

“In a time of universal deceit, telling the truth is a revolutionary act.”
— George Orwell
I can think of no other specialty or subspecialty in the profession of medicine where non-existent expertise can be incontestably announced and implemented. If I claimed to be an ace neurosurgeon or an expert otolaryngologist and started practicing my claimed skills in the hospital I would be called on it pretty quick by both colleagues and patients–deemed a delusional fraud and run out on a rail within a week. Both law enforcement, attorneys and psychiatry would be called in short order.
Yet doctors who have not met the usual and customary standards for professional and educational quality that have been identified for medical specialties and subspecialties are able to claim expertise in “addiction medicine” and everybody just lets them.
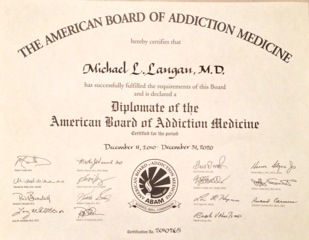
To make this point I sat for the 2010 American Board of Addiction Medicine Certification Examination. I did this to make a point–kind of like seeing how easy it is to buy a gun at a Walmart.
I simply went to the ABAM Website, completed the application and paid the fee.
The requirements to sit for the exam included so many “practice experience hours” over the past five years and 50 CME credits related to addiction.
With a year of psychopharmacology research, a half-day per week moonlighting at the MBTA medical clinic giving drug tests to bus drivers and another overnight moonlighting job giving medical clearance to patients at a local psychiatric hospital detox unit I satisfied the first requirement. For the latter I looked through the last five years of morning reports, noontime lectures and grand rounds I went to and added them up and, falling a little short supplemented the CME credits with some online modules.
And with that I was given a date at Pearson to take the test.
I have absolutely no training or education in the field of addiction medicine. I didn’t pick up a book or study anything. I did not prepare at all. I did not even get a good night’s sleep the night before and stayed up until 2:30 a.m. Nevertheless I went to the testing facility the next morning and finished the test within an hour and a half. My score is below. Aced it. Passing score was 394 and I got a 459.

And the point I am trying to make is I am no expert in Addiction Medicine. Neither is 4000 of me. Yet the letter below says I am. Majority apparently rules.
Giving false expertise to the unqualified and granting them power over others is just as dangerous as the gun from Walmart. They can both kill.
An interest in something does not an expert make. If we allow this then the ASAM 12-step chronic brain disease model not only swallows addiction medicine but tarnishes all of medicine. An imposition by force and the deep pockets of the billion dollar drug and alcohol testing, assessment and treatment industry.
ASAM is not a true medical specialty. It is a special interest group. ABAM is not recognized by the American Board of Medical Specialties (ABMS).
The arguments seem to be:
1) Addiction is a prevalent “disease” that needs to be “treated;”
2) There are not enough Addiction Psychiatrists to diagnose and treat them.
3) Being an M.D. addict or alcoholic gives enough knowledge and apprenticeship skills to diagnose and treat others with the same affliction.
4) Let’s utilize them to fill the void.
This is logical fallacy and it is dangerous.
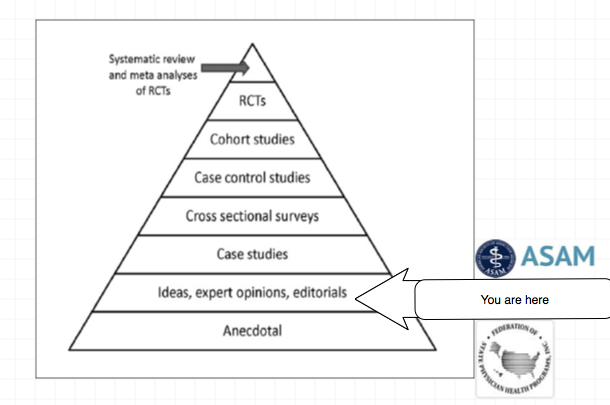
The validity and reliability of opinions lie in their underlying methodology and evidence base. Reliance on the personal authority of any expert or group of experts is the fallacy of appeal to authority.
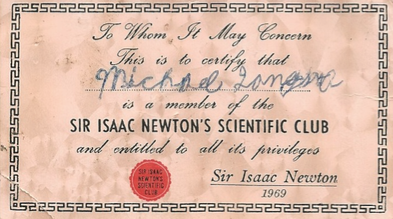
An interest in something does not an expert make. I had an interest in science as a child but my certification as a member of Sir Isaac Newton’s Scientific Club did not make me a scientist.
I have asthma but that does not make me a Pulmonologist. That addiction “specialist” diagnosing and treating you may have 5 years prior been a proctologist; and maybe not even a very good one at that.
Somewhere there may be doctor with no post-graduate training in surgery wielding a scalpel and calling himself an expert surgeon, but it is difficult to imagine that he is a very good one.
I received my ABMS certification without meeting a single person. It was all done by mail. This fits the very definition of “Diploma Mill.” This is not to besmirch those with a sincere interest in helping others with addiction. Many if not most of those involved are sincere. But this is not expertise. This is not authority. And, as we have seen, this low bar opens the door for some very bad apples.

“This election is not about issues,” Rick Davis, John McCain’s campaign manager said this week. “This election is about a composite view of what people take away from these candidates.” That’s a scary thought. For the takeaway is so often base, a reflection more of people’s fears and insecurities than of our hopes and dreams.
— Judith Warner, New York Times, September 4, 2008



 The field of psychology also defines strict guidelines for board certification. The American Board of Professional Psychology was incorporated in 1947 with the support of the American Psychological Association. The ABPP is a unitary governing body of separately incorporated specialty examining boards which assures the establishment, implementation, and maintenance of specialty standards and examinations by its member boards. Through its Central Office, a wide range of administrative support services are provided to ABPP Boards, Board-certified specialists, and the public. Specialization in a defined area within the practice of psychology connotes competency acquired through an organized sequence of formal education, training, and experience. In order to qualify as a specialty affiliated with the ABPP, a specialty must be represented by an examining board which is stable, national in scope, and reflects the current development of the specialty. A specialty board is accepted for affiliation following an intensive self-study and a favorable review by the ABPP affirming that the standards for affiliation have been met. These standards include a thorough description of the area of practice and the pattern of competencies required therein as well as requirements for education, training, and experience, the research basis of the specialty, practice guidelines, and a demonstrated capacity to examine candidates for the specialty on a national level.
The field of psychology also defines strict guidelines for board certification. The American Board of Professional Psychology was incorporated in 1947 with the support of the American Psychological Association. The ABPP is a unitary governing body of separately incorporated specialty examining boards which assures the establishment, implementation, and maintenance of specialty standards and examinations by its member boards. Through its Central Office, a wide range of administrative support services are provided to ABPP Boards, Board-certified specialists, and the public. Specialization in a defined area within the practice of psychology connotes competency acquired through an organized sequence of formal education, training, and experience. In order to qualify as a specialty affiliated with the ABPP, a specialty must be represented by an examining board which is stable, national in scope, and reflects the current development of the specialty. A specialty board is accepted for affiliation following an intensive self-study and a favorable review by the ABPP affirming that the standards for affiliation have been met. These standards include a thorough description of the area of practice and the pattern of competencies required therein as well as requirements for education, training, and experience, the research basis of the specialty, practice guidelines, and a demonstrated capacity to examine candidates for the specialty on a national level.



 Trumpeting the false dichotomy that addiction is a “brain disease” and not a “moral failing” while portraying themselves as altruistic advocates of the afflicted, this subgroup of the ASAM has cultivated an organization that exudes authority, knowledge, respectability, and advocacy. But they are an illegitimate authority and others must be made cognizant of this fact.
Trumpeting the false dichotomy that addiction is a “brain disease” and not a “moral failing” while portraying themselves as altruistic advocates of the afflicted, this subgroup of the ASAM has cultivated an organization that exudes authority, knowledge, respectability, and advocacy. But they are an illegitimate authority and others must be made cognizant of this fact.
 State PHPs are very strict when it comes to choice in rehabilitation facilities for for physicians in need of assessment and treatment for substance abuse.
State PHPs are very strict when it comes to choice in rehabilitation facilities for for physicians in need of assessment and treatment for substance abuse.
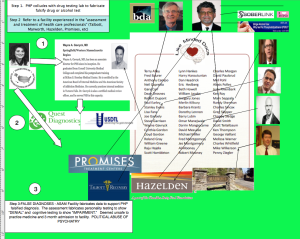 One of the issues Knight and Boyd discussed was the conflicts of interest between the state PHPs and the evaluation centers.
One of the issues Knight and Boyd discussed was the conflicts of interest between the state PHPs and the evaluation centers.


































Hi Mr.Goldsmith,
Currently, these ‘PHP approved evaluation’ centers are the exact same facilities as the PHP ‘treatment’ centers. There centers also have financial relationships with PHP programs and PHP directors.
They charge upwards of $5,000 dollars to the physician plus travel and lodging expenses, because they are often out-of-state.
Former ASAM leader and PHP director Dr.Talbott owned such a facility with a judge as a co-investor. Dr.Talbott was convicted by a jury in a US court of law of coercing a doctor into unnecessary ‘treatment’ for financial gain. How many of these 78% recovery rate come from physicians falsely diagnosed? Dr.Fata, the Michigan doctor convicted of giving false cancer diagnoses, also touted his high ‘treatment success rate’
We’d like you to correct these current questionable practices by ASAM and PHPs. A true independence of diagnosticians and PHPs is a good place to start, with strict oversight and auditing to eliminate all and any financial ties and conflicts of interest. PHP leadership and directors should be replaced by physicians with demonstrated commitment to ethics and personal rights.
Do these steps sound reasonable to you?