…”PHPs are intentionally misdiagnosing substance abuse and behavioral disorders in physicians who do not have them in order to give them unneeded treatment and force them into monitoring contracts to both make money and gain control.
It undermines the very integrity of the profession. It is particularly vile when the betrayal of trust involves doing the opposite with what one was entrusted.“… — Michael Lawrence Langan.
Physician Suicide–What to do When Your Doctor Dies Suddenly by Pamela Wible, M.D.
Physician Suicide 101: Secrets, Lies & Solutions by Dr. Pamela Wible, M.D
Physician Suicide 101: Secrets, Lies & Solutions By Dr. Pamela Wible, M.D. will hopefully serve as a stepping-stone to start discussing Physician Health Programs (PHPs) and their relationship to physician suicide. (click on photo above to access article).
The current state-of-affairs is one of unrestrained managerial authority and absolute power with no meaningful oversight, regulation or accountability. Moreover, the authority bestowed on this group is both illegitimate and irrational. The Federation of State Physician Health Programs is composed of American Society of Addiction Medicine “specialists” in “Addiction Medicine.” The ASAM is not even recognized by the American Board of Medical Specialties as a bona fide specialty. It is a Self-Designated-Medical-Specialty; an AMA term used to keep track of what any group of doctors…
The Petition can be found here. Or better yet, sign the petition and call her at 617-727-6200. The evidence that Physician Health Services, Inc. (PHS) is committing crimes has been free-floating for the past two years. It has been posted on Reddit, Twitter, Facebook, Linkedin, blogged, faxed, and phoned. The response? Absolute silence.
The documentary evidence of crimes is self-evident. It is indefensible. It is inexcusable that criminal activity is taking place within the walls of the Massachusetts Medical Society. The fact that PHS is unregulated and without any meaningful accountability is irrelevant. They are engaging in criminal activity within the walls of an institution whose very foundation is the antithesis of this groups actions and it must be addressed. Either support what the documents show or do something about it.
So please sign this petition and call Massachusetts State Auditor Suzanne Bump at 617-727-6200
Institutional injustice just like that being committed by Luis Sanchez, Linda Bresnahan and the corrupt MRO Wayne Gavryck is killing doctors across the country. They need to be held accountable. Help me hold them accountable.
You do not need to be from Massachusetts to sign this petition. It is to raise public awareness–hopefully enough to elicit more exposure of this problem to prompt audits not only in Massachusetts but in other states as was recently done in North Carolina. The N.C. state auditor conducted an investigation and found poor oversight of the state PHP by both the state Medical Society and the state Medical Board, a lack of due process for physician’s who disputed the PHP’s evaluations and requirements, and multiple instances of potential conflicts-of-interest.
Dr. J. Wesley Boyd, who was previously an Associate Director at Physician Health Services, inc., the Massachusetts PHP is recommending that state government agencies audit their PHPs and his own state won’t even do it! This is despite clear evidence that the Massachusetts PHP, Physician Health Services, Inc. is engaging in forensic fraud, ethical misconduct, HIPAA violations and crimes that Deb Stoller of the Massachusetts Board of Registration in Medicine Physician Health and Compliance Unit has been aware of and is most likely complicit in. The Massachusetts State Auditor, Suzanne Bump, has refused to conduct an investigation. Why is this? I’d like to know why?
“After a group of North Carolina physicians complained about their state PHP to the state auditor, the auditor conducted an investigation (link is external)and found poor oversight of the PHP by both the state medical society and the board of medicine, a lack of due process for physicians who disputed the PHP’s evaluations and/or recommendations, and multiple instances of potential conflicts of interest.
The national federation of PHPs ought to implement national standards for its members and commence routine audits of its members. Other state governmental agencies ought to audit their PHPs as well, to ensure that their vast power is wielded judiciously and with oversight.”
The Massachusetts PHP is much worse. The Massachusetts PHP is engaging in unconscionable conduct including forensic fraud and self-evident criminal activity that is indefensible from within the walls of the Massachusetts Medical Society. Most are not aware of this. They need to be. This rigged game is a national problem and how the racket works in Massachusetts can be seen here.
The corruption is undeniable and the actions are indefensible, unethical and unconscionable. Please help me shine a light on these criminals. Corruption needs to be acknowledged and investigated. Ignoring it and hoping it might go away seldom works.
The Massachusetts Auditor should either be able to defend the actions of PHS and the BORM Physician Health and Compliance Unit or investigate. It is as simple as that.
I would like to begin this discussion with the 1st reason that made give me inspiration and additional courage to continue with this struggle and made understand that, no matter what happens, I have to continue with the discussion of this matter — Thank you Dr. Langan for giving me that additional inspiration — difficult to find the appropriate words to describe the type of ill-treatment, degradation, and humiliation that defines forced psychiatric treatment — especially when this is used to suppress dissenting ideas questioning the safety and effectiveness…
For as long as there have been people, there have been sources of guidance. Deities, prophets, leaders; all have persisted through time and have been highly influential on our world. We look to them for answers to our problems, for ways to improve our lives, and we try to model our own lives in their image or vision. For thousands of years, humans modeled themselves after a god, or many gods, and these all-powerful beings generally rewarded “good” behaviour and punished “bad” behaviour. Unexplainable phenomena were attributed to these beings’ anger or sadness, and joyous, miraculous events were attributed to their pleasure and exuberance in response to our following of their teachings.
Overall, people trusted in their worshiped deity to maintain a natural order to the world, and for thousands of years it seemed like things were going pretty well. Until modern science, putting your faith in whatever deity you…
To have striven, to have made an effort, to have been true to certain ideals — this alone is worth the struggle. We are here to add what we can to, not to get what we can from, life. – William Osler
Diagnostic Medicine
Diagnostic medicine is the process of identifying the condition or disease that a patient has and ruling out conditions or diseases the patient does not have through assessment of the patient’s signs, symptoms, and results of various diagnostic tests.
Diagnostic Test Accuracy
Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
If a test’s results do not differ between alternative states of health, then the test has insignificant accuracy; if the results do not overlap with other states of health then the test has perfect accuracy. Most tests accuracies fall between these two extremes.
The intrinsic accuracy of a test is measured by comparing the test results to the “true condition status.”
‘True condition status” refers to one of two mutually exclusive states. Either acondition is present or it is absent.
We determine true condition status by means of a “gold standard” which is a source of information completely different from the test under evaluation which tells us the true condition status of the patient.
Say we want to develop a new rapid test for detecting strep throat. Strep throat is caused by the Streptococcus bacteria. Although more common in children and adolescents it can occur in people of all ages. Strep throat is one of many possible causes of sore throat and pharyngitis. It is contagious and can cause complications such as rheumatic and scarlet fever. Treatment with antibiotics can shorten the course of the disease and reduce the risk of complications.
A throat culture is obtained by swabbing the patient’s throat with a cotton swab. The sample is then sent to the lab where it is cultured. If strep is present it will grow on the culture and look as below. The bacteria either grows on the culture or it doesn’t. A throat culture is the “gold standard” for diagnosing strep throat. The problem is it may take two days to get back.
Sensitivity and Specificity
The two most important measures of diagnostic test accuracy are sensitivityand specificity.
The probability that a test will be positive in someone with the condition = Sensitivity
The Probability that a test will be negative in someone without the condition = Specificity
For diagnosing strep throat we want our test to be as close as possible to the gold standard in terms of both sensitivity and specificity.
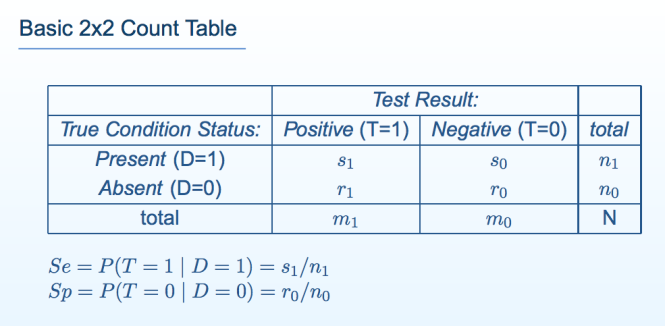
Sensitivity and specificity can be illustrated by a table with two rows and two columns. This simple Decision Matrixwhere the rows summarize the data according to the true condition status of the patients and the columns summarize the test results. This table is called a “count table” because it indicates the numbers of patients in various categories. The total number of patients with and without the condition is, respectively n\ and n0; the total number of patients with the condition who test positive and negative is respectively s\ and s0; and the total number of patients without the condition who test positive and negative is respectively r\ and ro.
The total number of patients in the study group N, is equal to N = si+so+rx+ro, or N = n\ + no·
The true condition status is symbolized by the variable D, where D = 1 if the condition is present and D= 0 if the condition is absent.
Test results indicating the condition is present are called positive; those indicating the condition is absent are called negative.
Test results are symbolized by the variable T, where T =1 denotes positive test results and T= 0 denotes negative test results.
The sensitivity (Se) of a test is its ability to detect the condition when it is present.
We write sensitivity as Se = P(T = 1 | D = 1), which is read:
“sensitivity (Se) is the probability (P) that the test result is positive (T = 1), given that the condition is present (D = 1).”
Among the n\ patients with the condition, s\ test positive; thus, Se = s\/n\.
The specificity (Sp) of a test is its ability to exclude the condition in patients without the condition.
We write specificity as Sp — P(T = 0 | D — 0), which is read:
“specificity (Sp) is the probability (P) that the test result is negative (T = 0), given that the condition is absent (D = 0).”
Among no patients without the condition, ro test negative; thus, Sp — TQ/UQ
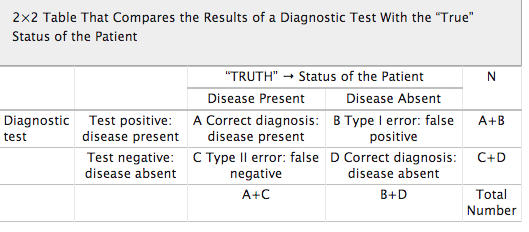
False Negative and False Positive Tests
There are consequences associated with all test results.
False Negative Tests: If a test falsely indicates the absence of a condition in someone who truly has it then treatment can be delayed or not provided.
The consequences of a false negative strep test depend on what we do with it. Serious consequences can arise if we use our new strep test as the sole basis for subsequent decision making. Putting complete trust in the negative test result would lead to no antibiotic treatment provided to a patient with Strep and can lead to continued illness, spread of the disease and complications that would not have occurred if antibiotics were provided. The patient could potentially get rheumatic or scarlet fever.
If the new test is negative but a culture was drawn the false results could delay treatment by a couple days or so but treatment is nevertheless provided. The consequences are likely to be minimal. It is highly unlikely a patient would get rheumatic or scarlet fever as, although a little later, they are still being treated with the proper antibiotics.
False Positive Tests: If a test falsely indicates the presence of a condition in someone who does not truly have it then unnecessary tests and treatments can occur. Incorrect treatment and false labeling of patients can also occur.
In the case of a false positive strep test, a patient may undergo a course of antibiotics when they do not need them. Although the patient may suffer side-effects from the antibiotics the severity and duration of any of these consequences are minimal.
The importance of a Diagnostic Accuracy in testing is directly proportional to the tests potential to cause patient consequences and harm.
Diagnostic Medicine uses a patient’s signs, symptoms and the results of various diagnostic tests to arrive at a diagnosis.
In diagnosing strep throat a good clinician will take into account a number of variables in consideration of a differential diagnosis and base testing and treatment on the preponderance of information supporting or opposing the diagnosis.
For strep throat using the new test in addition to a throat culture, history and careful physical exam and basing the decision to prescribe antibiotics on clinical acumen based on the overall picture is the best approach. The test can be considered a piece of the puzzle but does not define it. Therefore the risk of a false positive or false negative is minimal as it is just one data point.
Diagnostic accuracy is necessary if a test is being used as the basis for further tests and treatment. If a test is being used as the sole basis for further tests and treatment it needs to be accurate. If the results of a test can cause significant patient harm or death then it needs to be either 100% accurate or combined with other highly accurate tests to confirm the diagnosis.
The specificity of a test is particularly important as a false positive can result in unneeded interventions and treatment. Stand-alone tests used in diagnosis and treatment need to be both sensitive and specific. Diagnostic accuracy is a product of consequences of false-negative and false positive tests.
Diagnostic Research Methodology
Research to discover the accuracy of a diagnostic test should be straightforward; administer the test to a group of people and see if it works.
The test being tested is the “index test”. Results of the index test are compared with the results of a “gold standard” reference test.
The research question is, “How accurately do index test results predict the (true, gold standard) reference test results?”
Diagnostic test accuracy studies require a sample of subjects who have been given the test under evaluation, some form of scoring of the tests findings and a reference or “gold standard” to which the test findings are compared. Examples include autopsy reports, surgery findings and pathology results from biopsy findings.
The gold standard for a patient’s true disease status may not always be available. A brain biopsy could be considered a gold standard for diagnosing Alzheimer’s disease but is neither practical nor humane.
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool is a set of fourteen questions that investigate the methodologic quality of scientific studies that quantify diagnostic test performance.
The questions identify research methodologies known to bias the accuracies research discovers.
Multiple factors need to be considered in evaluating the diagnostic accuracy of a test including diagnostic validation and verification. Is the test testing what it is supposed to be testing for and are we doing it correctly?
Diagnostic accuracy of a test necessitates a reference standard, The reference standard can be the best available method for establishing the presence or absence of a condition (such as the throat culture for strep throat) or a combination of methods (imaging, neuropsychological testing, clinical exam, etc. in Alzheimer’s disease.
Any test that is going to be used as a basis for decisions that impact other human beings needs to be validated before it is introduced on the market. The literature needs to be reviewed critically and trials must be designed using objective evidence that validates the test is testing for what it purports to be and verifies the correct methodology of the test. Verification that the test is being collected, handled, stored, transported and processed correctly is requisite.
Cutoff levels, , cross-reactivity and myriad other issues need to be worked out prior to bringing a diagnostic test to market.
The reliability, validity and accuracy of drug test results needs to be known prior to using a test. Specificity and sensitivity must be known prior to using a test on any population.
This should go without saying as to do anything else would be irresponsible and careless.
References
Evidence-based medicine, systematic reviews, and guidelines in interventional pain management: part 7: systematic reviews and meta-analyses of diagnostic accuracy studies Pain Physician 2009, 12(6):929-963. PubMed Abstract | Publisher Full Text
Jaeschke R, Guyatt G, Lijmer J: Diagnostic tests. In Users’ guides to the medical literature: a manual for evidence-based clinical practice. Edited by Guyatt G, Rennie D. AMA Press; 2002:121-140.
Streiner DL: Diagnosing tests: using and misusing diagnostic and screening tests.J Pers Assess 2003, 81(3):209-219. PubMed Abstract | Publisher Full Text
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J: The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003., 3(25) http://www.biomedcentral.com/1471-2288/3/25webcite
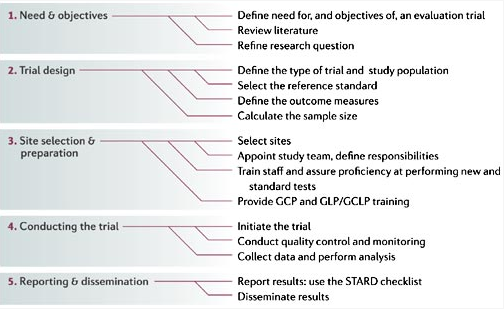
GCP, good clinical practice; GCLP, good clinical laboratory practice; GLP, good laboratory practice; STARD, standards for reporting of diagnostic accuracy. See Section III, 2.13 From Nature Reviews Microbiology 4, S20–S32 (1 December 2006) | doi:10.1038/nrmicro1570
There seems to be a willful ignorance or apathy among the medical profession at large regarding Physician Health Programs (PHPs). Perhaps most take the side of the PHPs complacent in the belief that these groups are just helping sick doctors and protecting the public. The mere accusation of substance abuse or “disruptive” behavior is in-and-of- itself used to disregard the claims of the accused. Any and all complaints of malpractice, misconduct and even crimes are deflected, turfed or dismissed–rendered as nothing more than “bellyaching.”
In reality the misconduct and abuse perpetrated by the PHPs is commensurate with the behavior of Dr. Farid Fata, the Detroit Oncologist who intentionally misdiagnosed patients with cancer so he could make money off unnecessary chemotherapy treatment. Dr. Fata’s egregious betrayal of trust and unconscionable acts generated a flurry of comments. His vile acts resulted in an appropriate response.
The exact same misconduct is being perpetrated by PHPs but being overlooked, justified or otherwise ignored. Dr. Fata intentionally misdiagnosed patients with cancer who did not have cancer so he could give them chemotherapy to make money. PHPs are intentionally misdiagnosing substance abuse and behavioral disorders in physicians who do not have them in order to give them unneeded treatment and force them into monitoring contracts to both make money and gain control.
It undermines the very integrity of the profession. It is particularly vile when the betrayal of trust involves doing the opposite with what one was entrusted. Abuse of positions of power, trust and influence in the field of medicine need to be both prevented, recognized and addressed. Oversight, regulation and accountability are essential if this is going to be accomplished. There are no exceptions. Policies and procedures must be enforced in a consistent manner.
As the Medical Review Officer (MRO) for the Massachusetts state Physician Health Program (PHP), Physician Health Services, Inc. (PHS, inc.), Dr. Wayne Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody in any and all drug and alcohol testing is intact before reporting a test as positive.
Dr. Gavryck evidently did not do that here. In fact for more than a year he helped cover up an alcohol test that was intentionally fabricated at the behest of PHS Medical Director Dr. Luis Sanchez, M.D. and Director of Operations Linda Bresnahan (who told me when I confronted her with the fact that I have never had or ever even been suspected of having an alcohol problem “you have an Irish last name–good luck finding anyone who will believe you!”)
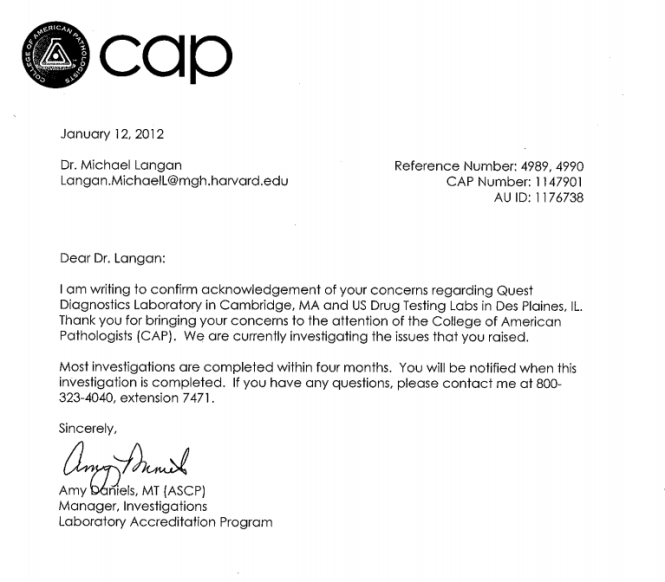
It took a formal complaint with the College of American Pathologists to get the truth out. The whole fiasco can be seen here and here.
What Gavryck and his co-conspirators did is egregious and ethically reprehensible. It shows a complete lack of moral compass and personal integrity. What was done from collection to report to coverup and everything in-between is indefensible on all levels (procedurally, ethically, and legally).
The documentary evidence shows with clarity that this was not accident or oversight. It was intentional and purposeful misconduct. I think everyone would agree that there should be zero-tolerance for forensic fraud in positions of power. Any person of honor and civility would agree.
Transparency, regulation, and accountability are necessary for these groups. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. I’ll erase my blog and vanish into the woodwork. But If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Sanchez and Bresnahan (much like Annie Dookhan) he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths.
Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
It is people just like this who are killing physicians across the country. The body count is vast and multiple. And those who are caught doing dirty deeds such as this need to be held accountable.
Please help me get this exposed, corrected, and rectified. The doctors of Massachusetts and the doctors of this entire country deserve better than this.
Details of how the state PHP scam operates can be seen below as pertains to my case. Occurring in most states under the FSPHP ( although some are worse than others) the Method of Operation (M.O) is the same.
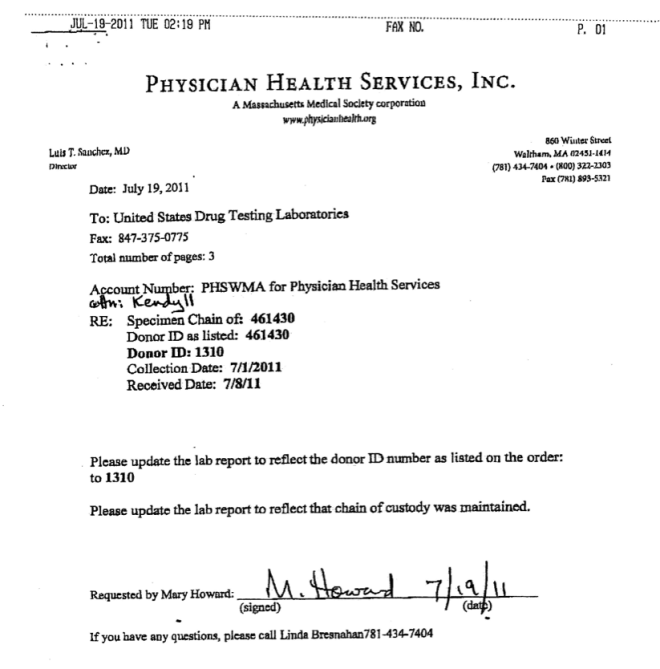
I. July 28th, 2011. Reporting a Positive Test
This letter from Physician Health Services, Inc. Medical Director (and past President of FSPHP) Dr. Luis Sanchez, M.D. to the Massachusetts Medical Board reports a markedly high level for Phosphatidylethanol (PEth), an alcohol biomarker test being used by Physician Health Programs to detect alcohol use.
The cutoff for heavy drinking is anything greater than 20 ng/mL. Mine came back at a level of 365.4 ng/ml! This level is suggestive of end-stage alcoholism and putting away a half-gallon a day of the hard stuff. It is, in fact, reportedly the second highest level in history and the other guy was dead on arrival.
After reporting the blood test as dirty, Sanchez then requests a “reevaluation.”
II. Requested Evaluation Limited to “Like-Minded Docs”
I was given three choices for this re-evaluation as listed above. The Medical Directors can all be found on this list of “Like-Minded Docs” Their philosophy of 12-step “intervention” can be seen here.
This referral to “like-minds” is part of the state Physician Health Program scam. It is essentially self-referral as the choices are limited to “PHP-approved” assessment and treatment centers. For doctors (and now pilots) an objective and independent referral is out of the question. It is, in fact, a rigged system.
Dr. Greg Skipper, the physician who proposed and promoted the use of EtG, EtS, PEth and other non FDA approved “Laboratory Developed Tests (LDTs) for forensic testing is also on the list.
Former White House Drug Czar Dr. Robert Dupont who is claiming Physician Health Programs (PHPs) are the “new paradigm” for substance abuse treatment is also on the list. Dupont wants to use the PHP model (including the non-FDA approved drug and alcohol tests they introduced) for other Employee Assistance Programs (EAPs) and populations (including kids and students.).
III. November 29, 2011. PHS Agrees to my Request for “Litigation Packet”
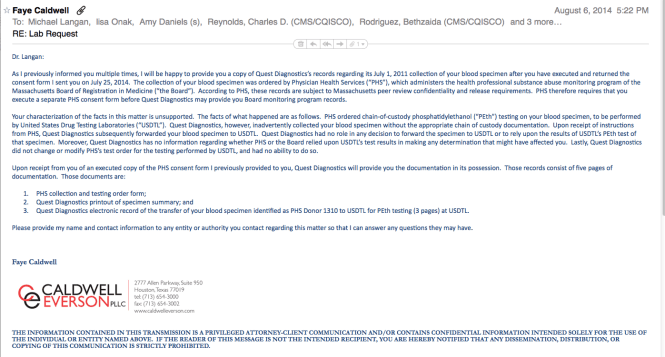
Any and all forensic drug and alcohol testing requires strict chain-of-custody. Documentation of chain-of-custody is necessary to protects both those ordering and doing the testing and the person being tested. Forensic laboratories provide documentation of chain-of-custody in a document called a “litigation packet.”
On November 29, 2011 PHS agreed to my request.
IV. Discovering Procedural Misconduct and Forensic Fraud
The screenshot above is an ID card used for random drug and alcohol testing. It is a card issued by Physician Health Services, Inc. and contains my picture, my initials and an ID # 1310. The number #1310 is a unique identifier like a social security number or medical record number. It is used to document “chain-of-custody” for testing and identifies who I am for laboratory testing.
The document below is a fax from Physician Health Services, Inc.
The document is signed by Mary Howard , whose job description is as below:
“If you have any questions” the document sates, “please call Linda Bresnahan 781-434-7404.” Ms. Howard assists Ms. Bresnahan in the drug and alcohol testing of doctors monitored by PHS.
Don’t expect a “whodunnit” version of CSI victories in this Op-ed blog article about a darker side of the forensic sciences. It is from an author with ample forensic credentials and experience from both within and outside criminal courts of the US. The article has topics ranging from the continued use of outdated or grossly over hyped “CSI” methods, ethical and moral failures in some forensic groups, to the criminal courts inability to understand much of anything about what is “real ” versus self-serving personal opinion called “science.” A measure of proof confirming these systemic problems is the article’s presenting a glimpse into the multi-million dollar costs to taxpayers for damages won by those wrongfully convicted with the help of court-qualified forensic testimony. Some optimism about better scientific scrutiny is presented but the institutional inertia resisting legitimate change in some forensic organizations, government agencies, and criminal justice institutions is still…





















 The Plan to… Require Doctors to Drug-Test all Patients
The Plan to… Require Doctors to Drug-Test all Patients