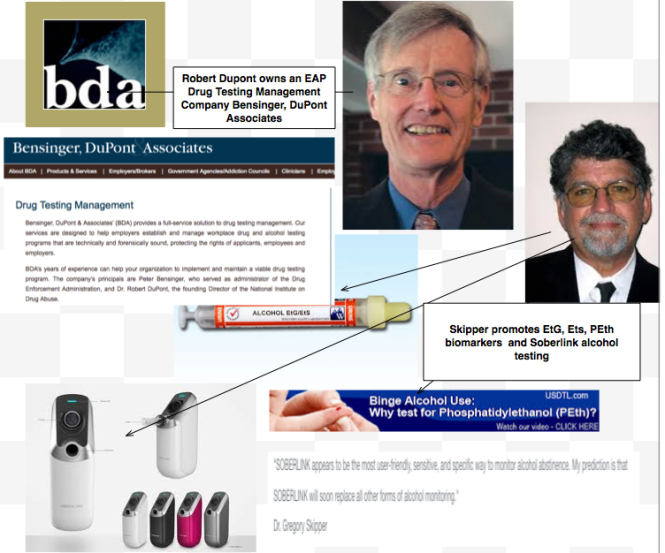
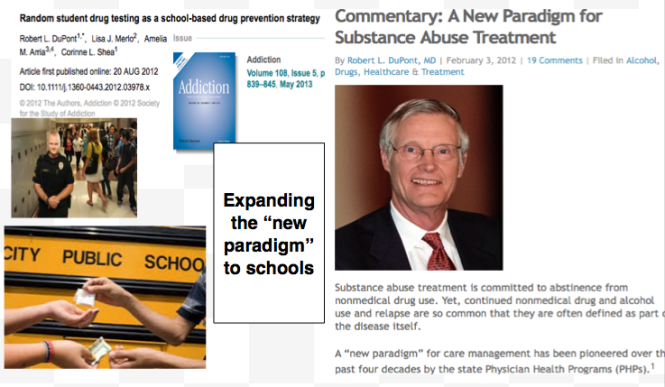
Although the current use of these tests is limited to the criminal justice system and professional monitoring programs this may soon change as the American Society of Addiction Medicine is proposing a “new paradigm” of zero-tolerance random widespread drug and alcohol testing. This is outlined in the ASAM White Paper on Drug Testing and described by Robert Dupont in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) annual conference in 2012.
The ASAM White paper states drug testing is “vastly underutilized” throughout healthcare and describes the use of drug testing “within the practice of medicine and, beyond that, broadly within American Society.”
As the consequences of a single unregulated “forensic” test result can be grave, far-reaching and even permanent it is critical that these tests be included in the debate on regulation of LDTs.
Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.11
Expert opinion is the lowest level of evidence available in the EBM paradigm.12,13 Fortunately, the scientific method and Cochrane type critical analysis of the available evidence is a tool to help people progress toward the truth despite their susceptibilities to unconscious confirmatory bias or conscious confirmatory distortion .14 Unfortunately, no one has used these tools address they panoply of tests of unknown validity that have already entered the market ; poised to be used on virtually everyone.
Please donate to DisruptedPhysician.com below
https://www.gofundme.com/PHPReform
Laboratory Developed Tests


The importance of reliability, validity and accuracy in all medical and laboratory testing–there are no exceptions
 Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
If a test’s results do not differ between alternative states of health, then the test has insignificant accuracy; if the results do not overlap with other states of health then the test has perfect accuracy. Most tests accuracies fall between these two extremes.
The intrinsic accuracy of a test is measured by comparing the test results to the “true condition status.”
‘True condition status” refers to one of two mutually exclusive states. Either a condition is present or it is absent.
We determine true condition status by means of a “gold standard” which is a source of information completely different from the test under evaluation which tells us the true condition status of the patient.

Please donate to DisruptedPhysician.com below
https://www.gofundme.com/PHPReform
Share this:

Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug testing: The plan to introduce junk-science lab tests into the healthcare system and randomly drug test students in schools
 As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.

Share this:

Quacks Selling Snake Oil-EtG and the Big Con.

It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong.
-Thomas Sowell
“EtG” stands for ethyl glucuronide, a metabolite of alcohol, and was reported by Gregory Skipper, M.D. and Friedrich Wurst, M.D., in November 2002 at an international meeting of the American Medical Society, to provide proof of alcohol consumption as much as 5 days after drinking an alcoholic beverage, well after the alcohol itself had been eliminated from the body.
Almost 98% of ingested alcohol is eliminated through the liver in an oxidation process that involves its conversion to acetaldehyde and acetic acid, but the remaining 2% is eliminated through the urine, sweat, or breath.1
- Ethyl Glucuronide (EtG) was introduced in 1999 as a biomarker for alcohol consumption,2 and was subsequently suggested as a tool to monitor health professionals by Dr. Gregory Skipper because of its high sensitivity to ethanol ingestion.3 In his study Dr. Skipper arbitrarily chose a value of 100 as a cut-off for EtG. The rationale behind this value is not cited.
In 2003, because of these and other reportedly remarkable results (e.g., positive findings, confirmed by admissions by the tested individuals, after traditional urine tests had registered negative)
EtG testing began in the United States after Dr. Skipper pitched it to National Medical Services, Inc. (NMS Labs) and it was developed as a Laboratory Developed Test (LDT).
The relevance to the article below is the fact that the EtG paved the way for the hair tests described. The EtG is the index case and prototype for an array of unproven forensic tests introduced to the market as LDTs.
The LDT pathway was basically developed for laboratory tests that would not otherwise come to market due to the prohibitive costs of FDA approval (for example a test for a rare disease). Bringing an LDT to market does not require testing in humans (in vivo). Nor does it require that it be shown the test is testing for what it is purportedly testing for (validity). It is essentially an honor system. It was not designed for “forensic” testing but for simple testing with low risk.
None of this testing is approved by the FDA. It is essentially an unregulated industry.
NMS became a leading proponent of EtG testing and, starting in 2003, began publishing claims promoting the absolute validity and reliability of the EtG in detecting alcohol. Akin to the vitamin and supplement industry those promoting and selling the tests could say anything they want—and they did.
NMS initially established a reporting limit or cutoff of 250ng/ml at or over which EtG test results would be reported as “positive” for drinking alcohol. This was later upped to 500ng/ml, then 1000 ng/ml.
NMS reported it as the “Gold Standard” claiming any value above 250 ng/ml indicated “ethanol consumption.”
 It was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8
It was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8
 As the cutoff value got higher they added another minor metabolite of alcohol, EtS, as a “confirmatory” LDT.
As the cutoff value got higher they added another minor metabolite of alcohol, EtS, as a “confirmatory” LDT.
The authors of a 2011 study demonstrating that hand sanitizer alone could result in EtG and EtS concentrations of 1998 and 94 mug/g creatinine concluded that:
“in patients being monitored for ethanol use by urinary EtG concentrations, currently accepted EtG cutoffs do not distinguish between ethanol consumption and incidental exposures, particularly when uine specimens are obtained shortly after sustained use of ethanol containing hand sanitizer.”9
Sauerkraut and bananas have even recently been shown to cause positive EtG levels.10
A 2010 study found that consumption of baker’s yeast with sugar and water11 led to the formation of elevated EtG and EtS above the standard cutoff. EtG can originate from post-collection synthesis if bacteria is present in the urine.12 Collection and handling routines can result in false-positive samples.13
EtG varies among individuals.14 Factors that may underlie this variability include gender, age, ethnic group, and genetic polymorphisms.
“Exposure to ethanol-containing medications, of which there are many, is another potential source of “false” positives.15
On August 12, 2006, The Wall Street Journal published a front-page article, titled “A Test for Alcohol – And Its Flaws.”.16
Quoting Dr. Skipper, among others, the article includes:
“Little advertised, though, is that EtG can detect alcohol even in people who didn’t drink. Any trace of alcohol may register, even that ingested or inhaled through food, medicine, personal-care products or hand sanitizer.”
“The test ‘can’t distinguish between beer and Purell’ hand sanitizer, says H. Westley Clark, director of the Federal Substance Abuse and Mental Health Services Administration. . . ‘When you’re looking at loss of job, loss of child, loss of privileges, you want to make sure the test is right”, he says…”
“Use of this screen has gotten ahead of the science,’ says Gregory Skipper…”
Methinks Dr. Skipper might have realized this when he initially proposed it as an accurate test after a pilot study done on only a handful of subjects. Or perhaps when he used the LDT pathway to bypass FDA approval and oversight.
On September 28, 2006, SAMHSA, a federal agency that is part of the U.S. Department of Health and Human Resources, issued an Advisory, which on the first page contained a “grey box” warning, as follows:
“Currently, the use of an EtG test in determining abstinence lacks sufficient proven specificity for use as primary or sole evidence that an individual prohibited from drinking, in a criminal justice or a regulatory compliance context, has truly been drinking. Legal or disciplinary action based solely on a positive EtG, or other test discussed in this Advisory is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”17
Bias has been identified as a large problem with drug trials.18 Industry-sponsored research is nearly four times as likely to be favorable to the company’s product as NIH-sponsored research.19 As an example, one survey of seventy articles about the safety of Norvasc (amlodipine) found that 96% of the authors who were supportive of the drugs had financial ties to the companies that made them.20
But what about the multi billion dollar drug-testing industry and the financial ties here?
Imagine if this was a drug and not a drug-test.
Essentially Greg Skipper and the FSPHP arm of ASAM launched a very lucrative joint business venture with a commercial drug-testing lab. They introduced the test via a loophole as a laboratory developed test. An LDT has no FDA regulation so the lab was able to promote, market and sell these tests with no meaningful oversight or accountability.
The lab then contracted with state licensing boards and their state PHPs (who designed, implemented and managed drug and alcohol testing programs for nurses and doctors). A mutually beneficial scheme for the labs (who collect the samples) and the PHPs (who utilize, interpret and report the results.
The PHPs develop the arbitrary cutoff levels based on alleged “scientific” research and the labs promote whatever they say. “Gold-Standard,” “accurate” and “reliable.”
How many lives were ruined by this test? How many careers were lost, families shattered and futures erased. I would venture to say a lot. Just look through all of the legal cases as I have. It is unconscionable. Sociopathic profiteering.
How many committed suicide feeling helpless, hopeless and entrapped?
And the labs have taken a “stand your ground” approach. Never admit wrongdoing. Never settle.
In a February 2007 article in the magazine “New Scientist,” Dr. Skipper is quoted
that:
“…there is not yet an agreed threshold concentration that can be used to separate people who have been drinking from those exposed to alcohol from other sources. Below 1000 nanograms of EtG per millilitre of urine is probably ‘innocent’, and above 5000 booze is almost certainly to blame. In between there is a “question zone…”
No Dr. Skipper—it is you who is most certainly to blame and you alone. Every time you upped the threshold you claimed it was reliable and accurate starting with a level of 100.
And what of all the people whose lives you ruined by introducing junk science with no evidence base via a regulatory loophole. “probably innocent?” Shame on you Dr. Skipper…. Shame..shame..shame.
- Bean P. State of the art contemporary biomarkers of alcohol consumption. MLO Med Lab Obs. Nov 2005;37(11):10-12, 14, 16-17; quiz 18-19.
- Wurst FM, Kempter C, Seidl S, Alt A. Ethyl glucuronide–a marker of alcohol consumption and a relapse marker with clinical and forensic implications. Alcohol Alcohol. Jan-Feb 1999;34(1):71-77.
- Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
- Costantino A, Digregorio EJ, Korn W, Spayd S, Rieders F. The effect of the use of mouthwash on ethylglucuronide concentrations in urine. J Anal Toxicol. Nov-Dec 2006;30(9):659-662.
- Reisfield GM, Goldberger BA, Pesce AJ, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. J Anal Toxicol. Jun 2011;35(5):264-268.
- Rosano TG, Lin J. Ethyl glucuronide excretion in humans following oral administration of and dermal exposure to ethanol. J Anal Toxicol. Oct 2008;32(8):594-600.
- Thierauf A, Gnann H, Wohlfarth A, et al. Urine tested positive for ethyl glucuronide and ethyl sulphate after the consumption of “non-alcoholic” beer. Forensic Sci Int. Oct 10 2010;202(1-3):82-85.
- Hoiseth G, Yttredal B, Karinen R, Gjerde H, Christophersen A. Levels of ethyl glucuronide and ethyl sulfate in oral fluid, blood, and urine after use of mouthwash and ingestion of nonalcoholic wine. J Anal Toxicol. Mar 2010;34(2):84-88.
- Reisfield GM, Goldberger BA, Crews BO, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after sustained exposure to an ethanol-based hand sanitizer. J Anal Toxicol. Mar 2011;35(2):85-91.
- Musshoff F, Albermann E, Madea B. Ethyl glucuronide and ethyl sulfate in urine after consumption of various beverages and foods–misleading results? Int J Legal Med. Nov 2010;124(6):623-630.
- Thierauf A, Wohlfarth A, Auwarter V, Perdekamp MG, Wurst FM, Weinmann W. Urine tested positive for ethyl glucuronide and ethyl sulfate after the consumption of yeast and sugar. Forensic Sci Int. Oct 10 2010;202(1-3):e45-47.
- Helander A, Olsson I, Dahl H. Postcollection synthesis of ethyl glucuronide by bacteria in urine may cause false identification of alcohol consumption. Clin Chem. Oct 2007;53(10):1855-1857.
- Helander A, Hagelberg CA, Beck O, Petrini B. Unreliable alcohol testing in a shipping safety programme. Forensic Sci Int. Aug 10 2009;189(1-3):e45-47.
- Sarkola T, Dahl H, Eriksson CJ, Helander A. Urinary ethyl glucuronide and 5-hydroxytryptophol levels during repeated ethanol ingestion in healthy human subjects. Alcohol Alcohol. Jul-Aug 2003;38(4):347-351.
- Jatlow P, O’Malley SS. Clinical (nonforensic) application of ethyl glucuronide measurement: are we ready? Alcohol Clin Exp Res. Jun 2010;34(6):968-975.
- Helliker K. A test for alcohol–and its flaws. The Wall Street Journal2006.
- Administration SAaMHS. The role of biomarkers in the treatment of alcohol use disorders. In: Advisory SAT, ed2006:1-7.
- Bodenheimer T. Uneasy alliance–clinical investigators and the pharmaceutical industry. N Engl J Med. May 18 2000;342(20):1539-1544.
- Bekelman JE, Li Y, Gross CP. Scope and impact of financial conflicts of interest in biomedical research: a systematic review. JAMA. Jan 22-29 2003;289(4):454-465.
- Stelfox HT, Chua G, O’Rourke K, Detsky AS. Conflict of interest in the debate over calcium-channel antagonists. N Engl J Med. Jan 8 1998;338(2):101-106.
Share this:

An Open Letter to Senator Elizabeth Warren Regarding Laboratory Developed Tests, Physician Health Programs and Institutional Injustice

I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.

Share this:

EtG–The Rosie Ruiz of Bent Science and Bad Medicine
The Displacement of the idea that facts and evidence matter, by the idea that everything boils down to subjective interests and perspectives is — second only to American political campaigns — the most prominent and pernicious manifestation of anti-intellectualism in our time. — Larry Laudan, Science and Relativism (1990)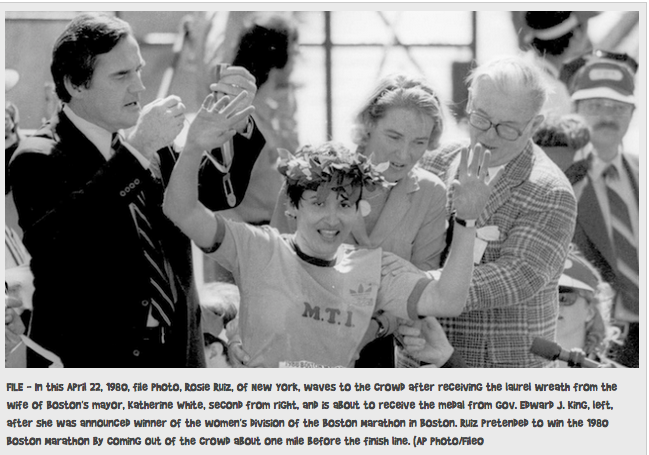 On April 21, 1980 Rosie Ruiz appeared to win the 84th Boston Marathon’s female category with a time of 2:31:56. Her time would have been the fastest female time in Boston Marathon history and and the third-fastest female time ever recorded in any marathon.
On April 21, 1980 Rosie Ruiz appeared to win the 84th Boston Marathon’s female category with a time of 2:31:56. Her time would have been the fastest female time in Boston Marathon history and and the third-fastest female time ever recorded in any marathon.
“Miss Ruiz, an administrative assistant for Metal Trading Inc. in Manhattan, received the traditional laurel wreath, a medal and a silver bowl for her victory,” According to the New York Times
Ruiz was unknown in the running world and her victory raised suspicions. After studying marathon photographs she didn’t appear in any of them until the very end and conducting interviews.
The problem was that, according to Runners World: “Ruiz had dropped out of the race, hopped on the subway, got off about a mile from the finish line, and ran in from there.” It is believed Ruiz intended to jump in in the middle of the pack but miscalculated when she joined so close to the end not realizing she was ahead of the other 448 female runners.
Marathon officials stripped Ruiz of her title on April 29, 1980, and named Jacqueline Gareau of Canada the women’s division champion with a time of 2:34:28. It was later discovered that she had also taken the subway during part of the New York City Marathon which qualified her for the Boston Marathon. In 1982 she was caught stealing money from her employer and was subsequently caught selling drugs to an undercover officer in Florida.
In the early 1950’s it was discovered that a small fraction of ingested alcohol in rabbits gets metabolized by conjugation with glucuronic acid to form Ethyl Glucuronide (EtG)..1,2 The potential of EtG as a marker for alcohol consumption was recognized in the 1990s and analytical methods for its determination were developed in urine, blood and hair.3-5
It’s use as a marker of alcohol consumption in forensic settings was subsequently suggested by Dr. Friedrich Wurst based on studies showing that urine EtG could be detected after complete elimination of alcohol from the body (up to 80 hours), and he suggested the alcohol biomarker be utilized in forensic monitoring to improve public health. 6,7
Wurst et al note that a “marker of high sensitivity and specificity capable of monitoring patients in treatment for alcohol or other drug abuse” could “improve therapy outcome and quality of life in patients, increase safety at work places and in traffic, avoid harm to the unborn during pregnancy (fetal alcohol syndrome) and reduce costs by making therapy more effective and reducing productivity loss.”7
A literature search from 1952 to 2002 yields one conclusion and once conclusion only; EtG measurements increase with alcohol ingestion. There are no studies considering what other factors might increase EtG measurements.
The false logic takes the following form:
- Premise: Event A occurred after (or with) event B.
- Conclusion: Therefore, event A caused event B.
But in 2003 Wurst and Gregory Skipper, M.D., FASAM, Medical Director of the Alabama Physician Health Program reported at an international meeting of the American Medical Society that EtG provided proof of alcohol consumption as much as 5 days after drinking an alcoholic beverage and that there are now a substantial number of studies in the world literature that support the clinical importance and reliability of EtG as a marker of recent alcohol consumption.8
“In the future it will be negligent not to test for EtG when monitoring recovering alcoholics,” reported Dr. Skipper.8
Also, in 2003, Skipper pitched the test to National Medical Services, Inc. (NMS labs) who then developed it as a Laboratory Developed Test (LDT).9
Because of its high sensitivity the newly marketed test was suggested as a tool to monitor health care professionals by Skipper in 2004.10 Skipper then approached the Federation of State Medical Boards and pitched the test to them proposing it be used in the assessment and monitoring of doctors by state Physician Health Programs. In a stunning example of policy entrepreneurship a market was created and filled simultaneously.

“Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs”11 published in the Journal of Medical Licensure and Discipline in 2004 found that “surreptitious alcohol use was a significant concern” for state Physician Health Programs (PHPs) yet no “best methods for detecting alcohol use.” The 36-question phone interview was conducted with directors of PHPs in 46 states regarding current methods of drug testing and notes: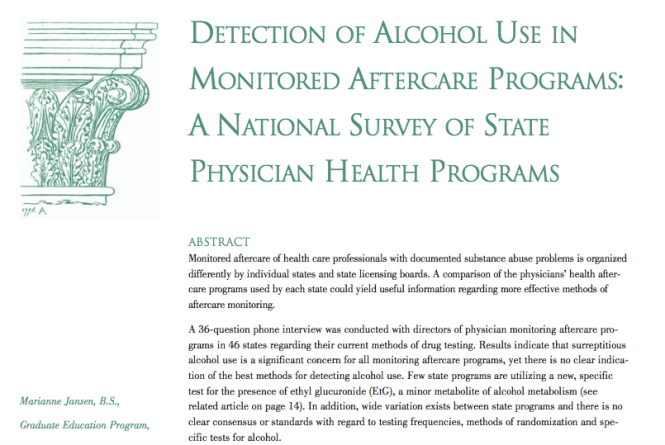
“Because alcohol is the most frequently abused substance adequate monitoring for alcohol is a major concern. During rehabilitation and recovery, the potential for alcohol abuse may increase due to the lack of efficient screening tests. The ingestion of alcohol while in aftercare is a violation of the contractual agreement made with the monitoring program and may lead to relapse and/or abuse of other psychoactive substances, thus rendering the practitioner unsafe to practice their profession. Therefore, alcohol detection remains an important component of contract compliance and sobriety.”
 They conclude that: “EtG can be detected in urine as long as 18 hours after blood alcohol levels reach zero and demonstrates exceptional specificity (100 percent) and sensitivity because even small amounts of alcohol (7 g, or less than one alcoholic beverage) can be detected.”
They conclude that: “EtG can be detected in urine as long as 18 hours after blood alcohol levels reach zero and demonstrates exceptional specificity (100 percent) and sensitivity because even small amounts of alcohol (7 g, or less than one alcoholic beverage) can be detected.”
This very same issue of the Journal of Medical Licensure and Discipline contains an article written by Skipper concerning new marker to detect alcohol use in “recovering physicians” that “has recently been introduced in the United States and an assay for EtG is now commercially available.”12

Skipper states that “EtG is not detectable unless alcohol has been consumed” and notes the “usefulness of the test was affirmed in one study involving psychiatric inpatients”
An EtG above 500 renders it “extremely unlikely” that alcohol was not ingested and adds “ In any event, if testing is positive” in monitored doctors it is advisable to refer them for further in-depth evaluation by clinicians or programs skilled and adept at evaluating physicians.”
In Bending Science: How Special Interests Corrupt Public Health Research13, Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using distorted or “bent” science to influence legal, regulatory and public health policy.
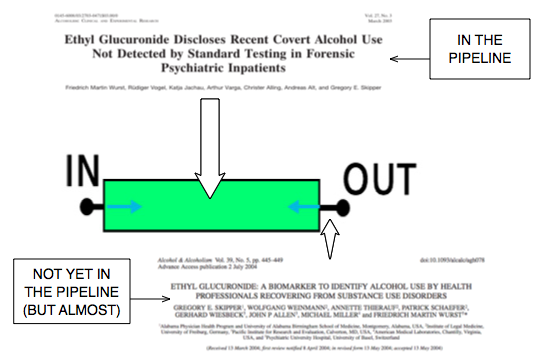
The authors describe a “separatist view” of the world that assumes scientific research is sufficiently reliable for public policy deliberations and legal proceedings once it flows out of the realm of science through a pipeline in which the scientific community has ensured through rigorous peer-review and professional oversight that the final product that exits the pipeline is unbiased and produced in accordance with the norms and procedures of science.

This view does not consider the possibility that the scientific work exiting the pipeline could be distorted and contaminated by biasing influences.
If we look at this through the lens of “bent science” several issues arise including a failure to adhere to the norms and standards of toxicology and forensic drug and alcohol testing, an absence of evidence base and glaring conflicts of interests.
Norms and Standards of Toxicology and Forensic Drug Testing
On September 15, 1986 President Ronald Reagan signed Executive Order 12,564 requiring that the urine of federal employees in “sensitive” jobs be sampled randomly for illegal drugs. In 1988 Congress followed with the Drug-Free Workplace Act and drug testing became common organizational practice by the mid 1990s. Most followed the federal norms and procedures in their testing.
The Department of Health and Human Services (DHHS) had established specific cutoff levels that define a positive result. These values were developed to help eliminate false-positive results.14 The cutoff levels were originally established at a drug concentration that produced an analytic signal some multiplicative factor above the noise level (the signal obtained from drug free urine).
“The concept of cutoff for major urine screening programs has two basic applications: the lower limit of reliable testing based on the techniques involved in the testing and the lower limit of reliable testing based on the possibility of interference from medications, foodstuffs, environmental exposure, or endogenous processes.”15
“Urine Drug Testing in Clinical Practice: Dispelling the myths & Designing Strategies cautions about “caveats to interpretation.” “As with any unexplained test result, it is important to clarify the interpretation with someone knowledgeable in clinical toxicology.”16
Evidence Base
What was in the pipeline when the EtG was proposed as a forensic monitoring tool can be illustrated below:
Taking Advantage of a Loophole
The EtG was developed by NMS labs as a “Laboratory—Developed Test” or LDT. The LDT pathway does not even require proof of validity, that the test is actually testing for what it claims to be testing, and with no FDA oversight a lab can claim any validity it wants in its marketing and sales, and they did. Proponents for regulation of LDTs argue this lack of oversight is a direct threat to patient care and safety. An viewpoint piece in JAMA states that a “patient’s life or death could hinge on whether a single, unregulated diagnostic test result is meaningful.” 17
In the case of EtG Skipper arbitrarily chose a value of 100 as a cut-off for EtG. The rationale behind this value is not cited. Interference with foods, medications and environmental exposures had not been worked out. The results were predictable.
Aftermath was Predictable and Therefore Avoidable
The case of EtG is exemplifies ‘policy entrepreneurship” and “bent science” at its worst. It shows how junk-science can be introduced into the market without any real difficulties or meaningful opposition and how self-interest is promoted in defiance of science in an effort to manipulate public policy. This is nothing more than opportunist exploitation of the regulatory framework and the FSMB eagerly complied. Without this “regulatory sanctification” none of these tests would have ever made it to market.
EtG was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash18,19, hand sanitizer gel20, nonalcoholic beer21, and nonalcoholic wine.22
“Exposure to ethanol-containing medications, of which there are many, is another potential source of “false” positives.
Forbidding patients/subjects access to such medications may be unrealistic, and even unwise.”23
The United States Substance Abuse and Mental Health Services Administration warned against using a positive EtG as primary or sole evidence of drinking for disciplinary or legal action.24 The advisory states:
“Although positive biomarker results should be taken seriously, use of certain biomarkers, such as EtG, is now warranted as stand-alone confirmation of relapse because research has not yet established an acceptable standard to distinguish possible exposure to alcohol in various commercial products from consumption of alcoholic beverages.”
The Wall Street Journal in 2006 reported the problems with the EtG to the general public.25
The authors of a 2011 study demonstrating that hand sanitizer alone could result in EtG concentrations of 1998 concluded that:
“in patients being monitored for ethanol use by urinary EtG concentrations, currently accepted EtG cutoffs do not distinguish between ethanol consumption and incidental exposures, particularly when urine specimens are obtained shortly after sustained use of ethanol containing hand sanitizer.”26
 Sauerkraut and bananas have even recently been shown to cause positive EtG levels.27
Sauerkraut and bananas have even recently been shown to cause positive EtG levels.27
A 2010 study found that consumption of baker’s yeast with sugar and water28 led to the formation of elevated EtG above the standard cutoff.
EtG can originate from post-collection synthesis if bacteria is present in the urine.29 Collection and handling routines can result in false-positive samples.30
EtG varies among individuals.31 Factors that may underlie this variability include gender, age, ethnic group, and genetic polymorphisms.

The Cochrane Collaboration does systematic reviews of the literature using conscientious, explicit, and judicious criteria to in order to produce and disseminate only high quality and evidenced based health care, exclude bias, and enhance transparency.
The Cochrane database is internationally recognized as the standard in evidence based health care. It records just 5 controlled trials under the topic ethyl glucuronide.22,31-33
These 5 studies represent the only high-quality evidence regarding EtG to date. Information provided by the five studies suggests the following, and only the following:
- EtG measurements increase with alcohol ingestion.
- The window of detection is shorter than what is commonly proposed (80 hours).
- Individual values are variable both within and between subjects.
- Non-alcoholic wine can cause positive levels.
During this time period any rational authority would have admitted error and removed the test from the market. Skipper’s approach was to keep raising the cutoff level from 100 to 250 to 500 to 1000. With EtG paving the way for other laboratory developed tests he then added “confirmatory” LDTs such as EtS and PEth. The EtS was found to have the same problems and PEth inevitably will but this is now a billion dollar market and they plan on using these tests on almost everyone including kids.
There has been no academic, public policy or conflict of interest analysis of all of this. As probably the worst case of bent-science in history there needs to be.
- Kamil A, Smith JN, Williams RT. A New Aspect of Ethanol Metabolism: Isolation of ethylglucuronide. Biochemical Journal. 1952;51:32-33.
- Kamil IA, Smith JN, Williams RT. Studies in detoxication. L. The isolation of methyl and ethyl glucuronides from the urine of rabbits receiving methanol and ethanol. The Biochemical journal. Jun 1953;54(3):390-392.
- Schmitt G, Aderjan R, Keller T, Wu M. Ethyl glucuronide: an unusual ethanol metabolite in humans. Synthesis, analytical data, and determination in serum and urine. Journal of analytical toxicology. Mar-Apr 1995;19(2):91-94.
- Schmitt G, Droenner P, Skopp G, Aderjan R. Ethyl glucuronide concentration in serum of human volunteers, teetotalers, and suspected drinking drivers. Journal of forensic sciences. Nov 1997;42(6):1099-1102.
- Aderjan RE. Ethyl glucuronide. A non-volatile ethanol metabolite in hair. 1995.
- Wurst FM, Seidl S, Alt A, Metzger J. [Direct ethanol metabolite ethyl glucuronide. Its value as alcohol intake and recurrence marker, methods of detection and prospects]. Psychiatrische Praxis. Nov 2000;27(8):367-371.
- Wurst FM, Seidl S, Ladewig D, Muller-Spahn F, Alt A. Ethyl glucuronide: on the time course of excretion in urine during detoxification. Addiction biology. Oct 2002;7(4):427-434.
- Martin DM, G.E. S, Costantino A. Alcohol Use Can Now be Detected for Days Rather than Hours Using a New Test, Ethyl Glucuronide. 2003; http://www3.firstlab.com/media/16032/EtGFirstLabReport.pdf.
- Skipper G. “Urine Luck” Overview of New Drug Testing Technologies and Conundrums. http://gregskippermd.weebly.com/uploads/7/4/7/5/74751/skipper.urine_luck_2014_aaap_meeting.pdf. Accessed March 17, 2015.
- Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
- Jansen M, Bell LB, Sucher MA, Stoehr JD. Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs. Journal of Medical Licensure and Discipline. 2004;90(2):8-13
- Skipper G, Weinmann W, Wurst F. Ethylglucuronide (EtG): A New Marker to Detect Alcohol Use in Recovering Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):14-17.
- McGarity TO, Wagner WE. Bending Science: How Special Interests Corrupt Public Health Research. Cambridge, MA: Harvard University Press; 2008.
- US Department of Health and Human Services. Mandatory guidelines and proposed revisions to mandatory guidelines for federal workplace drug testing programs: notices. Federal Register. April 13, 2004;69(71):19659-19660.
- Clark HW. The role of physicians as medical review officers in workplace drug testing programs. In pursuit of the last nanogram. West J Med. May 1990;152(5):514-524.
- Resnick RB, Volavka J, Freedman AM, Thomas M. Studies of EN-1639A (naltrexone): a new narcotic antagonist. Am J Psychiatry. Jun 1974;131(6):646-650.
- Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
- Costantino A, Digregorio EJ, Korn W, Spayd S, Rieders F. The effect of the use of mouthwash on ethylglucuronide concentrations in urine. Journal of analytical toxicology. Nov-Dec 2006;30(9):659-662.
- Reisfield GM, Goldberger BA, Pesce AJ, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. Journal of analytical toxicology. Jun 2011;35(5):264-268.
- Rosano TG, Lin J. Ethyl glucuronide excretion in humans following oral administration of and dermal exposure to ethanol. Journal of analytical toxicology. Oct 2008;32(8):594-600.
- Thierauf A, Gnann H, Wohlfarth A, et al. Urine tested positive for ethyl glucuronide and ethyl sulphate after the consumption of “non-alcoholic” beer. Forensic Sci Int. Oct 10 2010;202(1-3):82-85.
- Hoiseth G, Yttredal B, Karinen R, Gjerde H, Christophersen A. Levels of ethyl glucuronide and ethyl sulfate in oral fluid, blood, and urine after use of mouthwash and ingestion of nonalcoholic wine. J Anal Toxicol. Mar 2010;34(2):84-88.
- Jatlow P, O’Malley SS. Clinical (nonforensic) application of ethyl glucuronide measurement: are we ready? Alcohol Clin Exp Res. Jun 2010;34(6):968-975.
- Administration SAaMHS. The role of biomarkers in the treatment of alcohol use disorders. In: Advisory SAT, ed2006:1-7.
- Helliker K. A test for alcohol–and its flaws. The Wall Street Journal2006.
- Reisfield GM, Goldberger BA, Crews BO, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after sustained exposure to an ethanol-based hand sanitizer. Journal of analytical toxicology. Mar 2011;35(2):85-91.
- Musshoff F, Albermann E, Madea B. Ethyl glucuronide and ethyl sulfate in urine after consumption of various beverages and foods–misleading results? Int J Legal Med. Nov 2010;124(6):623-630.
- Thierauf A, Wohlfarth A, Auwarter V, Perdekamp MG, Wurst FM, Weinmann W. Urine tested positive for ethyl glucuronide and ethyl sulfate after the consumption of yeast and sugar. Forensic Sci Int. Oct 10 2010;202(1-3):e45-47.
- Helander A, Olsson I, Dahl H. Postcollection synthesis of ethyl glucuronide by bacteria in urine may cause false identification of alcohol consumption. Clinical chemistry. Oct 2007;53(10):1855-1857.
- Helander A, Hagelberg CA, Beck O, Petrini B. Unreliable alcohol testing in a shipping safety programme. Forensic science international. Aug 10 2009;189(1-3):e45-47.
- Sarkola T, Dahl H, Eriksson CJ, Helander A. Urinary ethyl glucuronide and 5-hydroxytryptophol levels during repeated ethanol ingestion in healthy human subjects. Alcohol and alcoholism. Jul-Aug 2003;38(4):347-351.
- Hoiseth G, Bernard JP, Stephanson N, et al. Comparison between the urinary alcohol markers EtG, EtS, and GTOL/5-HIAA in a controlled drinking experiment. Alcohol and alcoholism. Mar-Apr 2008;43(2):187-191.
- Wojcik MH, Hawthorne JS. Sensitivity of commercial ethyl glucuronide (ETG) testing in screening for alcohol abstinence. Alcohol and alcoholism. Jul-Aug 2007;42(4):317-320.

Share this:

An Open Letter to Senator Elizabeth Warren Regarding Laboratory Developed Tests, Physician Health Programs and Institutional Injustice

—There is no place in science for consensus or opinion, only evidence.-Claude Bernard
Dear Senator Warren,
Thank you for your reply regarding laboratory developed tests (LDTs) and the need for regulatory oversight. As you mention, LDTs are developed without FDA approval—a pathway in which is not even necessary to prove validity of a test (that it is actually testing what it claims to be testing for) to bring it to market. With no FDA oversight or regulation a commercial lab can claim any validity they want in marketing these tests. The regulation debate has focused on the reliability and validity of a number of clinical tests marketed with unverified claims of accuracy such as prenatal screening and Lyme disease and this lack of oversight is a direct threat to patient safety.
I am sure you would agree with me that the importance of tests diagnostic accuracy is directly proportional to that tests potential to cause patient harm if reported inaccurately.
Sensitivity and specificity are important components of any diagnostic test because there are consequences associated with both false-positive and false negative results.
A test falsely indicating the absence of a condition in someone who truly has it can delay or prevent needed treatment wile a test falsely indicating the presence of a condition in someone who does not truly have it can result in unnecessary testing and treatment.
Incorrect treatment and false labeling of patients can also occur. Therefore diagnostic accuracy is paramount if a test is being used as the basis for further tests and treatment. Any test being used as a basis for further tests or treatment needs to be accurate. It needs to be reliable and valid. Moreover, if the consequences of a test can result in significant patient harm (such as unneeded chemotherapy) it needs to be either 100% accurate or be combined with other tests to confirm the true diagnosis.
“Forensic” vs. “Clinical” Laboratory Testing
“Forensic” testing differs from “clinical” testing because of the consequences and the process is tightly controlled because false-positive results are unacceptable as the consequences can be grave, far-reaching and even permanent.
Forensic testing demands special handling and safeguards to protect the donor such as validated tests, certified labs, strict chain-of-custody procedures and MRO (Medical Review Officer) review. These safeguards of quality control assure the validity and integrity of the specimen. The LDT pathway was not designed for forensic tests.
Forensic Laboratory Developed Tests (LDTs)
Paradoxically, laboratory developed tests with the potential to cause life-changing and possibly irreparable harm have been absent from the regulatory debate; LDT drug and alcohol tests used for “forensic” monitoring purposes.
A panoply of tests using urine, blood, hair, fingernails breath and saliva have been developed and brought to market since 2003 when the first one was introduced by Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, who “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.” 1
Developed as an LDT, Skipper and NMS then claimed the alcohol biomarker (which was discovered in the 1950s) “appeared to be 100 percent specific” in detecting covert use of alcohol based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male. 2 With this “evidence-base” and a not yet published paper in the pipeline,3 Skipper then pitched the test to the Federation of State Medical Boards (FSMB) as an accurate and reliable tool detect covert alcohol use in health care professionals.
Policy Entrepreneurship
In “Agendas, Alternatives, and Public Policies,”4 John W. Kingdon describes the problem, policy and political streams involved in public policy making. When these three streams come together a specific problem becomes important on the agenda, policies matching the problem get attention, and then policy change becomes possible.
Kingdon also describes “policy entrepreneurs’ who use their knowledge of the process to further their own policy ends. They ‘lie in wait… with their solutions at hand, waiting for problems to float by to which they can attach their solutions, waiting for a development in the political stream they can use to their advantage.”4
And due to a perfect confluence of streams ( Institute of Medicine report that 44,000 people die each year due to medical error,5 media reports of “impaired physicians,” the the war-on-drugs, etc.) the FSMB was swayed into accepting not just the validity but the necessity of using an alcohol biomarker of unknown reliability and validity on doctors referred to or monitored by state Physician Health Programs (PHPs) .
As the national organization that gives guidance to state medical boards through public policy development and recommendations, the individual state medical boards adopted use of the test without critical appraisal and no meaningful opposition.
Shortly after its founding in 1912, the FSMB began publishing a journal called the Quarterly of the Federation of State Boards of the United States. Now known as the Journal of Medical Regulation, the publication has archived all issues with full articles dating back to 1967 and, as the official journal of the national organization involved in medical licensing and regulation this facilitates an unskewed and impartial examination of how and when specific issues and problems were presented and who presented them and, in doing so, the “policy entrepreneurship” Kingdon describes can be seen quite clearly. For example a 1995 issue containing articles written by the program directors of PHPs in 8 different states contains an FSMB editorial acknowledging the reported 90% success rate claimed of these programs (in part attributed to the 90-day inpatient treatment programs) that concludes:
“Cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” 6
No one bothered to examine the methodology of these reports to discern the validity of the claims and it is this acceptance of faith without objective assessment that has allowed the passage of flawed public policy in medical regulation.
Nowhere is “policy entrepreneurship” more glaringly displayed as it is in a 2004 issue promoting the use of EtG in monitoring doctors as under the same cover is an article identifying both the need7 for such a test and an article providing the solution.8
“Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs,” a survey of state Physician Health Programs (PHPs) concludes that “surreptitious alcohol use” is a significant concern” for PHPs, there is no current “best method” for detection, but a promising new test with “exceptional specificity (100 percent) and sensitivity” in detecting small amounts of alcohol for up to 18 hours has recently become available.7
This same issue contains an article authored by Skipper about a new marker “not detectable unless alcohol has been consumed” recently introduced in the United States and now commercially available.”8
Notably absent from both of these articles is Skipper’s role in the commercial availability of the test. This conflict-of-interest is nowhere mentioned in this display of “creating a market then filling it.”
This “regulatory sanctification” of the test implied its tacit approval by the medical profession (i.e. “if they are using it on doctors it must be valid”) and facilitated its marketing to other monitoring agencies (nurses, airline pilots) as well as Courts and Probation Departments where those doing the monitoring had absolute power while those being monitored had no voice.
In Bending Science: How Special Interests Corrupt Public Health Research9, Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using carefully crafted distorted or “bent” science to influence legal, regulatory and public health policy. The authors describe how those making these decisions often assume the information that reaches them has been sufficiently vetted by the scientific community as it flows through a pipeline of rigorous peer-review and professional oversight and that the final product that exits the pipeline is unbiased and produced in accordance with the norms and procedures of science.
McGarity and Wagner note the serious and sometimes horrific consequences of bent science and provide examples involving Tobacco and Big Pharma . The authors call for:
“..immediate action to reduce the role that bent science plays in regulatory and judicial decision making” and the need for the scientific community to be involved in “designing and implementing reform.”
“Shedding even a little light on how advocates bend policy -relevant science could go a long way toward remedying these problems. Indeed, precisely because the advocates have overtaken the law in this area, heightened attention to the social costs of bending science could itself precipitate significant change.”
In the case of EtG this shedding of light is not very hard as no “carefully crafted” studies bending science were used to sway opinion. None existed. The only items in the pipeline were directly related to Skipper. If anyone dare to look, the Emperor has no clothes.
Lack of Answerability and Accountability
There are difficulties in challenging bent science including a general lack of recognition of the problem and an absence of counter-studies to oppose deliberately manufactured ends-oriented research. This has proven true with the myriad LDTs introduced into the marketplace as no counter-forces or competing economic interests producing counter-studies exist.
Multiple lawsuits, including a class-action, have been decided in favor of the labs who have taken a stand-your-ground approach supported by a body of industry-related “research” they or their affiliates produced to support the validity and reliability of the tests.
Those affected by these tests either have no power or have had their power removed. Most do not have the resources to mount a defense let alone produce counter-studies questioning the reliability and validity of the tests.
Most employee drug testing follows Department of Health and Human Services (DHHS) guidelines using FDA-approved tests that have specific cutoff levels defining a positive-result in an effort to eliminate false-positive results.10 Procedural safeguards are in place in these programs to protect the donor. Forensic testing programs using LDTs provide no such safeguards as the testing is unregulated and there is no oversight from outside actors.
Unlike clinical LDTs “forensic” LDTs are even exempt from CLIA oversight. The only avenue for complaint is through the College of American Pathologists (CAP) and, as an accrediting agency, they can only address problems by ensuring compliance with CAP guidelines. If an investigation concludes lab error or misconduct CAP can mandate the lab correct the test result and come into compliance with their guidelines under threat of loss of accreditation but no other consequences exist. Accountability has been removed yet the consequences to those harmed by these are significant and without remedy.
State Physician Health Programs
As is the case with the LDTs they introduced, Physician Health Programs have no oversight or regulation. A 2013 Audit of the North Carolina PHP 11 prompted by complaints from doctors and performed by State Auditor Beth Woods found absolutely no oversight of the program by either the state medical board or medical society and that “abuse could occur without being detected.”
The Audit also found that doctors were predominantly referred to the same “PHP-approved” out-of-state facilities to which they in part attribute their high success rates in treatment. Interestingly the PHP could not identify what quality indicators or quantitative measurements were used by the PHP to “approve” the “PHP-approved” facilities.
In January of 2015 a Federal class action lawsuit was filed in the Eastern District of Michigan against the state PHP program and found health care providers were subject to the same referral system using these out-of-state facilities. The suit alleges constitutional violations related to the forced medical treatment of health care professionals and the “callous and reckless termination of professional licenses without due process.” 12
As with North Carolina, the Michigan PHP will be unable to provide what quality indicators and quantitative measurements are being used to “qualify” and “approve these facilities. None exist. The sole indicators for approving these assessment centers are ideological and economic. In fact, the medical directors of most, if not all, of these facilities can be seen on this list of “like-minded docs.”
You once said “People feel like the system is rigged against them. And here’s the painful part: they’re right. The system is rigged.”
As the Michigan lawsuit notes: “Unfortunately, a once well-meaning program has turned into a highly punitive and involuntary program where health professionals are forced into extensive and unnecessary substance abuse/dependence treatment under the threat of the arbitrary application of pre-hearing deprivations.”
This has become the rule not the exception. The Federation of State Physician Health Programs (FSPHP), the same group to which Dr. Skipper belongs, has systematically taken over these programs state by state by removing competent and caring doctors not agreeing with the groupthink and silenced them under threat of litigation if they violate their confidentiality agreements and “peer review” statutes.
The same system of coercion, control and abuse exists in Massachusetts. In the past week alone I have heard from a medical student, a resident and two doctors who complained of misconduct misconduct involving fraudulent testing and falsified diagnoses.
In “Ethical and Managerial Considerations Regarding State Physician Health Programs,” published in the Journal of Addiction Medicine in 2012, Drs. John Knight, M.D. and J. Wesley Boyd, M.D., PhD who collectively have more than 20 years experience with the Massachusetts Physician Health Program (PHP) state that:
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”13
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 13
They recommend the relationship between PHP’s and the evaluation and treatment centers and licensing boards be transparent and that national standards be developed “that can be debated by all physicians, not just those who work within PHPs.”13
Accountability, or answerability, is necessary to prevent corruption. This requires both the provision of information and justification for actions. What was done and why? Accountability also requires that consequences be imposed on those who engage in misconduct.
In discussing the financial conflicts-of-interest between PHPs and “PHP-approved” assessment centers Knight and Boyd state:
“..if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.”
To “consciously tailor a diagnosis” is fraud. It is political abuse of psychiatry. And it is not only the assessment and treatment centers willing to “tailor” a diagnosis; so too are the labs involved.
Physician Suicide
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.
The Massachusetts Medical Society and Massachusetts DPH claim no oversight of the Massachusetts PHP, PHS.inc. The Massachusetts Board of Registration in Medicine (BORM) will not address ethical or even criminal complaints about the doctors involved in the PHP and there is good evidence that some members of the BORM are in fact complicit in unethical and even criminal behavior. As the Massachusetts AGO represents the BORM they defer issues back to them and dig no deeper.
Drs. Knight and Boyd have suggested State Audits and we are hoping that MA State Auditor Suzanne Bump will investigate the MA PHP and the Board of Registration in Medicine’s Physician Health and Compliance Unit shortly.
One major problem is that barriers have been put in place to prevent information from getting to the right people.
The majority of people at medical societies, boards, departments of public health and other organizations are individuals of integrity and honesty but the system has been erected so that valid complaints are deflected, delayed, dismissed or otherwise tabled by sympathizers, apologists and those complicity. The criminal activity the Massachusetts PHP is engaging in is undeniable and indefensible but who is going to hold them to account?
It is going to take a while to reform this system of institutional abuse and it has to be done state by state. Please take a look at the facts and documentary evidence and help me hold them accountable. This needs to be exposed, acknowledged and addressed. Doctors are dying from this system of institutional abuse. It is a public health emergency no one is talking about. Yet those behind the PHP programs are claiming this system of coercion, abuse and control is the “gold standard” of addiction treatment and, using another loophole, they want to expand this system to mainstream healthcare.
Sincerely,
Michael L. Langan, M.D.
- Skipper G. Exploring the Reliability, Frequency, and Methods of Drug Testing: What is Enough to Ensure Compliance?: Alcohol Markers and Devices. 2013; http://www.fsphp.org/Skipper, Exploring the Reliability Frequency and Methods 2 Presentation.pdf.
- Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcoholism, clinical and experimental research. Mar 2003;27(3):471-476.
- Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
- Kingdon JW. Agendas, alternatives, and public policies. Updated 2nd ed. Boston: Longman; 2011.
- Leape LL. Institute of Medicine medical error figures are not exaggerated. JAMA : the journal of the American Medical Association. Jul 5 2000;284(1):95-97.
- Schneidman B. The Philosophy of Rehabilitation for Impaired Physicians. The Federal Bulletin: The Journal of Medical Licensure and Discipline. 1995;82(3):125-127.
- Jansen M, Bell LB, Sucher MA, Stoehr JD. Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs. Journal of Medical Licensure and Discipline. 2004;90(2):8-13
- Skipper G, Weinmann W, Wurst F. Ethylglucuronide (EtG): A New Marker to Detect Alcohol Use in Recovering Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):14-17.
- McGarity TO, Wagner WE. Bending Science: How Special Interests Corrupt Public Health Research. Cambridge, MA: Harvard University Press; 2008.
- US Department of Health and Human Services. Mandatory guidelines and proposed revisions to mandatory guidelines for federal workplace drug testing programs: notices. Federal Register. April 13, 2004;69(71):19659-19660.
- Wood B. State of North Carolina Performance Audit North Carolina Physicians Health Program. . http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf. Accessed March 17, 2015.
- U.S. District Court Eastern District of Michigan, Case No: 2:15-cv-10337-AJT-RSW (2015). Carole Lucas, R.N., Tara Vialpandno, R.N., Scott Sanders, R.N., Kelly Schultz, P.A., and all other similarly situated health professionals v. Michigan Department of Licensing and Regulatory Affairs, Carole Engel, J.D.Former Director of Michigan Bureau of Health Professions, Ulliance, Inc. (State Contractor), Carolyn Batchelor (HPRP Contract Administrator), Stephen Batchelor (HPRP Contract Administrator), and Nikki Jones, LMSW. Filed January 30, 2015.
- Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.



Share this:

Integrity and Accountability—Defend the MRO Procedurally, Ethically or Legally and win 100 Volumes of the Classics in Medicine Library and Salk and Sabin Autographs!


- Sabin and Salk Autographs
“The incompetent or unprincipled physician, licensed to practice medicine by a too complaisant State, is the greatest menace to scientific medicine – as great a menace as all the cultists put together.” —Dr. Morris Fishbein (The Medical Follies. New York: Boni Liverlight, 1925 p. 71)
“There is no place in science for consensus or opinion, only evidence” —Claude Bernard

Sabin, Salk and the Classics in Medicine Library
Polio is nearly a thing of the past thanks to to Dr. Jonas Salk and Albert Sabin. In 1952 Salk discovered and developed the first successful vaccine for polio and combined with Albert Sabin’s 1961 oral vaccination the du0 effectively obliterated the contagious polio virus. Once a deadly threat to our country and future there were 93,000 cases of polio reported in the…
View original post 1,952 more words
Share this:

Still looking for Statisticians, Biostatisticians and Epidemiologists to debunk Junk-Science
 Wanted!–a Few Statisticians, Biostatisticians and Epidemiologists who want to make a difference in Medicine, Society and our Future
Wanted!–a Few Statisticians, Biostatisticians and Epidemiologists who want to make a difference in Medicine, Society and our FutureUp until the birth of the EtG, tests used for forensic drug and alcohol monitoring had to go through the arduous, expensive and necessary FDA approval process. The LDT pathway was designed to develop simple tests with little risk that have low market potential (i;e. the cost of the normal FDA approval process would prohibit them from coming to market). The LDT pathway was designed to improve patient care in the diagnosis and treatment of patients. It was not designed for forensic tests. LDT approval does not require in vivo testing. It is essentially an honor system and to develop an LDT it is not even necessary to prove that the test is actually testing what it is purportedly testing for (validity).
So with little to no evidence base an ASAM/FSPHP physician introduced the EtG, had it developed and marketed as a LDT in collusion with unscrupulous labs, and then began using it on physicians being monitored by State PHPs. This then spread to other monitoring organizations in which there was a large power-differential between those ordering the tests and those being tested (criminal-justice, other professional monitoring programs). These biomarkers have never been used in Federal Drug Testing, SAMHSA approved, DOT, and other organizations where unions or other organizations are present and looking out for the best interests of those being tested.
Share this:

Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug testing: The plan to Introduce Laboratory Developed Tests into Mainstream Healthcare

Chain-of-Custody refers to the document or paper trail showing the collection, control, transfer, analysis and disposition of laboratory tests. It is the written documentation of a specimen from the moment of collection to the final destination to the review and reporting of the final results. The multi-part chain-of-custody form or “custody and control” form is part and parcel of this process. It contains stickers to sign and seal the specimen so that it cannot be tampered with and the form itself is signed by the appropriate parties as the test specimen travels from place to place. Information is added to the form as it travels from person to person. It has been given the status of a legal document as it has the ability to invalidate a specimen with incomplete information. Once the sample is analyzed it is reviewed by a Medical Review Officer (MRO) for final review. In the case of a positive test it is the responsibility of the MRO to ascertain an intact chain-of-custody, determine whether an alternative explanation exists for the positive test such as a prescribed medication, and then and only then report the test as a “true positive.”
The MRO looks for what are called “fatal flaws” and, should one be present, invalidates the test. A fatal flaw requires the test be rejected as it were never drawn. It invalidates it and it cannot be used.  Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Specimen integrity is critical in forensic drug testing, but so too is the integrity of the people involved.
Forensic Versus Clinical Drug Testing
According to the ASAM White Paper on Drug Testing, clinical drug-testing “employs the same sound procedures, safeguard, and systems of information management that are used for all other health-related laboratory tests, tests on which life-and-death medical decisions are commonly made.” In the box below they describe the multiple safeguards in place and requirements demanded of “forensic” drug testing but do not mention the reason these uncompromising and multiple specifications exist is to protect the donor from a false accusation of drug or alcohol use. They proceed to define “clinical drug testing” as “part of a patient examination performed for the purposes of diagnosis, treatment, and the promotion of long term recovery” noting that clinical testing “must meet the established standards of medical practice and benefit the therapeutic relationship, rather than meeting the formal legal requirements of forensic testing.” The authors then state that the “majority of drug testing done today” includes both forensic and clinical elements using individuals on parole and probation as examples.
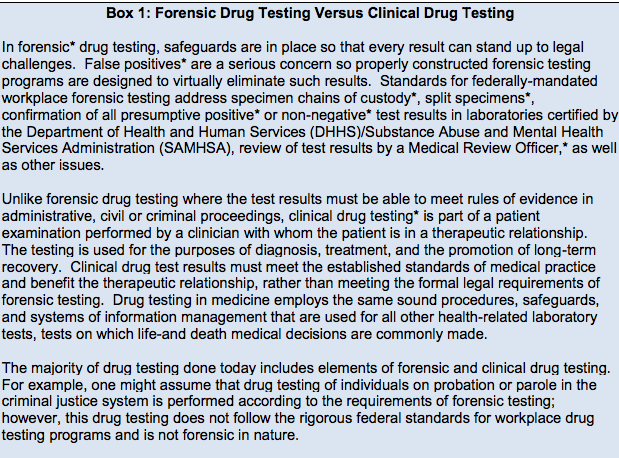
From the ASAM White Paper on Drug Testing
The logical fallacy here is striking. It is comparing apples and oranges. After detailing the specific quality assurance safeguards designed to prevent the donor of a drug or alcohol test from being falsely accused of illicit use, the authors give a general definition and purpose of “clinical” testing then state that when testing for drugs the systems in place are up to snuff as they are already being used to make “life-and-death medical decisions.” The take-home message is that “forensic” testing is unnecessary hyperbole designed for legal challenges. The clinical lab systems in place are used for critically important testing and can therefore be used for drug-testing–after all, parolees and probationers don’t require it.
Forensic guidelines were developed in collaboration with occupational and environmental medicine specialists, clinical and forensic toxicologists, pathologists and others and the recommended requirements agreed upon by this consortium exists solely to assure validity and accuracy in the testing process. These requirements exist to protect the donor and If the “clinical” testing context fit the bill then “forensic” testing would not have evolved.
Labs ordered clinically in the course of patient care are interpreted within the context of multiple other pieces of data. Lab errors occur all the time and are interpreted in that context. Oftentimes a lab will not fit with the clinical picture and, when that happens, a repeat lab is ordered for verification. Specimens get collected in the wrong tube and specimens get lost but in the clinical setting they simply get reordered and there are no consequences to patient care. In contrast drug testing is an all-or-none one-shot test and the results have consequences. It is for that reason they must be valid. Chain-of-custody and MRO review are critical and that is why most drug-testing programs follow the forensic protocol. And the example of non-forensic drug-testing parolees and probationers is misleading. Any Employee Assistance Program that has a union or some other group looking out for their best interests uses strict “forensic” guidelines. Parolees and probationers have no power and have no choice. Besides, the National Association of Drug Court Professionals uses the Laboratory Developed Tests these same people introduced to test individuals on probation or parole in the criminal justice system just as they do in the PHPs.
The ASAM White Paper:
“Encourages wider and “smarter” use of drug testing within the practice of medicine and, beyond that, broadly within American society. Smarter drug testing means increased use of random testing* rather than the more common scheduled testing,* and it means testing not only urine but also other matrices such as blood, oral fluid (saliva), hair, nails, sweatand breath when those matrices match the intended assessment process. In addition, smarter testing means testing based upon clinical indication for a broad and rotating panel of drugs”
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.
A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.