Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Although he specifies the numerical percentage “in physicians at 7.9%,”3 he avoids the use of numbers (14.6%) in the general population. He instead uses the qualifier “somewhat less.” Why is this?
My guess is because it understates the statistical fact that the prevalence found by Kessler in the general population was almost twice that found by Hughes in physicians.
You see, “Somewhat less” is a “detensifier.” It creates an impression of a small disparity between doctors and the general population.
In propaganda this is what is known as a “weasel phrase.” Weasel phrases are used to obfuscate the truth. Weasel phrases mislead those either without the time, or without the sense to see or look any deeper. The problem is it works.
“Methodologic differences may account for this difference,” Earley states, as the Hughes study “surveyed 9, 600 physicians by mail” and “relied on honest and denial-free reports by the physicians; the Kessler study utilized face-to-face interviews with trained interviewers.”1
This is an example of language framing. Language framing uses words and phrases to direct attention to a point of view to advance a vested interest.
In this case the use of the phrase “honest and denial free” in the context of physician reporting imparts associative meaning to the reader.
As denial is a recurring motif and cardinal attribute of physician addiction according to the paradigm, the connotation is that the reports by physicians may have been influenced by dishonesty and denial while face-to-face interviews done by “trained” interviewers were not.
“Framing” is another propaganda technique designed to tell the audience how to interpret the information given through context. The message here is that the somewhat less lifetime prevalence of substance abuse and addiction in physicians found by anonymous mail survey may be underreported as a result of both methodology and denial.
But in actual fact there is a large body of research regarding “social desirability bias” that shows the converse to be true.
One of the most consistent findings of studies of this kind is that socially desirable responding is significantly more likely with face-to-face administered data collection compared with self-administered anonymous modes.4-6
Tourangeau et al. reviewed seven studies comparing self-reports of drug use in surveys conducted in different modes. For each estimate obtained in the studies they calculated the ratio of drug use reported in self-reported surveys to the corresponding estimates in interviewer administered surveys and found that 57 of 63 different comparisons showed higher levels of reporting of drug use in the self-reported mode.7
The principal cause of social desirability bias is the level of perceived anonymity of the reporting situation.7
Evidence-based research does not support Earley’s claim that methodological differences in study design explain the difference in reported lifetime prevalence of substance abuse or addiction between physicians and the general population in these two studies.
Evidence based research would, in fact, make the findings more robust.
Moreover, I find it hard to comprehend the psychodynamics, motivation, and logic of denial and dishonesty in influencing an anonymous survey. So too would anyone else who dare peer beneath the veil. It is, in fact, a Potemkin village. In reality the emperor has no clothes.
Earley PE. Physician Health Programs and Addiction among Physicians. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed. Baltimore: Lippincott Williams & Wilkens; 2009:531-547.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Sudman S, Bradburn NM. Response effects in surveys: A review and synthesis. Chicago: Aldine Publishing; 1974.
Tourangeau R, Smith TW. Collecting sensitive information with different modes of data collection. In: Couper MP, Baker RP, Bethlehem J, et al., eds. Computer assisted survey information collection. New York: John Wiley & Sons, Inc.; 1998.
Dillman DA. Mail and telephone surveys: The total design method. New York: Wiley-Interscience; 1978.
Tourangeau R, Rips LJ, Rasinski KA. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000.
American Society of Addiction Medicine: Patient Placement Criteria. Chevy Chase, MD: American Society of Addiction Medicine; 2000.
Merlo LJ, Gold MS. Successful Treatment of Physicians With Addictions: Addiction Impairs More Physicians Than Any Other Disease. Psychiatric Times. 2009;26(9):1-8.
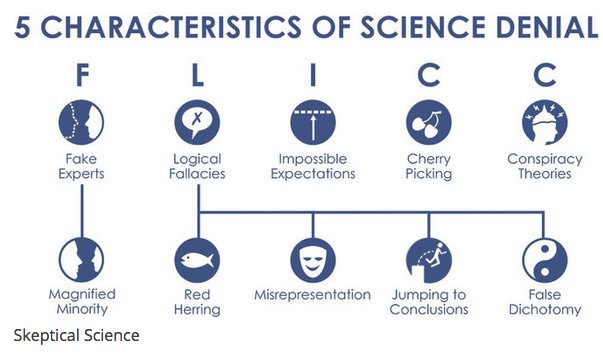
Science denial has real, societal consequences. Denial of the link between HIV and AIDS led to more than 330,000 premature deaths in South Africa. Denial of the link between smoking and cancer has caused millions of premature deaths. Thanks to vaccination denial, preventable diseases are making a comeback.
Denial is not something we can ignore or, well, deny. So what does scientific research say is the most effective response? Common wisdom says that communicating more science should be the solution. But a growing body of evidence indicates that this approach can actually backfire, reinforcing people’s prior beliefs.
When you present evidence that threatens a person’s worldview, it can actually strengthen their beliefs. This is called the “worldview backfire effect”. One of the first scientific experiments that observed this effect dates back to 1975.
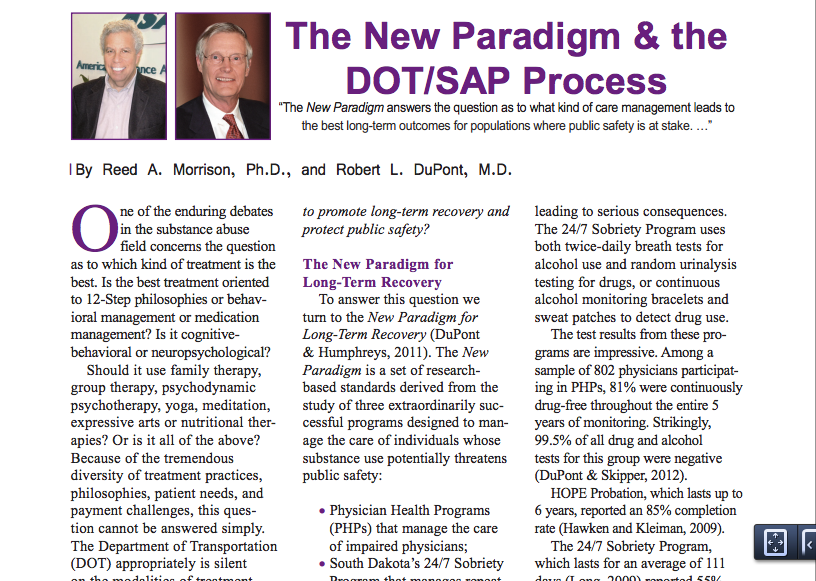
In 2012 former Nixon Drug Czar Robert Dupont, MD delivered the keynote speech at the Drug and Alcohol Testing Industry Association (DATIA) annual conference and described a “new paradigm” for addiction and substance abuse treatment. He advocated zero tolerance for alcohol and drug use enforced by monitoring with frequent random drug and alcohol tests. Detection of any substances is met with “swift and certain consequences.”
And then he proposed expansion of this paradigm to other populations including workplace, healthcare, and schools.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.” The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical Society updated its mission to read:
“The purposes of the Massachusetts Medical Society shall be to do all things as may be necessary and appropriate to advance medical knowledge, to develop and maintain the highest professional and ethical standards of medical practice and health care, and to promote medical institutions formed on liberal principles for the health, benefit and welfare of citizens of the commonwealth.”
With a foundation and history built and based on of scholarship and critical thought we need to support the highest levels of science, fact, intelligence and reason. Stupidity tries but it should not rein. Before the Boston Society for the Diffusion of Useful Knowledge in 1842, Dr. Oliver Wendell Holmes delivered two long lectures entitled “Homeopathy and Its Kindred Delusions.” He characterized one of its popular practitioners, Dr. Robert Wesselhoeft, as one of those:
“Emperics [quacks], ignorant barbers, and men of that sort…who announce themselves ready to relinquish all the accumulated treasure of our art, to trifle with life upon the strength of these fantastic theories.” That “pretended science” as Holmes called it, was “a mingled mass of perverse ingenuity, of tinsel erudition, of imbecile credulity, and artful misrepresentation, too often mingled in practice…with heartless and shameless imposition.”
And Holmes words are as apt and appropriate today as they were in mid 19th Century Boston! Probably more so.
History has recurrently proved that false constructs and groundless concepts allow for endless error.
The Massachusetts Medical Society needs to come to the realization that Physician Health Services is engaging in procedural, ethical and legal breaches. The evidence is clear that past medical director Dr. Luis Sanchez and Director of operations Linda Bresnahan are engaging in not only unethical but criminal activity within the walls of the MMS. Egregious misconduct including forensic fraud and political abuse of psychiatry can be seen in detail here, here and here.This is not a matter of opinion but a matter of fact. It has been ascertained by outside agencies and can also be confirmed by two former associate directors at PHS. What more does the MMS need? This type of misconduct can have grave and far reaching consequences for referred doctors and needs to be addressed urgently with precise, firm methods. To ignore the problem or suggest that it does not exist will only cause more damage.The majority of Massachusetts Medical Society members are honest, thoughtful and responsible. Most are unaware of the ethical and criminal allegations concerning PHS.. It is time they become aware as sunshine is the best disinfectant. As the most crucial step in solving a problem is admitting it exists I am requesting this be ascertained or refuted based on the documents and examined procedurally, ethically and legally. If there is no problem then the MMS should have no problem supporting or justifying the actions of Dr. Luis Sanchez, Dr. Wayne Gavryck and Linda Bresnahan. If the MMS cannot justify, support or defend these actions then it must be concluded that these individuals have violated professional protocol,, professional and community ethics and the law. And if that is the case it is the responsibility of the MMS to admit the problem exists, define it and address it. It is the responsibility of the MMS to facilitate exposure and that those engaged in wrongdoing be held appropriately accountable for their actions. I am sure no one at the MMS would disagree that forensic fraud be met with Zero-tolerance. The criminal and ethical violations shown here do not comport with any codes of conduct including those of the medical society. Those engaging in forensic fraud must be removed.
Good leadership requires correct moral and ethical behavior of both the individual and the organization. . Integrity is necessary for establishing relationships of trust. It requires a true heart and an honest soul. People of integrity instinctively do the “right thing” in any and all circumstances. Adherence to ethical codes of the profession is a universal obligation. It excludes all exceptions. Without ethical integrity, falsity will flourish.
The documentary evidence here shows fraud. It is intentional. All parties involved knew what they were doing, knew it was wrong but did it anyway. The schism between pious rhetoric and reality is wide.
One measure of integrity is truthfulness to words and deeds. These people claim professionalism, ethics and integrity. The documents show a reality of hypocrisy and sanctimony. But the hypocrisy seen here is also a danger because the careers and lives of doctors in Massachusetts are in these peoples hands.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.”The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical…
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers, and consumers of health care products, and the general public.”
In this they have succeeded.
And in the year 2014 Stimson’s characterization of the “impaired physician movement” remains as accurate and apt as it was in 1985. But the “number of evangelical recovered alcoholic and addict physicians” has increased dramatically (outnumbering Addiction Psychiatry by 4:1) and their involvement in “ medical society and treatment programs” has been realized and enforced through the state Physician Health Programs and their “PHP-approved’ assessment and treatment centers.
Their“ability to make authoritative pronouncements on physician impairment…based on their own claim to insider’s knowledge”has become public policy and sanctified by Regulatory Medicine.
And the 1953 Alcoholics Anonymous prophecy that “With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world” is also coming to pass.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to doctors and how they might be involved in the descent from suicidal ideation to suicidal planning to completed suicide.
Depression and Substance Abuse Comparable to General Population
Depression and substance abuse are the two biggest risk factors for suicide. The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria suggest that physicians have the same rates (8-14%) of substance abuse and dependence as the rest of the population 3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 found a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
State Physician Health Programs
Perhaps it is how physicians are treated differently when they develop a substance abuse or mental health problem.
Physician Health Programs (PHP) can be considered an equivalent to Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Originally developed as “impaired physician” programs, the PHPs were created to help doctors who developed problems with substance abuse or addiction an alternative to disciplinary action by State Medical Boards. These programs existed in almost every state by 1980. Often staffed by volunteer physicians and funded State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referrals. Most EAPs were developed with the collaboration of workers unions or some other group supporting the rights and interests of the workers. As there is no such organization representing doctors, PHPs developed in the absence of regulation or oversight. As a consequence there is no meaningful accountability.
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”8
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “that the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 8 They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”8 Unfortunately this has not happened. Most physicians have no idea that the state physician health programs have been taken over by the “impaired physicians movement.”
In his Psychology Todayblog, Boyd again recommends oversight and regulation of PHPs. He cites the North Carolina Physicians Health Program Audit released in April of 2014 that reported the below key findings:
As with Knight and Boyd’s paper outlining the ethical and managerial problems in PHPs, the NC PHP audit finding that abuse could occur and not be detected generated little interest from either the medical community or the media.
Although state PHPs present themselves as confidential caring programs of benevolence they are essentially monitoring programs for physicians who can be referred to them for issues such as being behind on chart notes. If the PHP feels a doctor is in need of PHP “services” they must then abide by any and all demands of the PHP or be reported to their medical board under threat of loss of licensure.
LDTs bypass the FDA approval process and have no meaningful regulatory oversight. The LDT pathway was not designed for “forensic” tests but clinical tests with low risk. Some are arguing for regulation and oversight of LDTs due to questionable validity and risk of patient harm.13
These same physicians are claiming a high success rate for PH programs9 and suggesting that they be used for random testing of all physicians.14
As with LDTs, the state PHPs are unregulated, and without oversight. State medical societies and departments of health have no control over state PHPs.
Their opacity is bolstered by peer-review immunity, HIPPA, HCQIA, and confidentiality agreements. The monitored physician is forced to abide by any and all demands of the PHP no matter how unreasonable-all under the coloration of medical utility and without any evidentiary standard or right to appeal.
The ASAM has a certification process for physicians and claim to be “addiction” specialists. This “board certification” is not recognized by the American Board of Medical Specialties and is not a recognized medical specialty. The goal of the ASAM is to be recognized as the experts in addiction medicine with the consensus expert opinion based on the 12-step prohibitionist brain disease model. The ASAM has aligned itself with a number of inpatient drug treatment centers (Hazelden, Talbott, Marworth, Bradford,etc) and are heavily funded by the drug testing industry. It is in fact a “rigged game.”
State PHPs are non-profit non-governmental organizations and have been granted quasi-governmental immunity by most State legislatures from legal liability.
By infiltrating “impaired physician” programs they have established themselves in almost every state by joining, gaining power, and removing dissenters. Groupthink and 12-step indoctrination are the goals. By advertising as advocates for doctors who are “caring,” “confidential resources,” “giving help,” and advocating for “colleagues in need” the outward appearance is one of benevolence.
The biggest obstacle is that this system allows them to throw the normal rules of conduct under the imperative of a higher goal assumed to trump all other consideration. Those outside of programs either defend or ignore the reports of ethical and criminal violations, complacent in their trust of these “experts” claiming they are just helping sick doctors and protecting the public.
With no oversight or regulatory body involved this is all done with impunity, immunity, and undercover. They use the accusation of substance abuse as an indication to disregard the claims of the accused. The physician is left without rights, depersonalized, and dehumanized. The imposition of confinement, stigmatization, lack of oversight of the organizations, peer-review protected confidentiality, and lack of procedural protection is a one-way train to hopelessness and despair.
By establishing a system that of coercion, control, secrecy, and misinformation, the FSPHP is claiming an “80% success rate” 15and deeming the “PHP-blueprint” as “the new paradigm in addiction medicine treatment.
The ASAM/FSPHP had a major influence on the DSM-V where drug abuse and dependence are no longer separate entities. They are also working behind the scenes to get legislation to randomly drug test all physicians.
They are now after the “disruptive physician” and the evidentiary criteria are fairly low and red flags include “deviating from workplace norm in dress or conduct” and being tardy for meetings.
They have identified “the aging physician” as a potential problem because “as the population of physicians ages,””cognitive functioning” becomes “a more common threat to the quality of medical care.”
The majority of physicians are unaware that the Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment in 2011 that uses addiction as an example of a “potentially impairing illness.” According to the Federation of State Physician Health Programs …”physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years. This is a critically important distinction. Illness is the existence of a disease. Impairment is a functional classification and implies the inability of the person affected by disease to perform specific activities.”
“Process addiction” was added as a potentially impairing illness including compulsive gambling, compulsive spending, compulsive video gaming, and “workaholism.” According to the FSPHP “the presence of a process addiction can be problematic or even impairing in itself, and it can contribute to relapse of a physician in recovery. As such, process addictions should be identified and treated.” They define three levels of relapse including the novel “relapse without use.”
Bullying, Helplessness, Hopelessness and Despair
Perceived helplessness is significantly associated with suicide.16 So too is hopelessness, and the feeling that no matter what you do there is simply no way out17,18 Bullying is known to be a predominant trigger for adolescent suicide19-21 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.22
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.23,24 The “Cry of Pain” model 25,26 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life.
There is also evidence that rescue factors such as social supports may play a role in preventing suicide. These rescue factors act buffers to protect against suicide in the face of varying degrees of life stress.27,28 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 29 and support at work when difficulties arose appeared to be a protective factor for the male physicians.30 Research involving Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.31,32 Organizational justice is related to fairness and refers to an individuals perception of an organizations behaviors, decisions, and actions and how these influence one’s own attitudes and behaviors and has been identified as a psychosocial predictor of health and wellbeing3334 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.35,36
A recent report indicates that job stress, coupled with inadequate treatment for mental illness may play a role in physician suicide..
Using data from the National Violent Death Reporting System the investigators compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.1
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians.
They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity.
We have heard of numerous suicides due to these institutionally unjust programs. Three doctors died by suicide in Oklahoma in a one month period alone (August 2014). All three were being monitored by the Oklahoma PHP. I went to an all boys high-school of less than 350 students yet a classmate a couple years ahead of me died by suicide a few months ago. He was being monitored by the Washington PHP. His crime? A DUI in 2009–a one-off situational mistake that in all likelihood would never have recurred. But as is often the case with those ensnared by state PHPs he was forced to have a “re-assessment” as his five-year monitoring contract was coming to an end. These re-assessments are often precipitated by a positive Laboratory Developed Test (LDT) and state medical boards mandate these assessments can only be done at an out-of-state “PHP-approved” facility. Told he could no longer operate and was unsafe to practice medicine by the PHP and assessment center he then hanged himself. And at the conclusion of Dr. Pamela Wible’s haunting video below are listed just the known suicides of doctors; many were being monitored by their state PHPs–including the first name on the list– Dr. Gregory Miday.
None of these deaths were investigated. None were covered in the mainstream media. These are red flags that need to be acknowledged and addressed! This anecdotal evidence suggests the oft-used estimate of 400 suicides per year (an entire medical school class) is a vast underestimation of reality—extrapolating just the five deaths above to the entire population of US doctors suggests we are losing at least an entire medical school per year.
As physicians we need to demand transparency, oversight, regulation and auditing by outside groups. This is a public health emergency.
To wit:
They first came after the substance abusers and I did not speak out because I was not a substance abuser.
They then came for those with psychiatric diagnoses and I did not speak out because I was not diagnosed with a psychiatric disorder.
They then came after the “disruptive physician” and I did not speak out because I was not disruptive.
They then came after the aging physician and I did not speak out because I was young.
They then came after me and there was no one else to speak out for me.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ Health Programs. Journal of Medical Regulation. Mar 2010;95(4):10-25.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol and alcoholism. Sep-Oct 2004;39(5):445-449.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results. Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study. European addiction research. 2014;20(3):137-142.
Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
Pham JC, Pronovost PJ, Skipper GE. Identification of physician impairment. JAMA : the journal of the American Medical Association. May 22 2013;309(20):2101-2102.
McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. Bmj. 2008;337:a2038.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis. 2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors. Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.
The ASAM plans to introduce non-FDA approved “forensic” Laboratory Developed Tests (LDTs) into mainstream healthcare via a loophole. This same group introduced most of these tests through a loophole and now they want to drug-and alcohol TEST EVERYBODY including STUDENTS AND KIDS through another loophole! These tests are of unknown reliability and accuracy. The LDT pathway does not even require proof that the test is even valid (i.e. that the test is actually testing for the substance it claims to be testing) but with no FDA oversight or regulation the labs can claim anything they want in marketing it and they do.
If a doctor collects a test on a “patient” the test is rendered “clinical” rather than “forensic” and by deeming this drug-testing “clinical” rather than “forensic” they can then call the consequences of a positive test “treatment” rather than “punishment. ” It is via this loophole they plan to introduce and unleash the panoply of junk-science tests currently being used on other groups who have no say in the matter (probationers, parolees, private professional monitoring groups, etc. ) onto the general population at large. A boon for the Drug and Alcohol Testing Industry Association and the assessment and treatment industry but a bane to the rest of society. And to prevent this from happening more people need to be talking about this.
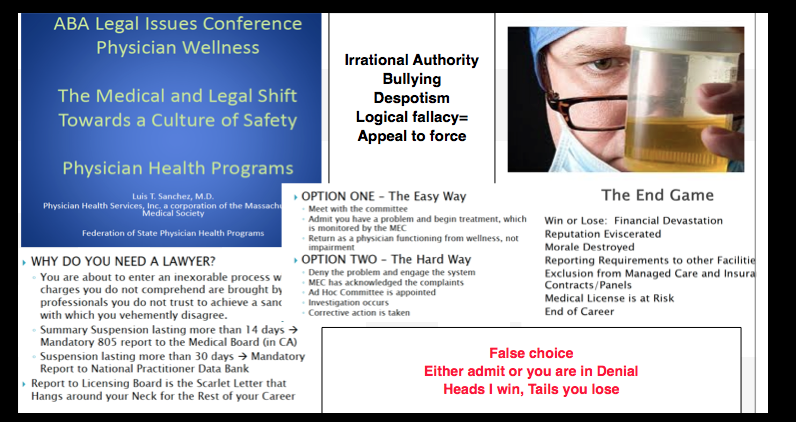
The blue slides below are from a presentation at the 2014 FSPHP spring meeting in Denver, Colorado and can be seen here. The presentation was given by past FSPHP President Gary Carr, MD, Current FSPHP President Warren Prendergast, MD, West Virginia PHP Director Brad Hall, MD and Montana PHP Director Mike Ramirez, MS.
This needs to be seen as a “to-do” list.
A.A. = ASAM = FSPHP
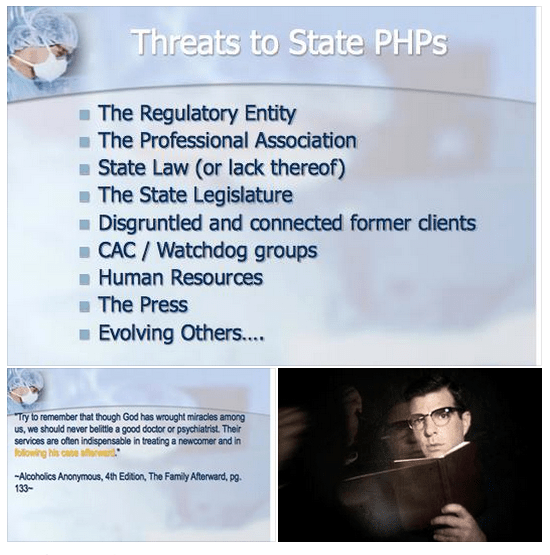
The quote is from Alcoholics Anonymous and the full passage is as follows:
“We are convinced that a spiritual mode of living is a most powerful health restorative. We, who have recovered from serious drinking, are miracles of mental health. But we have seen remarkable transformations in our bodies. Hardly one of our crowd now shows any mark of dissipation. But this does not mean that we disregard human health measures. God has abundantly supplied this world with fine doctors, psychologists, and practitioners of various kinds. Do not hesitate to take your health problems to such persons. Most of them give freely of themselves, that their fellows may enjoy sound minds and bodies. Try to remember that though God has wrought miracles among us, we should never belittle a good doctor or psychiatrist. Their services are often indispensable in treating a newcomer and in following his case afterward.”–Alcoholics Anonymous, 4th Edition, The Family Afterward
Federation of State Physician Health Program (FSPHP) physicians often quote A.A. because they are defined by A.A. in both mechanics and mentality. The “impaired physician” movement began with evangelical recovered addict and alcoholic physicians whose recovery was based on 12- step spirituality. As this group molded into the American Society of Addiction Medicine (ASAM) many of them found employment at 12-step rehabilitation facilities and others joined their state Physician Health Programs and organized under the FSPHP. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insiders knowledge of recovery as brandished in this A.A. passage which I find condescending toward the medical profession and oddly narcissistic.
This special knowledge, of course, was based on the chronic relapsing brain disease model with lifelong abstinence and participation in 12-step recovery.
These “miracles of mental health” joined their state PHPs and those who did not agree with their rigid inflexible views were removed. Those with access to special secret knowledge were eventually able to outvote those with intelligence and open minds as this groupthink infested and eventually monopolized PHPs.
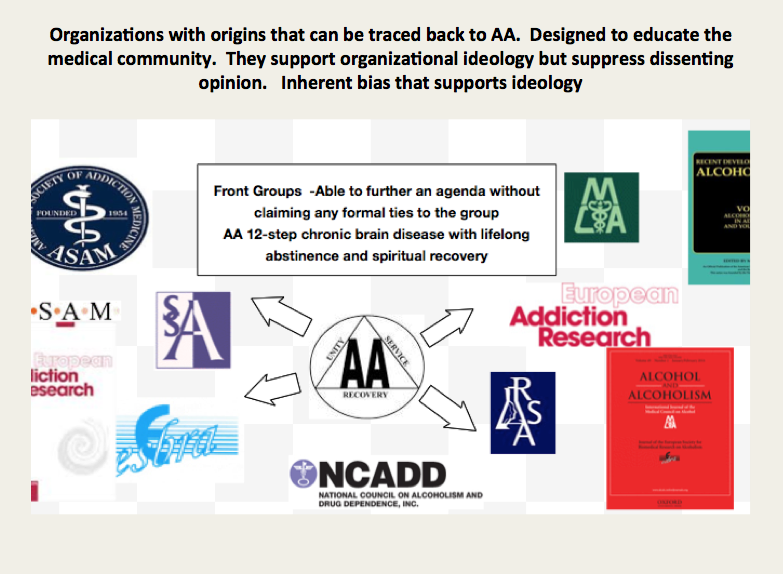
It is important to understand that the ideology of A.A. is the ideology of the ASAM is the ideology of the FSPHP
Like all “front-groups” the ASAM purports to serve one agenda while in reality serving another. The ASAM claims to be a “physician society with a focus on addiction and its treatment” According to their website their mission is to
increase access to and improve the quality of addiction treatment;
to educate physicians (including medical and osteopathic students), other health care providers and the public;
to support research and prevention;
to promote the appropriate role of the physician in the care of patients with addiction;
and to establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers and consumers of health care services, and the general public
In order to accomplish this the American Board of Addiction Medicine certifies doctors to “provide assurance to the American public that Addiction Medicine physicians have the knowledge and skills to prevent, recognize and treat addiction.”
Ostensibly these are laudable goals that are almost universally endorsed. The perceived organizational purpose and public persona are altruistic and humanitarian. Treating addiction not only saves individual lives but improves the community. It is for the common good.
Abuse Hidden Under Benevolence and Torture as Treatment
History reveals that all manner of abuse can lie underneath a patina of benevolence. In the past few months alone we have both Bill Cosby and the British Parliamentary pedophile ring as prototypical examples. Both cases reveal a decades long coverup of allegations in which the abusers escaped little or no investigation into their alleged crimes. Abuse of power with a large gap between the power of the abuser and the powerlessness of the abused is a common denominator. If the abuser endorses our own beliefs systems it creates a discord that promotes disbelief. It does not fit. Accusations are dismissed, deflected or otherwise suppressed. Power effectively extinguishes the truth. Disbelieved and delegitimized, information is suppressed, charges are not filed and law enforcement and the media turn a blinkered eye for decades. Indifference, disbelief, rationalization and cognitive dissonance prevent exposure and accountability. Hidden in plain site the truth was there and easy to find. The problem was no one was looking. Most did not want to look.
It does not take much sleuthing to uncover what is beneath the veil of the American Society of Addiction Medicine. The history, mentality and mechanics are well documented and reveal where they came from, how they evolved and what they have planned. It is a complicated web and hard to explain but once the pieces of the puzzle are fit together it is clear. But it involves assembling a complex puzzle by finding the individual pieces scattered in disparate areas including the regulatory, clinical, administrative and professional niches of the medical profession, Alcoholics Anonymous and 12-step related organization, public policy, all levels of the political arena and other areas. Once put together the portrait is clear.
In reality the ASAM is a political action group or special interest group that is designed to cement the chronic relapsing brain disease model with lifelong abstinence and spiritual recovery as the one and only treatment for addiction. A.A. is used as the energy source of the operation. By labeling addiction a “disease” requiring “treatment” in which someone is helpless they are able to dictate all aspects by coercion and control. But in my opinion the A.A. ideology is just used as a ruse to support the multi-billion dollar drug and alcohol testing, assessment and treatment industry. The zero-tolerance mindset of the “treaters” combined with the “helplessness” of the diseased enables them to erect a revolving door of testing, assessment and treatment that provides them with both control and a steady stream of money.
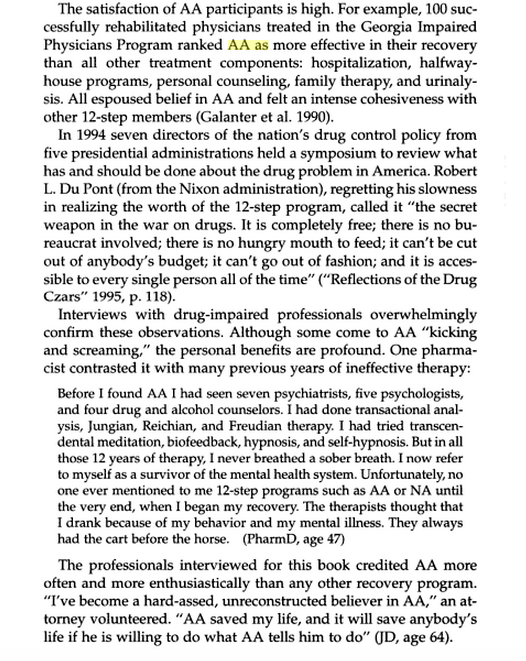
The FSPHP mandates 12-step ideology on all doctors in a zero-tolerance system of abuse and control while at the same time putting out misinformation that the PHP programs are the “new paradigm.” The page below is from the book Drug-Impaired Professionals by Robert Holman Coombs.
This is they type of propaganda these groups have propagated. What is described above is absurd and unrealistic but it is reported, reproduced and repeated to the point that it is accepted as the truth.
The majority of physicians referred to these programs are not even addicts. These programs of Zero-tolerance and 12-step indoctrination are based on coercion and control. They are causing many doctors to die by suicide as they are feeling hopeless, helpless and defeated. This portrayal of a group of blissful 12-stepping doctors over the moon because they found spirituality is nonsense.
But you will not find many doctors speaking out against them for fear of “contingency management.” Disagreeing or even questioning PHP practices including the validity of 12-step can literally cost you your license.
I have spoken to multiple physicians and nurses and have encouraged them to tell their stories here but they are afraid of retribution and “unintended consequences.” And who can blame them?
They can send you back to one of the “PHP-approved” facilities for “stinkin thinkin.”
Unfortunately the ASAM and FSPHP have successfully bamboozled others into believing they are true experts with noble intent. They have bamboozled the Federation of State Medical Boards (FSMB) to the point where they have gained autonomy and unrestrained managerial prerogative. They essentially use the state Boards to impose sanction on doctors who they report doctors for “noncompliance” which includes disagreeing with or questioning mandated A.A or refusing to admit you have a chronic relapsing brain disease when you in fact do not. They are in fact imposing A.A. on doctors and forcing them to accept their thinking under threat of loss of licensure. This violates the Establishment Clause and is a very serious problem that is being ignored. It is a slippery slope we are on.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness” that predates impairment often by many years.”
It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A. A. language –stinking thinking.”
The ASAM has monopolized addiction treatment in the United States. But what the FSPHP arm has done is far more sinister. A.A. has effectively taken over regulatory medicine and the private lives of doctors as a form of social control. A doctor can be referred to a PHP for virtually anything and if the PHP believes he or she is in need of an assessment it will be done by a “PHP-approved” facility which means it will be done by a 12-step facility. The PHP selects who will be monitored and dictates every aspect of what that entails and the entire process is done within the confines of A.A. ideology. It is a, in fact, a rigged game as the medical directors of the PHP approved facilities can all be seen on this list of like-minded docs who refer to theselves as “trusted servants” and “believe that evidence from extensive, well-designed studies demonstrates the great benefits of Twelve-Step recovery modalities including Twelve Step Facilitation in promoting long-term recovery.”
A.A. is imposed on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. And the bottom line is that A.A. has taken over all aspects of “physician health” and is forcing doctors to accept doctrine that is perhaps helpful to a few, useless or unneeded for many, and harmful and sometimes lethal to others. This is unacceptable and it needs to be recognized.
“New Paradigm” of Zero-Tolerance and 12-step Spirituality Based on “success” of PHP to Move to Other Occupations and Kids.
To move this “new paradigm” to other populations they had to gain control of the doctors first. They have not only created a monopoly but buffered themselves from physicians who may disagree with what they are doing to others. This current system essentially stifles them.
The power, immunity and impunity this group yields over doctors was done silently and with no opposition. It was done by sequential public-policy steps. This is why anyone interested in civil liberties and human rights should recognize the menace this presents to society. The scaffold is in place and they are just adding more nooses. Just ask the airline pilots. They plan to impose similar systems on teachers, students and athletes.
And this is all spelled out in the ASAM White Paper on Drug Testing. What people need to realized is what is described therein is just a few public policy steps away from them. The only organization they have to convince is the organization that regulates any type of professional license, employment or benefit.
Gaining regulatory sway in the medical field and control over individual doctors was necessary to move this model to other populations. It is merely a stepping stone for things to come. It is only a few public policy steps from us to you.
This impacts us all. It enables control of research, public policy and public health. It is a system that suppresses dissent and shapes conformity. The FSPHP encourages the confidential referral of outliers.
The ASAM is pro-drug war and anti-medical marijuana. This essentially silences most doctors for fear of being recognized and being brought in. I know many doctors who will not even talk about it in public.
This is fixed doctrine and will not change.
That is why the ACLU and other groups who promote civil rights, those who are against the drug war and anyone involved in Medical Marijuana need to step in. These groups need to recognize the reality of who these people are, what they have planned and understand why they need to be stopped. They are currently not even in the public eye and by outward appearances they appear to be benign. In truth they are malignant and rapidly metastasizing without any symptoms.
In Order to Stop This the Following Must be Done
1) get a team of epidemiologists/statisticians to attack the “evidence-base” and “research” that the ASAM/FSPHP has used to support their claims (junk science, pseudoscience, success of 12-step, etc) and do a Cochrane type meta-analysis that will show there is little to no basis for it.
2) Demand accountability of the PHPs. Assign accountability to the Medical Societies and Departments of Public Health. Demand they be accountable for state-contractors with the Medical Boards (many of whom are complicit–in Massachusetts the Board of Registration in Medicine is simply an extension of the state PHP-i.e. Like-minds.
3) Demand that the criminal activity taking place within these PHPs be addressed by law enforcement.
4) Demand the Attorney General enforce the rampant Establishment Clause Violations occurring with mass 12-step coercion.
5) Identify and expose the backgrounds of many of the individuals involved including felons and double felons who reinvented themselves as “addiction medicine” doctors. Many of these individuals are repeat offenders with a history of manipulating the system who should have never had their licenses returned. In my opinion the ASAM/FSPHP/LMD rigged system is an example of corporate psychopathy. While corporate level psychopathy is estimated at around 3% the numbers here appear to be much higher if one looks at the moral disengagement, unethical decision making, lack of empathy and externalization of blame evident in their personal histories.
6) Correctly identify that this system of institutional injustice is responsible for the astronomical suicide rate in physicians. This is due to the fact that doctors who need help are not getting it for fear of being ensnared by the state PHP and those already ensnared are being subject to coercion, abuse, institutional injustice, degradation, dehumanization, delegitimization and civil and human rights abuses and that this is a public health emergency that needs to be addressed.
7) reveal the scam set up between the PHPs, rogue labs, and “PHP-preferred” assessment and treatment gulags.
8) show how this is only a few public policy steps from Doctors to Pilots to Teachers to students to kids. etc. etc.
This necessitates that we get the conversation going before it is too late.
“That everyone shall exert himself in that state of life in which he is placed, to practice true humanity towards his fellow men, on that depends the future of mankind.” – Albert Schweitzer“By and by never comes” –St Augustine
“A day’s impact is better than a month of dead pull”-Justice Oliver Wendell Holmes, Jr.
I am looking for a few honest and credible statisticians, biostatisticians or epidemiologists who want to make a difference in the spirit of service and helping others. I can’t pay you but you would be combating injustice, corruption and dishonesty. You would be doing your part in helping the Medical Profession, honest and decent doctors, our country and perhaps our future.
It is only a few public policy steps and minor changes in state regulatory statutes before what is described in the ASAM White Paper on Drug Testing comes to fruition. Before we know it the Drug and Alcohol Testing Industries “New Paradigm” as described here by Robert Dupont will be ushered in as it did with doctors; not with a bang but a whimper. From the ASAM white Paper:
“THIS WHITE PAPER ENCOURAGES WIDER AND “SMARTER” USE OF DRUG TESTING WITHIN THE PRACTICE OF MEDICINE AND, BEYOND THAT,BROADLY WITHIN AMERICAN SOCIETY. SMARTER DRUG TESTING MEANS INCREASED USE OF RANDOM TESTING* RATHER THAN THE MORE COMMON SCHEDULED TESTING,* AND IT MEANS TESTING NOT ONLY URINE BUT ALSO OTHER MATRICES SUCH AS BLOOD, ORAL FLUID (SALIVA), HAIR, NAILS, SWEAT AND BREATH WHEN THOSE MATRICES MATCH THE INTENDED ASSESSMENT PROCESS. IN ADDITION, SMARTER TESTING MEANS TESTING BASED UPON CLINICAL INDICATION FOR A BROAD AND ROTATING PANEL OF DRUGS RATHER THAN ONLY TESTING FOR THE TRADITIONAL FIVE-DRUG PANEL.”
To prevent this future drug testing dystopia, that includes testing schoolchildren, we need to take a step back and analyze the reliability and credibility of the “evidence-base” behind these multiple non-FDA approved forensic drug and alcohol tests and testing devices the ASAM proposes be used on the population at large utilizing the Medical Profession as a urine collection agency and bypassing forensic drug testing protocol by calling this “evaluation” and treatment rather than “monitoring” and punishment. New definitions, loopholes, secrecy and subterfuge are the bread and butter of these prohibitionist profiteers.
Amazingly, there has been no Academic review of these tests, let alone a Cochrane type critical analysis. It is essentially untapped territory. In addition there has been no Institute of Medicine type Conflict of Interest Analysis. And that is why I am asking for help from statisticians, biostatisticians and epidemiologists. The task would entail a review of the literature prior to the introduction of these tests for evidence base of forensic applicability (there essentially is none) and a review of the literature peri-and post marketing of these devices to assess the reliability and credibility of the underlying methodology and ascertain the evidence-base. The goal would be publication in both academic journals and presentation to the general public through media publication with the assistance of investigative journalists and other writers. The goal is to get the truth out about these tests and allow both the medial profession and public at large to awaken to the menace this presents to medicine, our society and our future.
Lack of Evidence-Base, Bias and Conflicts of Interest: Making the Data Fit the Hypothesis
I am no epidemiologist or statistician but as with pornography I know junk-science when I see it. Almost all of these tests were introduced with little or no evidence-base and, as with most of their endeavors, they did it below board via loopholes and cutting corners.
The overwhelming majority of papers are small, methodologically flawed, non-randomized, non-blinded retrospective studies in that appear to make the data fit the hypothesis. The authors can invariably be linked to those profiting from the tests of the testing process ( the patent holder, doctors associated with the drug testing labs, ASAM or FSPHP, Robert Dupont, Greg Skipper, etc.)
Ethyl Glucuronide (EtG) was introduced in 1999 as a biomarker for alcohol consumption,1 and was subsequently suggested as a tool to monitor health professionals by Dr. Gregory Skipper because of its high sensitivity to ethanol ingestion.2
Described as the “innovator of EtG as an alcohol biomarker,” Skipper and Friedrich Wurst, “convinced” NMS labs in Pennsylvania “to start performing EtG testing in 2002.
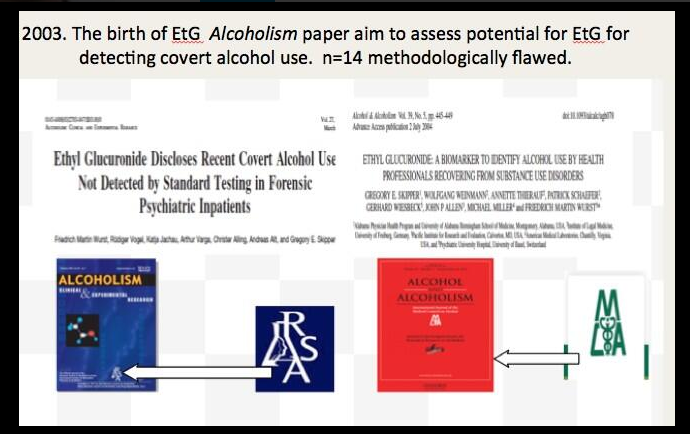
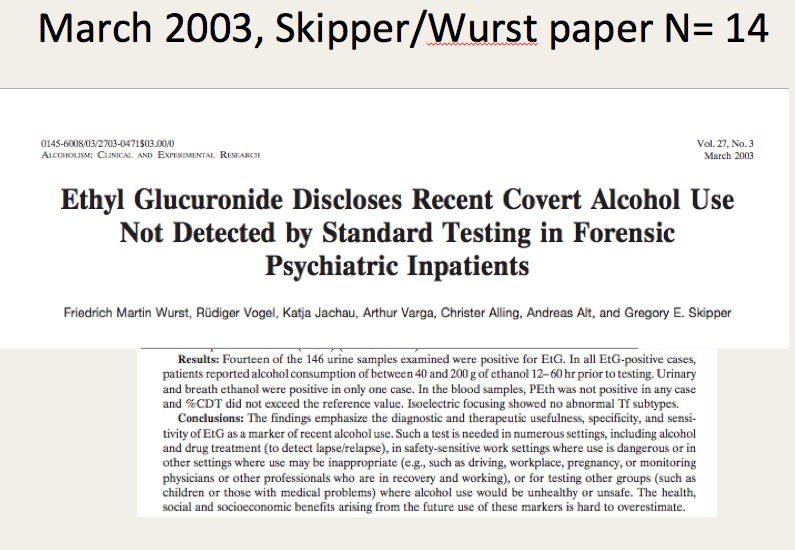
The study most often cited as 100% proof that there is 100% accuracy in EtG testing proving alcohol consumption involved a mere 35 forensic psychiatric inpatients in Germany that was published in 2003.3
Shortly thereafter the Physician Health Programs began using it in monitoring doctors and other professional monitoring programs soon followed.
Laboratory Developed Tests -A Loophole to Avoid FDA Approval and Accountability
Up until the birth of the EtG tests used for forensic drug and alcohol monitoring had to go through the arduous, expensive and necessary FDA approval process. The LDT pathway was designed to develop simple tests with little risk that have low market potential (i;e. the cost of the normal FDA approval process would prohibit them from coming to market). The LDT pathway was designed to improve patient care and help improve diagnosis and treatment. It was not designed for forensic tests. LDT approval does not require in vivo testing. It is essentially an honor system and to develop an LDT it is not even necessary to prove that the test is actually testing what it is purportedly testing for (validity).
So with little to no evidence base they introduced the EtG, had it developed and marketed as a LDT in collusion with unscrupulous labs, and then began using it on physicians being monitored by State PHPs. This then spread to other monitoring organizations in which there was a large power-differential between those ordering the tests and those being tested (criminal-justice, other professional monitoring programs). These biomarkers have never been used in Federal Drug Testing, SAMHSA approved, DOT, and other organizations where unions or other organizations are present and looking out for the best interests of those being tested.
Another example of how this group removes accountability. There has been essentially no oversight or regulation of LDTs. Although there was a recent push for regulation of these tests the Drug and Alcohol Testing Industry Association lobby made sure that forensic tests would be exempt.
They then began publishing “research” on the EtG using the physicians being monitored as subjects. Many of the studies promoting the EtG and other biomarkers can be found in Journals that are linked to organizations that are linked to AA and were organized to educate the medical community.
These small, methodologically flawed studies amount to little more than opinion pieces but This “evidence-base” is predominantly in biased journals published by biased medical “societies.
The EtG was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8Sauerkraut and bananas have even been shown to cause positive EtG levels.9
The United States Substance Abuse and Mental Health Services Administration warned against using a positive EtG as primary or sole evidence of drinking for disciplinary or legal action.10The Wall Street Journal in 2006 reported the problems with the EtG to the general public.11As any rational authority would do, the majority of monitoring agencies abandoned the EtG after these flaws were revealed. The PHPs did not. They continued to use the EtG on doctors uninterruptedly by telling them to avoid any products that could potentially contain alcohol; a ubiquitous substance in the environment. Since that time they have justified and rationalized (EtG)2,1213 use by sequentially raising cutoff levels from 100 to 250 to 500 to 1000 to 2000 to now unknown and adding other LDTs as “confirmation tests such as Ethyl Sulfate (EtS)14,15 Phosphatidyl-Ethanol ( Peth)1617 and other devices such as the Subcutaneous Remote Alcohol Monitoring Bracelet (SCRAM) and, their newest device the Cellular Photo Digital Breathalyzer (CPDB) that has recently been launched, just like the EtG with little to no evidence base other than a pilot study done by Greg Skipper and Robert Dupont.18
A 2013 article published in an ASAM incubated journal Alcoholism: Clinical and Experimental Research promotes the Phosphatidyl-ethanol (PEth ) test to confirm drinking.16 The study was done on physicians being monitored by the Alabama Physician Health Program who tested positive for EtG/EtS alcohol biomarkers. It is co-authored by Robert Dupont, Greg Skipper, and Friedrich Wurst and involved 18 subjects who tested positive for EtG/EtS of whom 7 claimed they did not drink. After finding that 5 of the 7 tested negative for PEth they concluded that “positive PEth testing following positive EtG/EtS results confirms recent drinking. Hard to wrap your head around the science in that one.Skipper is also using both Scram ankle bracelets and the CPDB monitoring in pilots in the Human Interventional Motivational Study (HIMS) Program that was developed in 2009 to “identify, treat and, eventually, re-certify airline pilots with substance abuse problems.
The Cochrane Collaboration does systematic reviews of the literature using conscientious, explicit, and judicious criteria to in order to produce and disseminate only high quality and evidenced based health care, exclude bias, and enhance transparency. The Cochrane database is a current and evolving database that includes the accuracy of diagnostic tests and is internationally recognized as the standard in evidence based health care. This benchmark for evidence based health care and systematic reviews, records just 5 controlled trials under the topic ethyl glucuronide.8,19-21 These 5 studies represent the only high-quality evidence regarding EtG applying to EtG. Information provided by the five studies suggests the following, and only the following:
EtG and EtS measurements increase with alcohol ingestion.
The window of detection is shorter than what is commonly proposed (80 hours).
Individual values are variable both within and between subjects.
Non alcoholic wine can cause positive levels.
Notably, there are no studies that fit Cochrane Criteria, other than non-alcoholic wine, that look at the pharmacokinetics of EtG or EtS in terms of dose-response curves, cut-off levels, specificity drug and food interactions, or modes of ingestion.
SAMHSA notes that there is little research on PEth and that EtG, EtS, and PEth “do not have a strong research base,” and that “it is not known at this time how the test results might be affected by the presence of physical diseases, ethnicity, gender, time, or the use of other drugs. Until considerable more research has occurred, use of these markers should be considered experimental.”
Phosphatidylethanol (PEth), SCRAM, and the yields no data as a test in the Cochrane library.
SAMHSA notes that there is little research on PEth and that EtG, EtS, and PEth “do not have a strong research base,” and that “it is not known at this time how the test results might be affected by the presence of physical diseases, ethnicity, gender, time, or the use of other drugs. Until considerable more research has occurred, use of these markers should be considered experimental.”
Evidence based medicine (EBM) can be defined as the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.22
Medical progress and scientific advancement is occurring so fast that the volume of medical literature is expanding at a rate of greater than 7% per year.23
Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.22
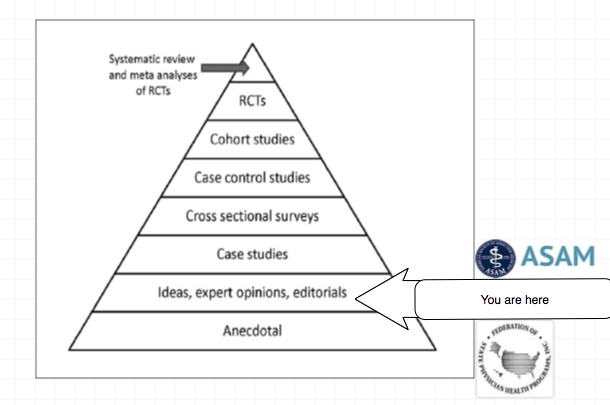
Expert opinion is the lowest level of evidence available in the EBM paradigm.24,25
Fortunately, the scientific method is a tool to help people progress toward the truth despite their susceptibilities to confirmation bias and other errors.26
Unfortunately, due to a confluence of factors (including political) this has not been done. But, unless we want a future as envisioned by Robert Dupont and explained in the the ASAM White Paper on Drug Testing we need to act now. This is not a “New Paradigm” but a “New Inquisition.”
Wurst FM, Kempter C, Seidl S, Alt A. Ethyl glucuronide–a marker of alcohol consumption and a relapse marker with clinical and forensic implications. Alcohol Alcohol. Jan-Feb 1999;34(1):71-77.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcohol Clin Exp Res. Mar 2003;27(3):471-476.
Costantino A, Digregorio EJ, Korn W, Spayd S, Rieders F. The effect of the use of mouthwash on ethylglucuronide concentrations in urine. J Anal Toxicol. Nov-Dec 2006;30(9):659-662.
Reisfield GM, Goldberger BA, Pesce AJ, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. J Anal Toxicol. Jun 2011;35(5):264-268.
Rosano TG, Lin J. Ethyl glucuronide excretion in humans following oral administration of and dermal exposure to ethanol. J Anal Toxicol. Oct 2008;32(8):594-600.
Thierauf A, Gnann H, Wohlfarth A, et al. Urine tested positive for ethyl glucuronide and ethyl sulphate after the consumption of “non-alcoholic” beer. Forensic Sci Int. Oct 10 2010;202(1-3):82-85.
Hoiseth G, Yttredal B, Karinen R, Gjerde H, Christophersen A. Levels of ethyl glucuronide and ethyl sulfate in oral fluid, blood, and urine after use of mouthwash and ingestion of nonalcoholic wine. J Anal Toxicol. Mar 2010;34(2):84-88.
Musshoff F, Albermann E, Madea B. Ethyl glucuronide and ethyl sulfate in urine after consumption of various beverages and foods–misleading results? Int J Legal Med. Nov 2010;124(6):623-630.
Administration SAaMHS. The role of biomarkers in the treatment of alcohol use disorders. In: Advisory SAT, ed2006:1-7.
Helliker K. A test for alcohol–and its flaws. The Wall Street Journal2006.
Wurst FM, Skipper GE, Weinmann W. Ethyl glucuronide–the direct ethanol metabolite on the threshold from science to routine use. Addiction. Dec 2003;98 Suppl 2:51-61.
Wurst FM, Alling C, Aradottir S, et al. Emerging biomarkers: new directions and clinical applications. Alcoholism, clinical and experimental research. Mar 2005;29(3):465-473.
Anton RF. Commentary on: ethyl glucuronide and ethyl sulfate assays in clinical trials, interpretation, and limitations: results of a dose ranging alcohol challenge study and 2 clinical trials. Alcoholism, clinical and experimental research. Jul 2014;38(7):1826-1828.
Hernandez Redondo A, Schroeck A, Kneubuehl B, Weinmann W. Determination of ethyl glucuronide and ethyl sulfate from dried blood spots. International journal of legal medicine. Jul 2013;127(4):769-775.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results. Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Hahn JA, Dobkin LM, Mayanja B, et al. Phosphatidylethanol (PEth) as a biomarker of alcohol consumption in HIV-positive patients in sub-Saharan Africa. Alcoholism, clinical and experimental research. May 2012;36(5):854-862.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study. European addiction research. 2014;20(3):137-142.
Hoiseth G, Bernard JP, Stephanson N, et al. Comparison between the urinary alcohol markers EtG, EtS, and GTOL/5-HIAA in a controlled drinking experiment. Alcohol Alcohol. Mar-Apr 2008;43(2):187-191.
Wojcik MH, Hawthorne JS. Sensitivity of commercial ethyl glucuronide (ETG) testing in screening for alcohol abstinence. Alcohol Alcohol. Jul-Aug 2007;42(4):317-320.
Sarkola T, Dahl H, Eriksson CJ, Helander A. Urinary ethyl glucuronide and 5-hydroxytryptophol levels during repeated ethanol ingestion in healthy human subjects. Alcohol Alcohol. Jul-Aug 2003;38(4):347-351.
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. Jan 13 1996;312(7023):71-72.


 Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3