilled negotiators and lawyers with administrative law experience would do well to consider representation for doctors before medical boards regarding “physician health” matters.
It is not that esoteric, complicated or difficult. As with the rest of the population, most have just not critically analyzed the issues behind the curtain.
Crooked Board Attorneys
Perhaps the lowest bottom feeders playing a role in this culture of impunity are those whose job is to ostensibly ensure that due process and fundamental fairness are followed. It is becoming quite clear that some of the state employed attorneys within medical boards control the flow of information by picking and choosing what is before the board for consideration. Many of these attorneys go on to represent doctors in cases before the board. If these attorneys acted as zealous advocates on behalf of their clients they would never get a referral again and because of this the system is plugged with an attorney pool unwilling to win but simply compromise.


 To sign the petition please click here.
To sign the petition please click here.State Physician Health Programs (PHPs) were originally developed by competent and caring physicians to help colleagues who developed problems with addiction or substance abuse.
As an alternative to disciplinary action by state Medical Boards they provided a safe haven for sick doctors while also protecting the public from impaired physicians.This image as a humanitarian agency with virtuous organizational purpose has created an absence of the need to guard. Any system can be subverted, but as self-governing organizations with no meaningful transparency, oversight, regulation or accountability these organizations were particularly vulnerable to exploitation.
State PHPs have been gradually taken over by the Federation of State Physician Health Programs (FSPHP). The FSPHP is an offshoot of the American Society of Addiction Medicine (ASAM), the self-proclaimed “voice of addiction medicine.”
A “self-designated” medical specialty, American Board of Addiction Medicine (ABAM) “board certification” is not recognized by the American Board of Medical Specialties (ABMS).
Through a torrent of propaganda and misinformation, however, combined with strategic and successful lobbying efforts they have gained tremendous sway in the field of addiction medicine. Advancing the 12-step rehab drug testing agenda they have modified and monopolized the field. By cozying up to regulatory boards and politicians they have altered the rules, statutes, and regulations to provide immunity, impunity, and confidentiality. All of this was done without difficulty or any meaningful opposition. They have swayed legal opinion and successfully tinkered with the system to amend rules and policies.
Many consider the ASAM and FSPHP to be corporate front groups, organizations whose agendas match those of corporate interests but who claim no formal relationship. In this case the agenda is 12-step rehabilitation industry and the drug testing industry. Over the past 10 years the ASAM has grown to over 3000 physicians. Within this group there is a subset of recovery fundamentalists who have populated the PHPs. Many have also become medical directors of the rehabilitation facilities to which they refer. By removing dissenting physician who do not agree with the groupthink they have successfully taken over the State PHP system. The evidentiary standard is low. They encourage confidential referral from colleagues and provide immunity to those who refer. If the PHP believes a physician “could benefit” form their services there is no choice. The FSPHP political apparatus exerts a monopoly of force. It selects who will be monitored and dictates every aspect of the evaluation and monitoring process. Conflicts of interest abound.
Control has replaced conduct and ideology has trumped science and reason. It is a system that fosters corruption and impunity. There have been reports of gross misconduct and breaches of standards of care, ethical violations, and civil rights violations. Basic human rights violations and criminal activity has been reported.
In Massachusetts caring and competent physicians such as J. Wesley Boyd and John R. Knight were removed from the State PHP, Physician Health Services, Inc. (PHS). In an article written for the Journal of Addiction Medicine in 2012 they address some of these concerns and suggest the “broader medical community begin to reassess PHPs as a whole.” They recommend independent oversight, transparency, national standards, periodic auditing, and an appeals process. They state:
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate outside the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are therefore, not in a position to voice what might be legitimate objections to PHP’s practices.”
The FSPHP has introduced junk science such as Ethyl Glucuronide, Ethyl Sulfate, and Phosphatidylethanol as long term alcohol biomarkers with no evidence base. They did this by getting them approved as “Laboratory Developed Tests” (LDTs) to bypass FDA scrutiny. There is no evidence-based support for these tests but the FSPHP convinced Regulatory Agencies (medical boards) that they were valid tests. This “medical sanctification” of these bogus tests resulted in other monitoring programs utilizing them and, unregulated by the FDA, the labs doing the tests could claim they were accurate and reliable with no repercussion. they are claiming the PHP programs as the “new paradigm in addiction treatment” claiming an 80% success rate. They have also created a myth that medical mistakes are the result of a hidden cadre of drug addicted doctors and are behind the recent call to randomly drug test all physicians. Of course who will run such a program? They will. They also want to expand to other organizations such as the DOT.
There is a lot of anecdotal evidence that the marked suicide rate in physicians is because of this.
The propaganda and misinformation is based on a study that is misleading and full of methodological flaws.
In “Ethical and Managerial Considerations Regarding State Physician Health Programs,” published in the Journal of Addiction Medicine in 2012, John Knight, M.D. and J. Wesley Boyd, M.D., PhD recommend ”the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.”
They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”
In evaluating a physician this group is not gathering data to form a hypothesis but making data fit a hypothesis that arrived well before the physician did. And this may be part of the explanation for the recent marked increase in physician suicide. With guilt assumed from the start, no due process, no appeal, and no way out physicians are being bullied, demoralized, and dehumanized to the point of hopelessness. This needs to end now.
Medicine is predicated on competence, good-faith, and integrity. Medical ethics necessitates beneficence, respect, and autonomy. The scaffold erected here is designed for coercion and control. Exposure, transparency, and accountability are urgent. An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
In addition it is a “rigged game” as the ASAM makes the public policy and the FSPHP enforces it. Furthermore the FSPHP mandates that physicians be evaluated at a “PHP-approved” facility. All of the medical directors of these facilities (which number around 20) are ASAM physicians “in recovery.” It is essentially self-referral.
A State Audit done in North Carolina found no oversight or regulation of the State PHP from either the state Medical Board or the Medical Society. In addition they found lack of due process for physicians and exposed the conflicts of interest between the PHP and the out of state treatment programs. They concluded abuse could occur but not be detected. It is the same scaffold present in Massachusetts.
The Medical Director and CEO of the North Carolina Physicians Health Program (NCPHP) Dr. Warren J. Pendergast, M.D. is the immediate past President of the Federation of State Physician Health Programs (FSPHP) and the audit findings of the NCPHP are standard operational procedure for other state programs fully infiltrated by the FSPHP.
The same infrastructure that exists in North Carolina and Massachusetts exists in other states. In this system there is absolutely no oversight from the medical board, the medical society, department of health or anyone else for that matter. They truly have removed all aspects of accountability.
PHS, inc. has been given cart blanche power in the assessment, treatment, monitoring, and disposition of all physicians referred to them.
The previous Medical Director of the Massachusetts PHP, Physicians Health Services, Inc. (PHS) for fourteen years (prior to Dr. Steve Adelman) , Dr. Luis Sanchez, is also a past President of the FSPHP.
And although PHS did not enter into formal partnership with the FSPHP until 2013, Sanchez and PHS Director of Operations Linda Bresnahan (who was interviewed for the recent Medscape article critical of PHPs) have both had long term involvement in the political hierarchy of the FSPHP and, in fact, helped develop the prototype for other states.
PHS, inc. exclusive use of out of state treatment programs has been challenged. In the past PHS, Inc. has adamantly refused to allow physicians to be evaluated in State despite it being one of the medical hubs of the country. Physicians in Massachusetts who are referred for evaluation in Kansas, Georgia, Alabama, and West Virginia as PHS has convinced the Board that only these facilities are ‘experienced in the assessment and treatment of health care professionals.”
In actual fact the medical directors of all of these preferred facilities are also ASAM physicians with the vast majority being in 12-step “recovery” themselves and close colleagues, if not friends of the medical directors of other state PHPs.
There is also documentary evidence that PHS, inc. is colluding with third parties (labs and treatment centers) to misrepresent test results and diagnoses in conspiracy to commit fraud. Documentation shows purposeful and intentional act to commit “confirmatory distortion” which is the deliberate misinterpretation or misrepresentation of facts to support a predetermined hypothesis.
Knight and Boyd note in “Ethical and Managerial Considerations Regarding State Physician Health Programs” “To further complicate matters, many evaluation/ treatment centers depend on state PHP referrals for their financial viability. Because of this, if, in its referral of a physician, the PHP highlights a physician as particularly problematic, the evaluation center might—whether consciously or otherwise— tailor its diagnoses and recommendations in a way that will support the PHP’s impression of that physician.
To consciously “tailor” a diagnosis or recommendation based on the PHPs impression of a physician is fraud.
Documentary evidence shows how PHS, inc. is engaging in fraud by colluding with a “PHP-approved” assessment center to fabricate and falsify neuropsychological tests to show “denial” and “relapse” with normal objective raw data being interpreted as abnormal. (again verified by a third-party oversight agency which resulted in the colluding party being forced to correct the results under threat of disciplinary action).
But without any regulation or meaningful oversight of PHS and no appeal process or avenue for the reporting or investigation for the physician, PHS has been able to get away with this misconduct with impunity and immunity. Complaints are either ignored, dismissed, or justified by sympathizers, apologists and a great deal of “willful ignorance.”
There should be zero tolerance for forensic fraud at all levels but when a person’s career, life and liberty are at stake and the perpetrator is in a position of power this conduct is particularly egregious. The damage done by a positive drug or alcohol test can be severe, far-reaching, and permanent. Intentionally and purposefully misrepresenting drug or alcohol tests by manipulation and fraud is unethical and needs to be addressed in real time. Those who engage in such behavior need to be held accountable for their actions.
For these reasons I petition Suzanne Bump to initiate a performance audit on PHS, inc. to detect fraud and abuse. There is currently no meaningful way to report, investigate, and hold accountable abuse of power in PHS, inc. Transparency, oversight, regulation, and accountability are essential.
The Physicians of the Commonwealth of Massachusetts deserve better than this.