Accountability is rooted in organizational purpose and public trust. Unfortunately, humanitarian ideals have been trampled by the imposition of corporate front groups who advance hidden agendas under guises of science and scholarship and patinas of benevolence. Rife with conflicts of interest, these groups obfuscate, mislead and exploit us to further an underlying political and corporate agenda. Healthcare and medicine has been infiltrated by various groups that pose a serious threat to both the humanitarian and evidence based aspects.
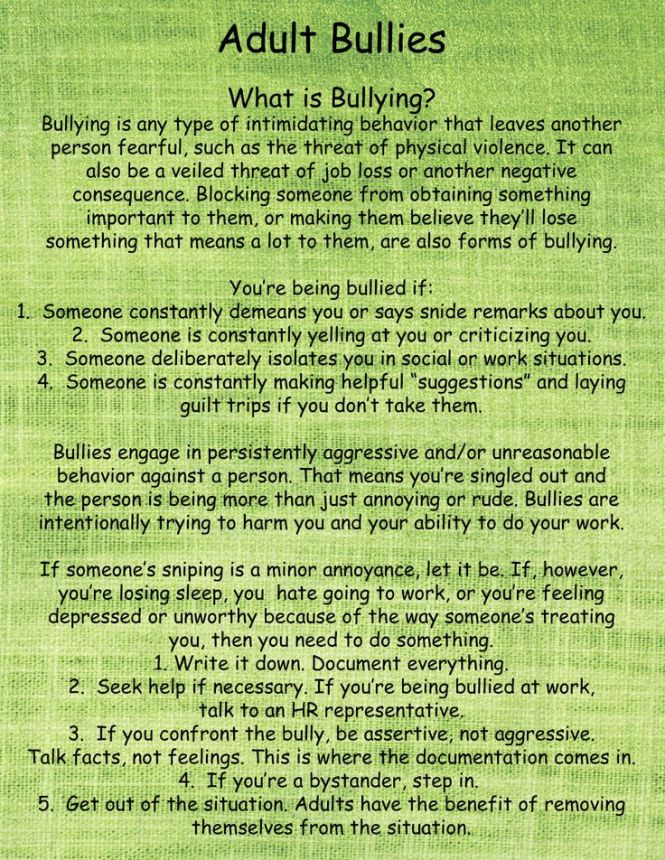
You are mistaken if you believe that bullies only lurk in school hallways and on playgrounds… Mean kids grow up and become parents, co-workers, and bosses. They work in offices, businesses, for governments, in police departments, law offices, and charitable organizations.
They are cowards who lack the ability to work out problems in a reasoned, adult manner.
They need a fan club of followers and admirers who support their evil deeds, “flying monkeys” to persecute their targets, and/or technology to hide behind.
The adult bully character pathology is characterized by a lack of empathy, craving for power, manipulativeness, and deceptiveness. Bullies feel entitled to use others as they wish and they derive sadistic pleasure from the harm they cause.
We are publishing an article on the subject of medical boards. We will be investigating this topic closely and are welcoming public contributions as part of this process. We encourage providers or patients who have been harmed by such measures to help bring them to light. If you know of anyone harmed, please report it to US Legal Research. To contact your state representative regarding this topic, please visit UsLegalResearch.org.
Background
Is our country really plagued by an abundance of bad doctors?
By Marion A. Stahl
An alarming amount of war stories seem to be floating around the news lately regarding bizarre medical board actions, physicians being jailed, and even physicians committing suicide. In response to this trend, we resolved to conduct a close investigation to identify the patterns among various states. While this phenomenon is by no means new, it does seem to have reached epidemic proportions in the past year…
“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.” Father Cornelius Loos ( 1592 )
How Impaired Physicians Can be Helped–Medscape Business of Medicine Article Published February 24, 2015. Click on image to access
How can impaired Physicians be helped?
1. Impairment among physicians is growing: Why?
Answer: It is not. State Physician Health Programs (PHPs) are “diagnosing” impairment when there is no impairment. They are pathologizing the normal and expanding in scope to increase the grand scale of the hunt.
2. What’s the Prognosis for Impaired Physicians?
Answer: Not Good. Those who need help (the truly impaired) are afraid to get help for fear of being monitored by their state PHP while many of those ensnared by PHPs are not impaired. There is absolutely no oversight, regulation or accountability. This needs to be evaluated in the context of physician suicide. The system is one of institutional injustice and abuse of power.
3. Is your knowledge of physician impairment up-to-date?
Answer: No. This will only occur after an evidence-based Cochrane type review separates information from misinformation; An objective non-biased investigation by outside actors identifying any conflicts-of-interest, misconduct or lack of evidence-base in the current system and separating the art and science of the medical profession from the politicalization and exploitation of the medical profession.
As Drs. John Knight and J. Wesley Boyd note in Ethical and Managerial Considerations Regarding State Physician Health Programs, published in the Journal of the American Society of Addiction Medicine, this is what is known as “tailoring a diagnosis”–a euphemism for the political abuse of psychiatry. According to the Global Initiative on Psychiatry “Political abuse of psychiatry refers to the misuse of psychiatric diagnosis, treatment and detention for the purposes of obstructing the fundamental human rights of certain individuals and groups in a given society.” The shoe fits here. In fact it fits very well.
The Global Initiative on Psychiatry opposes the Political_Abuse_of_Psychiatry wherever it may occur and “supports those psychiatrists and psychiatric organizations that pressure the offending states to discontinue the practice and lobby vigorously those organizations which are wavering. The main way for individuals and organizations to work is through diplomatic channels. It is necessary to expose the practice and to embarrass countries that are at fault by expelling them from organizations such as the World Psychiatric Association. This can only be ensured by properly organized open investigation of psychiatric practice and interviews with the alleged victims”
Political abuse of psychiatry in the profession of medicine needs to be treated in the same way.
An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
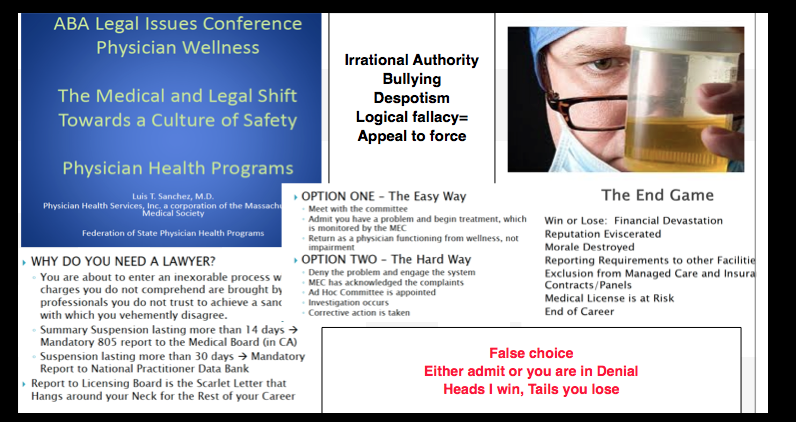
In evaluating a physician for “impairment” or being “disruptive” the Physician Health Programs (PHPs) under the Federation of State Physician Health Programs (FSPHP) are not gathering data to form a hypothesis. They are making data fit a hypothesis that arrived at the out-of-state “PHP-approved” assessment center well before the alleged miscreant doctor.
With guilt assumed from the start, no due process, no appeal, and no way out physicians are being bullied, demoralized, and dehumanized to the point of hopelessness, helplessness and despair.
This needs to end now.
Medicine is predicated on competence, good-faith, and integrity.
Medical ethics necessitates beneficence, respect, and autonomy.
The scaffold erected here is designed for coercion and control.
Exposure, transparency, and accountability are urgent.
I recently spoke with a former colleague who shared a story of a young 17-year-old who was killed during a physical restraint (stay tuned for my Personal Stories Week on Psychcentral, coming August 17th-24th, for more on this story). She was not only disgusted by her colleagues but shocked that the agency suspended these three men with pay. This story sparked another story which sparked a series of questions about unethical behaviors and what they look like within mental health agencies. I have taken the opportunity to list a few below. Please feel free to share your experiences of unethical behaviors within mental health agencies in the comments section below.
What are common unethical practices?
It’s difficult for many families to determine what is ethical and what is unethical. Here is a list of unethical behaviors that often occur in mental health facilities:
I was living in Tangier in 1957, and I had spent a month in a tiny room in the Casbah staring at the toe of my foot. The room had filled up with empty Eukodol cartons; I suddenly realized I was not doing anything. I was dying. I was just apt to be finished. So I flew to London and turned myself over to Dr. John Yerbury Dent for treatment. I’d heard of his success with the apomorphine treatment. Apomorphine is simply morphine boiled in hydrochloric acid; it’s nonaddictive. What the apomorphine did was to regulate my metabolism. It’s a metabolic regulator. It cured me physiologically. I’d already taken the cure once at Lexington, and although I was off drugs when I got out, there was a physiological residue. Apomorphine eliminated that. I’ve been trying to get people in this country interested…
The Medical Profession, Moral Entrepreneurship, and Social Control
Sociologist Stanley Cohen used the term “”moral panic” to characterize the amplification of deviance by the media, the public, and agents of social control.1 Labeled as being outside the central core values of consensual society, the deviants in the designated group are perceived as posing a threat to both the values of society and society itself. Belief in the seriousness of the situation justifies intolerance and unfair treatment of the accused. The evidentiary standard is lowered.
Howard Becker describes the role of “moral entrepreneurs,” who crusade for making and enforcing rules that benefit their own interests by bringing them to the attention of the public and those in positions of power and authority under the guise of righting a society evil. 2
And according to cultural theorist Stuart Hall, the media obtain their information from the primary definers of social reality in authoritative positions and amplify the perceived threat to the existing social order. The authorities then act to eliminate the threat.3 The dominant ideas or ideologies are reproduced by relying on the opinions of the defining authority and then spread through the media. The communal good has been assailed.
As a society governed by organizations, associations, institutions and regulatory bodies, the medical profession is not immune to “moral panics.” A threat to patient care or the values of the profession can be identified and amplified. A buildup of public concern fueled by media attention ensues creating a need for governing bodies to act. Medical Professionalism and the Public Health has been assailed.
Unbeknownst to the general public and most members of the medical profession at large, certain groups have gained tremendous sway within medical society. Through moral entrepreneurship they have gained authority and become the primary definers of the governance of the medical profession and the social control of doctors. To benefit their own interests they have fostered and fueled “moral panics” and “moral crusades. ” Exhorting authorities to fight these threats by any means necessary they have successfully made and enforced rules and regulations and introduced new definitions and tools with no meaningful resistance or opposition.
The Inquisition did not have to convince individual citizens or the general public of their beliefs to advance an agenda; just Ecclesiastical and Political Authority. Similarly, the “impaired physicians movement” did not have to convince individual doctors or the medical profession of their beliefs to further a self-serving agenda; just regulatory and administrative authority.
Addiction Medicine Monopoly, False Authority and Conflicts of Interest
The “impaired physicians movement” can be defined as a group of physicians with alcohol and substance abuse problems who, having found sobriety through 12-step spirituality, banded together to promote the ideology behind their personal “recovery” to other doctors and the medical community at large. In the 1980s the movement gained momentum and as their numbers grew began calling themselves specialists in “addiction medicine.” The American Society of Addiction Medicine (ASAM) is not a true specialty, but a Self-Designated-Practice-Specialty, which simply means that is what they are calling themselves. It reflects neither knowledge nor expertise.. “Board certification” by the American Board of Addiction Medicine (ABAM) is not recognized by the American Board of Medical Specialties (ABMS).
The ASAM is schooled in just one one uncompromising model of addiction with the majority attributing their very own sobriety to that model–the chronic relapsing “brain disease” with lifelong abstinence and 12-step spiritual recovery model. As the “voice of addiction medicine,” the ASAM has nevertheless defined the dominant treatment paradigm in the United States. ASAM doctors outnumber addiction psychiatrists by 4:1 and the movement is well funded. Because addiction is defined as a “disease”, addicts must be “treated” (more often coercive than voluntary), and “cured” (defined as abstinent). The billion dollar assessment and treatment industry and the drug and alcohol testing industry lucratively profits from this model which has grown to monopolize addiction treatment in the United States.
The goal of the ABAM Foundation is to “gain recognition of Addiction Medicine as a medical specialty by the American Board of Medical Specialties (ABMS).” A monopoly defined by self-appointed experts without recognized specialty training will soon likely Robber baron their way to being accepted as a true specialty.
Physician Health Programs, Regulatory Agencies, and Treatment Centers
Physician Health Programs (PHPs) meet with, assess, and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Unless being monitored by one, PHP practices are unknown to most physicians and operate outside the scrutiny of the medical community. Initially funded by State Medical Societies and staffed by volunteer physicians, PHPs served the dual function of helping sick doctors and protecting the public.
As the populations of ASAM physicians proliferated in the 1980s, many joined their state Physician Health Programs. PHP doctors who did not agree with the ASAM groupthink were gradually removed and they organized under the Federation of State Physician Health Programs (FSPHP). Other ASAM physicians found employment at treatment centers as staff physicians and medical directors.
The FSPHP cultivated a relationship with the Federation of State Medical Boards (FSMB) and the state PHPs formed alliances with their state medical boards. Promoting themselves as offering “treatment” rather than”punishment” they offered an alternative to disciplinary action. They then began promoting their successful outcomes in rehabilitating “impaired physicians”, and this history can be seen by examining the archives of the Journal of Medical Regulation and similar publications. In 1995 the Washington PHP claimed a success rate of 95.4%, Tennessee claimed 93% and Alabama 90%.
Part of this success was attributed to the specialized treatment centers for doctors directed by their ASAM colleagues such as Ridgeview Institute in Atlanta created by G. Douglas Talbott. Talbott, who helped organize and serve as past president of the ASAM claimed a 92.3 percent recovery rate. He also put forth a Medical Urban Legend–the proposition that doctors were a different species, separate from the rest of society, who needed special treatment three times longer than anyone else. Amazingly, this dicto simpliciter argument that can, in fact, be refuted simply by pointing it out was allowed to enter regulatory medicine unopposed. Simply because, sadly, no one ever pointed out the logical fallacy. It is now entrenched. Three months or more of treatment is standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value.
Physicians are unique only insofar as the unique elements required of the profession to become and be a physician such as going to medical school and completing the required board examinations. That’s it. I implore anyone to put forth any sound argument based on science and evidence that justifies a thrice lengthy stay in medical professionals. Not gonna happen. Thought stopping memes and logical fallacy is the best they have to offer. And, unfortunately this type of rabbling gibberish cuts the mustard in the regulatory medicine venue. A “low-bar” evidentiary standard is not the problem. If you look at the documentary evidence from a medico-historical perspective there never was a bar. The FSMB has essentially given the impaired physicians movement carte blanche authority and unrestrained managerial prerogative. A bar never even existed. It’s a laissez-faire Lord of the Flies free-for-all. The logical fallacy of appeal to authority–illegitimate and irrational authority. Bamboozled by smoke and mirrors.
A 1995 issue of the FSMB publication The Federal Bulletin: The Journal of Medical Licensure and Discipline contains reports on eight separate state PHPs. The “almost 90% success rate” was applauded by the editor, who added “cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” And more recent reports suggest PHPs reduce malpractice claims. They are now being promoted as a replicable model to be used in other populations.
The problem is no one bothered to examine the methodology to discern the validity of these claims. There has been no critical analysis or Cochrane type review of any of these studies which are invariably small, methodologically flawed, and biased.
The FSMB has accepted them as expert authority and their authoritative opinion as fact. It is this acceptance of faith without objective assessment that has allowed the ASAM and FSPH to advance their agenda. By confusing ideological opinion with professional knowledge, the FSMB and state Medical Boards have acted as willing gulls each step of the way. No counter-forces existed. And they still don’t. Junk science and unvalidated neuropsychological testing is used by these groups unconstrained and willfully. There is no regulation, oversight, or accountability. They are using polygraph testing (despite the AMA’s previous public policy statement deeming it junk) to both condemn “disruptive” surgeons and deem convicted pedophiles fit to return to work. They have introduced junk-science in drug and alcohol testing and unvalidated “neuropsychological” testing to detect “character-defects” by getting regulatory agencies to accept the validity of these tests not by the Scientific Method or Evidence Based Research but by (to coin a term) “Regulatory Sanctification”
To paraphrase one FSPHP member, “Who needs evidence-based medicine when the boards have already accepted these tests as valid?” Who indeed?
The ideological bias and financial conflicts of interest between PHPs and the treatment centers was also not recognized. It still isn’t. The spotlights are apparently all on Big Pharma in this regard. Some sunlight needs to be exposed in the direction of the billion dollar drug and alcohol testing and assessment industry as well.
Doctors were held at Ridgeview three times longer than the rest of the population (and at three times the cost) under threat of loss of licensure. Although there is no evidence base or plausible explanation why an entire profession would have a three-times longer length of stay than the rest of the population this continues to be the reality. There is no choice.
in 2011 The ASAM issued a Public Policy Statement on coordination between PHPs, regulatory agencies, and treatment providers recommending that only “PHP approved” treatment centers be used in the assessment and treatment of doctors. It specifically excludes non “PHP -recognized” facilities. And what defines a “PHP approved” treatment center? In addition to finding essentially no oversight by the state medical society and medical board, a recent audit of the North Carolina PHP found financial conflicts of interest and no documented criteria for selecting the out of state treatment centers they used. The common denominator the audit missed was that the 19 “PHP-approved” centers were all ASAM facilities just like Ridgeview whose medical directors can be seen on this list.
The appeal to authority logical fallacy has enabled the FSPHP to become the expert authority on physician impairment through the eyes of the medical boards. It has also allowed them to increase their scope.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that:
“Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with ‘potentially impairing illness.'”
According to the FSPHP, physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years.”
The policy extends PHP authority to cover physical illnesses affecting cognitive, motor, or perceptive skills, disruptive physician behavior, and “process addiction” (compulsive gambling, compulsive spending, video gaming, and “workaholism”). It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A A language –stinking thinking.” AA language has entered the Medical Profession and no one even blinked. It will get worse.
The ASAM has monopolized addiction treatment in the United States. It has imposed it on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. It selects who will be monitored and dictates every aspect of what that entails. It is a, in fact, a rigged game.
Inherent in this model is the importance of external control. It gives them power to exert control over the individual regardless of whether they need to be treated.
By bamboozling regulatory medicine this was accomplished. And the maintenance of this relationship is necessary as this presentation by an FSPHP physician warns, “guard this relationship jealously.”
Moral Panics and Moral Crusades
By introducing and fueling moral panics the ASAM/FSPHP political apparatus has been able to expand in both scope and power.
The Medscape article “Drug Abuse Among Doctors: Easy, Tempting, and Not Uncommon” published in the “Business of Medicine” section in January 2014 is characteristic example of the authoritative opinion, propaganda, and misinformation spun to maintain a pervasive climate of fear. Proof by anecdote. Physicians are “5 times as likely as the general public to misuse prescription drugs” according to Lisa Merlo, PhD. “Given the epidemic of prescription addiction sweeping the nation, that’s a grim statistic.”
Described as a “researcher at the University of Florida’s Center for Addiction Research and Education,” Merlo’s research involving 55 doctors being monitored by their state Physician Health Program published in the Journal of Addiction Medicine in October 2013 found “most physicians who abuse prescription drugs” do so to “relieve stress and physical or emotional pain.” Nowhere is it mentioned on Medscape that Merlo is the Director of Research for the Florida state PHP Professionals Research Network. Physician access to medications through prescriptions, “networks of professional contacts, and proximity to hospital and clinic supplies” gives them “rare access to powerful, highly sought-after drugs” says Marvin D. Seppala, chief medical officer at Hazelden. This access “sets them apart” and “not only foment a problem” but”perpetuate it” says Seppala. “Access “becomes an addict’s top priority” and they “will do everything in their power to ensure it continues.”
“They’re often described as the best workers in the hospital,” he says. “They’ll overwork to compensate for other ways in which they may be falling short, and to protect their supply. They’ll sign up for extra call and show up for rounds they don’t have to do.”-Dr. Marvin D. Seppala
Physicians are intelligent and skilled at hiding their addictions, he says. Few, no matter how desperate, seek help of their own accord.” In reality this is absurd. And if you look at any of the current “moral panics” that are being used to suggest random suspicion-less drug testing of all doctors or promoting the Physician Health Programs as the “New Paradigm” you will inevitably find a doctor, just like Marv Seppala who is on this list as an author or interviewee. It is a given.
The terms “impaired physician” and the “disruptive physician” are used as labels of deviancy. As deviants who allegedly threaten the very core of medicine (patient care) and the business of medicine (profit) they must be stopped at all costs. Belief in the seriousness of the situation justifies intolerance and unfair treatment. The evidentiary standard is lowered. Aided by a “conspiracy of silence” among doctors in which impaired colleagues are not reported necessitates identification of them by any means necessary. Increase the grand scale of the hunt.
In this way these front-groups have successfully acted as moral entrepreneurs to make and enforce rules and put forth new definitions and mandates that serve their own interests. A retrospective non -blinded non-randomized cohort study with serious underlying methodological errors involving 904 physicians being monitored by PHPs is now being used to “set the standard for recovery.”
Across the Country doctors are going to the media, law enforcement, the AGO, and the ACLU only to be turned a deaf ear. Many consider this a “parochial” issue best handled by the medical community. Doctors reporting crimes are turned back over to the very perpetrators of the crimes. The Medical Societies and professional organizations contribute to the problem by willful ignorance. Accusations are used to disregard the claims of the accused. It is a system of institutional injustice that is driving many doctors to suicide. Hopeless, helpless, and feeling entrapped many are taking this route. And no one is talking about it. This cannot be avoided any longer.
The next target is the “aging physician.” And as they have done with the “impaired” and “disruptive” physician” the FSPHP and their affiliates are setting the stage for another “moral crusade.”
Cohen S. Folk Devils and Moral Panics: The Creatio of the Mods and Rockers (New Edition). Oxford, U.K.: Martin Robertson; 1980.
Becker H. Outsiders: Studies in the Sociology of Deviance. New York: Free Press; 1963.
Hall SC, Critcher C, Jefferson T, Clark J, Roberts B. Policing the Crisis: Mugging, the State, and Law and Order. London: Macmillan; 1978.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to doctors and how they might be involved in the descent from suicidal ideation to suicidal planning to completed suicide.
Depression and Substance Abuse Comparable to General Population
Depression and substance abuse are the two biggest risk factors for suicide. The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria suggest that physicians have the same rates (8-14%) of substance abuse and dependence as the rest of the population 3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 found a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
State Physician Health Programs
Perhaps it is how physicians are treated differently when they develop a substance abuse or mental health problem.
Physician Health Programs (PHP) can be considered an equivalent to Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Originally developed as “impaired physician” programs, the PHPs were created to help doctors who developed problems with substance abuse or addiction an alternative to disciplinary action by State Medical Boards. These programs existed in almost every state by 1980. Often staffed by volunteer physicians and funded State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referrals. Most EAPs were developed with the collaboration of workers unions or some other group supporting the rights and interests of the workers. As there is no such organization representing doctors, PHPs developed in the absence of regulation or oversight. As a consequence there is no meaningful accountability.
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”8
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “that the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 8 They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”8 Unfortunately this has not happened. Most physicians have no idea that the state physician health programs have been taken over by the “impaired physicians movement.”
In his Psychology Todayblog, Boyd again recommends oversight and regulation of PHPs. He cites the North Carolina Physicians Health Program Audit released in April of 2014 that reported the below key findings:
As with Knight and Boyd’s paper outlining the ethical and managerial problems in PHPs, the NC PHP audit finding that abuse could occur and not be detected generated little interest from either the medical community or the media.
Although state PHPs present themselves as confidential caring programs of benevolence they are essentially monitoring programs for physicians who can be referred to them for issues such as being behind on chart notes. If the PHP feels a doctor is in need of PHP “services” they must then abide by any and all demands of the PHP or be reported to their medical board under threat of loss of licensure.
LDTs bypass the FDA approval process and have no meaningful regulatory oversight. The LDT pathway was not designed for “forensic” tests but clinical tests with low risk. Some are arguing for regulation and oversight of LDTs due to questionable validity and risk of patient harm.13
These same physicians are claiming a high success rate for PH programs9 and suggesting that they be used for random testing of all physicians.14
As with LDTs, the state PHPs are unregulated, and without oversight. State medical societies and departments of health have no control over state PHPs.
Their opacity is bolstered by peer-review immunity, HIPPA, HCQIA, and confidentiality agreements. The monitored physician is forced to abide by any and all demands of the PHP no matter how unreasonable-all under the coloration of medical utility and without any evidentiary standard or right to appeal.
The ASAM has a certification process for physicians and claim to be “addiction” specialists. This “board certification” is not recognized by the American Board of Medical Specialties and is not a recognized medical specialty. The goal of the ASAM is to be recognized as the experts in addiction medicine with the consensus expert opinion based on the 12-step prohibitionist brain disease model. The ASAM has aligned itself with a number of inpatient drug treatment centers (Hazelden, Talbott, Marworth, Bradford,etc) and are heavily funded by the drug testing industry. It is in fact a “rigged game.”
State PHPs are non-profit non-governmental organizations and have been granted quasi-governmental immunity by most State legislatures from legal liability.
By infiltrating “impaired physician” programs they have established themselves in almost every state by joining, gaining power, and removing dissenters. Groupthink and 12-step indoctrination are the goals. By advertising as advocates for doctors who are “caring,” “confidential resources,” “giving help,” and advocating for “colleagues in need” the outward appearance is one of benevolence.
The biggest obstacle is that this system allows them to throw the normal rules of conduct under the imperative of a higher goal assumed to trump all other consideration. Those outside of programs either defend or ignore the reports of ethical and criminal violations, complacent in their trust of these “experts” claiming they are just helping sick doctors and protecting the public.
With no oversight or regulatory body involved this is all done with impunity, immunity, and undercover. They use the accusation of substance abuse as an indication to disregard the claims of the accused. The physician is left without rights, depersonalized, and dehumanized. The imposition of confinement, stigmatization, lack of oversight of the organizations, peer-review protected confidentiality, and lack of procedural protection is a one-way train to hopelessness and despair.
By establishing a system that of coercion, control, secrecy, and misinformation, the FSPHP is claiming an “80% success rate” 15and deeming the “PHP-blueprint” as “the new paradigm in addiction medicine treatment.
The ASAM/FSPHP had a major influence on the DSM-V where drug abuse and dependence are no longer separate entities. They are also working behind the scenes to get legislation to randomly drug test all physicians.
They are now after the “disruptive physician” and the evidentiary criteria are fairly low and red flags include “deviating from workplace norm in dress or conduct” and being tardy for meetings.
They have identified “the aging physician” as a potential problem because “as the population of physicians ages,””cognitive functioning” becomes “a more common threat to the quality of medical care.”
The majority of physicians are unaware that the Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment in 2011 that uses addiction as an example of a “potentially impairing illness.” According to the Federation of State Physician Health Programs …”physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years. This is a critically important distinction. Illness is the existence of a disease. Impairment is a functional classification and implies the inability of the person affected by disease to perform specific activities.”
“Process addiction” was added as a potentially impairing illness including compulsive gambling, compulsive spending, compulsive video gaming, and “workaholism.” According to the FSPHP “the presence of a process addiction can be problematic or even impairing in itself, and it can contribute to relapse of a physician in recovery. As such, process addictions should be identified and treated.” They define three levels of relapse including the novel “relapse without use.”
Bullying, Helplessness, Hopelessness and Despair
Perceived helplessness is significantly associated with suicide.16 So too is hopelessness, and the feeling that no matter what you do there is simply no way out17,18 Bullying is known to be a predominant trigger for adolescent suicide19-21 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.22
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.23,24 The “Cry of Pain” model 25,26 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life.
There is also evidence that rescue factors such as social supports may play a role in preventing suicide. These rescue factors act buffers to protect against suicide in the face of varying degrees of life stress.27,28 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 29 and support at work when difficulties arose appeared to be a protective factor for the male physicians.30 Research involving Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.31,32 Organizational justice is related to fairness and refers to an individuals perception of an organizations behaviors, decisions, and actions and how these influence one’s own attitudes and behaviors and has been identified as a psychosocial predictor of health and wellbeing3334 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.35,36
A recent report indicates that job stress, coupled with inadequate treatment for mental illness may play a role in physician suicide..
Using data from the National Violent Death Reporting System the investigators compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.1
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians.
They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity.
We have heard of numerous suicides due to these institutionally unjust programs. Three doctors died by suicide in Oklahoma in a one month period alone (August 2014). All three were being monitored by the Oklahoma PHP. I went to an all boys high-school of less than 350 students yet a classmate a couple years ahead of me died by suicide a few months ago. He was being monitored by the Washington PHP. His crime? A DUI in 2009–a one-off situational mistake that in all likelihood would never have recurred. But as is often the case with those ensnared by state PHPs he was forced to have a “re-assessment” as his five-year monitoring contract was coming to an end. These re-assessments are often precipitated by a positive Laboratory Developed Test (LDT) and state medical boards mandate these assessments can only be done at an out-of-state “PHP-approved” facility. Told he could no longer operate and was unsafe to practice medicine by the PHP and assessment center he then hanged himself. And at the conclusion of Dr. Pamela Wible’s haunting video below are listed just the known suicides of doctors; many were being monitored by their state PHPs–including the first name on the list– Dr. Gregory Miday.
None of these deaths were investigated. None were covered in the mainstream media. These are red flags that need to be acknowledged and addressed! This anecdotal evidence suggests the oft-used estimate of 400 suicides per year (an entire medical school class) is a vast underestimation of reality—extrapolating just the five deaths above to the entire population of US doctors suggests we are losing at least an entire medical school per year.
As physicians we need to demand transparency, oversight, regulation and auditing by outside groups. This is a public health emergency.
To wit:
They first came after the substance abusers and I did not speak out because I was not a substance abuser.
They then came for those with psychiatric diagnoses and I did not speak out because I was not diagnosed with a psychiatric disorder.
They then came after the “disruptive physician” and I did not speak out because I was not disruptive.
They then came after the aging physician and I did not speak out because I was young.
They then came after me and there was no one else to speak out for me.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ Health Programs. Journal of Medical Regulation. Mar 2010;95(4):10-25.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol and alcoholism. Sep-Oct 2004;39(5):445-449.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results. Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study. European addiction research. 2014;20(3):137-142.
Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
Pham JC, Pronovost PJ, Skipper GE. Identification of physician impairment. JAMA : the journal of the American Medical Association. May 22 2013;309(20):2101-2102.
McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. Bmj. 2008;337:a2038.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis. 2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors. Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
Eighty years ago, Leonarde Keeler’s lie detector made its debut in court. Decades later, we’re still paying the price for his con job.
Eighty years ago this week, inventor Leonarde Keeler proudly proclaimed hisexpert testimony before a Wisconsin jury to be “a signal victory for those who believe in scientific crime detection.”
One of the creators of the modern-day polygraph, the man named after Leonardo da Vinci by his father in the hopes that he would do similarly great things, had just presented his findings in the case of Cecil Loniello and Tony Grignano, two young men on trial for the attempted murder of a police officer as they fled the scene of a robbery. The judge in the case had sought out the polygraph because of the technology’s showing at the 1933 World’s Fair police exhibit. Both sides had agreed to allow the test—the defendants…









 The adult bully character pathology is characterized by a lack of empathy, craving for power, manipulativeness, and deceptiveness. Bullies feel entitled to use others as they wish and they derive sadistic pleasure from the harm they cause.
The adult bully character pathology is characterized by a lack of empathy, craving for power, manipulativeness, and deceptiveness. Bullies feel entitled to use others as they wish and they derive sadistic pleasure from the harm they cause.