The 12-red flags below are very applicable to American Society of Addiction Medicine (ASAM) related consensus and public policy. When viewed through this lens the science and research all falls apart.
(1) When different claims get bundled together.
(2) When ad hominem attacks against dissenters predominate.
(3) When scientists are pressured to toe the party line.
(4) When publishing and peer review in the discipline is cliquish.
(5) When dissenting opinions are excluded from the relevant peer-reviewed literature not because of weak evidence or bad arguments but as part of a strategy to marginalize dissent.
(6) When the actual peer-reviewed literature is misrepresented.
(7) When consensus is declared hurriedly or before it even exists.
(8) When the subject matter seems, by its nature, to resist consensus.
(9) When “scientists say” or “science says” is a common locution.
(10) When it is being used to justify dramatic political or economic policies.
(11) When the “consensus” is maintained by an army of water-carrying journalists who defend it with uncritical and partisan zeal, and seem intent on helping certain scientists with their messaging rather than reporting on the field as objectively as possible.
(12) When we keep being told that there’s a scientific consensus.


At a glance: this drug in 2012
413K
Medicare Part D Claims$147M
Retail Cost
Suboxone Cost by State – Top 10 – State Claims Cost Massachusetts 51,132 $15M Pennsylvania 26,679 $9.16M New York 24,069 $9.03M Michigan 19,746 $7.72M Florida 19,403 $7.59M Ohio 18,201 $6.22M Kentucky 17,427 $5.66M Tennessee 16,108 $5.49M California 15,232 $6.03M Texas 14,8 $5.88M
Complete list via ProPublica: http://projects.propublica.org/checkup/drugs/2017
Top 10 prescribers of Suboxone: names & cities not included in this blog post – available via ProPublica – Provider Medicare Claims State Internal Medicine 2,583 Alabama Psychiatry 1,329 Massachusetts M.D Specialist 1,08 Indiana Psychiatry 898 Massachusetts Family Medicine 861 Michigan Addiction Medicine 852 Michigan Family Medicine 825 Alabama Emergency Medicine 743 Tennessee Specialist 681 Vermont Adult Medicine 671 Pennsylvania
Complete list via ProPublica: http://projects.propublica.org/checkup/drugs/2017
View original post 884 more words


As the Medical Review Officer (MRO) for the Massachusetts state Physician Health Program (PHP), Physician Health Services, Inc. (PHS, inc.), Dr. Wayne Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody in any and all drug and alcohol testing is intact before reporting a test as positive.

Note Dr Gavryck is: 1. Certified by ASAM; 2. A .Certified Medical Review Officer (MRO) who “serves PHS in this capacity.” Although Dr. Gavryck serves PHS I would beg to differ on the MRO function. Accessed from PHS Website 1/15/2015 http://www.massmed.org/Physician_Health_Services/About/PHS_Associate_Directors/#.VM1dZlXF-hY
Dr. Gavryck evidently did not do that here. In fact for more than a year he helped cover up an alcohol test that was intentionally fabricated at the behest of PHS Director of Operations Linda Bresnahan (who told me when I confronted her with the fact that I have never had or ever even been suspected of having an alcohol problem “you have an Irish last name–good luck finding anyone who will believe you!”
It took a formal complaint with the College of American Pathologists to get the truth out. The whole fiasco can be seen here and here.
What Gavryck and his co-conspirators did is egregious and ethically reprehensible. It shows a complete lack of moral compass and personal integrity. What was done from collection to report to coverup and everything in-between is indefensible on all levels (procedurally, ethically, and legally).
The documentary evidence shows with clarity that this was not accident or oversight. It was intentional and purposeful misconduct. I think everyone would agree that there should be zero-tolerance for forensic fraud in positions of power. Any person of honor and civility would agree.
Transparency, regulation, and accountability are necessary for these groups. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. I’ll erase my blog and vanish into the woodwork. But If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Sanchez and Bresnahan (much like Annie Dookhan) he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths.
Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
It is people just like this who are killing physicians across the country. The body count is vast and multiple. And those who are caught doing dirty deeds such as this need to be held accountable.
Please help me get this exposed, corrected, and rectified. The doctors of Massachusetts and the doctors of this entire country deserve better than this.

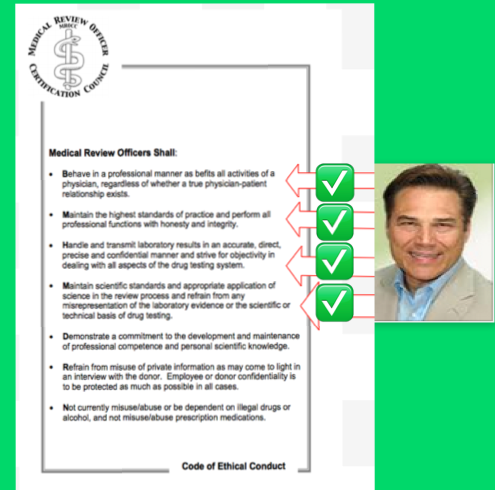
The MRO Code of Ethics–Seems like Dr. Gavryck’s breaking them in sequential order!


“The incompetent or unprincipled physician, licensed to practice medicine by a too complaisant State, is the greatest menace to scientific medicine – as great a menace as all the cultists put together.” —Dr. Morris Fishbein (The Medical Follies. New York: Boni Liverlight, 1925 p. 71)
“There is no place in science for consensus or opinion, only evidence” —Claude Bernard

Polio is nearly a thing of the past thanks to to Dr. Jonas Salk and Albert Sabin. In 1952 Salk discovered and developed the first successful vaccine for polio and combined with Albert Sabin’s 1961 oral vaccination the du0 effectively obliterated the contagious polio virus. Once a deadly threat to our country and future there were 93,000 cases of polio reported in the…
View original post 1,952 more words

A concise and understandable overview of the principles of Medical Ethics. As moral entrepreneurs the “impaired physician movement” and its offshoots have used the logical fallacy of appeal to authority to convince regulators, politicians and the general public to accept Consequential and Utilitarian ethics in their handling of those with or merely accused of having addictive disorders or substance abuse issues. And in doing so they routinely violate the Four Principles of Medical Ethics–Autonomy, Non-Maleficence, Beneficence and Justice. This needs to end.
The Symptoms of One Addicted to Medicine
So to start off my blog I thought I’d do a quick recap of the Basic Ethical ideas that underpin Medical Ethics and the Four principles of medical ethics.
There are three basic Medical Ethics ideas:
> Deontology
> Consequentialism /Utilitarianism
> Virtue ethics
Deontology:
Actions are right or wrong in themselves
One must balance rights and duties
One can only act on maxims which we can will as universal law without contradiction
Consequentialism/ Utilitarianism
Righteousness of an action is determined by the goodness of the consequences it brings
The end justifies the means
About maximising good
Virtue Ethics
Whether an action is right or wrong depends primarily on the virtues or vices shown in performing the action.
The Four Principles of Medical Ethics
1.Respect for Autonomy
Patients should be able to make informed and voluntary decisions giving an independence of decision
Basis of ‘informed consent’
2.Principle of…
View original post 136 more words


Saying the “like minded docs” are not ASAM is like saying the “tea party” is not part of the GOP.
Mission
- “Support the education of physicians and the public regarding the importance of psychosocial and spiritual interventions for the treatment of all persons with substance use disorders.
- Encourage the judicious use of Twelve Step recovery modalities for the treatment of substance use disorders.
- Encourage ABAM Fellowship training programs to require sufficient experience in the use of psychosocial, spiritual and Twelve Step interventions and to include test questions to discern a Fellows knowledge base regarding these aspects.
- Continue to provide presentations that support the philosophy of “Like Minded Docs” to ASAM, treatment providers, public, judicial and political arenas.
- Support the current ASAM Twelve Step Action Group.
- Support all activities that raise the consciousness regarding the importance of psychosocial and spiritual interventions.
- Promote further studies into the biological, social, psychological and spiritual aspects of recovery.
- Maintain the “high road” and not disparage alternative forms of treatment, but rather to promote those aspects…
View original post 145 more words

 “Because I can Biotches! That’s right..because I can!”
“Because I can Biotches! That’s right..because I can!”
View original post 1,470 more words


White House Drug Czar (1973-1977) Robert Dupont, M.D. (ASAM, FSPHP) and co-author Greg Skipper, M.D, (ASAM, FSPHP) describe the necessity for wider application of this new paradigm in an article published in the Journal of Psychoactive Drugs in 2012. In reviewing the “successes” of similar programs monitoring commercial pilots, attorneys, probationers, and those in the criminal justice system, they proclaim the “need to reach more of the 1.5 million Americans who annually enter substance abuse treatment, which now is all too often a revolving door.”1
Dupont and Skipper conclude:
This model of care management for substance use disorders has been pioneered by a small and innovative group of the nation’s physicians in their determination to help other physicians save their careers and families while also protecting their patients from the harmful consequences of continued substance abuse. In fulfilling the professional admonition “physician: first heal thyself,” these physicians have created a model with wide applicability and great promise.1
- Dupont RL, Skipper GE. Six lessons from state physician health programs to promote long-term recovery. Journal of psychoactive drugs. Jan-Mar 2012;44(1):72-78.



I. Evidence regarding the effectiveness of ASAM interventions.
II. Evidence regarding the ASAM patient placement criteria.
III. More about forced interventions (coercion into treatment).
“How To Achieve an 80 Percent Recovery Rate” —Stuart Gitlow, President of the @ASAMorg
How To Achieve an 80 Percent Recovery Rate
Published on October 16, 2012 by Stuart Gitlow, President of the American Society of Addiction Medicine (ASAM). Read the original post via the ASAM President’s BlogRecovery rates over 80% appear to be rather consistently identified both by PHPs and by studies of pilots conducted by the FAA and by independent airlines. These long term recovery rates appear dramatically superior to the recovery rates obtained within the general population, which, depending on what literature you believe, seems to lie somewhere in the 40-50% area. –Stuart Gitlow
No…
View original post 798 more words