

|
I count no man a Philosopher who hath not, be it before the court of his Conscience or at the assizes of his Intellect, accused himself of a scurrilous Invention, and stood condemned by his own Judgement a brazen Charlatan.’
|
Pseudoscience




Junk-Science in the Medical Profession: The Resurgence of Polygraph “Lie-Detection” in an age of Evidence-Based Medicine

 Circa 1995
Circa 1995
The article below was published in the now defunct magazine Gray Areas almost twenty years ago. (Vol. 4, No. 1, Spring 1995 pp. 75-77). Antipolygraph.og founder George Maschke noted in 2008 that article “makes a good introduction to the pseudoscience of polygraphy” and “the criticisms of polygraphy remain valid today.” They remain valid in 2014.
The Art of Deception: Polygraph Lie Detection
By Michael Lawrence Langan, M.D.
I’d swear to it on my very soul, If I lie, may I fall down cold.”
– Rubin and Cherise
(Hunter/Garcia)
The accuracy of polygraphic lie detection is slightly above chance. Nevertheless, State and local police departments and law enforcement agencies across the United States are devoted proponents of this unscientific and specious device. In addition, the American public seems to lend an implicit credence to the “lie detector” as evinced by its ubiquitous use on television crime shows and…
View original post 2,617 more words
Share this:

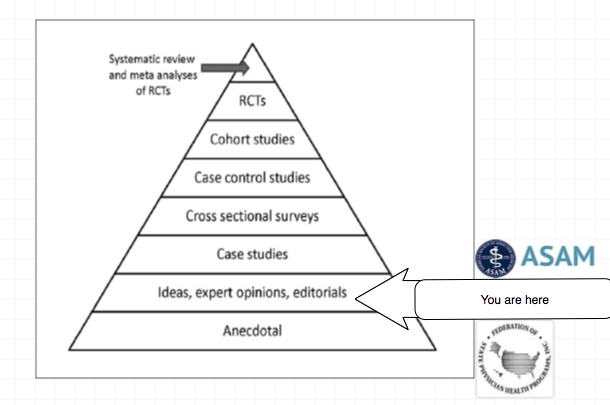
How We Know What to Rely Upon







When to Doubt a Scientific Consensus

The 12-red flags below are very applicable to American Society of Addiction Medicine (ASAM) related consensus and public policy. When viewed through this lens the science and research all falls apart.
(1) When different claims get bundled together.
(2) When ad hominem attacks against dissenters predominate.
(3) When scientists are pressured to toe the party line.
(4) When publishing and peer review in the discipline is cliquish.
(5) When dissenting opinions are excluded from the relevant peer-reviewed literature not because of weak evidence or bad arguments but as part of a strategy to marginalize dissent.
(6) When the actual peer-reviewed literature is misrepresented.
(7) When consensus is declared hurriedly or before it even exists.
(8) When the subject matter seems, by its nature, to resist consensus.
(9) When “scientists say” or “science says” is a common locution.
(10) When it is being used to justify dramatic political or economic policies.
(11) When the “consensus” is maintained by an army of water-carrying journalists who defend it with uncritical and partisan zeal, and seem intent on helping certain scientists with their messaging rather than reporting on the field as objectively as possible.
(12) When we keep being told that there’s a scientific consensus.
Share this:

Against the Rising Tide: Looking for Biostatisticians and Epidemiologists to help shape Drug-Testing Policy to be more Evidence-Based
It is only a few public policy steps and minor changes in state regulatory statutes before what is described in the ASAM White Paper on Drug Testing comes to fruition. Before we know it the Drug and Alcohol Testing Industries “New Paradigm” as described here by Robert Dupont will be ushered in. From the ASAM white Paper:
“THIS WHITE PAPER ENCOURAGES WIDER AND “SMARTER” USE OF DRUG TESTING WITHIN THE PRACTICE OF MEDICINE AND, BEYOND THAT,BROADLY WITHIN AMERICAN SOCIETY. SMARTER DRUG TESTING MEANS INCREASED USE OF RANDOM TESTING* RATHER THAN THE MORE COMMON SCHEDULED TESTING,* AND IT MEANS TESTING NOT ONLY URINE BUT ALSO OTHER MATRICES SUCH AS BLOOD, ORAL FLUID (SALIVA), HAIR, NAILS, SWEAT AND BREATH WHEN THOSE MATRICES MATCH THE INTENDED ASSESSMENT PROCESS. IN ADDITION, SMARTER TESTING MEANS TESTING BASED UPON CLINICAL INDICATION FOR A BROAD AND ROTATING PANEL OF DRUGS RATHER THAN ONLY TESTING FOR THE TRADITIONAL FIVE-DRUG PANEL.”Backed by the multi-billion dollar drug and alcohol testing, assessment and treatment industry the public policy positions of the American Society of Addiction Medicine (ASAM) have invariably passed. There has been little if any meaningful opposition.
To prevent this future drug testing dystopia, that includes testing schoolchildren, we need to take a step back and analyze the reliability and credibility of the “evidence-base” behind these multiple non-FDA approved (Introduced as Laboratory Developed Tests (LDTs) to bypass FDA approval) “forensic” drug and alcohol tests and testing devices (The alcohol biomarkers EtG, EtS, PEth; SCRAM (Subcutaneous Remote Alcohol Monitoring Bracelet);CDPB (Cellular Digital Photo Breathalyzer); and Hair Testing- Psychemedics, etc.) the ASAM proposes be used on the population at large. These tests include nail, hair, saliva, breath, blood and urine and they plan on utilizing the Medical Profession as a urine collection agency by calling this testing a “medical evaluation” rather than “monitoring” for drug and alcohol use. This change in semantics enables them to bypass the usual forensic drug testing protocol (that includes strict chain-of-custody collection and MRO review) designed to minimize false-positives because the results of erroneous test can be grave and far reaching. According to the ASAM white paper the “clinical” collection of specimens as is good enough as the results of a positive test will result in “treatment” rather than “punishment.”
Amazingly, there has been no Academic review of these tests, let alone a Cochrane type critical analysis. It is essentially untapped territory. In addition there has been no Institute of Medicine type Conflict of Interest Analysis.
And that is why I am asking for help from statisticians, biostatisticians and epidemiologists. The task would entail a review of the literature prior to the introduction of these tests for evidence base of forensic applicability (there essentially is none) and a review of the literature peri-and post marketing of these devices to assess the reliability and credibility of the underlying methodology and ascertain the evidence-base. The goal would be publication in both academic journals and presentation to the general public through media publication with the assistance of investigative journalists and other writers. The goal is to get the truth out about these tests and allow both the medial profession and public at large to awaken to the menace this represents. I can’t pay you but you would be combating injustice, corruption and dishonesty. You would be doing your part in helping the Medical Profession, honest and decent doctors, our country and perhaps our future.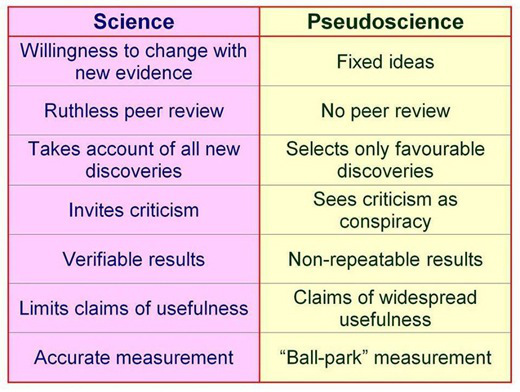
Share this:

Disrupted Physician 101.1: The “Impaired Physician Movement” and the History of the American Society of Addiction Medicine (ASAM)
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers, and consumers of health care products, and the general public.”
In this they have succeeded.
And in the year 2014 Stimson’s characterization of the “impaired physician movement” remains as accurate and apt as it was in 1985. But the “number of evangelical recovered alcoholic and addict physicians” has increased dramatically (outnumbering Addiction Psychiatry by 4:1) and their involvement in “ medical society and treatment programs” has been realized and enforced through the state Physician Health Programs and their “PHP-approved’ assessment and treatment centers.
Their “ability to make authoritative pronouncements on physician impairment…based on their own claim to insider’s knowledge” has become public policy and sanctified by Regulatory Medicine -essentially the Word of the Lord.
And the 1953 Alcoholics Anonymous prophecy that “With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world” is also coming to pass.
But the world is not changing for the better as that arm around the shoulder of religion has its fingers deep in the pockets of the multi-billion dollar drug and alcohol testing and assessment and treatment industries. And the arm around the shoulder of medicine has its fingers clamped tightly around its throat; a stranglehold in full throttle suffocating the Profession of Medicine with no meaningful opposition I can see.

