

|September 24, 2015
R. Jeffrey Goldsmith, MD, DLFAPA, FASAM; Gary D. Carr, MD FAAFP, FASAM, DABAM
To the Editor:
We are writing on behalf of the American Society of Addiction Medicine (ASAM) regarding the Medscape 08/19/15 article “Physician Health Programs: More Harm than Good?” authored by Pauline Anderson. ASAM is a professional society representing more than 3,600 physicians and associated professionals dedicated to increasing access and improving the quality of addiction treatment. We have a robust body of policy statements supporting the role of physician health programs and an active Physician Health Committee, which includes current and past directors of state physician health programs (PHPs), as well as current past leadership of the Federation of State Physician Health Programs (FSPHP). ASAM believes this article does not fully represent the outstanding, professional, ethical and honest work done by our states’ PHPs.
This recent Medscape article reviews the complaints of several individuals who, in one fashion or other, have become dismayed with their state Physician Health Program (PHP). The article reviews their allegations in some depth and goes on to discuss investigations of PHPs in Michigan and North Carolina, with emphasis on the latter. The article reviews concerns over lack of due process, out of state treatment requirements, cost of treatment, “expensive contracts,” treatment center demands for payments, lack of PHP oversight, conflicts of interest, etc. All in all it presented a very disparaging view of state PHPs.
Physician Health Programs were created in the 1970s after an article featured the high numbers of suicides among Oregon physicians following licensure revocation for addictive illness. Both the AMA and the Federation of State Medical Boards (FSMB) called on individual states to develop programs to assist these physicians. Early PHP work involved addiction alone and later grew to include all psychiatric illness when PHPs identified significant psychiatric comorbidity among their addiction participants. Some PHPs with expertise and funding also assist with the “disruptive” or more accurately, the “distressed physician,” typically a physician in need of interpersonal coaching to improve communication. Others assist physicians who have engaged in sexual boundary violations and for whom there is an underlying, untreated psychiatric disorder at play.
The author failed to note the national study of PHPs called project Blue Print. This study revealed that nationally, PHP participants demonstrate a 78% success in recovery without relapse at an average of 7.2 years of monitoring. If we consider those who suffer a brief relapse and then enjoy success, that number exceeds 90%. The only other organization that shows that level of effectiveness is the airline industry, which, like medicine, employs safety sensitive professionals. These organizations have raised the bar for those treating addictive illness around the country. Is there a reason the author failed to even mention this?
The author communicates that those involved in a PHP have no due process. This is a mischaracterization. Before PHPs, physicians with these illnesses dealt directly with their state medical boards and were often disciplined merely for being ill. The PHPs have, in effect, been allowed to serve as a “buffer” to this system. The PHP offers the physician with potentially impairing illness an opportunity for a multidisciplinary evaluation at a choice of nationally recognized facilities. If treatment is indicated, they are given options for centers equipped to provide treatment. If they disagree with the evaluation, they are given the option of a second opinion evaluation. The PHP itself, with one exception, does not independently diagnose or treat. At any time — from the initial contact with the PHP and thereafter — the physician has the right to present their case directly to the state Medical Board. If they are being mistreated or unfairly diagnosed, they have complete due process with their Medical Board. PHPs do not exist to judge “guilt and innocence” or to determine what medical practice act statutes were violated. They exist to provide assistance and support to a physician who is ill and to support that physician’s restoration to wellness and a safe return to practice.
One of the author’s sources highlighted the North Carolina Audit — an exhaustive investigation. The Audit reviewed the NC program from stem to stern, including the details of over 100 cases. Their findings were released in April 14, 2015. There were NO instances of abuse by the program, misappropriations of funds or conflicts of interest identified by two subject experts employed by the State and independent of the PHP. The auditor made recommendations which the program has since instituted to protect itself and protect against even the appearance of impropriety. That’s it. To me, that feels pretty close to exoneration.
The author’s sources allege PHPs can be heavyhanded or demanding, “forcing” doctors into expensive out of state treatments, requiring
“expensive” contracts and the like. If you are a physician with addictive illness characterized by denial of that illness due to fear and shame, the process of evaluation and the introduction to treatment, when indicated, can feel intimidating. When a physician is afflicted with a potentially impairing illness, the privilege to practice medicine may be lost, in the absence of restorative treatment. While Medical Boards employ discipline to protect the public, PHPs offer an alternative to discipline. Namely, PHPs support physicians by directing them to evaluators and treatment programs with the requisite expertise to care for professionals in safety sensitive employment. Physicians, when they are patients, should not expect to dictate where, when and how their treatment will take place. Selfdiagnosis and selftreatment is uniformly discouraged in the medical profession. However, physicians may pursue second opinion consultations, just as patients in the general population are encouraged to do.
Once successfully treated, the physician engages in a contract with the PHP which entails careful monitoring of the health condition and accountability. In turn, the PHP can confidently advocate for the physician’s return to practice before their regulatory board, hospital credentialing bodies, malpractice carriers and others. Is it too much to ask that a physician recovering from illness be accountable to a PHP and in doing so, obviate the Medical Board’s need to discipline? If a doctor is going to take my daughter to surgery, I would appreciate the assurance that the doctor is safe to do so.
PHPs are highly effective. Were it otherwise, they would have ceased to exist years ago. Are they accountable? They are held to account every day by their state medical boards and professional associations, their state hospitals and the partners of every doctor they work with. A single incident of patient harm by a PHPmonitored doctor would result in public outrage, and in all likelihood fuel onesided, misleading articles like that produced by Ms. Anderson. There would be tremendous pressure on the medical boards to abandon the PHP model and start revoking licensure. That could easily happen. It would take us back to the licensure revocations observed in the 1970s, destroying the careers of physicians and denying the public access to an important resource, particularly at a time we are encountering physician shortages.
We submit, you will find no group of professionals in the country who have done more for physicians with potentially impairing illness than the state PHPs who comprise the FSPHP. They devote their careers to the task of assisting colleagues who, without their help, would certainly no longer be practicing medicine and in many instances would be dead of their disease. They are most often led by professionals who are devoted to helping those colleagues who are suffering and at risk for suicide. Day after day, they man the gate of help and hope and do all they can for the doctors who need them while fending off detractors, including organizations in favor of abolishing PHPs and shaming ill physicians through public discipline. In my view, the loss of PHPs and the safety they provide to physicians in crisis would do “More Harm than Good.” PHPs exist because they work. For every doctor the author interviewed to disparage their work, there are thousands who would attest to the benefit derived from their involvement with a PHP.
ASAM believes this article was not representative of the outstanding, professional, ethical and honest work done by our states PHPs. We, and all our patients, are fortunate to have them. Their success rate with complicated illnesses raises the bar for our entire field. They remind us that such success in treating these illnesses should not be the exception — it should be our expectation for all our patients.
Sincerely,
R. Jeffrey Goldsmith, MD, DLFAPA, FASAM
President, American Society of Addiction Medicine
Gary D. Carr, MD FAAFP, FASAM, DABAM Chair, ASAM Physician Health Committee
Cite this article: ASAM Responds to ‘Physician Health Programs: More Harm Than Good?’. Medscape. Sep 24, 2015.
And here is a suggestion. Instead of waving the usual tripe and rabble designed to obfuscate and deflect why don’t you simply answer the questions posed which are direct, simple and serious? Answer the questions posed. Why is that so hard?
@Dr. Michael Langan I hope this comment section does draw the thoughtful and open-minded reviews by the press, lawmakers, and the public of the “PHP-Blueprint”.
Cochrane-type review? Never happen! And re consensus as a type of validation of scientific thought…well, Socrates ran up against it, as did Copernicus, all those in Hitler’s concentration camps, Stalin’s gulags, etc. Scientific consensus as proof that the world is flat, is the center of the universe, that Jews can be discovered by the shape of their heads, and that the government must mold the attitudes of the public through the reparation of its psychiatrists into correct thinking (we could throw in Mao here, but I think I made my point).
PHP have harmed physicians. As you can see from these articles, many of them. The reasons these articles exist and have so much support is because of the outrage at the egregious experiences so many doctors, impaired and non-impaired, necessary and voluntary, have had with the current leadership at these programs. Physicians and others are outraged at PHPs harming physicians. If PHP operated efficiently and ethically, there would not be so many voices speaking out.
As an ASAM leader, you have responsibility to do an internal review of your diplomates. Read and review each physicians’ complaints serioulsy and with empathy. Stop dismissing the experiences of physicians- your own colleagues. These are very serious evidence of misconduct and coercion by your own diplomates here. If there wasn’t, PHP and ASAM wouldn’t be in the news.
I believe that PHPs have a purpose can be run ethically, but with the right leadership, rules, and auditing. Enforce a strict ban of financial conflicts of interest at the PHPs. Directors should be physicians with demonstrated commitment to ethics and personal rights.
What do you think of these steps for reform?
Dr Goldsmith,
I present a very simple and straightforward question and this necessitates a simple and straightforward answer. The ASAM frequently makes “public policy” statements that involve PHPs. In 2011 the ASAM put out a public policy statement regarding “coordination” among PHPs, regulatory agencies and assessment and treatment providers. One public policy statement the ASAM put forth was that regulatory agencies( I.e. Medical Boards ) only use “PHP-approved” centers in the assessment and treatment of doctors. Could you enlighten us to what objective qualitative criteria and quantitative measurements were used by your society and the FSPHP to “approve” these facilities? You must have a list of these facilities and what indicators were used in advocating them exclusively? To summarize these direct and not opened ended questions. 1. What qualitative criteria and quantitative measurements were used by the FSPHP in approving “PHP-approved” facilities? 2. Do you have a list of these facilities?
Please answer the question. If you cannot ( or will not) then please answer the following . What compels ASAM to make public policy statements limiting a doctor’s choice in assessment and treatment if they can’t even name the facilities or what the criteria are in choosing them?
@Dr. Michael Langan As documented by the NC Auditor, NCPHP had no criteria for the selection of its “preferred programs” to which a subject physician is “recommended” (under virtual bad order) to submit to, their compliance demanded under threat of immediate license suspension. (This is yet another reason why every state auditor needs to follow the NC Auditor’s lead and conduct a comprehensive Performance Audit of its PHP – every state is liable for the violations of these state-sanctioned programs!)
Further, I wrote FSPHP several years ago requesting such a list and its criteria for inclusion and my letter was not answered. And this is a professional Federation?
I wrote to NCPHP and requested their list. Not answered.
Shouldn’t it be of considerable concern that both a state and national program refuse to provide their “preferred program” list and the criteria for being designated such? Isn’t limiting the choice of one’s evaluation and treatment program to only select out-of-state cash only programs sort of a slap in the face to existing in-state resources who provide, under the watchful eye of insurance commissioners, health insurers and DHHS, top notch, compassionate MH and SA evaluation and treatment services?
What do you think these legitimate observers might think about coerced use of polygraph examinations? Use of SAMHSA contraindicated lab tests such as EtG? Of maximal sentencing to extended monitoring involving use of “preferred laboratories” and the protocol for such testing denied to the subject physician? Of no grievance mechanism for the captive patient?
@Dr. Kernan Manion @Dr. Michael Langan I too have asked the NCPHP for a list of those facilities to which they refer patients and was refused the list on the grounds that it might indicate favoritism among facilities. What??
@Dr. Michael Langan I agree that these are important questions and cry out for an answer. Why would Drs. Goldsmith and Carr, as well as many others, refuse to respond to such questions?
Dr Goldsmith,
Another few straightforward and simple questions. These simply require a yes or no answer. Many readers here might not be aware of the answers.
Is the ASAM or ABAM currently recognized by the American Board of Medical Specialties (ABMS)? Has it ever been.? Is “addiction medicine” a medical specialty or sub-specialty as defined by ABMS?
Does ABAM certification reflect knowledge, education and training in a given specialty as defined jointly by IOM. ACGME and ABMS?
Is ASAM a true “medical specialty” or a “Self Designated Practice Specialty”. (SDPS). – an AMA census term used to keep track of what any group of doctors are calling themselves at the moment such as the Society of Ringside Medicine or Society for Bloodless Surgery?
@Dr. Michael Langan I find your questions to be very sensible and well-reasoned, and to be questions which would be of significant interest to the readers. The responses are a simple yes or no, and should be readily answered by a knowledgeable individual.
Drs. Goldsmith and Carr, could you please answer the man’s questions?
“Physicians, when they are patients, should not expect to dictate where, when and how their treatment will take place.” Really? Why is it that patients, when they are patients, are allowed to do just that? Why is it that my now deceased son was not allowed to seek treatment, including inpatient care, at a local addiction treatment center even after his own private psychiatrist had approved such? What qualifies PHP approved treatment centers over centers such as the Harris House in St. Louis?
Additionally, the concept of “potentially impairing” illness is absurd. Aren’t all illnesses potentially impairing? And particulary mental illnesses?
The threat of loss of licensure has not changed with the institution of PHP’s. Instead, the net of “potenitally impairing” conditions has been cast ever wider. Where is the data that shows that the rate of physician suciide has been lowered with the institution of PHPs? How many physicians with “potentially impairing” illnesses, who are not, in fact impaired, are threatened with loss of licensure and livelihood?
How many physicians have died by suicide while being monitored by PHPs? Where is ASAM and the FSPHP at when it comes to collecting such basic data?
“PHPs wouldn’t be in existence if they didn’t work”? Really? The logic here escapes me. Work by what measure and by whose standard and for what purpose?
The reality is that the entire system is based on ideolgy rather than science.
Drs. Goldsmith and Carr:
Your letter to the editor in protest of the article “Physician Health Programs: More Harm Than Good?” decrying the one-sidedness and negativity of the findings and comments is as vacuous and laden with rosy generalization as FSPHP President Dr. Doris Gundersen’s, which itself drew nearly 200 comments.
Further, your letter insults the integrity of the author whose intent was simply to raise the question of whether there are problems with the PHP system as it is currently deployed. Hers was not intended to be another PR fluff piece like that done earlier in Medscape (see “How Impaired Physicians Can Be Helped” http://www.medscape.com/viewarticle/840112).
You noted that the vast majority of comments were negative. Well? Why didn’t those of the thousands you reference who have had such a favorable experience write in to share their story? Further, obviously not every PHP is of equal demerit. I would certainly hope that the majority have had some genuine successful intervention. But referencing a cluster of successes, no matter how large (and that is indeed unknown), doesn’t address the central issues – at all.
As you know, pharmaceutical trials can have stunningly miraculous cures and yet still be taken off the market. Why? Because the drugs may have killed or maimed the ones who weren’t fortunate enough to be the cures. The PHP program I believe ought to be looked at as a lot like a drug trial. And what we’re seeing in these responses is that a significant number of outcomes are disastrous!
Your letter entirely begs the questions at hand. There are profoundly important issues which have been raised, both within the body of the article and in the abundant responses detailing horrible cases of abuse: inappropriate compulsory referral to PHP by Medical Board; false portrayal of diagnostic evaluation as “peer review;” wrongful conduct of a binding forensic diagnostic psychiatric evaluation; wrong / fraudulent diagnosis; fraudulent assessment of degree of severity of illness; referral to only “preferred evaluation facilities;” inappropriate and abusive treatment; wrongful detention; denial of both due process and what might best be termed “medical due process;” utterly no recourse to grievance; draconian monitoring for diagnoses and illness severity not warranting such … the list goes on.
And yet, you address none of this.
Further, you, like Dr. Gundersen, parroted the same disinformation about the NC Audit report. It was in fact distinctly NOT an exoneration. And I will detail that for you in a separate comment.
I hope you will recognize that adopting the same self-pitying “victim” stance as Dr. Gundersen (as in people not recognizing how wonderful PHPs are [and surely must be as they are predominantly run by people in your professional society]) and broadly proclaiming the salvific work you and PHPs do and manifesting an attitude of how it is beyond reproach is not going to wash here either.
My hunch is that you, like Dr. Gundersen before, will simply refuse to engage in the dialog. Personally, I think that’s an unwise choice. But it would be entirely consistent with the avoidant behavior of this enterprise.
Let me be amongst the first in these responses to invite you (and Dr. Gundersen) into an open dialog, in a forum which will be AV recorded and made available publicly, in which several of us who have investigated these profound programatic abuses present our findings and provide you an opportunity to share your perspectives and planned organizational response. But I suspect that, like the invitations offered to Dr. Gundersen and Dr. Gaither in the related articles, you too will run from the invitation.
In doing so, I think you do your society and FSPHP and the entire PHP movement a great disservice.
Perhaps ASAM might like to have such a panel presentation at their next meeting? I’m confident I and my colleagues would be honored to participate. One caveat: it must be recorded.
I await your response.
The comments posted in response to a series of articles on Medscape about physician illness, PHPs, medical boards, etc. are tantamount to cyberbullying. It is not likely you will get responses to your questions when they are posted with such antagonism and sarcasm. Many of you have expressed your concern about physician suicide. Using social media in this fashion does nothing to stem the tide. Further, these comments are memorialized in time. Would you want your patients to observe you attacking other physicians this way? Rethink your approach.
Please give examples as what you write does not comport with what is writren. Asking yes/no questions and that specific and direct topics be addressed constitutes cyberbulliong? I think most readers and patients can see through that logical fallacy– especially by someone hiding behind initials.
@Dr. A M A number of us haven’t gotten any responses when multiple respectful and deferentially worded inquiries have been submitted directly to these agencies’ medical directors & PHP board chairs, medical board presidents, medical society presidents, FSPHP directors, an ASAM president …. I hope you will understand that the frustration from such non-response to multiple physicians’ inquiries, coupled as this has been with thorough denial of due process, no grievance mechanism for affected physicians and costly interruption of one’s career, is to be expected.
Further, I think it’s very important to distinguish confrontation from cyberbullying. Just because one is displeased with an assertive response does not constitute grounds to level the allegation of cyberbullying. In fact, making such an allegation could itself be seen as a veiled ad hominem attack which serves only to beg the important questions at hand and distract the reader.
Dr. AM, did you read the previous stories of physician desperation (and what amounts to false imprisonment and psychological torture occurring in certain programs) in the related articles? Do you REALLY think that responses like these are going to contribute to physician suicide? Really??? I suspect just the opposite. Physicians and other healthcare professionals wrongfully ensnared in PHP / Board Kafkaesque nightmares are likely to feel a sense of hope that this assaultive, unregulated and out-of-control program, operated under the protection of medical boards which decline to oversee it or respond to a deluge of complaints, is finally being confronted. Certainly that’s what I’ve heard from the over 30 physicians with whom I’ve spoken in the last several months.
Lastly, to the issue of my patients reading these responses – you bet! I’d love it! I’m hoping it’ll serve as an example of standing up and speaking your truth and demanding accountability.
@Dr. A M I am mystified by your accusation of ill will towards the comments. Clearly any bitterness or anguish you perceive on the part of prior commenters is secondary to real harm that these organizations have effected. Please list specifics so that Drs. Langan and Manion can respond with due process to your allegations. From what I have read, they have simply outlined with factual details the real or potential harms that PHP programs pose.
Dr. A.M.
Many of the docs who have posted commentary no longer have patients. My son certainly doesn’t. Many respondents are justifiably angry. Anger is an appropriate response to unfair treatment. I’m not certain what you perceive to be cyber bullying. The questions that have been raised, regardless of emotional tone, are legitimate ones, and demand answers. Labeling critics as cyber bullies does nothing to forward the conversation about these very important…and quite literally….life or death issues.
Some of us actually use are real names. Apparently we feel no shame in raising these serious questions. We quite earnestly would like answers.
@Dr. A M I disagree that asking questions amounts to cyberbullying. I have asked a simple and very straightforward question: How does one make a diagnosis of an illness in a patient who has none of the signs and symptoms of the illness and who does not meet the required diagnostic criteria for that illness?
This is to my mind a sensible, well-reasoned question that cries out for an answer. I have posed this question to the Medical Director and Clinical Director of the NCPHP; to the President of the NC Medical Board; to the Medical Director of the NCMB; the Executive Director of the NCMB; to Dr. Gunderson as President of FSPHP, and now to these two physicians. No one will answer the question and I suggest to you the reasons are obvious.
If you, as an ENT surgeon, had a patient with no symptoms and a benign biopsy and you performed radical cancer surgery on that patient, you might find yourself on the carpet before the Tissue Committee, the Operating Room Committee, the Medical Records Committee, the M & M Committee, the Chief of Surgery, the Medical Center Director, and on and on.
These people in the substance abuse field have no checks and balances; there are no committees and no one observing their work. As the NC State Auditor reported, the NC Medical Board and the NC Medical Society were not properly supervising the NCPHP.
To ask a simple question of how was a diagnosis made when the patient did not meet the diagnostic criteria is perfectly appropriate and cries out for an answer.
Dr. Langan, You are making my point for me. You characterize my observation as “logical fallacy” and accuse me of hiding behind initials. Moving on to more constructive, respectful discussions. Dr. M
What is your name Dr. A.M.? Knowing who you are might help us in moving on to constructive dialogue.
They are neither characterizations nor observations but simple statements of fact. The “tantamount to cyberbullying” statement is logical fallacy being used to disregard the specific, substantive and similar claims and you are hiding behind anonymity by using initials.
@ Dr A M On the contrary your three days of silence amidst dozens of thoughtful and intelligent comments is making Dr Langan’s case for him. Even under the mask of anonymity you have yet to contribute anything remotely resembling the “constructive” and “respectful” discussion on which you pontificate. You are undoubtedly part of this profiteering enterprise ( my guess is you either run one of the “PHP-approved” assessment and treatment centers or a “Like-minded doc.” Why? Pious rhetoric devoid of substance is pathognomonic of this group. They preach “professionalism” but haven’t an ounce; parade “evidence-base” bereft of evidence and proclaim pathology in others when in reality they are the sickest of the sick– predominantly narcissists and sociopaths. Bullies claiming they are being bullied is a shoe that fits them ( hence you) very well.
Where’s the beef?” There isn’t any. The emperor has no clothes and when “logical fallacy” doesn’t work and you are faced with the naked truth all you can do is crawl back under your rocks like feral cats. Why so quiet?? I’d be happy to participate in a constructive discussion with you but that ain’t gonna happen now is it? You have nothing to offer but smoke screens, digressions and moved goalposts. And by all means please engage.
Dear Drs. Goldsmith & Carr:
In your recent letter-to-the-editor, you reference the 2014 Audit of North Carolina’s PHP, and falsely state:
“There were NO instances of abuse by the program, misappropriations of funds or conflicts of interest identified by two subject experts employed by the State and independent of the PHP. That’s it. To me, that feels pretty close to exoneration.”
Let me correct you about the NCPHP Audit truly reported:
– The Program controls did not provide reasonable assurance that an abuse of authority would be prevented or timely detected if it occurred.
– The Program did not have objective, impartial due process procedures for physicians who disputed the Program’s evaluations and directives.
– The Medical Board did not conduct periodic evaluations of the Physicians Health Program to ensure compliance with state laws, written agreements, and best practices.
– The Medical Society did not use its appointees on the Program’s Board of Directors to provide adequate oversight of the Program’s operations.
The NC PHP Audit was far from exoneration!
You go on to argue that PHP’s have such a high success rate. According to the study you reference:
“At five year follow-up, 64% completed their contract, 631 78.7% physicians were licensed and working, 10.8% had their licenses revoked, 28 (3.5%) had voluntarily left medicine, and 30 (3.7%) had died (6 suicides).”
I’m not sure I would call this a huge success. Only 64% completed their contracts, some physicians decided to leave their careers and 30 patients died with at least 6 documented suicides!
Six physician suicides is tragic. PHP’s were meant to help address this problem and I’m sure that, overall, PHP’s have saved lives. PHP’s have also helped many people with serious problems, and I want to make clear that I recognize and acknowledge that fact.
However, state medical boards and PHP’s have also hurt the physician suicide cause. I have to argue that any disciplinary action for a mental health condition has and will continue to discourage physicians from seeking help.
I understand there is a tricky balance between protecting the public and allowing a physician to practice, but both the boards and PHP’s have swung so far towards always doing the legally safe/protect the public that physicians are not being treated fairly, and sometimes even punished and taken out of practice even though they are innocent and not impaired.
As part of the 2014 Gallup-Healthways Well-Being Index survey, 17.5% of Americans and 10.5% of physicians reported having been diagnosed with depression at some point in their lifetime; and 10.4% of Americans and 5.7% of physicians currently have depression or are being treated for it.
There are currently over 900,000 licensed physicians currently practicing in our country. At least 50,000 of us have been diagnosed with a mental health condition at some point in our lives.
When you and the President of the FSPHP use language like “potentially impairing condition,” I become very concerned about what would happen if those 50,000+ physicians in our country were referred to a PHP for evaluation. How many of these physicians would be required to undergo a $5000 5-day inpatient evaluation?
The road could become very slippery if there isn’t a system of checks and balances, independent oversight, transparency, legal due process, etc. that demands and ensures that no physician is ever harmed in any way by a PHP; and if there is harm done then there should be legal consequences.
You submit that:
“no group of professionals in the country have done more for physicians with potentially impairing illness than the state PHPs who comprise the FSPHP. They devote their careers to the task of assisting colleagues who, without their help, would certainly no longer be practicing medicine and in many instances would be dead of their disease. They are most often led by professionals who are devoted to helping those colleagues who are suffering and at risk for suicide.”
Yet there is no evidence to support this. PHP’s and the FSPHP were formed and exist to treat physicians who have severe addiction problems. Even your BluePrint project study was based on addiction patients.
But now, it seems, you are attempting to expand your role in protecting the public from “potentially impairing illness,” which is a far cry from severe disabling addiction problems. I would argue my PCP and, perhaps, confidential treatment by a psychiatrist or therapist/counselor would do more to help me and my colleagues who are suffering than you and your coercive task force.
I also think it is quite clear that Pamela Wible, M.D. has been, and continues to be, the true leader confronting physician suicide. And her comments suggest she also has reservations about the suggested expanded role of PHP’s to include “potentially impairing illnesses.”
@Dr. P J This is very concerning! “potentially impairing illnesses”! that is Orwellian, just that—double-talk. Let’s keep them rehabs churning! the PIP=Potentially Impaired Physician”! Man, what a concept!
PHPs detecting physicians potentially impaired…what a concept! brilliant! gotta round ’em up before they hurt someone!
The “PHP-blueprint” with links
@Dr. Michael Langan Truly troubling. Thanks for your astute research. Readers might find it helpful to know that Dr. Langan’s site contains an extensive history of the PHP movement and its unexamined susceptibility to profiteering and corruption.
As you point out, the “blueprint” which fuels this pseudo-authoritative program posing as a legitimate medical organization, operating with no oversight or accountability, is liable to spread to cover every professional who requires licensure by some board, and in fact, to every EAP (Employee Assistance Program) whose counseling services are offered as a “benefit” to its naive employees. The corporate EAPs will be particularly susceptible to lucrative buy-in.
This elaborate program, with its pre-arranged “preferred programs and facilities” and “preferred labs” and “preferred therapists” in the community and “preferred lawyers who understand how we work” and “preferred re-education programs” for docs who were alleged to have mis-prescribed will result in an exponential rise in referrals to its lucrative pipeline. And, as we’ve learned from physicians in NC, MA, WA, FL, MI, MO and many other state PHPs, once you’re in the system, your career is essentially over.
PHPs – renamed “PROFESSIONALS Health Programs” – will be presented to other boards throughout the country as “the authoritative medical approach” using their non-peer reviewed studies and will be capable of being used to derail any professional’s career. Internal whistleblowers, independent thinkers, competitors within an industry – no problem. Send them to your PHP on trumped up and unsubstantiated allegations, submit your complaint anonymously so there’s no tracing it, and that professional’s career is done. Spouses, aggrieved clients – want to end a professional’s career? Simply make an anonymous allegation and the professional’s licensing board happily refers the subject professional to the PHP. Done. Clean. No need for messy divorce or lawsuits; better, you’ll avoid the due process and laws of civil procedure that are required in that forum.
That’s the exceedingly dangerous power of these programs which currently operate with utterly no oversight or accountability. They have become a Frankenstein created in the labs of medical boards and medical societies, neither of which now wants to take ownership. (And understandably so – the liability for each state and medical society is immense! (See class action lawsuit in MI: http://www.chapmanlawgroup.com/hprp-class-action/ In that suit, members of the MI medical board and its PHP are jointly named. The alleged violations include denial of due process, unlawful restriction of civil liberties and conspiracy by both agencies to orchestrate these violations. Defendants are named in the profession and personal capacities.)
If the reader has any doubts about the reality of the highly lucrative private evaluation and treatment referral pipeline, you might wish to see the documentary “The Business of Recovery.” (http://www.thebusinessofrecovery.com)
I encourage all to write to the APA and AMA and to your state auditor and medical society to immediately open investigations into these dangerously powerful unsupervised pseudo-psychiatric programs.
You would also benefit from seeing Dr. Susan Haney’s excellent presentation to the AMA House of Delegates on concerns about the potential for corruption in the PHP program against the backdrop of the explosive growth of the specialized “Addictions Treatment Programs Designed Especially for Physicians.” Dr. Haney was definitely ahead of the curve in exposing this. (http://www.osmapandtheforum.org/upload/Oregon11.pdf)
Goldsmith’s claim that NC PHP is pure as wind driven snow is unfortunately not so. First, I saw it myself. I saw what the NC Medical Board posted on a physician, and then took it down because it was untrue. Furthermore I am aware of a murder which can be tied securely to the NCMB’s lawyer driven apparatus which took a medical license abruptly leading to a solid case of abandonment. And I have a witness to this murder as I now know what happened to the patient’s family; they attend my church. Lastly, I know of a pharmacist who was railroaded. too. Seondly, When the NC Med Board forced the pharmacist to undergo care AFTER the theft of pills was pinned to the pharmacist’s pharm tech and he was jailed and is now doing time, Why did the board not forgive her original sentence? Lastly, Goldsmith can’t read. The NC auditor’s report forced changes.
Dear Drs. Goldsmith and Carr:
(PART ONE)
Thank you for taking a position on this important subject matter. I wish to raise some objections to your defense of PHP’s.
In your first paragraph, you characterize the American Society of Addiction Medicine as a professional society of 3600 physicians and others devoted to improving addiction treatment. However, you do not mention that Addiction Medicine is a self-designated medical specialty with barriers to entry that are qualitatively lower than those of any of the ABMS specialties. The thrust of mentioning this observation is that your claim to a specialized fund of knowledge can be reasonably questioned while I am willing to stipulate that you have issues about which you advocate passionately. My concern is about your dual roles in both advocating for your viewpoints and enjoying the authority to enforce your perspectives on fellow physicians through your operation of PHP’s.
In your second paragraph, I draw the conclusion that you know you have received criticism in the public domain about the operation of state PHP’s from licensed professionals.
In your third paragraph, you relate your version of the history of physician health programs. Without challenging your view of the salient factors leading to the emergence of PHP’s, it is important to note that the context in which PHP’s operate has changed substantially from that present when they first appeared on the scene. The stringency of state medical board actions, the coordination of state medical board actions, the Healthcare Quality Improvement Act of 1986, the Americans with Disability Act of 1990, the wholesale corporate transformation of American medicine, the dilution of the concept of professionalism as applied to physicians, and the JCAHO invention of the category, “disruptive physician” have all had a role in changing the impacts of PHP’s, however well-intentioned they may have once been.
In your fourth paragraph, you point out the failure of PHP’s critics on Medscape to acknowledge the contributions of the Blueprint Project. In fact, when I query the NLM and NCBI databases for a study by that name, I am unable find anything. I did find a 2012 article written by authors at Colorado’s Physician Health Program that referred to the existence of a Blueprint Project and concluded that Colorado’s performance was in line with US norms. I cannot find evidence that the Blueprint Project is widely-cited by anyone who does not work for a PHP. The only impression I had of the CPHP paper was of the small sample size and systematic methodological biases of this study reporting the performance of a program that has intersected with thousands of Colorado physicians (based on estimates from their case numbering system). Their claims about low recidivism rates are difficult to interpret without access to information about actual return to clinical practice, continued presence in Colorado, retirement, or even survival of these “treated” physicians. Moreover, I note the conspicuous absence of a credible reference population of physicians. Sinclair Lewis, in Arrowsmith, described this as fallacious “post hoc, propter hoc” reasoning.
(Continued)
(Part Two)
The fifth paragraph is replete with unsupportable assertions. The first is about “due process” afforded by these programs. I can only mention counter-examples that have emerged from my observations in Colorado. Physicians who self-refer to Colorado’s program (about 80-90% of participants) are encouraged in this action by CPHP’s assurances that they will be helped. The concept of “due process” is as relevant to most of these physicians as it may be to patients seeking medical care. “Process” is not the issue at all. Rather it is an improved outcome. However, if the idea of due process is extended to include “dual agency”, there is quite a lot about which to object. Karen McGovern, the program director of the Colorado Medical Board since 2013, trained as a nurse and a lawyer, stated under oath on September 23, 2015 in Denver County Court, that Colorado’s PHP was a “treatment provider”. Colorado’s PHP will refer physicians to lists of attorneys, psychologists, and psychiatrists with whom they prefer their clients work. CPHP records contain diagnoses, treatment recommendations, professional referrals, and fitness for duty recommendations. HIPAA waivers about release of medical information are sought and archived. However, CPHP enjoys a unique status in Colorado medicine in maintaining an ambiguous status as a treatment provider and a forensic evaluator. Every other type of forensic medical evaluation in Colorado proceeds ONLY after execution of an acknowledgement by the examinee or his guardian of the forensic nature of the medical encounter and the absence of a doctor-patient relationship. Such an acknowledgement has never been a component of CPHP’s enrollment paperwork. After years of CPHP participation, I asked a physician employed at the program whether we had a “doctor-patient relationship”. The answer was an emphatic, “No!” At that point, I mentioned never having been asked to acknowledge that understanding with CPHP, and, as a physician who does fitness for duty evaluations as part of my job, that I considered such a practice to be a boundary violation and in direct conflict with the published and enforceable description of the doctor-patient relationship contained in the Colorado Medical Practice Act under “Board Policies”. On September 4, 2015, I received 90 minutes’ notice of summary suspension of my license because I was no longer participating with CPHP. When I undertook extraordinary efforts to get a post-suspension hearing, I asked CPHP representatives to testify for me OR the Colorado Medical Board as to whether I had stopped participation with CPHP, they declined to testify about their assertions to the Colorado Medical Board. Despite this, the medical board did not lift the suspension and would not say why. I can provide many more examples of the absence of anything resembling “due process” or even basic forthrightness in dealing with CPHP, but in the interest of space, I will rest on the presentation of this one glaring counter-example. Moreover, the alternative of directly presenting medical fitness for duty evidence to the Colorado Medical Board does not exist. That statement is completely untrue. Also, the statement that CPHP takes no position on whether some activity constitutes “medical practice” is unfounded. This is a legal matter that CPHP enforces and they use their own definitions. From my experience, CPHP will extend its definition of impermissible medical practice to what amounts to “thought crimes” in its efforts to keep ill and/or sanctioned physicians from supporting their families. CPHP does make use of out-of-state physician treatment facilities, primarily in Kansas, which are enormously expensive and disruptive when a physician is at his most vulnerable and which have a proclivity to employ pseudo-scientific interventions such as polygraphy, group confrontation sessions, and all manner of “12-steppery”. The assertion that medical boards afford physicians due process is complete nonsense. They do their work relying almost exclusively on hearsay evidence and their internal processes are obscured from scrutiny by the dual barriers of “peer review privilege’ and “deliberative process”. In fact, in Colorado, it is not discoverable under CORA requests (Colorado’s version of FOIA) how members of the Colorado board are nominated, vetted, appointed, or reviewed. Apart from the State Auditor, whose office has broad powers to review state agency performance, one cannot discern to whom the Colorado Medical Board is accountable in state government. Also, the Colorado PHP is not independent of the State of Colorado. Its activities are supported by physician licensing surcharges and to a lesser extent by some charitable donations.
(Continued)
(Part Three)
The fifth paragraph of the Goldsmith-Carr rebuttal created the impression that PHP’s provide a rehabilitative function. I contend that the only evidence for such a claim is based on tautology rather than data. I asked that DORA, the Colorado state agency that contain the Colorado Medical Board, has any evidence for its agency claims that Colorado is a “rehabilitation state” in regards physician discipline. I made the inquiry under the authority granted to every Colorado citizen by the Colorado Open Records Act or “CORA”. Here is the test of the response to my official inquiry made to the Colorado Medical Board:
“We are receipt of your August 5, 2015 request, purusant to the Colorado Open Records Act, to provide “[a]ny information compiled by the Division of Registrations that tabulates, quantifies, or analyzes the impact of Colorado Medical Board investigations, sanctions, and other potentially-adverse Board actions on the safety of physicians in practice, on the rate of return to work or “successful rehabilitation” among these physicians, and on the rates of practice closure, early retirement, bankruptcy, and adverse health consequences.”
Upon review of Division records, we have no records responsive to your request.
However, we do have in our possession a report authored by the Center for Personalized Education for Physicians (“CPEP”). This report was based by data tabulated/compiled by CPEP and was not commissioned or endorsed by the Division or the Medical Board. Notwithstanding, the report does address recidivism rates for physicians engaging in the CPEP educational evlauation and program and is therefore being produced.”
The sixth paragraph makes the claim that the North Carolina state auditor “exonerated” North Carolina’s PHP. This is a gross mis-characterization of the state auditor’s findings and scope of its authority to exonerate.
The seventh paragraph makes the assertion that PHP’s exist to perform the delegated function from medical boards of protecting the public from unsafe physicians. As I pointed out above, in Colorado, the home to Doris Gundersen, MD, President of the Federation of State Physician Health Programs, no data exist to support the assertion of any positive public health or safety benefits.
The eighth paragraph asserts that PHP’s exist to “confidently adocate” for a physician’s return to practice when appropriate. Where are the data to support this assertion? Is this another tautology? Who, in fact, has been kept from harm at the hands of these “impaired” or disruptive” physicians?
The ninth paragraph advances the argument that since PHP’s continue to exist, they must effective. That statement would seem more appropriate in a work of satire. How many state and Federal corporate and agricultural subsidy programs continue to exist in the absence of any evidence of their continued usefulness to the general public? The other part of this paragraph makes the claim to the existence of a false dichotomy by saying abolition of the state PHP’s would re-institute a Draconian “reign of error” by state medical boards. That may be true but in the search for a leper with the most digits, why is it not an option to consider the eradication of leprosy?
The tenth and eleventh paragraphs basically present no new assertions or arguments.
My claim is that Colorado’s PHP is one of the planet’s last vestiges of “Soviet-era psychiatry” and operates outside the constraints of the Colorado Medical Practice Act. It does much more harm than good and is answerable to no one. The claim that the CPHP may be better than the Colorado Medical Board might be true. But it is also faint praise.
In considering both sides of this very polarized debate, I feel it is important to state two facts upon which I think both sides could agree:
1. Physicians in distress do require help – highly skilled, compassionate, and evidence-based medical and psychological care. They also require help that is tailored to their individual needs.
2. PHP’s, while perhaps originally intended for this purpose, have developed in such a way that, too often, they overlook individual needs and serve more as policing bodies than health care services.
I am all too aware of PHP’s that treat almost every physician under the same guidelines/restrictions regardless of diagnosis and of the reasons the physician entered the contract to begin with (even if a physician entered the contract voluntarily).
So perhaps we could collaborate to design a type of PHP that brings us back to the original purpose? I would be excited for the opportunity to be part of such a project.
@Dr. Justine Dembo Thank you for your refreshing proposal. I so wish these programs – individual state PHPs, state medical boards, FSPHP, ASAM and APA – would be open to collaborative dialog and interested in constructing a truly fair, ethical and compassionate PHP system. Sadly, they are not. Even as witnessed i these two letters to the editor from FSPHP President Dr. Gundersen and ASAM President and Medical Director Goldsmith and Carr. In the presence of such an outcry, and the resounding silence of these organizations response to concerns raised, one gets the sense that they are not only not interested in collaborating, they are invested in concealing the illegal workings of their programs.
This is clearly counter to the spirit of medical transparency as well as medical professionalism.
I think it is fair to say that, if any physician is even contemplating voluntarily going to a PHP presuming its provision of benevolent tailored mental health care services, they really ought to reconsider.
@Dr. Justine Dembo I believe that PHPs have a purpose can be run ethically, but with the right leadership, rules, and auditing. Enforce a strict ban of financial conflicts of interest at the PHPs.
Directors should be physicians with demonstrated commitment to ethics and personal rights.
These articles are calls for responsibility and and reform. There are ethical ex-PHP doctors in every state,such as Dr.Boyd in MA, who can provide leadership for PHPs to get back to their intended purpose. Such a project would indeed be worthwhile and a great service to physicians and patients alike.
The consequences of action by the Colorado Medical Board and the Physicians Health Program:
https://www.linkedin.com/pulse/state-colorado-closed-mountain-west-workers-free-horiagon-md-mocch
The Medical Board working as tools of Colorado corporations and insurers is indefensible. This action is in the interest of a very few and not the general public.
With all due respect to Drs. Goldsmith and Carr, I find their response to be little more than a generalized fluff piece that really addresses nothing. In my opinion, their response is full of distortions, untrue statements, and attempts at justification.
Since I am one of those “individuals who, in one fashion or other, have become dismayed with their state Physician Health Program (PHP)” and am one of the individuals named in the original article, I want to make a lengthy response to Drs. Goldsmith and Carr.
Let me note that I filed an extensive ethical complaint of some twenty pages against a member of ASAM, and I filed the complaint with the then-President of ASAM. In due course, I received a response stating that in fact ASAM had no Code of Ethics, despite the fact that I had referenced by number in my complaint each of the specific ASAM ethical codes I believed had been violated. I informed the President of ASAM that in fact his organization did have a Code of Ethics and directed him to the Code of Ethics on the Internet. He thanked me for pointing out that his organization did have an ethical code and for directing him to that Code, but stated that these were only suggestions and were not enforceable by ASAM. Unbelievable. The President of ASAM doesn’t know that his organization has a Code of Ethics! It would suggest that the Code of Ethics didn’t get used much.
I want to make clear to Drs. Goldsmith and Carr why others and I became “dismayed” with the state PHP. The NCPHP was not vetting anonymous complaints in the least. One physician was accused of smelling of alcohol at work in the hospital, and of being late to work, not answering pages, and other such complaints. I personally vetted that complaint by going to the hospital where that physician was employed and talked with his colleagues, his treatment team, his physician supervisor, the social worker with whom he worked daily, the human resources office and others. I found that ALL allegations against this physician were NOT TRUE. When I tried to discuss my findings with NCPHP personnel, the Medical Director and Clinical Director refused to talk to me even though I had a power of attorney from the physician. I made clear that I thought each and every allegation was a sham and was untrue.
The physician was referred by the NCPHP to a center “equipped to provide treatment”, as Drs. Goldsmith and Carr characterize such facilities in their response. At that “center equipped to provide treatment”, the physician patient was allegedly told three times by the substance abuse specialist that he did not meet the diagnostic standards for even alcohol abuse. The substance abuse specialist wondered why NCPHP had even sent the patient to the facility as he did not meet the diagnostic standards for even alcohol abuse. A complete battery of psychological testing over seven hours showed that the patient had no anxiety, no depression, no organic changes to the brain, and that he was of superior intelligence. The physical examination reported in the medical record allegedly did not take place, according to the physician patient; the physical examination notes “no marks or scars” and yet the patient had had abdominal surgery and a total hip replacement.
However, this patient was told at the exit interview that he would not be cleared with the NC Medical Board to return to practice and that he must be hospitalized. He left and returned to North Carolina.
I attempted to speak with the Medical Director of the facility at which the physician patient had been evaluated. I telephoned seven times and sent a certified, return receipt requested letter requesting an appointment with her. She refused the letter and it came back to me unopened. Anytime the Medical Director of a facility refuses to speak with a legitimate person with proper releases about how a diagnosis was made, one must immediately begin to smell a rat.
The physician in question went for a second opinion, but this was only after the NCPHP Medical Director contacted the facility with information concerning the first evaluation. So much for a fair, competent, ethical evaluation. The psychiatrist at the second facility noted that the patient did not meet the diagnostic criteria for alcohol abuse, and that the physician had been accused by an anonymous person and thus could not be questioned. The diagnosis at the second facility? Alcohol abuse, and the patient needed outpatient monitoring for ten years. Unbelievable!
Again, under the authority of a durable power of attorney, I attempted to speak with the Medical Director and Clinical Director of the NCPHP about my concerns. They refused to respond to me, and in fact noted in the NCPHP record that they had made a decision not to talk with me. It is not clear on what basis they would not talk with me when I had every legal right to talk with them. I did send them letters stating that in my opinion all of this was a sham, was fraud, was medically unsupportable, and was highly unethical.
The physician patient was seen by a private practice addiction psychiatrist for another opinion. This practitioner had been on the NCPHP Board of Directors, and had evaluated and treated patients for the NCPHP. This practitioner told me in writing that the physician patient did not meet the diagnostic standards for alcohol abuse, but that one could nonetheless make the diagnosis. He declined to tell me how one does that. In my opinion, this is nothing more than gross incompetence, fraud, theft, fails to meet the standard of care and is malpractice.
I hope Drs. Goldsmith and Carr are beginning to see why some physicians become “dismayed with their state PHP”. Can anyone even imagine such nonsense happening at Duke Hospital, at the University of North Carolina Hospital, or other such facilities?
Drs. Goldsmith and Carr state, “the author communicates that those involved in a PHP have no due process. This is a mischaracterization”. This statement by Goldsmith and Carr is absolutely untrue and is a blatant misrepresentation. The NC State Auditor noted at length that there was no due process at the NCPHP and gave three very specific and detailed reasons why there was no due process. Further, the Auditor noted that due process was specifically required by NC State Statutes and by the contract between the NC Medical Board and the NCPHP. Thus, the NCPHP had been practicing in violation of existing law.
Goldsmith and Carr note that the Auditor reviewed the details of over 100 cases at the NCPHP and found no incidents of abuse. This is totally misleading and incorrect as stated. The fact is that at the time of the audit the physician patients were not able to obtain a copy of their own records and had no idea of what was in their record. Now that physician patients are able to finally get a copy of their NCPHP record, they are finding all sorts of untrue statements, distortions, hearsay presented as fact, and misleading innuendo located in their records. To a surveyor or consultant, the record might appear satisfactory if one did not recognize the untruths, distortions, innuendo, and hearsay presented as fact in the record.
Goldsmith and Carr state that the Auditor found no evidence of “abuse” by the NCPHP. This again is incorrect, misleading, and untrue. What the Auditor actually found is “The audit found no indications of abuse by the Program; however, abuse could occur and not be detected because the Program lacks objective, impartial due process procedures for physicians who dispute its evaluations and directives”.
The Auditor also found “Abuse could occur and not be detected because the Program gave the CEO/Medical Director and the Clinical Director excessive influence over the process of reviewing physician complaints, and physicians were not allowed to effectively represent themselves when disputing evaluations”. “Abuse could occur and not be detected because the North Carolina Medical Board did not periodically evaluate the Program, and the NC Medical Society did not provide adequate oversight”. Thus, Goldsmith and Carr have totally misrepresented what the Auditor stated.
Goldsmith and Carr state, “if you are a physician with addictive illness characterized by denial of that illness….”. Goldsmith and Carr seem to be missing the point and avoiding that what is being discussed are persons who do not have the illness with which they have been diagnosed. These people do not have “addictive illness” in the least and yet are being diagnosed with such.
Goldsmith and Carr note, “Physicians, when they are the patient, should not expect to dictate where, when and how their treatment will take place. Self-diagnosis and self-treatment is uniformly discouraged in the medical profession.” The reality is that physicians are not uninformed, uneducated people and they can readily discern when they have been misdiagnosed and are being given a diagnosis for which they do not meet the diagnostic criteria. In other words, they can usually detect a scam.
Goldsmith and Carr state, “physicians may pursue second opinion consultations, just as patients in the general population are encouraged to do”. This is totally misleading as stated, because the physician patient must go to one of the PHP approved facilities for a second opinion, and only after the personnel from the PHP have contacted the second facility privately and given that facility information that may or may not be true. This is not a legitimate second opinion consultation, but is instead a stacked deck. It would be interesting to study how often a second opinion consultation from the PHP differs in diagnosis from the original diagnosis.
I would like for Goldsmith and Carr to respond to one simple question: How do you make a diagnosis of a condition in a patient when the patient does not have any of the required symptoms or required diagnostic criteria for that diagnosis? I have posed that question to personnel at the NCPHP, at the NCMB, to Dr. Gundersen and others and no one can or will respond. Drs. Goldsmith and Carr, please respond to the question.
I have been practicing medicine for 52 years in academia, in the military, and in other venues, and I have never seen anything as bad as I have seen the PHP system to be. I firmly believe that the American Medical Association, the American College of Surgeons, the American College of Physicians, the American Psychiatric Association and other groups must come together and investigate the alleged abuses and severe shortcomings of the PHPs.
I ask Drs. Goldsmith and Carr to provide a reference for “the national study of PHPs called Project Blue Print” and for any other peer-reviewed, indexed, controlled study that shows the efficacy of PHPs.
Many physician respondents to Dr. Gundersen’s reply have asked Dr. Gundersen, as President of the FSPHP, for this information and she declined to provide such.
Please post the references to all of these documents so that we can all read the studies, study the design, and contemplate the conclusions reached.
In discussing the NC State Auditor’s findings, Goldsmith and Carr state “the auditor made recommendations which the program has since instituted to protect itself and protect against even the appearance of impropriety”. Really? I ask Dr. Goldsmith and Carr to be more specific and tell the readership exactly what the NCPHP has done to “protect itself and protect against even the appearance of impropriety”. What about protecting the patient? Has anything been done to provide due process for the patient, to ensure diagnostic accuracy of the patient, to provide the complete NCPHP medical record to the patient, and to vet anonymous complaints received about a physician?
@Dr. Jesse Cavenar Indeed, the wording of their response is most curious. “… protect itself and protect against even the appearance of impropriety.” What is it “protecting itself” from? Further scrutiny? And protecting oneself against the appearance of wrongdoing says nothing about ensuring that no wrongdoing will occur. Rather, it simply conveys that one is more interested in further concealing the wrongdoing.
Indeed, where is ASAM’s concern about the physician patient subjected to these abuses? I hear none! Where is there a response from Drs. Carr and Goldsmith and from Dr. Gundersen an expression of concern about the abuses that are occurring and a public resolve to investigate? Nowhere. Not one ounce of concern. It’s al about protecting the program.
Even after the NC Auditor found that NCPHP had grossly violated the due process rights of over 1,140 physicians over the preceding 10 years by denying them access to their evaluations (which NCPHP was creatively terming “peer review”)(see NC Auditors report on NCPHP: http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf), persons affiliated with NCPHP and NCMB went behind the scenes and introduced legislation which attempted to remove existing due process protections in the current law. (see http://www.ncleg.net/Applications/BillLookUp/LoadBillDocument.aspx?SessionCode=2015&DocNum=4019&SeqNum=0)(or see NCLeg: H543-PCS40415-SV-15 – see p4, line 27; the alternately proposed provisions are not a reasonable substitute for due process.)
Now, it appears, NCPHP has attempted to change its identity as a healthcare entity by eliminating its medical director position. How can a state-sanctioned psychiatric “fitness for duty” evaluation program in service to a state licensing board not have a medical director?
I must be missing something here. Why should any physician comply with an order to submit to a “mental evaluation” (as NC’s version of the Medical Practice Act refers to it) by a) personnel of an “educational public charity” which b) carries no malpractice insurance; c) has no specifications for the professional qualifications of its evaluators; d) has utterly no internal or external quality assurance program; e) has no effective oversight or accountability; f) persists in denying one due process; and g) whose actions and decisions the medical board still treats as infallible and incontestable? You’d have to be stark raving mad to submit to such a program! And even then, and perhaps especially then, you STILL shouldn’t go.
I have been concerned about the NCPHP allegedly ordering polygraph or “lie detector” examinations for certain patients. It is my understanding that the American Medical Association has declared polygraphic data to be junk science and has stated that polygraphs have no place in the practice of medicine.
I wrote to the President of the NC Medical Board asking for the official position of the NCMB regarding polygraph examinations for physician patients. There has been no response to my question.
In my opinion, if the allegations of ordered polygraph examinations are correct, it is very ill-advised for the NCPHP to subject physician patients to polygraph examinations in an attempt to make a diagnosis.
Drs. Goldsmith and Carr, what is the ASAM position on polygraphic examinations?
@Dr. Jesse Cavenar Polygraphs are often used in these evaluations to support the misused and overused concept of “denial.” These unscientific instruments are also used inappropriately to support “recovery” and recover the medical licenses of those they support (who interestingly often ending up working for the PHP and its associated drug and alcohol testing, assessment and treatment industry complex. Michael Ramirez, MS is on the Board of Directors of the FSPHP, the Western Regional Directors of the FSPHP and the clinical coordinator of the Montana PHP (the Montana Professionals Assistance Program). It is worth reading the Board Order below for Dr. James Peak who was convicted of child pornography in 2011 yet (unlike those writing here) had his license reinstated in no time at all thanks to Ramirez and the Montana PHP. The quote below reveals just how far off the tracks this current group is.
“Following his interview, Peak voluntarily surrendered his medical license, notified the hospital and clinic, and immediately entered and successfully completed a 90-day inpatient treatment program in Texas. While in treatment, Peak passed a polygraph examination confirming that he had not engaged in any hands-on conduct with children. Within a day of his return, Peak enrolled in sexual offender treatment in Billings, and is currently attending regular AA and Sex Addicts Anonymous meetings.”
I am curious as to how one qualifies to become a member of ASAM.
It is my understanding that the only way to have American Board of Medical Specialities certification in treating addictive illness is by qualifying for a subspecialty in Addiction Psychiatry under the American Board of Psychiatry and Neurology. How many of the 3600 ASAM members hold such a certification?
I am also curious if all (or any, for that matter) PHP preferred facilities are headed by physicians who hold such subspecialty certification.
Need investigative reporters. Anyone advocating the current system is making money off it including Dr Carr who is current medical director of a “PHP -approved” assessment and treatment center. He is in fact a so called “triple threat”and belongs to ASAM, FSPHP and Like-minded docs. Could you please identify the ideology behind Like-minded docs Dr.Carr? It appears, like yourself,the Medical directors of all the “PHP-approved are on this list. Friends referring to friends. How convenient and profitable.
Also don’t you run a 50 acre “sober house” with a 3 month minimum somewhere in Tennessee ? How’s the “diagnosis tailoring?”
Looking for an Investigative Reporter to Question MRO—-Procedural, Ethical and Legal Justification Needed
How about defending this MRO? He’s no different than Fata the MI doctor who fold patients without cancer they had cancer so he could treat them and make money.
Like most of the doctors found in this system he “reinvented” himself by getting “board certified”in “addiction medicine.” This is just a diploma mill for for people like Gavryck, Skipper, Tietelbaum and others to provide a “clean slate” and perceived expertise. ABAM certification is a joke – they are laughing all the way to the offshore banks.
https://www.linkedin.com/pulse/looking-investigative-reporter-question-ethical-legal-langan-m-d–1
@Dr. Eliza Blackwell Hello Dr. Langon – why do you find it necessary to present your views under a pseudonym – especially when you criticize other physicians for hiding under initials? People in glass houses should not throw stones.
Goldsmith and Carr. I am going to assume your doctoral thesis had WAY MORE FACTS than your rebuttal….. or you wouldn’t have graduated.
Medscape Article Critical of Physician Health Programs (PHPs): An Important Milestone in Exposing Abuse and Injustice
https://www.linkedin.com/pulse/medscape-article-critical-physician-health-programs-langan-m-d-
“The ASAM / FSPHP Blueprint” Part 1
Drs Goldsmith and Carr:
You raise the issue of the PHP “blueprint.”
As I review the documents which Dr. Langan directs to in an earlier post (http://disruptedphysician.com/tag/php-blueprint/), PHPs’ grand “blueprint” would attempt to position PHPs as the definitive “impaired professionals” program while posing as a legitimate medical / psychiatric organization providing assessment and referral. (Even this is inherently contradictory as PHPs deny that they conduct diagnostic assessments! How can this be if they are using clinicians’ professional training to ascertain the presence of an illness condition which allegedly requires further evaluation and hospitalization? Would one of you please define exactly what comprises a PHP “assessment” and what is the legal status of such?
However, the national PHP system remains one operating with utterly no oversight or accountability or even credentialing, neither of the organization itself or its personnel. State PHPs don’t even have any oversight by their own federation, FSPHP, as Dr. Gundersen previously stated.
This blueprint seems to suggest that the current PHP model (including its lack of any discernible internal or external Quality Assurance and of legal and financial accountability) is apparently intended to spread to eventually cover every professional who requires licensure by some board or company (e.g. commercial pilots), and perhaps even to every EAP (Employee Assistance Program) whose counseling services are offered as a benefit to its employees. One can understand how the corporate EAPs might be particularly susceptible to lucrative “buy-in.” (The confidential counseling “benefit” could soon become an employee’s nightmare, given their unrevealed dual agency role and immense potential for violations of confidentiality.)
This elaborate national PHP program, now with its pre-selected “preferred programs and facilities” and “preferred labs” and “preferred therapists” in the community and “preferred lawyers who understand how we work” and “preferred re-education programs” (e.g. for docs who were alleged to have mis-prescribed or accused of a boundary violation for accepting a gift from an appreciative patient or who are thought to have a “potentially impairing condition” for falling behind on their charting), will result in an exponential rise in referrals of “sufficiently-cash-available” employed professionals to its lucrative cash-only pipeline. And, as we’ve learned from physicians in NC, MA, WA, OR, FL, MI, MO and other state PHPs, once you’re “in the system,” your career is essentially over. And you’ll soon be bankrupt. And singled out and isolated from your medical colleagues with the implicit perception that “they must’ve really done something wrong; guess they had a dangerous addiction or mental illness I didn’t know about ….” And you’ll be out of resources to even hire counsel to defend your rights and your career.
And Governors and legislators and state ethics committees and professional association ethics committees will all defer to the presumed integrity of “the Program.” (They, of course, are naive to PHPs penchant for reckless regulatory joyrides.) And, because these programs single out docs serially, ensnaring what would appear to be a statistically insignificant number from amongst the state’s physician population, complaints of abuse of authority and process rarely make it to their attention. But even if they do, they’re generally discounted, as the officially labeled “impaired physician” is essentially disempowered by dint of their PHP-assigned diagnosis and license status. It’s likely this very mechanism is why these abusive programs have been able to operate in such a stealth way for so long. In fact, it’s such an effective mechanism that even both of you and Dr. Gundersen have in this forum essentially dismissed all detailed complaints of abuse (nearly 900 comments have been written amongst these related articles) as simply the angry voice of physicians disgruntled with their infallible PHP evaluation and treatment “recommendations” who are “still in denial.” What arrogant asininity.)
Should any state program have the right to behave in this manner? To effectively construct an impenetrable wall of denial that immobilizes a physician or any other licensed professional person, leaves utterly no legal recourse and prevents them from practicing their profession?
Remember, this is a program that is represented to the public as a benevolent program which seeks to restore the physician to his/her practice. Really? Coerced referrals, secret evaluations, overt denial of conduct of such diagnostic evaluations, fraudulent diagnosis, refusal to provide report of findings, referral to “preferred programs” under extortion of loss of license for non-compliance, referral to programs that psychologically abuse and traumatize patients, refusal of timely independent evaluation, and denial of due process. In fact, conduct in explicit violation of FSPHP’s own program guidelines. (See:http://www.fsphp.org/2005FSPHP_Guidelines.pdf) A program that refuses to hear urgent consumer complaints and that necessitates the intervention of a state auditor and a class action lawsuit to confront its flagrant illegality? A blueprint like this ought to be exposed for the world to see, so as to ensure that it never materializes. Drs Goldsmith and Carr, would you please do us the favor of presenting “the blueprint.” Please. A link on these pages would be sufficient.
This current PHP system, operating as it does with state sanction authority and state immunity, has become a veritable Kafkaesque nightmare that will eventually be seen as one of the darkest chapters in the history of American medicine. I believe it is your moral and ethical responsibility to take ownership of these abuses and conduct a full and transparent investigation. If you disagree, I would like to learn here the basis for your disagreement.
re “The ASAM / FSPHP Blueprint” Part 2
Drs. Goldsmith and Carr:
In ASAM’s / FSPHP’s grand blueprint, it appears that PHPs (some now considering renaming their programs to be more broadly applicable “PROFESSIONALS Health Programs”) will be presented to other professional boards throughout the country as “the authoritative medical approach” using ASAM’s and FSPHP’s non-peer reviewed studies allegedly substantiating the need for extreme hospitalization (3 months – at specially select cash-only hospitals, of course) and prolonged “monitoring” (5 years!).
Have you considered how such a system, absent oversight, accountability and due process, will be capable of being misused to derail any professional’s career? Imagine being able to funnel internal whistleblowers, independent thinkers, outliers who “don’t fit” (a convenient moniker for those with disliked racial and ethnic differences from the club), competitors within a specialty… into such an assessment for a “potentially impairing condition.”
Got a “problem doc?” As it stands now, not a problem for PHPs! Send them in on trumped up and unsubstantiated allegations or maybe a sham peer review, submit your complaint anonymously so there’s no tracing it, and that professional’s career is virtually vaporized. If you’re an institution that has generously donated to PHP’s tax deductible charity (many pose themselves as 501c3 “educational public charities”), one would suspect you’re more likely to get a fast-track response to your request for a problem physician’s “evaluation.”
Spouses, aggrieved clients – want to end a professional’s career? Simply make an anonymous allegation and the professional’s licensing board happily refers the subject professional to its affiliated PHP. Done. Clean. No need for messy divorce or drawn out lawsuits; better, you’ll avoid the burdensome due process mandate and pesky laws of civil procedure that are required in that forum.
Of course PHPs love referrals! A captive group of “rich docs” who are motivated to do anything to protect their careers and avoid being publicly shamed. Certainly keeps the staffing up and the pipeline flowing. And the downstream “preferred programs” love the lucrative stream of cash-rich compulsory referrals and continued denial of due process. Hey, want to really extract the truth from the doc? Send ‘em to the polygraph expert on staff. (See for one: “Acumen Assessments – Staff – Kipp Low, MCJhttp://www.acumenassessments.com/staff/)
And in serving as the official “approved 2nd opinion independent consultation,” they serve as the perfect foil in providing PHPs with the appearance of a truly independent opinion which confirms the PHPs referring diagnosis and further cements the subject physician’s fate. (“See, they think you’re addicted / mentally ill too. We knew we were right.”)
Medical boards also seem to love keeping the PHP pipeline running. In fact, according to one colleague who detailed this in a comment on a related article in this series, the president of the NCPHP Board of Directors informed him and 3 other extremely concerned psychiatrists who had requested to met with him and the NCPHP CEO that the NC Medical Board had actually asked NCPHP to “bring in more docs and make more diagnoses” (or wording to that effect). If the mere possibility of that doesn’t send chills down your spine and cause you great alarm about one of your hallmark programs, Drs. Goldsmith and Carr, I don’t know what would. Incidentally, this premiere program’s CEO and (former) Medical Director is the immediate past president of FSPHP and is one of your colleagues. Is there therefore any doubt that this is the operant philosophy of all PHPs? “Bring in more docs and make more diagnoses.” Does that concern you at all?
Why would a medical board explicitly request that a PHP to bring in more docs and make more diagnoses? Is it just that they want to be seen as justifying and self-perpetuating their bloated staffs and as being “tough on crime?” If I understand correctly, that allegation is currently under investigation (albeit it an internal one). (One pundit refers to an internal investigation as little more than giving a rapist a shower and a fresh set of clothes.) Admittedly, I’m a bit cynical about the prospects for a thorough and honest investigation. But it is important to stress that this allegation is being made by four senior psychiatrists, none of whom has any entanglements with either the NCMB or NCPHP. All of them had compared case histories of physicians they had in their practices and were alarmed about the flagrant misdiagnoses and unwarranted hospitalizations.
That’s the exceedingly dangerous power of these programs which currently operate with utterly no oversight or accountability (again, as documented by the NC Auditor – http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf). PHPs have become a Frankenstein created in the labs of medical boards and medical societies, neither of which now wants to take ownership. (And understandably so – the liability for each state and medical society is immense!)
re: “The ASAM / FSPHP Blueprint” Part 3
Drs. Goldsmith and Carr:
Have you seen the class action lawsuit against the Board and PHP in MI? (http://www.chapmanlawgroup.com/hprp-class-action/) In that suit, members of the MI medical board and its PHP [“HPRP” – “Health Professionals Recovery Program”] are jointly named. The suit’s alleged violations include denial of due process, unlawful restriction of civil liberties and conspiracy by both agencies to systematically orchestrate these violations. Defendants are named in their professional and personal capacities. Understandably, this has caused broad concern amongst medical boards and PHPs. Their concern is further heightened by the US Supreme Court’s decision against the NC Dental Board (v. FTC) (see: http://www.scotusblog.com/case-files/cases/north-carolina-board-of-dental-examiners-v-federal-trade-commission/) which, in addition to finding an antitrust violation had been committed by the NC Dental Board acting on behalf of the state, found that the NC Dental Board failed the legal requirements for legitimately being considered to be a state agency. The implications of this SCOTUS decision for state medical boards, especially in light of litigation for denial of due process and violations of civil liberties, is immense. Each member of a medical board may now be liable for actions committed by its affiliated state PHP to which it has provided state sanction and was supposed to have overseen.
I would like your response in this forum to these concerns, Drs. Goldsmith and Carr.
If the reader has any doubts about the reality of the highly lucrative private evaluation and treatment referral pipeline in the addictions industry, you might wish to see the documentary “The Business of Recovery.” (http://www.thebusinessofrecovery.com) PHPs are a central player in this industry. And the “blueprint” all but insures that they’ll be the biggest player of all.
Interested readers would also benefit from seeing Dr. Susan Haney’s excellent presentation to the AMA House of Delegates on concerns about the immense potential for corruption in the PHP program against the backdrop of the explosive growth of the specialized “Addictions Treatment Programs Designed Especially for Physicians.” Dr. Haney was definitely ahead of the curve in exposing this and I, for one, am deeply appreciative of the research she conducted in the preparation of this presentation. (http://www.osmapandtheforum.org/upload/Oregon11.pdf)
You have elected to write a letter to the Medscape editor decrying the overwhelming negative sentiment expressed about PHPs. I think it is entirely appropriate to demand your response to these concerns.
@Dr. Kernan Manion Here is a framework to help simplify an outside analysis of the current scaffold:
https://www.linkedin.com/pulse/decision-making-regulatory-medicine-framework-special-langan-m-d-
“They have a robust body of policy statements.” Seriously? What does that even mean? What they have is not one shred of actual data, since there is no double blind study and they can prove nothing.
Some of those who have commented here have heard my story, but I will continue to share until others don’t have a story, I was referred to a PHP in a state in the southeast by the hospital where I had privileges. Anger management was the reason. As I would soon be leaving the area, I agreed to appease the hospital. Of course, like many physicians, I had no idea what the PHP system was all about. Despite being sent for anger management, I was required to give a urine sample which was not shared with me until the day of my appointment. I did not deny the use of alcohol and admitted to having drinks on non call days. I was found to have elevated levels of EtG. I had never had legal issues related to alcohol or been accused of improprieties in relationship to my job. The PHP recommended that I undergo expensive out of state evaluations for anger/communication and substance abuse. After numerous discussions with my counsel and persons adding to this commentary, I refused to sign a contract with the PHP. I offered, the referring hospital, numerous amicable solutions to the situation. However, I was rebuffed at every occasion. I lost my privileges in May of 2014 and was reported to the NPDB in June of 2014. The Medical Board investigated. My employer terminated my contract. I have spent the last year trying to fight the good fight. The hospital bylaws allowed a Fair Hearing, which I won but the MEC overturned the ruling. Long story short. I have been out of work and it has taken me nearly 16 months to finally find two opportunities that are willing to overlook my past. I have written a novel that covers the subject. I’m nearly ready to submit it to a literary agent.
Through my dealings with the PHP I found them to be authoritarian and unbending. While I was willing to attend a course for anger management, I absolutely refused to attend a course for substance abuse. I had even entertained a monitoring agreement. However, the onerous nature of the contract kept me from that. My concerns were that I could breach the contract and be open to loss of anonymity if I tested AT ALL positive, failed to provide a sample on a day required, and greatest of all were travel restrictions. I was told they could not guarantee that I could return to the Midwest for my daughter’s wedding.
I presented all of this to my referring hospital including all of the recommendations from SAMHSA and numerous horror stories I had collected. The referring entity felt they must stick by the recommendations of the PHP.
Interestingly, the Board required me to be evaluated for anger issues only. They allowed me to select from a list of local providers. I attended one session. The counselor was dumbfounded as to why I was there. With all that had happened to me, I was paranoid. I begged her to give a recommendation of some sort. She recommended a program on communication. Again, I was given a list of courses by the Board. I was able to complete a course in communication/anger management on line and at home!
While I finally have two entities who have heard my story and are flabbergasted, I have been denied numerous permanent and locum tenens jobs because of the NPDB report. The monetary, physiological, and psychological trauma have been immense. My entire family is stressed beyond imagination. My relationship with my wife has taken a serious blow. At least I think I have a light at the end of the tunnel.
@Dr. D V So sorry to hear of your Kafkaesque nightmare. I hope that you have registered an objection with the NPDB. The current handbook is here: http://www.npdb.hrsa.gov
Astounding that the MEC overturned the result of the fair hearing. Thank God you had the wisdom not to knuckle under on the SA ruse. The board and/or PHP that did this to you ought to be reported to the relevant state auditor. PHPs in some states (e.g. NC) now have an auditor-mandated grievance mechanism. Might be worthwhile checking out.
@Dr. D V This is an incredible story and demonstrates to my mind the sheer incompetence of some of the PHPs. Just because one has a positive EtG does not mean that one has a substance abuse problem, and to suggest otherwise is folly. Any person who drinks alcohol on a regular basis, i.e. wine with dinner, may well have an EtG that is positive and it means nothing. Unless….one is wanting to make the Medical Board proud by grabbing another doctor, and make the diagnostic/referral center pleased by having another paying patient. It is just unbelievable that the PHP would want to refer someone to an expensive out of state evaluation program for anger management. Such demonstrates to my mind a complete lack of understanding of clinical medicine. When one reads a vignette such as you have written, it makes one question is the PHPs are acting in good faith.
I hope your light at the end of the tunnel works out.
@Dr. D V Thanks so much for your heart-rending story. Thanks for being a man of determination and courage! God bless you and keep you. Gail
Drs. Goldsmith and Carr:
I note that neither you nor any of your ASAM colleagues has made any response to the abundant concerns raised. As you know, Medscape having provided the opportunity for comments, this is essentially a dialog forum and ongoing exchange with the authors is encouraged. However, you and your colleagues have been remarkably silent.
The abuses referenced in this series of articles are so profound that the very legitimacy and ethicality of the PHP system is being questioned.
Further, these abuses are being committed by licensed medical professionals at both the PHPs they direct or staff and at the “preferred facilities” to which they order subject physicians – under unwarranted extortion of loss of license and public humiliation – to attend. Some of these PHP program and facility professionals are board certified psychiatrists.
PHPs operate in a regulatory netherworld. They conduct “assessments” for mental illness and substance abuse at the request of medical boards and yet claim they do not conduct diagnostic evaluations. (How is that even possible?) They claim that these assessments are “peer reviews” and yet they meet none of the criteria for legitimate peer review (as clearly established by HCQIA– The Health Care Quality Improvement Act, 42 U.S.C. Section 11101 et seq.) They publicly proclaim that physicians subjected to these evaluations have all the rights of due process and utmost confidentiality and yet flagrantly violate these provisions leaving violated physicians with no legal or medical recourse.
Further, while they present themselves in appearance as legitimate psychiatric / mental health entities, in actuality they claim that they are not even healthcare organizations and rather conduct these invasive and career-altering activities under the rubric of a state-sanctioned and immunized “educational public charity.” To me, this appears to be both institutional camouflage and the organizational equivalent of identity theft. However, it is organized psychiatry’s very identity that is being used for this dangerous masquerade. And organized psychiatry ought to be extremely concerned about such identity misappropriation. Because great harm is being done to the very integrity and public reputation of the field of psychiatry – no, to all of mental health, and in fact to American Medicine’s core values as we know them. (see: APA Code of Ethics and ACP Professionalism in Medicine)
You are presumably aware that virtually all of PHPs’ programs subscribe exclusively to a religious-based “AA 12-step” model which itself is not validated for effectiveness. Additionally, forced compliance with such a program is distinctly counter to constitutionally protected rights guaranteeing separation of religion and state.
I have spoken with multiple physicians and other healthcare providers who describe what amounts to psychiatric abuse at the hands of PHP CEOs and medical directors and directors and staff of FSPHP / ASAM “preferred programs.” The responsibility for investigating and prosecuting these abuses and providing for reparation falls directly in the hands of ASAM and FSPHP.
What have you as an organization done about these concerns? I suspect nothing. As noted by Dr. Cavenar, his submission of a detailed ethics complaint to ASAM about these abuses – the only way to bring such concerns forward short of litigation – yielded a response from the then current ASAM president that he didn’t know that ASAM had a code of ethics! And then on learning that they did, informed Dr. Cavenar that these weren’t really enforceable and were really just, sort of, well … “suggestions.”
The appropriate design and delivery of health care and its oversight by medical professionals is not based on “suggestion.” It is based on the accumulated knowledge of research-based science and the time-honored privilege of peer scrutiny. More so, it is a fiduciary duty and a sacred obligation. And to neglect that duty is both a profound ethical breach and a grievous offense to the very profession of medicine itself.
What are you now doing about this? I do hope the answer is different than that implied in your fatuous letter, heroically singing ASAM’s praises in its oh-so-devoted self-sacrificing rehabilitation endeavors while dismissing all of these cases as just those of a bunch of disgruntled losers dissatisfied with their PHP-assigned infallible diagnoses and treatment. Patients whose dissatisfaction you designate, through your insular and circular reasoning, as proof of their clearly still being “in denial” and not yet having gotten far enough along in their “steps” to embrace the loving and forgiving spirit of the exalted Big Book.
Dr. Goldsmith, as you are a physician with a specialty in psychiatry and are a DLFAPA – a Distinguished Life Fellow of the American Psychiatric Association – and the physician who serves as the current President of ASAM, I call upon you to open a comprehensive and fully transparent investigation into the operation of all aspects of the PHP system, at least those components as staffed by ASAM members (which I suspect will be nearly all of them, as, after all, the bulk of PHPs and its compulsorily attended “preferred facilities” are directed, owned or staffed by “like-minded docs”).
As an initial indication of your concern, you would do well to reach out to those of us who have spoken of our concerns and hear us out.
I also believe that it is your professional duty as a DLFAPA, upon learning of these concerns as abundantly expressed in these articles, to urgently seek from the APA the formation of an eminently qualified and thoroughly independent task force to examine not only these concerns but to carefully study the entire PHP system (and its quasi-psychiatric facade) as it is currently established and to make recommendations for its redesign, oversight and legal accountability.
Personally, it is my belief that the widespread abuse occurring within this supposedly compassionate and therapeutic program will soon be publicly seen as on a par with the Catholic Church’s pedophilia scandal. This one however involves involuntarily prolonged detention under extortion and profoundly harmful psychiatric abuse of a most malevolent kind. The sooner you and FSPHP and the APA and AMA demonstrate real concern and exercise stewardship in this, the better for all. I am certain that the longer this out-of-control program goes unexamined and unrestricted, the more harm will be done to physicians (and to the patients under their care), to the PHP movement itself and to organized psychiatry and medicine as a whole.
I welcome your reply at your earliest convenience on this forum.
@Dr. Kernan Manion I, like Dr. Goldsmith, am a Distinguished Life Fellow of the American Psychiatric Association and an Emeritus Fellow of the American College of Psychiatrists, as well as Professor and Vice Chairman Emeritus of the Department of Psychiatry at a major university. Furthermore, I was the Senior Medical Review Officer for the U.S. Army Substance Abuse Program, Europe, for eleven years.
I have called upon the Medical Director of the American Psychiatric Association, the President of the American Psychiatric Association, the President of the American College of Physicians and others to open a comprehensive and fully transparent investigation into all aspects of the PHP system. I am optimistic that such an investigation will take place.
In fact, it is my opinion that all of organized medicine, including the American Medical Association, American College of Surgeons, American Psychiatric Association, American College of Physicians and other such groups should join together in having a full investigation of the PHP system.
@Dr. Jesse Cavenar @Dr. Kernan Manion I am heartened to hear that. And, amongst many, I am deeply appreciative of your tireless involvement and advocacy on this issue.
As a registered nurse who was voluntarily admitted to a PHP in 2012, my own experience closely parallels that of Dr. DV’s below. As an employee in good standing at a very reputable teaching hospital, I naively believed that I would be treated well by the facility I worked for, as well as by the medical professionals I had no reason not to trust. Instead, when I asked for a life preserver, those trusted practitioners threw me an anchor instead. As a direct result of asking for help, I lost a 20-year career, and my previously impeccable reputation has been permanently sullied. It took me nearly two years to reinstate my professional license and to find employment. My family has been financially devastated, and my children suffered the consequences of my choice– the choice in which I mistakenly believed was the responsible one.
“Authoritarian” and “unbending” are possibly the most benign descriptions I would have ever considered. In my experience, the practitioners I encountered were almost ritualistically sadistic. It still remains inconceivable to me, that at a PHP facility in one of the major, premier healthcare systems in the southeast, that my peers and I would be routinely subject to shame, humiliation, and fear, based on the ever-present threat of losing our professional licensure. The dehumanizing interactions with the physicians and their staff was alternated with readings and interpretations of that travesty of a treatment protocol, the “Big Book”, and forced Bible study– regardless of our individual histories, beliefs, or needs. Such is the cutting edge nature of modern treatment modalities in the year 2015.
It is easy to be dismissive of complaints that seem outlandish; to presume that they must be exaggerated, or confabulated, or the grumblings of a vocal minority of bitter malcontents. It becomes more difficult to be so dismissive, however, when the individual stories are mounting in number, and all seem to share common threads of emotional abuse and financial extortion at the hands of a closeted industry with no oversight. I have recently been directed to a website where these increasingly common stories regarding such systemic abuse and one particular practitioner are shared at stopscottteitelbaum.com
I hope a very bright light will be shone on this industry to prevent others from being victimized.
,
In addition to the stopscottteitelbaum.com site, I also discovered that there’s a questionnaire for those who have been similarly abused. I guess that’s indicative of how serious that provider’s abuse problem is. It’s http://www.frcgainesville.com. I’m deeply relieved that legitimate medical attention is finally being paid to such programs. I know they are not in the intended spirit of PHPs or [nurses assistance] programs. Docs and nurses, like the rest of the population, occasionally run into SA and MH problems and need competent and compassionate help. However, these sorts of programs mentioned here are not at all the kind of help that is needed.
Also available for consideration is http://www.likemindeddocs.com/members.html, where many of the docs that run the PHP programs share their disregard for evidence-based protocols in favor of faith-based healing.
@Allison Lansdowne @A L Wow! Those sites are terrifying! I hope they are able to corral that Teitelbaum character. Like minded docs is equally appalling. The whole idea of a need for spiritual based healing is not something to which all people subscribe. It goes against the idea of separation of church and state.
State Auditors will find that EVERY “PHP-approved” facility is represented on this list of “Like-minded docs” (Hazelden = Seppala, Talbott = Earley, Florida Recovery Center = Teitelbaum, now Thompson). Over 2 dozen “PHP-approved” facilities are on the list.
FSPHP then President Pendergast could not provide the NC. State auditor what objective qualitative criteria or quantitative measurements the NC PHP ( and by extension FSPHP) used to “approve” a “PHP- approved” assessment and treatment center. The best he could come up with was “reputation” and “word of mouth.”
Think a minute of the import of this– it is akin to asking the FDA what criteria went into approving a drug or device for “FDA-approval” and them answering the reputation of the pharmaceutical manufacturer or “word on the street.”
This is friends referring to friends and this self-published list represents hubris.
Wow!
I guess Pope Francis missed the boat on his chance to canonize Dr. Goldsmith and his ilk, or should I say cohorts?
“We have a robust body of policy statements supporting the role of physician health programs and an active Physician Health Committee, which includes current and past directors of state physician health programs (PHPs), as well as current past leadership of the Federation of State Physician Health Programs (FSPHP). ”
Having a robust policy in no way mandates compliance and adherence to that policy. Once upon a time, the national speed limit was 55 mph; I confess to being nonadhereent and noncomplaint with that. Or as they say in the field of addiction medicine “Denial; it’s not just a river in Egypt anymore!”.
“The article reviews their allegations in some depth and goes on to discuss investigations of PHPs in Michigan and North Carolina, with emphasis on the latter. The article reviews concerns over lack of due process, out of state treatment requirements, cost of treatment, “expensive contracts,” treatment center demands for payments, lack of PHP oversight, conflicts of interest, etc. All in all it presented a very disparaging view of state PHPs.”
I concur, but only because that has been my experience in both Florida & NC. Florida sent me to a treatment plant that had a “28 day program”. All of the physician captives laughed when I told themI was there for that program. I was there until all of my assets ran out and was pronounced cured, had a chip-out ceremony in which I was voted most likely to relapse and left crazier than I was before being brainwashed there for 4 MONTHS! The center never picked up on a congenital syndrome I had.
NC had similar results after I was sent out of state for an “assessment” then “treatment” in the SAME facility that alleged “expertise in treating that congenital disorder”. At a formal NCMB hearing I was told I was their 8th patient with the disorder! Can anybody say “conflict of interest”?
“…the “distressed physician,” typically a physician in need of interpersonal coaching to improve communication”.
The physicians I’m familiar with were distressed to be under the glare of the Medical Board with referral to the PHP.
“The author failed to note the national study of PHPs called project Blue Print. This study revealed that nationally, PHP participants demonstrate a 78% success in recovery without relapse at an average of 7.2 years of monitoring.”
There’s a lot to be said for the coercion of having your license held over your head with the threat of loss of licensure. I’ve chosen to be alcohol abstinent for nearly 17 years; a small price to pay to help avoid future PHP experiences (which, alas, didn’t work due to my congenital issue).
“Before PHPs, physicians with these illnesses dealt directly with their state medical boards and were often disciplined merely for being ill.”
Been there, done that; despite having a PHP contract I was told to “just accept what the Board gives you; you’re guilty just by virtue of the fact that you are in front of them”.
“The author communicates that those involved in a PHP have no due process.”
The NC State Auditor mandated the formation of an appeals process. The NCPHP claims to have established such a process but won’t disclose who is on the board, what credentials those members have, how they were chosen or anything about that board unless the questioner comes to the NCPHP for an “evaluation, which is an euphemism for “hostage situation”.
“The PHP offers the physician with potentially impairing illness an opportunity for a multidisciplinary evaluation at a choice of nationally recognized facilities. If treatment is indicated, they are given options for centers equipped to provide treatment. If they disagree with the evaluation, they are given the option of a second opinion evaluation.”
In the case of James Fenn MD vs. NCMB https://glsuite.ncmedboard.org/DataTier/Documents/Repository/0/0/7/4/774d2bee-0332-4045-ab2d-42af6ba6de12.pdf the court overturned the NCMB’s disciplinary actions based on Dr. Fenn’s desire for an independent evaluation–independent of the NCPHP and Scott Teitelbaum at the University of Florida center where Fenn was sent for evaluation disclosing him to be alcohol dependent, despite his rare use of alcohol at the time–but being exposed to the NCMB & NCPHP would be enough to drive Bill Wilson, founder of AA to drink!
Dr. Goldsmith superficially comments the NC State Auditors results; http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf
The auditor revealed numerous other deficiencies that he failed to disclose in his letter. The Auditor only reviewed 100 charts. The report did not address numerous issues that others like me & I have been subjected to, they are to numerous to go into in this letter, but certainly parallel the comments made by numerous others on this forum regarding the PHP’s -(to be continued)
Continued
“…PHPs support physicians by directing them to evaluators and treatment programs with the requisite expertise to care for professionals in safety sensitive employment.”
NC has half a dozen medical schools and two dozen post-graduate mental health programs. Why then, are it’s “indentured subjects” referred out of state for their care? Oh yes! as the Auditor said, these out of state centers fund the NCPHP retreats held every 6 months or so.
“However, physicians may pursue second opinion consultations, just as patients in the general population are encouraged to do.”
Back to Dr. Fenn’s case–the only licensee who has taken the issue far enough (outside of the NCMB/NCPHP oligarchy) to an independent civil court for his exoneration.
“…the PHP can confidently advocate for the physician’s return to practice before their regulatory board, hospital credentialing bodies, malpractice carriers and others.”
Again, not my experience, but admittedly I’m a sample size of “1” (unless of course one counts the others who have written comments on the Medscape articles).
“They are held to account every day by their state medical boards and professional associations, their state hospitals and the partners of every doctor they work with. A single incident of patient harm by a PHP-monitored doctor would result in public outrage,…”
The NCMB is held by numerous state general statutes as are all medical boards. In 2003 SB 882 reaffirmed the limitations on the NCMB. Ithas been thoroughly ignored. They ignore those statutes, since they are “above the law” as is the NCPHP. Regarding “public outrage”; that may be true if the public were aware of it, but since there’s this pesky little thing known as HIPAA, the public is NOT aware of it! Does Dr. Goldsmith think we’re idiots?
“It would take us back to the licensure revocations observed in the 1970s…”
What is the difference between licensure revocations without the PHP’s vs. “indefinite suspensions” with the PHP’s?
“They are most often led by professionals who are devoted to helping those colleagues…”
The fact of the matter, is that it seems that the vast majority of folks who go into the field of addiction medicine have addiction histories themselves. Just because one is abstinent does not guarantee that they don’t suffer the other aspects of addiction “…drinking is but a symptom of our disease” (Quote taken from the Big Book of AA). I would offer that those in the PHP’s have unlimited power which activates their underlying addiction neural circuitry and turns them into manipulative monsters–despite their supposed use of their “other drug of choice”. Addicts “use” to alter their emotional state. Extreme power is also known to alter emotional states. They switch one addiction for another and do so at the EXPENSE of their colleagues!
Respectfully
A battle scarred veteran of the NCMB & NCPHP with a true interest in protecting others and improving the state of the art.
Stop with only using 12 step programs and use MAT.
@Dr. Paul Bowman. The majority of this group is not only anti- MAT but anti medication. They will take benzodiazepines away from epileptics and discontinue anti-depressants. The Massachusetts PHP, PHS inc. refuses to allow asthmatics metered dose inhalers because they use ethanol as a propellant ( since CFHC was universally banned as a propellant due to ozone concerns ) and it might ” interfere with EtG testing.” Earth to Steve Adelman asthma is a “real” disease not a “potentially impairing” one.
They are also against using Naloxone in the community to reverse OD. I have an email from one “like-minded doc” stating it sends the wrong message. “If these addicts start getting revived then how will others learn. Some need to die to keep others sober. If you can simply get a shot then it shows no consequences.”
It is hard to wrap your head around the mentality of these reprobates – we need to be outraged as a community and demand they be removed. Many need to be criminally charged!
I raised this question after the previous Medscape article. Is there any case of an opioid addicted physician participating in a PHP program who is being treated with Suboxone? No answer to date. Yet this is the current standard of care for other patients. Time for them to get with the practice of 21st century medicine.
@Dr. karen miday Dr. Carr has said in the past that suboxone is not permissable for physicians.
@Dr. karen miday Absolutely. It is on a case by case basis and a state-by-state basis. The concern is cognitive impairment with any opiate based treatment. In my state, physicians are permitted to practice while taking opiates, benzos and other potentially cognitive impairing medications provided they demonstrate cognitive intactness on screening instruments. It would be foolish to believe that physicians are not taking medications for anxiety, pain, etc — we simply need to be responsible about our health and not practice if we are unduly influenced by medications we need to be well.
A Must Read
Physician Suicide and “Physician Wellness” Programs–It’s time we start talking about the elephant in the room!
Physician Suicide and the Elephant in the Room Michael Langan, M.D.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to […]
Doctor Suicide, Suicide, M.D.Suicide, physician suicide
While in a PHP for addiction to prescription pain medication I developed after delayed diagnosis of compartment syndrome , and subsequent fasciotomy which was complicated by CRPS/RSD . I had some 20 months of sobriety, was finally back to practice for the last 6 months after being in treatment some 90 days, followed by residential care for 6 months, daily AA meetings biweekly “psychotherapy” etc all developed as part of my “treatment contract” by those I would never know or meet, at a cost of well over 100,000 dollars. I was able to resume work after about one 9 months of sobriety with continued daily participation in the PHP. At 20 months into the PHP I fractured and dislocated my left shoulder. I went to the ED, and explained that I was in “diversion” and could not take any narcotics unless approved by my “nurse monitor”, a prior psychiatric RN, who I spoke with every now and again in the PHP. She was my contact in the event of an emergency. I never once ever met anyone on the Diversion Evaluation Committee, as is guaranteed to me by the medical board in my state, in fact on my “treatment contract”. When the ED doctor told me he was admitting me to ortho and would likely require surgery, I still however,required emergency reduction of my shoulder as I was experiencing parathesias and weak pulses. I called the PHP nurse monitor, she informed me that “If I take anything more than a tylenol she would have my license” . I put the ED doctor on the phone so he could explain the need to reduce my fractured shoulder and his unwillingness to perform the procedure sans appropriate medication. She still repeated the same tylenol mantra. He then consulted the Othopedic shoulder specialist and Pain Management given the delicate nature of my situation. All this time, I am out of socket, and without pain medication. Finally , after speaking with all of the consultants at beside, they assuaged my fears, and said “there is absolutely no way anyone would expect us to do this without pain medication”. I know, with a decade of ED experience, I certainly would not, especially in light of the fracture! I believed that rationale thought would prevail and allowed the doctors to quickly reduce my shoulder after a bolus of iv dilaudid. I was then admitted for one week, the orthopod, proposing surgical ORIF of my fracture. I was able to contact the board from the hospital and explain what the PHP was trying to say, assuming they would see the inhumane nature and clear violation of my civil rights. They did not. They stated blankly essentially, “they said what ever the PHP said” That the PHP makes all the decisions and if they were going to call my “choice” to take the recommended pain medicine and/or anesthesia for the surgery…..I would lose my license. And, that is exactly what happened. When the detectives came from the board to have me evaluated, upon discharge from the hospital, I was still wearing my hospital wristband on one wrist and on the other a fundraising wristband I had been given for a little 9 year old girl whom I had saved her life, just a couple of weeks before the injury. The fact that I was in the paper and named as a” life-saving”. “thank God for…. ” etc and that I had participated in their PHP successfully and at great cost., did not matter, I lost my license. This was viewed as a “relapse” . Yep, my broken bones and dislocated shoulder was a “relapse ” I think about suicide and how I will put my life back together every day.
@michelle b I am on facebook! Look me up! We are in this together…
You are brave, determined, and in the right…this should be looked at by ADA lawyers. What a horror story! Thanks for sharing.
In times such as these, overwhelmed with “new” and rapidly mutating viruses and “superbugs”, poor border control with no serology testing mandated for all that come into this country except for just a few screenings performed by non-licensed medical personnel, the already overwhelmed healthcare system now needing more and more physicians and nurses alike to accommodate and care for those that enter this country illegally and are to be taken care of medically at the taxpayer, hospital, clinic, physician/nurse/staff expense while watching our hospitals file bankruptcy for non, little, or horrendously late reimbursement for those that have poor insurance plans they are forced to take or be penalized severely for by powers that be, I have to ask this simple question: who’s side are the PHP’s, ASAM, Boards etc. on? Are they not their brother’s keeper? Stated in the article above, they are supposed to be there to help… but are they? How many have been forced into these programs unjustly? And can anyone tell me, please if you know, how many patients were harmed by these providers that are in these programs? Because that’s what these programs are for, correct? Patient safety? Protecting patients from harm by a provider that has been given a diagnosis of some sort of mental illness, alcohol and/or drug addiction, and now, if they are GAY? Are every one of the providers that are in these programs guilty of harming another person? Because as it appears, if they ask for help, they themselves are being harmed. Mentally harmed. Financially harmed. Some physically harmed if they cannot take medication prescribed to them for fear of reprisal or losing their license for such. Is that helping?
Physician’s, providers of any type, and all medical personnel, have had severe cuts in pay, reimbursement, compensation of many types and have to see twice as many patients now opposed to years ago in attempt to keep their doors open. Patient care suffers. All medical personnel suffer because they are trying to do what’s asked of them because they believe in the oathes that they took. Many are trying to find other avenues to bring in more revenue in order to keep their staff. And the physician (s) and Judges that sentence and/or diagnose other physicians/providers and put mandates and regulatory stipulations on their colleagues either justly or injustly, and are making a profit by “helping” these accused providers, echos the violation of Starke’s Law. That, beyond a shadow of a doubt, is at the least a conflict of interest. And draws to light the question of abuse of both authority and power.
I, too, believe that these programs were originally set forth to help providers that may have problems and need help to continue to practice to the best of their ability. I believe the original intent was good. But like so many other programs, they can become corrupt. And it needs to be addressed and looked at by someone that is not going to benefit one way or the other by making recommendations perhaps. Fear of reprisal is a very big issue in medicine. Already physicians have to give up, to much extent, their 6th and 14th ammendment rights to face their accuser if they are complained about to the Boards and investigations are opened. We’ve all heard horror stories and malicious gossip of these things. All fear Board’s, PHP, and other agency involvement in their practice because the overlying theme is that they are all “guilty until proven innocent” and that should not be. These entities of which we speak are supposed to be helping, not hindering, supporting and not cutting down, their peers, colleagues, and friends.
What is happening is not right. These people of great knowledge and talent don’t deserve what is happening to them. We NEED medical personnel more than ever right now. It doesn’t make sense why so many are on the band wagon to harm their fellows. We have so much to worry about in healthcare that this just adds to the long list of why one SHOULDN’T want to be a provider, not why one SHOULD. Is it not the most noble of professions any longer?
Yes, Angela, what is happening is definitely not right. The outcome of my son’s referral to the Missouri PHP is that he is now dead. He certainly never harmed anyone, and by all accounts, was a talented young interenist who was about to become an oncologist. It makes absolutely no sense. Truth is, rather than protecting patients they are causing great harm by removing capable doctors from practice….some, like my son, forever. The answer to your question appears to be that they are on their own side. This is how they stay in business. My son found very adequate care elsewhere, and they would not allow it….especially because he was seeking treatment at a public facility that would not line their pockets. Had they encouraged it…or simply ok’ed it…he would very likely now be an oncologist. So, we can all give thanks to the MIssouri PHP for one less cancer specialist. Oh, and by the way, his relapse occured when he was on vacation in Puerto Rico, so certainly no patients were harmed. He self-reported when he returned.
I can report that the system in Tennessee and Mississippi are safe and effective for the physician. The ongoing connection to the program has helped alot with advocacy with hospitals, med mal companies, and state boards.
@Dr. P H That’s a bit like the Archbishop declaring that there is no sexual abuse going on in his diocese.
Further, how would you know they (the PHPs) are “safe and effective?” What gives you the authority to make such a fatuous global pronouncement covering two states’ PHPs and their shadowy network of “preferred programs?” Are you perhaps involved in the administration of these programs?
It is most curious that, representing yourself as a psychiatrist, you would make no mention of the voluminous comments in this and related articles concerning unwarranted referral, extortion and psychiatric abuse, not even acknowledging the pervasiveness of the problems reported in literally hundreds of comments.
Please say more about your experience and capacity to make such a dandy pronouncement.
Now, it IS possible that you’re a physician who has had multiple relapses and has actually been helped by these programs. Good for you and so be it. Continued recovery to you. But the only generalization you could offer here would be that certain components of these programs were helpful – to YOU. It is not even possible for an individually afflicted physician in recovery to make such a general pronouncement about “the system in two states.” Ludicrous.
And truly, through the present, nothing about these organizations – ASAM or FSPHP – manifests a shred of integrity. What these predatory PHP programs have done to physicians’ careers and even to their own mental health is nothing short of criminal.
Barring your straightforward response, one can only conclude you’re an ASAM shill hiding behind the anonymity of initials.
@Dr Kernan Manion. — you are correct Kwenan. It’s not too hard to figure these people out
@Dr. Kernan Manion @Dr. P H Dr. Manion, your attack on Dr. P H demonstrates why more physicians are not posting on this Medscape commentary opportunity. If someone disagrees with you, you shred them. You identify yourself as a victim but have little awareness of how you victimize others who are merely stating an opinion or sharing their personal experiences. You quickly make assumptions that they are somehow part of the machine against physicians ostensibly caught in the web of PHP abuses. Please let any and all posters comment and please, respect their views. People in glass houses should not throw stones, do you remember this simple truth?
@Dr. P H I would point you to the case of Dr. John Moffit – he killed himself as a direct result of the “help” of the Mississippi PHP.
@Dr. karen shackelford @Dr. P H And Dr. Shackelford, I would point out that you are disrespectful in publicizing this physician’s death – he is unable to speak for himself. You are out of line suggesting a direct correlation between his PHP involvement and his premature death. How could you possibly know the facts? You are being reckless in your conclusions.
You clearly have no idea of the truth. Until you identify yourself, I see no point to engaging with you further. Your agenda is clear.
@Dr. karen shackelford Karen is correct Dr AM. Why do you feel the need to hide behind your initials??
@Dr. sarah reade @Dr. karen shackelford There are many physicians posting anonymously here. Why should that matter?
@Dr. A M @Dr. karen shackelford @Dr. P H Dr. AM: It is because this physician is dead that I am speaking out. My knowledge of his situation came directly from him and later, from a staff member at the facility where he was forced to remain for outpatient therapy, which was the period during which he suicided. Nothing I have said was disrespectful of this physician. I know if the roles were reversed I would hope someone would speak out on my behalf.
@Dr. P H On what basis can you make these statements? Please tell us more.
@Dr. P H I concur with you Dr. PH based on contact with physicians I know practicing in these states. Well functioning PHPs do have a roll in educating medical executive committees, malpractice carriers and other credentialing bodies. It is an uphill battle to educate these entities that physicians can suffer from illnesses but not be impaired and that illness should not be met with discipline. I know physicians who are unable to sit for their board examinations simply because they are on stipulated agreements with medical boards related to illness and NOT criminal behavior. Physicians are not immune to illness. We are human beings. As long as we act responsibly in getting our illnesses treated, we should be afforded the privilege of practicing medicine, absent discipline!
The ASAM’s “Robust Body of Public Policy Statements” needs further explanation and exploration-namely what science and evidence was used as the basis for these declarations? Are these statements based on solid ground or do they simply represent “policy entrepreneurship”? (i.e. policy that is self-serving under the guise of righting the “public good.”)
In 2011 the ASAM issued a Public Policy Statement on Coordination between Treatment Providers, Professionals Health Programs, and Regulatory Agencies recommending physicians in need of assessment and treatment be referred only to “PHP approved” facilities and also that PHPs need the full cooperation of the board if they deem a monitored physician noncompliant as “criticism or doubt could unintentionally undermine the PHP” (incidentally this same notion was used to remove the sordid past histories, including criminal records, of many of those involved in this system).
In addition the ASAM wants regulatory agencies to recognize the PHP their expert in all matters relating to licensed professionals with “potentially impairing illness.” You read that right, “potentially impairing illness.” The Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting and approved the concept of “potentially impairing illness” and “relapse without use.”
Please provide an explanation for these public policy decisions. “Robust” as they are I can’t find any data to support them. Please educate us.
I went through the “Florida Physicians Recovery Network” which then became the “Physicians Resource Center”.
My experience was horrible. Ray Pomm MD was the director and the “mythical wizard behind the green curtain of Oz”. Nobody was sure if he even existed. It was nearly impossible to communicate with him–only by USPS mail and a response was usually via his staff.
I was sent to a God-forsaken treatment plant out of state, went through hell for 4 months after signing up for their “28 day program” and told “you can leave any time you want, there are no gates here”. The only reality was that those who didn’t complete their program would never practice again.
That’s a helluva gate! I was there for a misdiagnosis
Now the FL program wants to put a physician from the Florida Recovery Center in charge? A center with a policy of “working with” agencies such as the NCPHP “to ensure that correct care is given”.
This is also known collegially among PHP’s as an “independent assessment”.
Right; Am I the only person who sees a problem with this “independent assessment”? A colleague who was sent there was told by a therapist who refused to be named that he had “orders” for what the assessment would show. This colleague later had an independent evaluation at a center of his choice where a completely different assessment was given.
When I went through their program I found it to be a farce. They also missed my diagnosis, but thankfully didn’t return me to the “treatment plant from Hell” that I”d been subjected to previously.
Less than a year later while attending the mandatory “annual PRN retreat”, the psychiatrist that diagnosed me picked up a “white chip”–he had just had a relapse himself!
Now, let’s “improve” (via the PHP standards) the FL PRN, to do this in a manner suitable to the FSPHP’s it should be done up to their standards…
Hey, here’s a thought; Let’s use a guy with a web page devoted exclusively to him!
http://www.stopscottteitelbaum.com.
http://www.vitals.com/doctors/Dr_Scott_Teitelbaum/review
http://www.vitals.com/doctors/Dr_Scott_Teitelbaum/reviews
Yes, this would certainly be acceptable to the exemplary standards set by the FSHP, not only does he have his own personal web page, but he has detailed reviews from other sites as well (noted above).
And people wonder why there’s a problem with these PHP’s?
Really?
Another Wounded Healer (who won’t give up!)
@Dr. R O In 2000 the FSPHP advocated for Dr. Teiitelbaum before the CT Medical Board to get his medical license back. With this PHP advocacy he successfully did so but at the time two members of the CT Medical Board were opposed to returning his license due to a history of manipulating the system. Details can be seen on CT licensing website ( https://www.elicense.ct.gov/Lookup/LicenseLookup.aspx ) and include the following statements:
“The twice weekly random, observed urine screens imposed upon petitioner by the 1992 and 1994 Consent Agreements were insufficient to detect his then on-going substance abuse. Petitioner WAS QUITE ADEPT AT MANIPULATING The SYSTEM TO AVOID DETECTION.” (my emphasis).
It is important to recognize that a number of doctors in this system have similar histories.
@Dr. Michael Langan @Dr. R O Dr. Langan, it may be true that physicians working within treatment programs assisting physicians or employed by PHPs have a history of illness. My argument is that if physicians have been down that road and have successfully recovered from illness and want to help other physicians get well, this is not a crime, In fact, I would argue that these physicians have added credibility in that they have been successfully treated and in turn, want to help their colleagues. Are you stigmatizing them and suggesting that because they have been ill they are not qualified to treat their colleagues? Erica Franks MD has devoted her career to studying physician health and what she discovered is that physicians who engage in healthy habits are more likely to influence their patients in a positive way. So if I am an obese physician and I find a way to lose weight through better nutrition and adopt an exercise program, I believe I will have great credibility with my patients because I will have genuine empathy and credibility through my own weight loss success. How is this different from an addicted physician who recovers and shares his/her successful strategy with patients?
@Dr. R O This is concerning. You should never be mandated to attend a retreat at a treatment center. Please notify your medical board. Also, I am concerned about professional boundaries here – if a treating individual is accepting recovery chips among the people he is treating. I would encourage you to write a letter of concern to the PHP and also the medical board. I am truly sorry you had such a miserable experience. Also, I would encourage you to notify the FSPHP about these perceive conflicts of interest. While the FSPHP likely has not regulatory authority over this treatment program, they can conduct an inquiry and opine on the ethics or lack thereof, and choose to endorse the program or not.
@Dr. R O If there is an individual practitioner in your state who you believe is incompetent or unethical, you do have the right to file a complaint with your medical board. I would back that complaint with factual information. I would not want any physician to practice who is unethical or incompetent.
Where are the thousands attesting to the benefits of PHPs? They certainly didn’t respond to Ms Anderson’s article and they don’t seem to be doing so regarding this article. PHPs have the potential to assist and advocate for physicians unfortunately most physicians experience with PHPs has been coercive and detrimental to their personal and often professional well being.
@Dr. D R Only speculating here, but I believe those physicians who have had good experiences with PHPs are not following this thread, and if they are, feel intimidated by the negative vibe and choose to remain silent.
@Dr. A M @Dr. D R No, not likely…just you, the only defender of the Physician Destruction Programs, the Doctor Killers…400 suicides every year! Dr. AM…400. an entire medical school enrollment.
I hope you will read on and open your mind to the FACTS, the indisputable facts…PHPs KILL!
Physician Lives Matter, nu?
@Dr. Gail Hirschfield @Dr. A M @Dr. D R Physician lives absolutely matter. But your approach is a defeatist approach Dr. Hirschfield. No one will take you seriously because you are so reckless. To suggest PHPs kill is absolute slander. I hope you have a good attorney watching your back because you may be exposed to legal action.
@Dr. A M @Dr. Gail Hirschfield @Dr. D R
Slander? do you mean libel? since physicians have died, as presented here, through the recklessness AND coercion of their PHPs, then the fact speak for themselves. Dr. A M, I am not worried…look, as you surely must agree, evil flourishes when good men stand by and let it. I am not one of those who will stand by.
I’ll tell you another-“when small objects cast long, dark shadows, the sun is about to set”.
PHYSICIANS’ LIVES MATTER
@Dr. Gail Hirschfield @Dr. A M @Dr. D R Show me the facts Dr. Hirschfield, otherwise you are slandering individuals, organizations and doing nothing to promote physician health. You are simply making allegations and you have not posted any hard facts to support your claim. You have no credibility this way and you are consciously and deliberately, knowingly making harmful, derogatory statements. You simply lose credibility. You lose your opportunity to speak in support of your deceased colleagues and those who may pursue suicide. You are no hero or advocate in this regard. Your rhetoric falls short of the factual information so sorely missing in preventing the tragedy of physician suicide. If you really care, advocate for research, advocate for physician support resources. Simply denouncing organizations will get you nowhere. It is all too easy to denounce the efforts of others and clearly more challenging to make a commitment to being part of a movement to change the status quo. Be a part of the solution. Otherwise, you join the ranks of the perpetually disenchanted, unhappy, cynical, nay sayers who become solely preoccupied in their attempts to sabotage the efforts of those who are optimistic, have hope and invest mind and spirit in creating something good. Your choice.
One of my esteemed professors at the University of Mississippi School of Medicine had some stress-related issues – no substance abuse, no boundary issues – and was referred by the PHP to an “approved facility” for evaluation. He told me they had “recommended” he stay for ten to twelve weeks of outpatient treatment. He was deeply ashamed, he said, because he was yanked out of his job and his life, and was not given the option to pursue something more reasonable, such as the care of a local qualified and licensed physician. He killed himself a couple of weeks before Christmas in 2008. To be clear, he shot himself in the mouth. I don’t think the PHP was very helpful to him. It’s ironic, since his mother was, by all accounts, a talented and compassionate psychiatrist who was instrumental in setting up the PHP system in our state as a compassionate alternative to a medical board hearing for doctors.
Dr. Shackelford, I am so sorry to hear of this. I lost my 29 y.o physician son under similar circumstances. He never got over the shame induced by being yanked out of his residency program at Washington U in St. Louis for 3 months when he was sent out-of-state to a facility that was headed by a “like-minded doc.” I truly believe that it was his fear of having to do a repeat 90 days that triggered his suicidal crisis. Beyond my own grief, it is heartbreaking for me to think of all the patients who would have benifited from his care. He was a brilliant and meticulous clinician. He drank…oftentimes to excess…during his times away from the hospital, but was never impaired when seeing patients. It is high time for us to recognize the concept of “potenitally impairing” illness for what it is…. an excuse for those in power to profit from a captive audience. It is also high time for us to question the mental health of those who run these programs. Their Axis I dx of substance dependence may be in remission, but perhaps there may be some “potentially impairing” Axis II issues?
@Dr. karen miday This is indeed heartbreaking. But if your son was drinking in an abusive or dependent fashion, he deserved to get well, independent of his duty to do no harm to patients. Sooner or later, his alcohol problem would have impacted his ability to care for patients. This is the nature of addiction. I am only sorry that he did not find a mode of treatment that he connected with. This is something PHPs need to consider. One size does not fit all. I wonder if a different treatment plan to accommodate your son’s anxiety issues would have been more beneficial. All of this is hindsight, but worth considering for other physicians similarly situated.
Thank you Dr. A.M for your compassion. My son did indeed deserve to get well. He was working with his own private psychiatrist on these matters and had decided to attend an inpatient program at a public, local treatment faciltiy. His final calls were to his PHP to notify them of his intent. They discouraged his plan and instead suggested that he come in to talk with them.
This “nature of addiction” idea is an out-moded concept. I have read numerous scientifc articles that challenge this concept and explore the various presentations, course, and outcomes that addictive illnesses might have. There are actually legitimate studies that suggest that some young people grow out of their abusive drinking habits. There are also more than one treatment modality. Greg was repeatedly told that if he did not rigorously follow a 12 step, abstinence-based model of treatment, he would die of his illness. Now, please tell me of any other disease process that can only be treated with a single modality, and that has a fatal outcome if this single modality does not work. No wonder my son was despondent. This is not 1935, Dr. A.M.
@Dr. karen miday It is true that most young people grow out of malapdaptive driniking – this usually occurs after college. Many colleges condone a culture of binge drinking. For those individual who continue to drink excessively outside of this culture, you have to be concerned. I do not pretend to know of your son’s story. Many people have successfully conquered additction through a 12 step program. It does work. Otherwise, AA would have been abandoned long ago. I will submit that AA is not for everyone. I will also submit that some AA advocates are stringent Bible thumpers who alienate addicts who are agnostic or atheists. This is not good. I believe there are more than one ways to skin a cat, so to speak. AA is a miracle for many. But we have to remain sensitive to those who don’t identify with the concepts and are searching for another means of getting well. Rational Recovery, Life Ring and other programs are options It may be true that some physicians who have found salvation through an AA program may have difficulty considering other options for individuals who do not identify with a spiritual concept of recovery. We need to remain mindful of that fact, be flexible and offer alternatives.
Dr. A.M. Well said. I wish my son’s PHP had offered another alternative.
If you are involved in the leadership of the PHP system, I hope you will encourage all to consider the options you have suggested, as well as harm reduction with MAT for those whose binge drinking does not negatively affect patient care.
@Dr. karen miday I am not but will advocate for all that you suggest.
@Dr. karen miday no doubt—
@Dr. karen shackelford I cannot imagine any treatment facility recommending a 12 week stay absent an addiction diagnosis or other serious health problem. Is there more to this story? Very sad and needs to be investigated.
I am only repeating what the deceased told me personally. Perhaps Dr. Carr can shed some light since he was the director of the MS PHP at the time and it was at his insistence that the evaluation occurred in Kansas.
In my state, PHP’s are staffed by people with no qualification in medicine or psychiatry, and their training is not made public, if it exists. PHP’s may have started to assist medical personnel, but they have evolved into yet another layer of administration. What is worse is the punitive referral of physicians and nurses who are deemed “disruptive”.
@Dr. Lore Garten I would strongly recommend that you consult with your medical board and express your concerns. If your PHP employs personnel who lack the requisite expertise to truly assist physicians, that is a serious problem.
@Dr. A M @Dr. Lore Garten Yes, well…hmm…so…hmmm
The PHP in my state investigated me after I complained about a physically impaired practitioner. What happened after that was a witch hunt that turned up untrue allegations. Rather than confirm the veracity of the allegations, the PHP coerced me to go into a treatment program, which I did not need, forced me to close my practice and in concert with the medical board, they suspended my license. There was absolutely NO due process and I spent over a year in a legal battle which cost me thousands of dollars. They also ordered me into a forced psych evaluation in a locked Psych ward at McLean Hospital. The results of the evaluation were favorable toward me. The ALJ ordered the case files sealed, charges vacated, and ordered that I be publicly exonerated. Neither the medical board not the PHP did any of these things. Instead, the false allegations were leaked, I could not obtain malpractice insurance and my career and reputation were ruined. To describe them as draconian would be too nice.
The above article is an abomination and a total mischaracterization of the truth.
That would be in Massachusetts with PHS complicit with BORM Physician Health Compliance unit (headed by corrupt Board attorney Deb Stoller and her 2 minions ) correct?
Have you spoken with state auditor Suzanne Bump’s office? They are planning a stat audit and need your input. Also file report with Governor Charlie Baker. No oversight at MMS and they have “point people” who block the usual complaint pathways. ( I.e. MMS ethics committee, etc.). The corrupt BORM members need to be exposed and removed by Governor Baker.
@Dr. sarah reade Thank you for sharing your story. I am so saddened to read of such an abomination. Why even hire counsel if, after all that suffering and expense and effort, your victory gets overturned by a system that can abuse you in perpetuity? Independent of what state it occurred in, I hope you filed a protest and a request for investigation by the state auditor.
I also well understand how utterly exhausting this regulatory ordeal is. With articles like these in Medscape, I am confident we are going to expose the gross injustices and nightmarish imprisonments caused by this so out of control system.
@Dr. Kernan Manion @Dr. sarah reade Many thanks for your empathetic response!!
@Dr. sarah reade I am so very sorry, Dr. Reade! These horror stories really get to me!
“No one expects the Spanish Inquisition”! (from a Monty Python skit)
Which is what we have the equivalent of here and now…
Dr. Carr,
You should reveal your financial conflicts – after your tenure with the Mississippi Professional Health Program came to an end, you moved into a similar position in Washington State before returning to Mississippi to create the Professionals Health Network with Alexis Polles, formerly of Pine Grove and instrumental in creating the new disorder of sex addiction. The Professionals Health Network is targeted at non-physician professionals. You have created a new niche market. Kudos. You’ve made a silk purse out of a sow’s ear.
@Dr. karen shackelford Dr. Shcackelford you are out of line. Dr. Carr did not fabricate an illness of sex addiction. Compulsive sexual behavior is now recognized among physicians – this has been detected because some afflicted physicians use hospital owned computers to view pornography on line during work hours. Hospitals are seeking remedies for this issue. PHPs and other professional organizations are not seeking out referrals or fabricating problems. Get your facts straight before you condemn physicians you do not personally or professionally know.
Hello Dr. A.M. I am curious as to how doctors who view pornography on hospital computers are a danger to their patients…or is it that they are a “potential danger.” I understand that their behavior does not reflect well on the profession, but it also seems to me that there are other more reasonable remedies than referral to a 90 day 12 step-based inpatient program. Perhaps the hospital might simply terminate their privileges? This is what typically happens to employees who engage in such behaviors. I don’t think it is at all reasonable to assume that pornography-viewing physicians are harmful to their patients, but it is certainly up to the hospital to set its one standards. Again, I am not excusing the behavior. I simply do not see how this behavior is equated with impairment. I think the concept of “potential impairment” is absurd as it cannot be clearly defined, and any condition…mental or physical….might qualify. Do we really need to be casting a net this wide? This is certainly not about protecting patients. Patients would lose far too many qualified physicians.
Dr. Miday, With all due respect, are you kidding? If a physician views pornography on a hospital computer it would suggest to me that they are out of control. What they do on their own time is one thing, but if they lack the judgment to confine their pornographic preference to personal time I would have serious concerns about their judgment and impulse control As a hospital CMO or CEO, I would not want to pay a physician to view pornography when my expectation is that they are spending their time evaluating patients, reviewing laboratory work, educating families and perhaps educating medical students and residents. You are assuming that such a physician would automatically be referred to 90 days of residential treatment. Not so. I for one would view this behavior as unprofessional conduct and provide serious warning. If the behavior persisted I would refer the physician to a PHP to rule out a sexual disorder. Absent a sexual disorder I would terminate the physician’s employment. No one is suggesting this correlates with impairment. But I can say with some certainty, if a patient learns that his or her physician is viewing porno at a hospital, that patient will request to be transferred to another physician.
@Dr. karen miday It is inappropriate for physicians’ viewing porn at work to be anything but bad behavior which should result in discipline of some sort by their employers, not anything more outlandish than that.
It is inappropriate for this to go to any PHP. Maybe a Med Board could view it as unprofessional conduct, that is not for me to judge…but I will say that it is reaching to say it is anything requiring a coerced 12 step program, much less coerced “rehab” at a facility with financial links to the supply link—the PHP.
Physicians are not fish to be fished for —to supply some private, expensive rehab program with bodies. Sad.
@Dr. Gail Hirschfield @Dr. karen miday You are suggesting that the uniform response each PHP has to any infraction is a 90 day residential treatment. How wrong. PHPs do not have financial links to treatment centers or medical boards. Give me facts to suggest otherwise.
@Dr. A M @Dr. Gail Hirschfield @Dr. karen miday They will be forthcoming and have been presented in other comment sections on the companion stories. These links. Some have already been presented here by other posters. Did you miss them?
Compulsive sexual behavior has been around forever. Only in light of large potential profits would anyone try to medicalize the problem. Sex addiction doesn’t appear in the DSM, which is a fairly low bar.and yes, I do know Dr. Carr.
@Dr. karen shackelford Why do you find it necessary to vilify Dr. Carr. These are cheap shots Dr. Shackelford. What have you done to have your license suspended? What can you do to have your license restored and be allowed to help patients?
Your assumptions are inaccurate, Dr. AM
@Dr. karen shackelford Ad hominems bloom, I see…when Dr. AM has nothing else to say for himself…
@Dr. Gail Hirschfield @Dr. karen shackelford I am only asking you a question. You have posted some vicious comments about people in the PHP camp that you don’t even know. So, give me some context Dr. Hirschfield to your criticisms. I sincerely want to know how a TX PHP did you wrong.
@Dr. karen shackelford What assumptions? It is online that your license is suspended. I am curious about how that happened and why you believe PHPs have been so destructive to you personally. And if so, why are you not seeking legal remedies.? What has a PHP or medical board done, unprovoked, to cause you so much misery? Because if you were simply minding your own business, practicing medicine to the letter of the law, then it would make no sense to me that you are notw restricted from practicing medicine. Either something simply egregious has happened or you are not divulging all the facts that would create a rounded picture of your predicament. You are quick to vilify, criticize others and not reveal what you did to contribute to your adverse situaton
@Dr. A M @Dr. karen shackelford My license was not “suspended.” I mailed it in. I choose not to participate in a system of coercion, secrecy, and lies. Thankfully, unlike Dr. Moffit, I am still alive and well. Perhaps you will be kind enough to reveal your identity. I have absolutely nothing to hide from. Nor do I have any need to explain myself.
@Dr. A M @Dr. karen shackelford Currently, some PHPs are going after Gays for sexual misconduct,..um…well, really, enough said!
They are making a very, very serious mistake in doing so. I will see to it that Gay organizations are aware of PHP misconduct, actually…actually, I already have sent Dr. Langan’t link out to some on this subject:
@Dr. Gail Hirschfield @Dr. A M @Dr. karen shackelford Again, a reckless accusation with no facts. Give me specifics. Which PHP is discriminating against gay physicians? If those physicians are engaged in sexual misconduct with patients, regardless of sexual orientation, they should be intervened upon. Reckless accusations which have no merit, leads to no credibility.
@Dr. A M @Dr. Gail Hirschfield @Dr. karen shackelford Did you read the article? The facts are right there! in the article!
@Dr. Kernan Manion @Dr Jesse Cavenar –Below are the documents on Teitelbaum and Skipper spanning the 1980s to 1990s. They had ben previously been reported as “personal correspondence” and removed but they are public documents and this was in error.
@Dr. Michael Langan Dr. Langon, How do you represent yourself as caring for physicians when you find a need to out your colleagues in the house of medicine? You cannot know all of the specifics of their situations. This is so mean spirited. It tells me a lot about your character. How do you expect to receive compassion when you are so vicious in your attacks of other physicians, physicians you do not personally know. Do you not care about the impact on their careers, their families, their friends? Don’t present yourself as some victim when you so easily victimize others.
Dr. A.M. I am curious as to why you do not post with your name. Your are critical of Dr. Langen’s commentary and yet will not openly endorse your own. Dr. Langen has been clear about his position on this matter. His commentary is well-researched. Admittedly, it does not reflect well on the parties concerned. That is not his doing. He is simply trying to hold people accountable for their actions. I believe he has a great deal of compassion for the many physicians who have come forward to share their stories of loss of career, professional status, income, and in my son’s case, life. The majority of these physicians do not have a paper trail like the physicians he is exposing. Speaking of victims, I hope you will read the many comments that are posted. I, myself, am simply trying to protect other docs from my son’s fate. I simply cannot understand why the entire PHP system will not endorse concepts of transparency, accountability, and due process. These are basic principles of American justice. I believe many careers and many lives would be spared.
And again, speaking of transparency, I know who Dr. Langen is. I would love to know who you are.
@Dr. karen miday Why is it so important to you that I reveal my name when so many others posting here are doing so with some privacy? Most of the physicians commenting here have a significant paper trail detailing problems with their medical boards and NOT PHPs. Please do your research. A google search goes a long way. I do not know Dr. Langan personally, but I have followed some of his blogs and he simply leaves the impression of a resentful, disgruntled, grudge-bearing angry man who deals with his personal misfortunes by attacking others. He has likened physicians to Nazis and psychopaths. In my view this is simply slander. If he has a problem understanding why he does not get a seat at the table of reform, he should recognize that he himself has alienated that opportunity by insulting various institutions, organizations, individuals in his blind rage. It is difficult for me to perceive him as being victimized by a system, PHP or medical board, when he has done so much to hurt other people. Dr. Langan is a psychiatrist and I would expect him to have more insight. Enough said.
@Dr. A M @Dr. karen miday I am posting with my name. Gail Hirschfield M.D. Furthermore, I live in Texas, and I plan to rally a march in front of the PHP building in the near future do make sure the Texas PHP has some accountability for its horrifica actions.
I really don’t get your point, Dr. A.M. Would you at least care to share some facts to back up your assertions?
@Dr. A M @Dr. Michael Langan How did he out his colleagues?
@Dr. Gail Hirschfield @Dr. A M @Dr. Michael Langan By posting negative social media information. This is cowardly and cruel. Dr. Hirschfield, good luck to you in any physician advocacy work you do. I hope it does not involve demeaning, slandering or engaging in other libelous behavior toward fellow physicians.
@Dr. A M @Dr. Gail Hirschfield @Dr. Michael Langan
I still don’t get it, Dr. AM , which means that many another reader probably doesn’t either. I don’t understand why he could be considered cowardly and cruel by you. He presented public information…just as you have about me and others posting here…am I to consider you cowardly and cruel, Dr. Anonymous?
BTW, who do you suppose is actually looking at these comments, Dr. AM?
Dr. Reade, I am sorry for your plight, but you omit other facts which are retrievable on line. The information I read would certainly compel a health evaluation. Dr. Langan, I also read information about your history and what I gather is that you lacked credibility with your medical board not the PHP. Drs. Manion, Shackleford, Hirschfield, Horiagan et al. when I researched you on line, there was plenty of information to suggest that interventions were warranted. You only point out the failings of medical boards and PHPs and you do not reveal your own decisions and actions that led to legal snafus necessitating medical board involvement. I will not detail the specifics because I am not in the business of humiliating people.
Dr. Cavenar, I have come to believe that the Dr. A you describe in your postings was in all likelihood, a patient of yours. You have done little to de-identify his information. If I am correct, you are exploiting your patient for your own selfish interests, namely to slander the PHP in your state. This would constitute unethical behavior. Think about your choices and motives and potential fall out. I hope I am wrong about this, but if I am right, you are engaging in unethical behavior.
Finally, Dr. Miday, I am so sorry for your loss. But you too focus on the evils of PHPs when from what I gather from your posts, your son had an alcohol use disorder and a comorbid anxiety disorder. PHPs do not kill physicians, illnesses do. Before you vilify the people who tried to help your son, research the PHP in your state, request a meeting with the leadership. It is possible that they have been instructed not to discuss the case by legal counsel. This does not mean they are not devastated by the loss of a physician as you are. devastated by the loss of your son. From your posts I also gather that he was under the care of a private psychiatrist. Has this psychiatrist conducted a chain analysis to determine what missteps if any occurred? In all likelihood, your son’s psychiatrist had more intimate knowledge about your son than any medical board or PHP.
What I understand, from my own medical society and state medical board and PHP, is that each state is different in terms of how PHPs are funded, what contractual relationships they have with medical boards and what medical practice acts (defined by state statute) dictate. Generalizing in this scenario is unfair and unproductive. Many of you have complained that you are not getting answers to your questions. What I have observed is that when physicians post comment with views counter to your negativity, you attack them. I also wonder if the silence represents a type of solidarity between PHPs and their participants to not qualify your allegations and sometimes slanderous comments with a response.
My recommendation is that if you believe you have been denied due process, mistreated, misdiagnosed, etc, you pursue remedies in your individual states. Engage a defense attorney well versed in matters related to medical boards and PHPs. Talk to leadership of your local medical society. Provide specific factual information about your individual case. Engage with regulatory bodies in a respectful manner. Slandering, demeaning organizations or individuals will quickly lead to disengagement. You can also contact national organizations such as the AMA to voice your concerns. But please do it in a respectful manner or your complaints will fall on deaf ears.
As an aside, I visited the FSPHP website to learn more about the organization. It lists every state PHP and in a transparent fashion, reveals how they are funded, how they relate to their medical board, what health conditions they monitor, the individual members of their PHP, how to reach them. It also lists publications about physician health, newsletters, power point presentations from annual meetings and research findings. Each state website lists supportive information for physicians. Maybe I am naïve but I don’t perceive this organization in the same way you do. I am fortunate to have not suffered from a potentially impairing illness, but I would not hesitate to contact my state’s PHP if I was diagnosed with an illness that could impact my ability to provide safe patient care.
While there may be imperfections, throwing the baby out with the bath water does not help our profession. I am old enough to remember a time when physician work hours were not restricted, when interns lived in a hospital and were forbidden to marry and when medical boards publicly humiliated physicians by posting their vulnerabilities on a wall of shame. I support any effort to humanize physicians, move away from a disciplinary model of public safety to one of early intervention and ideally primary prevention.
When you attack your professional colleagues by name (Drs. Carr, Skipper et al) you simply lose credibility. The house of medicine divided is no house at all. As I previously posted, rethink your approach. You can portray yourselves as antiauthoritarian miscreants by doing what you are doing, or you can reorganize with factual information and approach organized medicine in a professional manner with your concerns. Your choice. Dr. M
Dr. Alfonso M., there is nothing online that suggests a need for a “health evaluation.” You are dangerously close to slander and defamation.
@Dr. karen shackelford Likewise, he has misrepresented me in a derogatory way here. What do we call that, legally? I have requested that his post be flagged as offensive to us all named by him in his silly attempt to shame and humiliate us. Which is a demonstration of the very attitudes we protest and make us filled with justified outrage.
@Dr. A M Dr. Miday, I am truly sorry you had to read these comments.
Dr. A.M. To be clear, I have never characterized the Missouri PHP or any other PHP as “evil.” I have also never blamed the Missouri PHP for my son’s death. What I have stated, and will do so again, is that my son was in a state of near panic about losing his medical license and that his contact with PHP treatment groups, both inpatient and outpatient, reinforced this fear, as well as shame regarding his illness; Also that he was repeatedly told that his illness was inevitably progressive and that he would die from his illness if he did not adhere to a 12 step abstinence model of threatment. And, finally, that the PHP, by their own admission, advised him to not go to the inpatient unit at the Harris House in St. Louis, as arranged by him and his psychiatrist in a session earlier the day of his death, and immediately prior to his phone interactions with several folks at the PHP. This, I believe, was a serious clinical error, and likely contributed to my son’s death. Also, the director of the PHP, when questioned, stated that there would be no internal review regarding my son’s death. I was profoundly disturbed by this. Additionally, I believe that whatever “issues” my son had were compounded by the shame subsequent to having been removed from his training program for a period of 3 months. I believe he would have fared much better in a local, outpatient program. I also believe, had he not been a physician, he would have been treated initially in such a program, as this is typically how addictive illnesses are treated, at least initially. His many colleagues at Washington University/Barnes Hospital willl vouch for the fact that he was never impaired in a work setting and was seen as a superior clinician.
If anyone in the Missouri PHP was devastated by Greg’s death, they have a strange way of showing it. I have yet to receive a note of condolence from the clinical director, the medical director, or anyone else employed there. This, Dr. A.M., speaks for itself.
In response to the ASAM reply by Dr. Goldsmith.
Dr. Goldsmith, Have you been through the program? If you were, how were you treated?
By now more than a 1000 replies to the comments regarding PHP’s on Kevin MD, Medscape, and Disrupted Physicians have come forth.
Stop. Listen. Sit quietly and contemplate what these Physicians are sharing with you and each other. Do not go into defense mode so quickly. I need you to not be the ASAM director for a few moments I need you to listen to the other whom are screaming for help. I need you to respect what these Physicians have been through and are sharing with you. You do not know it all. None of us do. You do not know the pain and suffering these Physicians have been through. You are refusing to hear them. They are sharing their pain with you but you are too quick to shun them. Please hear them, please listen to their stories. Call them, reach out and find out the truth.
This many professions do not reply to a subject with this many heartfelt responses for you to tell them they are all making this up. Better yet why would this many people make this up? Have you thought about this? Physicians are very busy people. They do not comment unless they are strongly compelled to.
How is it that the Florida PRN would take on a person so hated by the patients that he treats that the very patients have started a stop Dr. Teitelbaum.
http://www.stopscottteitelbaum.com/victims Do you really think this many people would be complaining about this man and the PHP’s if it were not true?
The majority of people whom have had the addiction gene turned on are thrilled to have recovery. No one is saying everything the PHP’s has done is wrong. But there are things that are being done you are not aware of. They have done things wrong. You would remove a Physician in need of treatment out of his duties. Some of the Physicians on the PHP teams need help.
These professionals responding to your letter are crying out and you ignore them, you tell them they are wrong. This many professionals cannot be wrong. The patient needs to be heard. Listen, they are telling you what they have suffered through.
As for the poor victim whom is suffering from PTSD from her treatment by Dr. Tietelbaum for addiction and then left the country. Do you not have a heart? Are you not capable of hearing their pain, their suffering? A good practitioner listens.
Most patients if allowed to speak will tell you what is wrong with themselves and they are generally on target. You cannot throw everyone under the same title of “addiction. “Oh they are just addicts still behaving like addicts.”
The responses to your letter are from Professionals and some Professionals with a mental health issues, they are not “just addicts”. Show these folks some respect! Some of them have never been addicted. And those with addiction issues never stopped being professionals. They are telling you something isn’t working. So many are begging to be heard and asking you for help!
Please do not just blow it off.
Why don’t you actually contact these professionals and find out what it is they are speaking about. Listen to their evidence.
I was raised by a father that always said one is innocent until proven guilty. What will it take for you to hear them? You tell them they are not being honest without firsthand knowledge of their experience. So many wounded healers want to share their proof of what happened to them with you? Why is it you that you are not giving those injured by other Physicians some of your time? Is it not possible for you to investigate the pain that is all over the place on this issue? Do you know what the Jewish people felt like when people say that the terror in the concentration camps did not happen? How long will you wear your blinders and ear plugs without responding by investigating all the noise? I beg you to listen to these people. I implore you. You have more power than they do. Do what is right. Do what is honorable. Do what you are being led to do. Find out what all the noise is about and investigate what is actually going on here.
Why not reach out and instead of being defensive, delve into the problem. There really is a problem going on with the PHP’s and Medical Boards.
There is a problem with Dr. Tietelbaum. Hr is the one who by definition is impaired!
Why not contact some of the people on the stop Dr. Tieltelbaum website, Medscape, Kevin MD and Disrupted Physician and speak with these people. Talk to all those that have actually been to him for treatment and listen to what they are saying. We do not need further issues with the PRN or the PHP programs in this country. They need to be cleaned up and good people brought in to replace the corruption that is going on inside of these programs. Please help us Dr. Goldsmith, don’t turn your back on us. Those whom have been harmed need your help. That is why they are crying out. You have the chance to be the HERO.
Thank You
Melissa Wiggins.
@Melissa Wiggins You speak for me and make so much sense! I hope you are heard by ASAM, I truly do. Doubt it, but I hope so. If these people can’t reform from within sufficiently, then there are plenty of us who will press forward with our concerns. To do otherwise would be to abandon the vulnerable among us. Thanks!
I haven’t read comments yet, though I did read this article which is full of outright lies, such as the one that physicians can get an outside opinion, etc. —patently absurd!
The PHP program concept is a lofty ideal, and I and many here agree with the need for a healthy and healing place doctors can turn to for good medical care and even for monitoring in a rational and reasonable, HUMANE way, but in fact PHPs currently are dismal failures at curtailing physician suicides, a fact stated by Dr. Gunderson, the President of the FSPH, acting as the spokesperson for the Federal Society of Physician Health Program, when she presented her reply or response to the original Medscape article which is now curiously closed to any further comment, “Do Physician Health Programs Do More Harm Than Good”. She stated that the physician suicide rate has “remained the same” (rather than that it actually increasing, which was her point, which in and of itself is a demonstrable lie). So, in no way are physician suicides declining, for any reason, and most especially not due to the palliative or restorative effects of the PHP organizations. In fact, they are on the rise. 400 last year—a whole, entire medical school.
I rest my case in this serious matter of physician suicide, PHPs failure-if not culpability-in that regard, and in fact, failure overall to promote “physican health” at all, quite the converse. I can refer you to another Medscape by Dr. Pamela Wible in which she asks the question, “Do PHPs contribute to the increase in physician suicide”? an open-ended question which invites the conversation concerning the possibility that PHP programs have actually resulted in promotion of physician suicides in many, many cases have worked to push physicians over the edge, making them doctor-kiillers. Her text suggests the affirmative, as do the many horror stories which showed up in the comment section (also closed), which actually frightened me, as docs thinking about suicides actually weighed in—and yes, they said the actions of their PHPs pushed them in the direction of killing themselves. I am working presently on this issue and will bring you more information about it in the near future—the corruption of the PHPs which have turned them into Physician Destruction Programs, when they could be such a force for benevolence and healing of our beleaguered and sometimes ill physicians.
So, I don’t want to overwhelm the reader with demonstrating to you one lie after another presented above, but here are two outright lies, facts available to the ASAM author who doesn’t want to bother himself with the nicety of having facts at his disposable, repeatedly presenting his pontifications as facts, when they are, in fact, his opinions, and opinions as we all know are like certain parts of the body—everyone has one.
When a person tells lies, not misrepresentations, but outright lies, how can you honestly believe anything that person has to say?
Gail Hirschfield M.D.
@Dr. Gail Hirschfield Dr. Hirschfield, you do not have factual information to support your deadly claims that PHPs = Dead Doctors. How absolutely reckless for you to post such a comment. I researched you on line and what I found was what you posted yourself. You had a driving citation for driving under the influence of alcohol. In the end, you were exonerated because your BAL was below the legal limit. However, it is not unreasonable for your medical board in Texas to want some reassurance that you did not suffer from an alcohol use disorder. I am speculating here, but I bet your medical board, upon knowledge of your legal citation, referred you to a PHP for an evaluation. I can only imagine that this felt over-the-top intrusive and was stressful for you. But please try to take a seat at the other end of the table. The medical boards are charged with protecting the public. While it may have been inherently stressful for you to undergo such an evaluation, in the end, you were cleared and allowed to resume the practice of medicine. As physicians, we are held to a higher standard and our practice of medicine is in fact a privilege and not a right. PHPs can and do advocate for physicians who exercise a “lapse in judgement” and in fact have no impairing illness. I have to believe that your angry response to your experience reflects (understandable) fear and shame related to having to answer to an authoritative body.
@Dr. A M @Dr. Gail Hirschfield Again, your facts about me personally are in error. but thanks for sharing what is out there on the internet. How kind of you!
Actually, I am influenced by the horror stories you read here I am saddened by physicans dying, pushed over the edge by both medical boards and their evil twin sisters, their PHPs.
I have no current engagement with any PHP, and I am putting out my name in public, to fight what I believe is a deadly evil…an epidemic of the worst kind…worthy of CDC investigation…I am on the verge of retiring and will not let this scourge upon our profession rest, nor will many of those you see here on this site.
“What Killed Dr. Greg”?
Again, PHYSICIANS’ LIVES MATTER
@Dr. Gail Hirschfield @Dr. A M How did a PHP damage you Dr. Hirschfield? You drank and drove. To be fair, your BAL was not above the legal limit but it did cause you to be ensnared by your medical board. How did the PHP in your state harm you?
@Dr. Gail Hirschfield @Dr. A M Dr. Hirschfield, you yourself posted your story and those are the “facts” I am relying on. How kind of me? You have accused PHPs of killing doctors. How utterly generous is that. Don’t be a victim and a hero at the same time.
@Dr. A M @Dr. Gail Hirschfield Of course I have factual information! You can read it here for yourself, and you seemed to already have read about how PHPs pushed physicians over the edge and caused them to kill themselves! There are two here in just the last few comments, and YOU responded to them! could you please wipe off your interior glasses? do I have to say the adage—“there are none so blind as those who WILL not see”?
@Dr. Gail Hirschfield @Dr. A M Again, you have no facts to substantiate your claims that PHPs cause doctors to commit suicide. This is simply egregious for you to purport. You simply want to vilify PHPs and have no knowledge of the literature pertaining to physician suicide. The truth is we do not know what unique risk factors are. This demands attention and research.
@Dr. A M @Dr. Gail Hirschfield I rely on the facts of the horror stories presented here by others. The facts are not open to misinterpretation.
See Dr. Wible’s requests for information above.
@Dr. Gail Hirschfield I hope you can back up your allegations with facts. Otherwise you are slandering your colleagues in a reckless and insensitive manner. I will look forward to your facts.
@Dr. A M @Dr. Gail Hirschfield I experienced their horrible tactics, first hand. WPHP is in bed with the state licensing Board as well as the Washington State Medical Society. It is all dirty.
@Dr. sarah reade @Dr. A M @Dr. Gail Hirschfield You make these allegations, but where are the facts? Tell me more.
@Dr. sarah reade @Dr. A M @Dr. Gail Hirschfield The medical board responded appropriately to your situation Dr. Reade. Again, I will not post the details, but your choices and behavior set in motion a series of reactions that you now resent………………
I forgot to add that after my experience with WPHP (Washington) and Greg Skipper, I was diagnosed with PTSD. I am still in treatment.
@Dr. sarah reade I hope you are getting the help you deserve Sarah. PTSD sucks and it is hard to overcome. God Speed.
@Dr. sarah reade I am on facebook…please feel free to look me up! I am so so saddened to read your history with your innocent entanglement with this evil PHP group and its deadly groups it refers to for financial gains. You are not alone, so please realize that.
Washington is very bad. I hope another Washington doc writes on this site! I will see if I can find his webpage about that…have you read anything on the net? I will look it up in the closed comments on the other Medscape articles,.,find his name and maybe contact him through his website he linked to there.
What do we want from the PHPs?
” transparency, accountability, and due process” —from Dr. Miday’s post below.
just like every other citizen of this great nation. ….Really, is that too much to ask? But right now, this is NOT the case with the PHP system. Quite the opposite.
The consequences of not obtaining basic fairness, and justice is that physicians involved with PHPs will continue to kill themselves or be devastated as we read here in this comment section.
PHYSICIANS’ LIVES MATTER
@Dr. A M, please keep commenting. See the attached blogposts regarding “TT Wilson”
http://disruptedphysician.com/2015/02/21/rantings-from-the-bully-pulpit/
http://disruptedphysician.com/2015/04/05/tt-wilsons-php-playbook/
As the vocabulary, grammar and authoritarian yet vacuous pronouncements are remarkably similar to yours I am wondering if you are one and the same? Readers what do you think? Applicable comments regarding TT are below and I present the same challenge to our anonymous Dr A. M. –namely, if he wishes to provide a rebuttal to any of the documentary evidence or substantive concerns here (or in my blog) then I challenge him to do so and if he can I will not only refrain from further commenting and apologize but delete my entire blog forevermore. Fair enough?
I have read through your multiple comments left here Dr. A M. and fail to discern any specific points you have raised. If so please clarify as all I see is the same rant–an angry symphony with just one note. -ML
“The three e-mails below were received within a twenty-four hour period from a physician supporting (and in all likelihood involved in) drug courts and physician health programs (PHPs). E-mails such as this are invariably anonymous and I usually drag them right to the trash where they belong but the trio below provides valuable insight into the mentality of those involved. And for that reason I am posting them as they were received.
Under the nom de plume of “TT Wilson” the author presents non-sequitur and fallacious logic to promote drug courts, PHPs and the sanctification of an illegitimate and irrational medical specialty.
He presents either/or logical fallacy and false dichotomy. You are either with us or against us! He appeals to professionalism yet his words show he has no inkling of the true definition, resorts to simple-minded cliches and meaningless platitudes and then sinks into ad hominem attacks on my blog and then me.
Ironically he accuses me me of ranting in a rant!
He is a prototypical example of the sham-artist physicians typically involved in these programs–an authoritarian paternalistic know-it-all who can only rant under the shield of gang-stalking power or a shroud of absolute anonymity.
As I have said time-and-time again if any factual errors exist in my blog I will not only remove them but remove my blog.
So I am going to make this offer to “TT Wilson”–if you wish to provide a rebuttal of any of the documentary evidence I provide in my blog herein then do so now. If you can I will delete the whole kit and kaboodle. Simple as that.
You Sir are an incompetent and a coward. If not then prove me wrong. I challenge you to reveal your true identity. Let’s level the playing field a tad on this. It is easy to present an opinion while cowardly hiding behind a veil of anonymity. Let’s see if you have the courage to debate this publicly.
I won’t be holding my breath on this one.”
Dr. A.M.
I don’t believe that you are an otolaryngologist, but believe instead that you are a family practitioner who has had one year of fellowship in addiction medicine. I believe I know who you are. I cannot understand your reluctance to clearly identify yourself and have a legitimate discussion of the issues instead of hiding behind a false identity, except it would become clear to all that you have a vested interest in supporting your position.
Since you identify and present yourself as a substance abuse expert, let me ask you this question:
How do you make a diagnosis of a condition in a patient when the patient has none of the signs or symptoms of that illness and is found by five substance abuse experts to not meet the diagnostic criteria for the illness with which he was diagnosed by the PHP? Further, the psychologist whom the patient was mandated by PHP to see agreed that he didn’t have alcohol abuse.
How does one do that, Dr. A.M? Does one just make up a diagnosis and then stick with it come hell or high water, all common sense and diagnostic criteria to the contrary? After all, the PHP personnel claim to have sovereign immunity so that they cannot be sued for malpractice. In NC, as you probably know, there was an attempt to get a bill through the state legislature recently—since the NC State Auditor’s audit of the PHP—stating explicitly that PHP personnel were immune from liability. I would venture to say that if the PHP personnel didn’t have alleged sovereign immunity, there would be malpractice litigation falling out of the ceiling on them.
I am amazed by some of your comments, Dr. A.M. “PTSD sucks and is hard to overcome”. Really? Now that is a newsflash. “I have to believe that your angry response to your experience reflects (understandable) fear and shame related to having to answer to an authoritative body”. How can you possibly state this—or is it just a guess? “It is so mean spirited. It tells me a lot about your character”. What do you see as “mean spirited” about a posting of material that is in the public record and which is important for those following this discussion to know? “….leaves the impression of a resentful, disgruntled, grudge-bearing angry man who deals with his personal misfortunes by attacking others”. Oh, please. Dr. A.M., please leave the psychiatry to me, as I am a certified psychoanalyst and a certified psychiatrist with over fifty years experience. Stick with your family practice and substance abuse practice.
I would really enjoy having a meaningful discussion of the real issues with you. Perhaps we could meet for coffee or dinner as we live within twenty miles of each other.
I would love to hear from any of the thousands of physicians whose lives have been “saved” by PHPs on this comment section. Anyone? anyone? Buler?
Over and over this ASAM article refers to the “potentially impaired physician” as needing to be in the PHPs…that is chilling! How does one diagnose someone as “pre-impaired”? do Gays qualify, as they have such a hard time of it, so they are at a higher risk to become “impaired”? or fat people like me, because we swallow our emotions? how fat? what BMI? or old physicians because they have outlived their ability to think straight? how old? People with beards, men mostly, because they are surely covering up something and want to appear more menacing for some personal power gain? or? really, what are potentially impairing conditions? For that matter, what is the definition of “impaired”, exactly…being drunk and dropping a baby? I would say that is a no-brainer, but what about a DWI at a time not engaged in clinical duties? Re this silly Blue Print self-serving and jacked up study, if you filled your Blue Print study with those not really impaired, of course your rate of abstinence was high! They weren’t addicted in the first place! and of course you forgot to mention those who dropped out because of suicide. Where was the control group? Is this study reproducible? That doesn’t really matter to me and many of us, though, as it was a propaganda study to begin with.
Well, look, I can speak for the pre-impaired, as it turns out to be any and every physician who is still alive. So I qualify. But what about those pushed over the edge, and I am gathering data at the present as to how many were involved with their Boards/PHP programs? Who speaks for them? Certainly not the ASAM and sister organizations, like the FSPHP who deny their obvious culpability in these deaths, even though this was the proported reason (from the ASAM response above) for the formation of the PHPs and its FSPHP organization in the first place, the proof being that suicides have not declined, and in fact have risen to alarming rates…400 a year lately, 400 physicians each year coming to the conclusion that life itself wasn’t worth it.
Tell me what you have done, ASAM, about this deadly suicide problem. Of course, a dead doctor can’t pay the rehab centers and PHP dues, which may be why you are speaking of casting a wider net now to gather in the pre-impaired, because those truly impaired and desperate have a sad way of dropping out of your clutches.
Medscape encourages debate on its commenting forum but please note the following policy:
Medscape’s commenting platform provides a forum for physicians and healthcare professionals to share their thoughts on those Medscape articles for which the platform is enabled. We welcome your comments on these articles -both supportive and critical- and we value the communication that ensues. We do, however, require that you be considerate of your fellow Medscape users and refrain from posting comments that contain profanity, harassment, advertisements or any other content that is prohibited by the MedscapeTerms of Use. We also discourage excessively long and repetitive comments. The Medscape moderators review comments to ensure that they are consistent with this Guide and the Medscape Terms of Use. Personal attacks on our staff, authors and other commenters will be rejected.
This is from Dr. Langan, and I think it bears repeating, or at least, he speaks for me here:
“To be clear, doctors who are impaired by drug and alcohol abuse need to be removed from practice to protect the public and receive treatment; doctors who are abusive to others or engage in behavior that threatens patient care need to be held accountable for their actions; and doctors who are cognitively impaired due to dementia need to be removed from practice and evaluated by the proper specialists. If a diagnosis of dementia is confirmed then they need to be removed from practice.”
What is called for is “transparency, accountability, and due process” of any organization taking on the tasking of defining who is impaired, who is abusive, and who is cognitively impaired. And that is what is not happening now. And that is unacceptable, and in fact, destructive and deadly for our American physicians…the “good docs”.
Curious if there is any way to find out the numbers of physicians in PHPs at this time and the total numbers who have been treated and released back to practice vs. those who have “failed” treatment. Also would like to know numbers of suicides while under PHP treatment. Is this information available? I have spoken previously about my concerns regarding an increased suicide rate in PHPs. http://www.medscape.com/viewarticle/850023
I understand doctors have been helped by PHPs and others have been harmed. We have no way of knowing true numbers without some transparency of data. Where is this data housed? Anyone know? A scientific approach to discussing this topic with facts would be most useful at this juncture.
@Dr. Pamela Wible Still, Dr. Wible, if you “treat” a physician who doesn’t need any treatment of any sort and return them back to practice, I would say you could game up a pretty good track record! Also, those who “failed”, well they would either have to stay longer in PHP or be turned over to the Boards for license revocation, or take themselves out, way too often the case—well even one physician taking this route is too many.
In response to Dr. A.M.
I am very troubled by what I see as your widely dispersed insensitive and even ad hominem attacks toward those who have leveled legitimate criticism of the PHP program in these comments. Whatever you may think of commenters’ posting of their particular stories, and even of one commenter demonstrating the deeply problematic history of several of ASAM members’ own board disciplinary proceedings and severe drug histories, it does not give you the right to personally attack these commenters, especially doing so behind the shield of anonymity.
Even more troubling, you’ve done this specifically in light of several of these commenters recounting of what they perceive as their profound abuse by Boards and PHPs. Do you contend that you really know their cases from these various states and can so casually and globally dismiss them? Your scolding tone, telling them that they got what they deserved, is from my perspective akin to a therapist shaming a rape victim and telling them that they got what they deserved. It is deplorable and constitutes nothing less than psychiatric abuse. Is this the way you practice? Are you an ASAM member? Do you perhaps run a PHP preferred treatment center? If so, and if this is characteristic of your treatment approach, I would be very concerned for the patients’ well-being.
Since you seem to insist specifics in each of your retorts, witness this: “PTSD sucks and is hard to overcome”. Your reply smacks of insincerity and condescension. This after someone has indicated the extent of abuse they’ve suffered and is tentatively coming forward to tell their story. It is especially vindictive and sadistic in nature considering your having shamed the physician earlier.
Yet, in each of your responses, you entirely beg the question of alleged unfair or inappropriate treatment by their Board and PHP and proceed to attempt to shame each of them further.
You then provide a glib response essentially advising people to get an attorney if they feel they’ve been wronged. Such an attitude exemplifies the refractoriness of this system – you presumably representing it – to critical feedback and to change.
While it is not my goal to compel identity disclosure, it does concern me that you seem to adopt positions that mirror the very PHP model embraced by ASAM and FSPHP, positions that none of the leaders of these organizations has the temerity to take ownership of. Further, it suggests that the authoritarian scolding and shaming nature of your comments exemplifies the very demeanor of the organizations you seem to so fully endorse.
Many physicians over the span of these articles are clearly expressing their perception that they have been profoundly abused in the medical regulatory system and further misdiagnosed and mistreated by their PHP. Some contend that this misdiagnosis has been intentional, and that they have been systematically routed – again entirely deprived of medical due process – into a preferred network of extremely costly “treatment” programs run by ASAM profiteers who then torment these misdiagnosed physicians, deplete their bank account and shipwreck their careers.
What do you make of the problems being expressed here? You seem to believe that none of them has validity and that, if I were to paraphrase it, “everyone here has gotten the treatment they’ve deserved – by their Board and their PHP – because they’re nothing but a bunch of reprobates.” You’ve manifested no willingness to consider any of the substantive issues being alleged, namely that a very significant number of physicians are enduring great miscarriage of justice at the hands of their boards and that a significant number of physicians are being not only mistreated but HARMED by their state PHP acting in concert with their Board.
A number of us feel that the sheer scope and seriousness of these alleged PHP abuses , of which I suspect we are only seeing the tip of the iceberg, constitutes a veritable public health emergency. And it’s an emergency that refuses to be addressed by individual PHPs, by FSPHP and by ASAM and further can’t be addressed by Medical Boards because most PHPs are not duly licensed as legitimate medical corporations which should fall under the Board’s jurisdiction.
What are your suggestions as to how this might be addressed?
If you can’t direct your attention to these system-wide concerns, Dr. A.M., and all you can do is make ad hominem attacks and further traumatize those who have already been traumatized, I would request that you remove yourself from the discussion in order, as you might put it ,“to restore integrity to the house of medicine.”
There are profoundly serious problems being described here. And many here are seeking respectful dialog, prompt resolution of critical problems and collaborative engagement in examining and re-designing a PHP system that is safe and effective, one that is compassionately geared toward authentic treatment is properly overseen and fully accountable.
@Dr. Kernan Manion Yes, many of us are calling for:
Transparency, Accountability, and Due Process
of the PHP organizations, three basic tenets of civilized and democratic organizations. Fairness and Justice…words worth fighting for…
To Dr. A.M., Dr. Goldman, and Dr. Carr
The whole concept of “potentially impaired physicians” is so asinine and ludicrous
it is difficult to even comment on it. When four psychiatrists from around the state of NC met with the Medical Director of the NCPHP to express our concerns about the functioning of the NCPHP, the Medical Director stated very clearly to the four of us that a patient had to meet the diagnostic criteria found in the Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association in order to be diagnosed with a mental or substance abuse disorder. We all agreed. When confronted with one case in which the patient met none of the diagnostic criteria from DSM, according to five substance abuse specialists, and yet was diagnosed with a disorder and detained in the NCPHP for thirteen months at a cost of $94,000 in time and money, the Medical Director was unable to explain it. There was absolute silence and a “deer in the headlights” look.
Now we hear this concept of “potentially impaired physicians”. As others have stated, please tell us about this “potentially impairing” concept, and what things are potentially impairing in a physician. It appears to me that the idea of a doctor drinking alcohol at all is considered “potentially impairing”. This is a ridiculous notion with absolutely no medical or scientific underpinning. Many people in the world drink alcohol almost daily throughout their lives with absolutely no problem in the short run or long run.
The silence of Drs. Goldman, Carr, and Dr. A.M. is indeed troubling. As you three are the acknowledged experts, please respond and explain this Gordian knot.
To Dr. A.M.
I note with interest that you have listed on the Medical Board webpage in a description of your practice that you do:
Addiction Medicine
Addictionology — as your Primary Practice
Aerospace Medicine
Alcohol and Drug Abuse
Anesthesiology Pain Management
Family Medicine
Psychiatry
Yet, it appears to me from the training that you have listed on the Medical Board webpage that you had one year of surgery residency, a family practice residency, and a one-year family medicine/addiction fellowship.
It appears that you have had no formal psychiatry training, and yet you list that you do psychiatry. Really? What type of psychiatry do you do? It is amazing that you could practice psychiatry with no formal training. I have had eight years of formal training in psychiatry and I still find it very difficult to practice in a manner that I find acceptable to my own standards.
I would never make a diagnosis in someone who I had not examined, but some observers might question whether this is extreme grandiosity, malignant narcissism, adolescent omnipotentiality, or some combination of the three.
My question remains on the table and unanswered: How do you make a diagnosis of an illness when the patient has no signs or symptoms of the illness and meets none of the required diagnostic criteria?
It might be helpful for readers to know that you are “Director of Addiction Medicine and Recovery” and are on the “Board of Directors and deeply involved in all operations of the rehab center” at a treatment facility. If this is not correct, please so state and I will stand corrected.
Many others and I await enlightenment from you on these questions.
@Dr. Jesse Cavenar Or someone with deep pockets to fill…hmmm, why does that not surprise me? I will say that the Aerospace medicine credential seems right on the mark, though.
Dr. Cavenar—please let me remind you that all that is necessary for rounding up physicians “needing” a treatment program is that they might be potentially impaired! (and have some sort of funds available)…so you don’t really have to have a diagnosis per se…that is much too fussy! just look like you might have a diagnosis to someone or another around, maybe the building superintendent, not that I am making any sort of disparaging references to that honest worker!
Those who work within the FSPHP and the “preferred” centers get special treatment “outside” the usual channels. During Dr. Carr’s tenure he has allegedly been through treatment 8x for relapses.
@Dr. L N — 8 times! Wow!
@Dr. L N What sort of preferred treatment? Could you elaborate? For instance if their preferred treatment, and some have quite an addiction problem, works for them, and it is more humane, then can it be offered to all who need it? Substance addiction is a medical problem and needs cutting edge treatment, as it is devastating, but the methods to treat those suffering from it must not be barbaric, worse than the illness itself!
I think those running these programs, certificates or not, use cookie cutter methods, old school, and these obviously are deadly “solutions”.
If the special treatments are effective in working towards keeping the illness of addiction under control, then they should be applied to all who need them, right? Of course, the fact that this doc had to go to treatment eight times sort of demonstrates maybe that these special treatments aren’t so great, but he obviously has quite a time with his genetic illness.
@Dr. Gail Hirschfield @Dr. L N It is “special” treatment rather than special “treatment.” Those within te FSPHP are “protected” and when they “relapse” they handle it internally and the boards allow it. They have essentially been given carte blanche freedom
If it is indeed 8 x. I would say the special treatment is not working but the most important point is that, if this is indeed true it is 8 chances more than the doctors posting here got and their problems ( if they even have any) are small potatoes compared to this. How many chances did GC give those monitored in the WA program? Zero. And I know of several suicides of food docs while he was in charge.
That should read “good docs” rather than “food docs”
@Dr. E B Ok, so you are clearly saying here that you know of several good docs who killed themselves while this very ill physician who had to go into some sort of “special” treatment x8 (which could have been “no” treatment, but a washing of his deadly personal illness under the rug—boy, THAT really helped him!) was in charge of the Washington PHP…
so an ill and struggling doc was put in such a powerful position? that in and of itself is shocking. The outcome was physician deaths…in this case a PHP was implicated or even caused docs to kill themselves. I don’t see how anyone can now dispute the malignant effect of PHP programs upon physician lives. It IS an urgent public emergency, an epidemic of physician death and morbidity, destruction.
Look: PHP=DEAD DOCS
Look: PHP=PHYSICIAN DESTRUCTION PROGRAM
Look: PHYSICIANS’ LIVES MATTER
Look: 400 PHYSICANS KILLED LAST YEAR
We have factual proof of all of the above. We who speak out here have no rebuttal.
I saw a sign that said “Why doesn’t somebody do something about this? But then I realized that I AM somebody”!
I am someone speaking out no matter the cost to me in retaliation, in retribution, or threats of same. I am a practicing physician with much to lose. I have a current license, and I take care of the indigent here in Texas. I have no actual dog in this dog and pony show, except that I care and literally can’t stand by while these horrific injustices continue to occur when there are clearly better ways, and it fact, some easy fixes, as we have seen from a poster speaking up for Maryland’s program.
The time is now, before another physician’s life is lost. More than one physician a day kills themselves. 400 last year.
A friend, an OB/GYN, in one of these PHP’s who gained some weight, was mandated to attend Over-eaters Anonymous meetings, to her regimen of therapy and daily 12 step meetings for addiction to sleeping pills….she balked and they took her license, essentially because she was a bit too chubby. They bullied her in an inhumane way, and lost a valuable physician in a time of “shortage”. Careful…big brother can happen to any of us
The problem is not PHPs but the current individuals running them under the FSPHP and anyone reading the now over 1000 collective comments can see that clearly.
Need to remove the power from FSPHP state by state and remove the specific individuals who are allegedly committing civil and human rights violations and engaging in misconduct while investigations take place.
. An ombudsman system needs to be set up immediately while this is investigated. One of the arguments that the FSPHP uses is that they are ” the only game in town.” Here’s new for you- they are not. Plenty of competent ethical docs out there willing to work transparently, with oversight and without conflicts of interest.
Physician health programs: the Maryland experience.
Platman S, et al. J Addict Med. 2013 Nov-Dec.
Show full citation
Abstract
BACKGROUND: This article briefly summarizes not only the history of physician health programs, including their singular success, but also their struggle to maintain the ethical integrity of the programs, their appropriate autonomy, and the privacy of physicians enrolled in them.
METHOD: We review the history of the Maryland Physicians Health Program, how it initially developed and was funded, how the program became funded by the state, how this ultimately caused serious problems, and how these were eventually resolved.
RESULTS: Maryland was able to achieve a 2-program solution that protected both the voluntary participants while meeting the needs of the state licensing board for participants mandated by the state licensing board. This result has been well received by both the physician community and the state licensing board.
CONCLUSIONS: How the problems were solved and the ultimate agreement provide a model for others to use.
@Dr. Eliza B I asked previously if anyone knew of a program that was humane and worked to protect the public, and I was directed to the Maryland program That needs to be explored.
Yes, what is needed is common decency, civility, fairness and justice. What we have is an out of control barbarism.
I was a victim of human rights violations committed by the PHP farmed out the group called Maximus. While in the “Diversion program” with 18 month clean sober, over 130,000 invested to date, I fractured and dislocated my shoulder. When arriving in the ED I told the MD of my circumstances and requested a drug test as part of my in addition to standard radiographs. The ED MD ordered IV pain medication right away seeing my pain. I refused, until I could reach my “diversion nurse counselor”. The ED doc consulted Pain Management and Ortho given the added level of complexity. Ortho advised that they immediately give me dilaudid and place my fractured shoulder back in socket as my hand was numb and my pulses were weak., then I be admitted for surgery. When I finally reached the PHP monitor, her she told me that if I “take anything other than tylenol ( including for surgery)she would have my license” My team of 4 physicians now at this point( a hospitalist, ortho, PM and ED) all agreed that this was ill advised and I must have my shoulder placed back into socket immediately. That assuredly, this nurse knew not what she spoke and as soon as Monday morning came and they could contact the medical board….I would certainly be vindicated”post-procedure”, as even my contract read,that “medical care recommended by a reasonable licensed physician could not be prohibited” by participation in the program. I let the orthopedist, give me dilaudid and reduce my shoulder. I was admitted to the hospital for one week, while the Orthopod tried to induce me to have the surgery. Pain Management managed my acute pain, with full knowledge of my situation. All the doctors tried to contact the medical board to tell them of my unique surgery. That I should not be kicked out of the program. And, I should have the surgery I needed. The medical board took my license. Upon discharge from the hospital, the the medical board detectives came to my door to inform me, that I couldn’t work. I knew I could not even get myself dressed. When the board detectives came to take my license I had my hospital wrist band on one hand, and a wrist band circulating around our beach community of Ladera Ranch, for the little girl whom I was just featured in the newspaper and on TV for saving her life. They told me I was a danger to the public. My life fell apart. It has never been the same. I had already paid some 130-160,000 in fees to the PHP, and related expenses, even though I “had a strong case to fight the board” as one attorney said. I had no more money left. They had taken everything from me. My life was over. Suicide is something I still think about as I try to piece my life together. There were human rights violations occurring. There were anesthesiologist in Diversion forced to have “back alley” surgeries while in the program, at their friends surgery centers, using diprovan, as it wasn’t checked for. If you had a minor surgery or God forbid a situation such as mine….you were kicked out and lost everything.
@C G I am horrified to read this and am so sorry for your plight. Many here have, as you can see on this and related Medscape and KevinMD articles, similar abuse stories. I hope you will use your own tragic experience to fight to confront this programatic insanity so that no more docs will have to face the same sort of Kafkaesque nightmare.
I strongly agree with Michael’s call for the emergency creation of an ombudsman system. There needs to be an emergency go-between who is going to serve as a sensible and informed link between the licensee who’s in a monitoring contract and the PHP. It would certainly seem to be in FSPHP’s best interest to institute such.
It would also appear that the person who threatened you with (and then acted on) active anti-advocacy for your simply following your entire team of doctors’s advice in a surgical emergency ought to be held fully liable, all the way to the medical director of the PHP whose final decision this was.
How a medical board could accept such a stance simply defies understanding. Was there any due process provided to you to confront this injustice?
@C G I would highly recommend that you make an appointment with the Office of the Governor of California and present your case there to some reasonable person. Further, I would recommend that you explore what group in the California legislature is responsible for oversight of state boards and then make an appointment to speak directly with the Senator and Representative who are the Chairman of such a group. In addition, I would think it advisable to find an investigative reporter with the largest newspaper(s) in the state and attempt to interest the reporter in doing a piece on your story.
I have heard of some outlandish cases, but what you present tops anything I have heard. It is very difficult to believe that such could take place in America as it sounds more like the actions of a third world country.
I hope you will post for us what attempts you have made thus far to right this perceived wrong.
@Dr. Jesse Cavenar @C G I have been thinking that some of us should take out large ads in influential newspapers delineating our concerns. This might be a good test case for that idea…like the large LA newspaper (is it LA Times?).
To Dr. L.N.
If I understand your post, your state that Dr. Carr during his tenure has “allegedly been through treatment eight times for relapses”. Is there proof of this, or are these merely allegations? If one logs on to the Tennessee Department of Health website for Tennessee licensed physicians, one finds a Gary Dwain Carr who holds a Tennessee medical license and that website clearly shows, “no actions by state regulatory board; no resignations in lieu of termination; no actions by hospitals; no criminal offenses; and no liability claims”. To all appearances, this is a perfect record.
Is it being suggested that somehow these alleged relapses never reached the medical board, or that somehow there was preferential treatment such that some PHP tolerated a physician patient having eight relapses with no action or report involving the respective medical board?
These are serious allegations that you have raised, and I hope there is proof of this and not merely allegations. Please clarify this for the readers.
@Dr. Jesse Cavenar Yes, that is an assertion that is very troubling. But if true, that would make him an easy pawn as the head of a PHP for anyone wishing to influence his decision-making…to divert docs to their programs, etc. —I mean easy to blackmail him.
Actually, Dr. Van Craig of the MSBML told me he left the MS PHP just before they fired him. A local lawyer told me he had relapsed. He resurfaced in WA but only lasted a short time there.
After Washington State, he decided to take Project Blueprint on the road, starting an impaired veterinarian program. He is in MS. Hattiesburg.
I think relapse is fair game considering the PHP is insisting their treatment paradigm is so effective.
@Dr. Jesse Cavenar Dr. karen shackelford Dr. Gail Hirschfield
I have heard the same thing from multiple sources but have not posted this on my blog as I have been unable to verify the assertions. I suspect they are true but no “paper trail” exists (presumably by design).
I am posting one of the comments that was sent to me below and have contacted the author to request elaboration here-ML
“The Like Minded Docs I know, Gary Carr and Scott Hambleden, have each been through rehab eight times. Gary Carr was fired as head of the PHP as a result of the obvious failure of drug and alcohol treatment to resolve any of his addiction issues or personality disorders. He then managed to get hired in Washington State, as head of their PHP. He left there at their request. He is currently pushing “Project Blueprint,” and I heard he was monitoring veterinarians. Scott H. was a counselor at Pine Grove – where your stay is indefinite and you are subjected to polygraph testing to assess your compliance. I tried to stick it out, but I became deeply depressed at the daily phone calls for drug testing and the forced adherence to the AA cult. My appointed drug and alcohol counselor (appointed by the PHP) told me I needed “more intensive therapy,” despite the fact that ten weeks did not have a lasting effect on my belief that the system was total crap. The mind control is unethical, and treatment is a long isolation/brainwashing session. Coercion is routine, with threat of public disgrace – everyone believes the medical board. People just don’t realize what is going on, although there has been more coverage in the media lately – Atlantic Monthly, the new documentary called “The Business of Recovery.” The misfits who run the PHPs are, in general, unethical quacks trying to redeem themselves professionally in the only field left to them.Addiction medicine as a specialty is a joke. People with a financial interest or personal stake in AA spend a lot of time and money to stifle scientific inquiry into the effectiveness of these treatment scams.”
Scott actually told me he had been in rehab eight times, by way of relating that the place he finally ended up at was great. I would say that treatment is of questionable efficacy.
@Dr. Michael Langan @Dr. Jesse Cavenar Each time I sign on to this series of Medscape articles and read the comments, my jaw drops in amazement. I simply had no idea of the immensity of the abuse of physicians nor of the pathology of the perpetrators.
In fact, some times I have to wonder – how can this possibly be true? The abuse stories are indeed troubling, but then to read that some of the PHP heads – ASAM / Like-minded docs – and the heads and staff of the programs are so troubled themselves ….
You know, it’s one thing to have an addictive disorder and to get help for it, and even to carry the “message of salvation” to one’s fellow afflicted docs. It’s another thing for the recovered doc to make a business of it. Okay I guess, all power to them. Great to turn lemons into lemonade – I congratulate them on their entrepreneurial mindedness.
But then, when I read that some of the docs who head these programs have not only made a dandy business but have themselves become like Stalinist – distinctly un-compassionate and vindictive – rulers, I get really concerned.
Then I learn that, as some have alleged, that when these ASAM / PHP heads themselves have their relapse, they don’t get the same treatment that the lowly “participant” docs in their system do. Rather, they get some sort of preferred – and undisclosed – treatment. Hmmm.
But now, at least per the reference you quote here, you allege that some of these PHP heads have actually had eight relapses?!?! Eight??? And that they still maintain their PHP Directorship positions? Well, if not at the same PHP, they get a free ticket to go head up another PHP or one of their “preferred” programs??? And they still maintain their medical license!?!?!? How is this possible???
I think we get on really shaky ground when these kinds of anecdotes are reported. Is there any reference to this? Because, if this is true, then what we’ve got is a network of extremely relapse-prone docs heading up PHPs, dictating abusive and unforgiving draconian policy and yet who themselves carry a lifelong “get out of jail free” card. Not only that, get out of jail and makes lots of dough in the lucrative physicians’ addictions industry.
Could you post a source here? This just continues to boggle the mind. I still can’t get my head around it.
@Dr. Kernan Manion @Dr. Michael Langan @Dr. Jesse Cavenar Per my comment above.
@Dr. Kernan Manion @Dr. Michael Langan @Dr. Jesse Cavenar
There is no public record I have been able to find. The quote above was left a a comment on my blogpost “Letters from the Abused and Afraid” and I have contacted the author.
http://disruptedphysician.com/2015/03/14/letters-from-those-abused-and-afraid/
@Dr. Michael Langan @Dr. Kernan Manion @Dr. Jesse Cavenar Horrifying link, Dr. Langan.
Lives destroyed. Lives lost. Somebody must do something about it…oh yeah, I am somebody, and thankfully, so are you! all the above, Dr. Wible, and all y’all soldiers in the field of dreams…











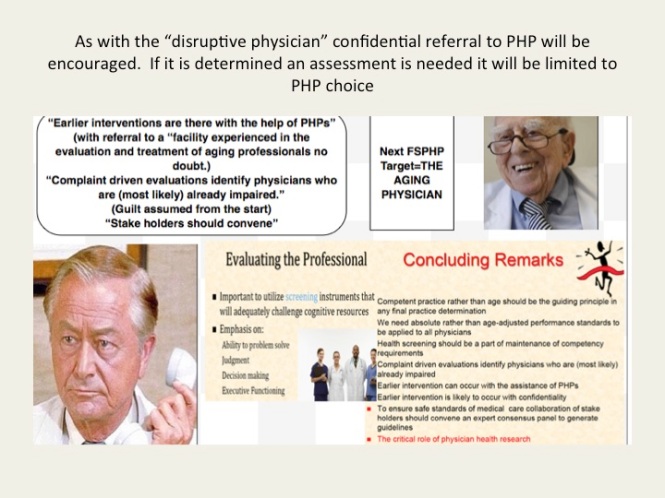
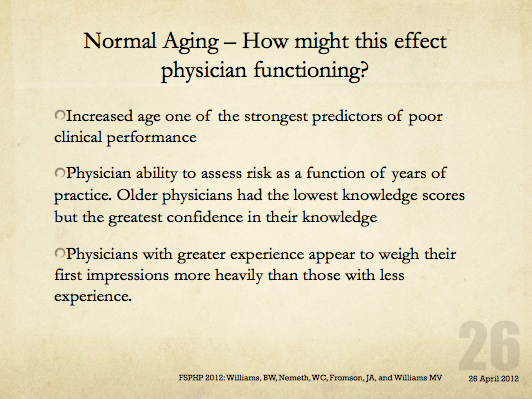

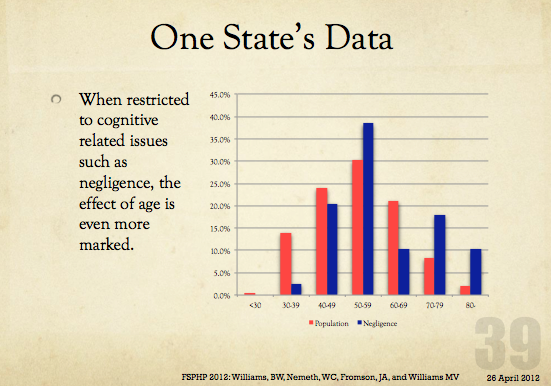














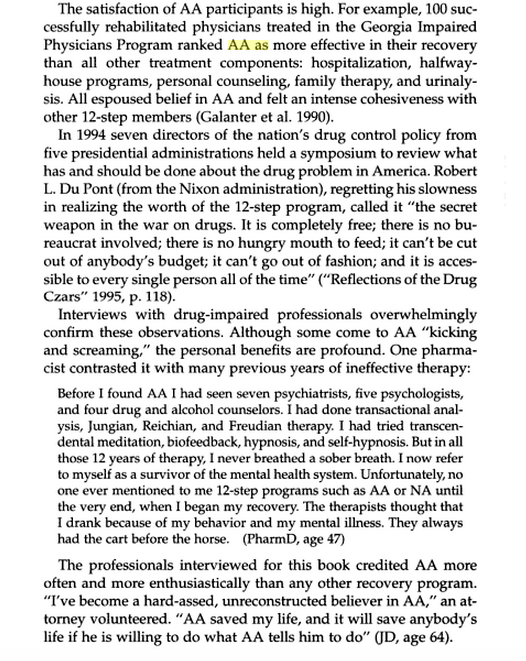











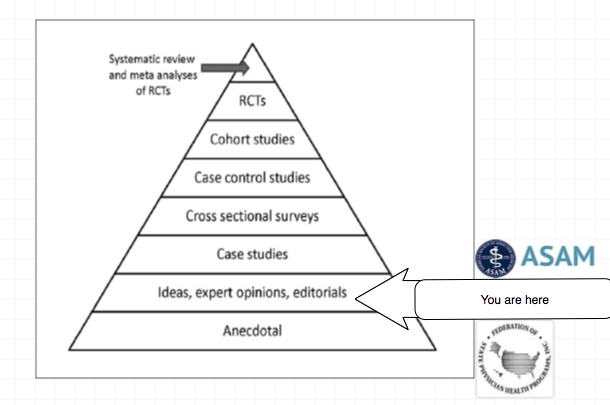
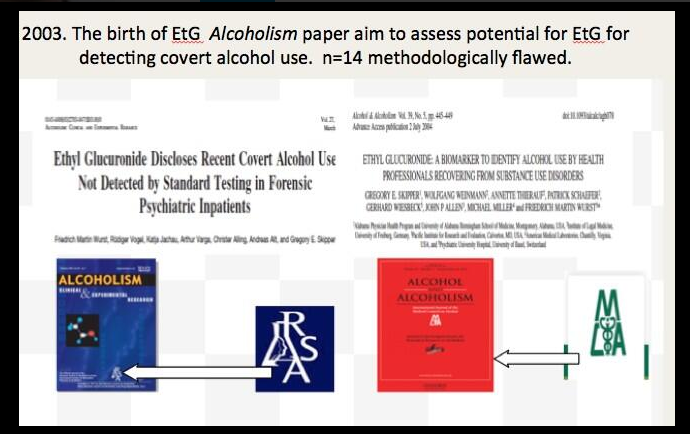
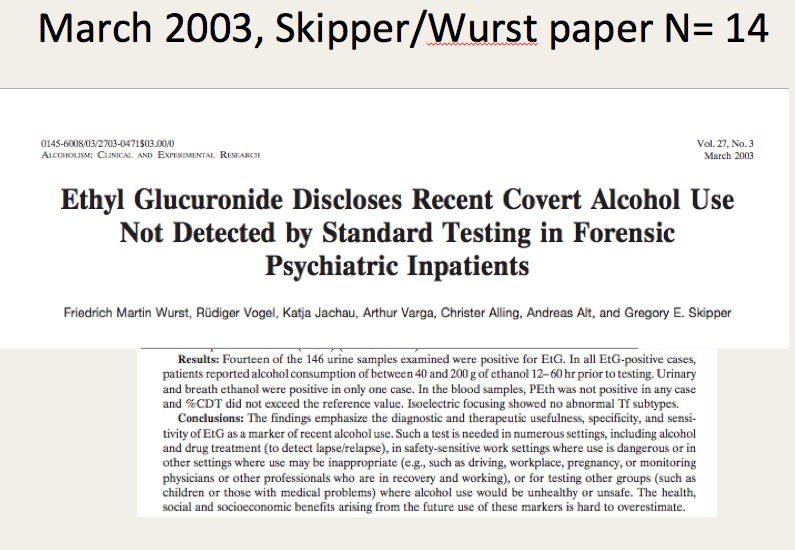
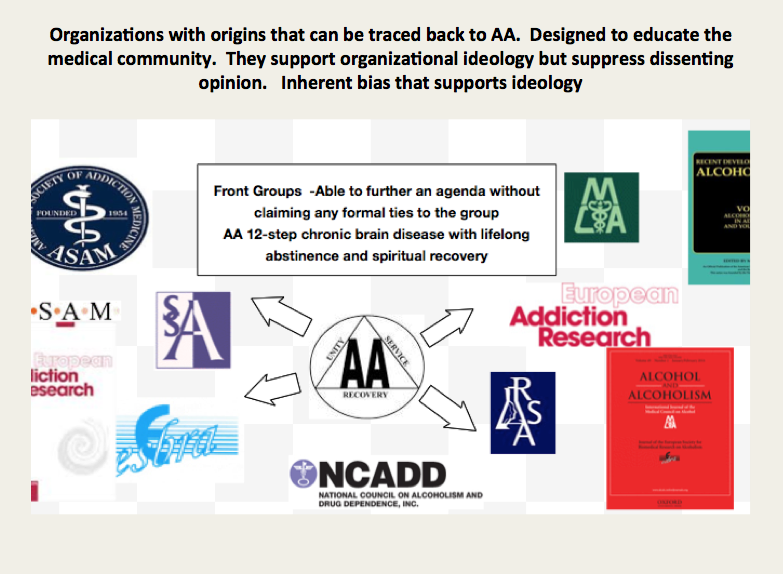











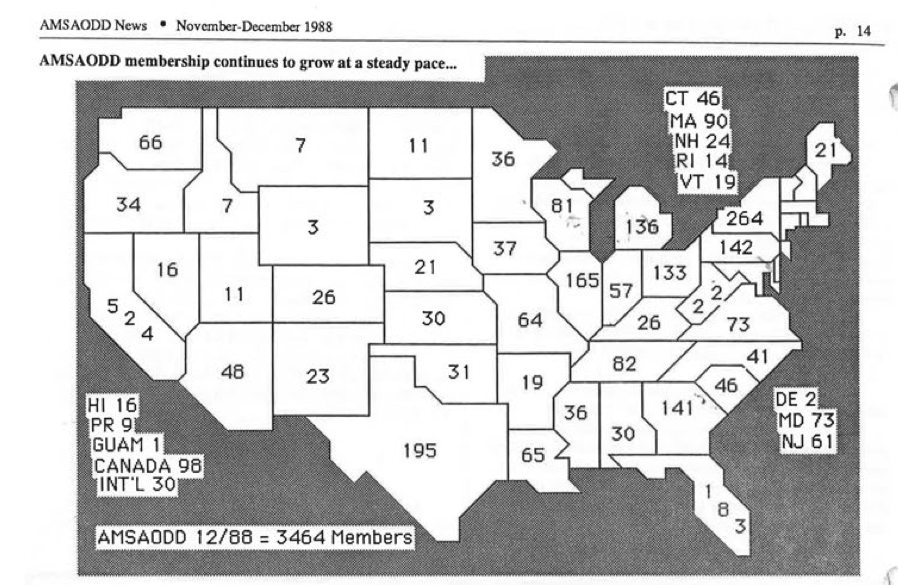

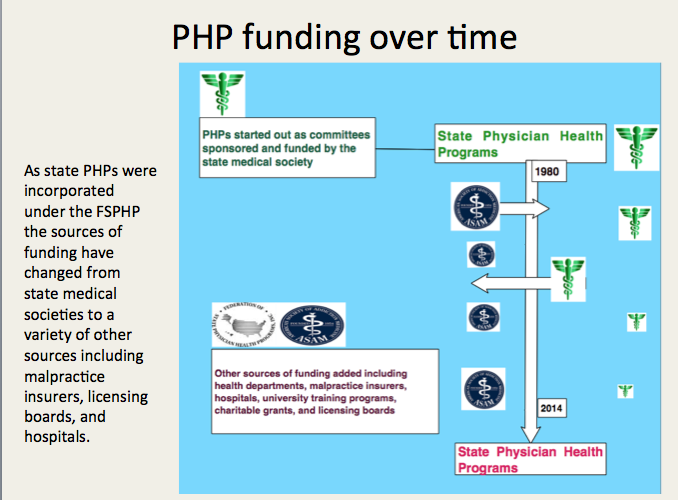




Hi Mr.Goldsmith,
Currently, these ‘PHP approved evaluation’ centers are the exact same facilities as the PHP ‘treatment’ centers. There centers also have financial relationships with PHP programs and PHP directors.
They charge upwards of $5,000 dollars to the physician plus travel and lodging expenses, because they are often out-of-state.
Former ASAM leader and PHP director Dr.Talbott owned such a facility with a judge as a co-investor. Dr.Talbott was convicted by a jury in a US court of law of coercing a doctor into unnecessary ‘treatment’ for financial gain. How many of these 78% recovery rate come from physicians falsely diagnosed? Dr.Fata, the Michigan doctor convicted of giving false cancer diagnoses, also touted his high ‘treatment success rate’
We’d like you to correct these current questionable practices by ASAM and PHPs. A true independence of diagnosticians and PHPs is a good place to start, with strict oversight and auditing to eliminate all and any financial ties and conflicts of interest. PHP leadership and directors should be replaced by physicians with demonstrated commitment to ethics and personal rights.
Do these steps sound reasonable to you?