 Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Although he specifies the numerical percentage “in physicians at 7.9%,”3 he avoids the use of numbers (14.6%) in the general population. He instead uses the qualifier “somewhat less.” Why is this?
My guess is because it understates the statistical fact that the prevalence found by Kessler in the general population was almost twice that found by Hughes in physicians.
You see, “Somewhat less” is a “detensifier.” It creates an impression of a small disparity between doctors and the general population.
In propaganda this is what is known as a “weasel phrase.” Weasel phrases are used to obfuscate the truth. Weasel phrases mislead those either without the time, or without the sense to see or look any deeper. The problem is it works.
“Methodologic differences may account for this difference,” Earley states, as the Hughes study “surveyed 9, 600 physicians by mail” and “relied on honest and denial-free reports by the physicians; the Kessler study utilized face-to-face interviews with trained interviewers.”1
This is an example of language framing. Language framing uses words and phrases to direct attention to a point of view to advance a vested interest.
In this case the use of the phrase “honest and denial free” in the context of physician reporting imparts associative meaning to the reader.
As denial is a recurring motif and cardinal attribute of physician addiction according to the paradigm, the connotation is that the reports by physicians may have been influenced by dishonesty and denial while face-to-face interviews done by “trained” interviewers were not.
“Framing” is another propaganda technique designed to tell the audience how to interpret the information given through context. The message here is that the somewhat less lifetime prevalence of substance abuse and addiction in physicians found by anonymous mail survey may be underreported as a result of both methodology and denial.
But in actual fact there is a large body of research regarding “social desirability bias” that shows the converse to be true.
One of the most consistent findings of studies of this kind is that socially desirable responding is significantly more likely with face-to-face administered data collection compared with self-administered anonymous modes.4-6
Tourangeau et al. reviewed seven studies comparing self-reports of drug use in surveys conducted in different modes. For each estimate obtained in the studies they calculated the ratio of drug use reported in self-reported surveys to the corresponding estimates in interviewer administered surveys and found that 57 of 63 different comparisons showed higher levels of reporting of drug use in the self-reported mode.7
The principal cause of social desirability bias is the level of perceived anonymity of the reporting situation.7
Evidence-based research does not support Earley’s claim that methodological differences in study design explain the difference in reported lifetime prevalence of substance abuse or addiction between physicians and the general population in these two studies.
Evidence based research would, in fact, make the findings more robust.
Moreover, I find it hard to comprehend the psychodynamics, motivation, and logic of denial and dishonesty in influencing an anonymous survey. So too would anyone else who dare peer beneath the veil. It is, in fact, a Potemkin village. In reality the emperor has no clothes.
- Earley PE. Physician Health Programs and Addiction among Physicians. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed. Baltimore: Lippincott Williams & Wilkens; 2009:531-547.
- Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
- Sudman S, Bradburn NM. Response effects in surveys: A review and synthesis. Chicago: Aldine Publishing; 1974.
- Tourangeau R, Smith TW. Collecting sensitive information with different modes of data collection. In: Couper MP, Baker RP, Bethlehem J, et al., eds. Computer assisted survey information collection. New York: John Wiley & Sons, Inc.; 1998.
- Dillman DA. Mail and telephone surveys: The total design method. New York: Wiley-Interscience; 1978.
- Tourangeau R, Rips LJ, Rasinski KA. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000.
- American Society of Addiction Medicine: Patient Placement Criteria. Chevy Chase, MD: American Society of Addiction Medicine; 2000.
- Merlo LJ, Gold MS. Successful Treatment of Physicians With Addictions: Addiction Impairs More Physicians Than Any Other Disease. Psychiatric Times. 2009;26(9):1-8.


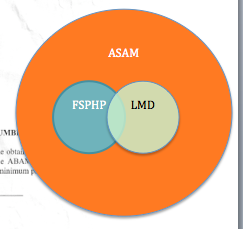
 Three shells and a pea–ASAM, FSPHP, and LMD
Three shells and a pea–ASAM, FSPHP, and LMD
 The auditor also noted this lack of concrete criteria goes against both
The auditor also noted this lack of concrete criteria goes against both 


















 Trumpeting the false dichotomy that addiction is a “brain disease” and not a “moral failing” while portraying themselves as altruistic advocates of the afflicted, this subgroup of the ASAM has cultivated an organization that exudes authority, knowledge, respectability, and advocacy. But they are an illegitimate authority and others must be made cognizant of this fact.
Trumpeting the false dichotomy that addiction is a “brain disease” and not a “moral failing” while portraying themselves as altruistic advocates of the afflicted, this subgroup of the ASAM has cultivated an organization that exudes authority, knowledge, respectability, and advocacy. But they are an illegitimate authority and others must be made cognizant of this fact.
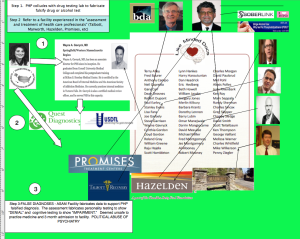 One of the issues Knight and Boyd discussed was the conflicts of interest between the state PHPs and the evaluation centers.
One of the issues Knight and Boyd discussed was the conflicts of interest between the state PHPs and the evaluation centers.