Dr. Langan graduated from Oregon Health Sciences University School Of Medicine, Portland Oregon with an MD 21 years ago. He had his residency training of Geriatric Medicine-Internal Medicine at Beth Israel Deaconess Medicine Center and Internal Medicine at St Vincent Hospital Medicine Center.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David…
We have skirted around this issue before on the ME-P; as well as our related physician-executive leadership, risk-management and career development essays in our books and print publications.
But now, we look directly into the face of the terminal demon/beast.
So, her is a powerful look at the growing problem of physician suicide by two leading physicians and expert-bloggers Michael Lawrence Langan MD; an ME-P “thought-leader” – as well as a video by Pamela Wible MD.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available…
The evidence that Physician Health Services, Inc. (PHS) is committing crimes has been free-floating for the past two years. It has been posted on Reddit, Twitter, Facebook, Linkedin, blogged, faxed, and phoned. The response? Absolute silence.
The procedural, ethical and criminal violations are clear and many. The incontrovertible evidence has been directly delivered to individuals who should address this but for some reason do not. This is not a matter of opinion folks but a matter of fact. Time and time again we hear of egregious misconduct hidden for decades because of cognitive dissonance and blinkered apathy.
They are engaging in criminal activity within the walls of an institution whose foundation is the antithesis of this groups actions and it must be addressed. Either support what the documents show or do something about it.
So please sign this petition and call Massachusetts State Auditor Suzanne Bump at 617-727-6200
Institutional injustice just like that being committed by Luis Sanchez, Linda Bresnahan and the corrupt MRO Wayne Gavryck is killing doctors across the country. They need to be held accountable. Help me hold them accountable.
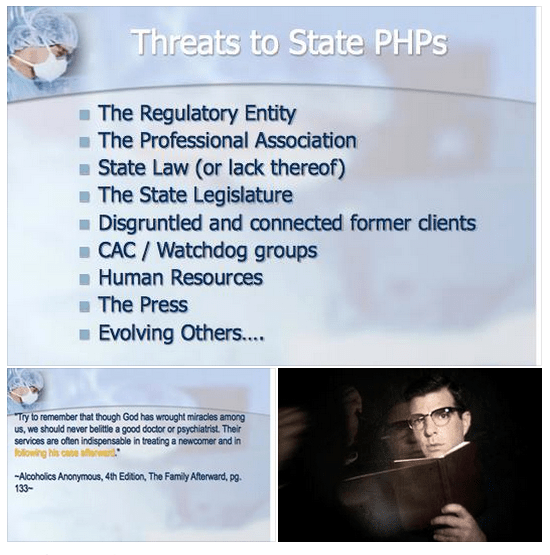
The blue slides below are from a presentation at the 2014 FSPHP spring meeting in Denver, Colorado and can be seen here. The presentation was given by past FSPHP President Gary Carr, MD, Current FSPHP President Warren Prendergast, MD, West Virginia PHP Director Brad Hall, MD and Montana PHP Director Mike Ramirez, MS.
This needs to be seen as a “to-do” list.
A.A. = ASAM = FSPHP
The quote is from Alcoholics Anonymous and the full passage is as follows:
“We are convinced that a spiritual mode of living is a most powerful health restorative. We, who have recovered from serious drinking, are miracles of mental health. But we have seen remarkable transformations in our bodies. Hardly one of our crowd now shows any mark of dissipation. But this does not mean that we disregard human health measures. God has abundantly supplied this world with fine doctors, psychologists, and practitioners of various kinds. Do not hesitate to take your health problems to such persons. Most of them give freely of themselves, that their fellows may enjoy sound minds and bodies. Try to remember that though God has wrought miracles among us, we should never belittle a good doctor or psychiatrist. Their services are often indispensable in treating a newcomer and in following his case afterward.”–Alcoholics Anonymous, 4th Edition, The Family Afterward
Federation of State Physician Health Program (FSPHP) physicians often quote A.A. because they are defined by A.A. in both mechanics and mentality. The “impaired physician” movement began with evangelical recovered addict and alcoholic physicians whose recovery was based on 12- step spirituality. As this group molded into the American Society of Addiction Medicine (ASAM) many of them found employment at 12-step rehabilitation facilities and others joined their state Physician Health Programs and organized under the FSPHP. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insiders knowledge of recovery as brandished in this A.A. passage which I find condescending toward the medical profession and oddly narcissistic.
This special knowledge, of course, was based on the chronic relapsing brain disease model with lifelong abstinence and participation in 12-step recovery.
These “miracles of mental health” joined their state PHPs and those who did not agree with their rigid inflexible views were removed. Those with access to special secret knowledge were eventually able to outvote those with intelligence and open minds as this groupthink infested and eventually monopolized PHPs.
It is important to understand that the ideology of A.A. is the ideology of the ASAM is the ideology of the FSPHP
Like all “front-groups” the ASAM purports to serve one agenda while in reality serving another. The ASAM claims to be a “physician society with a focus on addiction and its treatment” According to their website their mission is to
increase access to and improve the quality of addiction treatment;
to educate physicians (including medical and osteopathic students), other health care providers and the public;
to support research and prevention;
to promote the appropriate role of the physician in the care of patients with addiction;
and to establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers and consumers of health care services, and the general public
In order to accomplish this the American Board of Addiction Medicine certifies doctors to “provide assurance to the American public that Addiction Medicine physicians have the knowledge and skills to prevent, recognize and treat addiction.”
Ostensibly these are laudable goals that are almost universally endorsed. The perceived organizational purpose and public persona are altruistic and humanitarian. Treating addiction not only saves individual lives but improves the community. It is for the common good.
Abuse Hidden Under Benevolence and Torture as Treatment
History reveals that all manner of abuse can lie underneath a patina of benevolence. In the past few months alone we have both Bill Cosby and the British Parliamentary pedophile ring as prototypical examples. Both cases reveal a decades long coverup of allegations in which the abusers escaped little or no investigation into their alleged crimes. Abuse of power with a large gap between the power of the abuser and the powerlessness of the abused is a common denominator. If the abuser endorses our own beliefs systems it creates a discord that promotes disbelief. It does not fit. Accusations are dismissed, deflected or otherwise suppressed. Power effectively extinguishes the truth. Disbelieved and delegitimized, information is suppressed, charges are not filed and law enforcement and the media turn a blinkered eye for decades. Indifference, disbelief, rationalization and cognitive dissonance prevent exposure and accountability. Hidden in plain site the truth was there and easy to find. The problem was no one was looking. Most did not want to look.
It does not take much sleuthing to uncover what is beneath the veil of the American Society of Addiction Medicine. The history, mentality and mechanics are well documented and reveal where they came from, how they evolved and what they have planned. It is a complicated web and hard to explain but once the pieces of the puzzle are fit together it is clear. But it involves assembling a complex puzzle by finding the individual pieces scattered in disparate areas including the regulatory, clinical, administrative and professional niches of the medical profession, Alcoholics Anonymous and 12-step related organization, public policy, all levels of the political arena and other areas. Once put together the portrait is clear.
In reality the ASAM is a political action group or special interest group that is designed to cement the chronic relapsing brain disease model with lifelong abstinence and spiritual recovery as the one and only treatment for addiction. A.A. is used as the energy source of the operation. By labeling addiction a “disease” requiring “treatment” in which someone is helpless they are able to dictate all aspects by coercion and control. But in my opinion the A.A. ideology is just used as a ruse to support the multi-billion dollar drug and alcohol testing, assessment and treatment industry. The zero-tolerance mindset of the “treaters” combined with the “helplessness” of the diseased enables them to erect a revolving door of testing, assessment and treatment that provides them with both control and a steady stream of money.
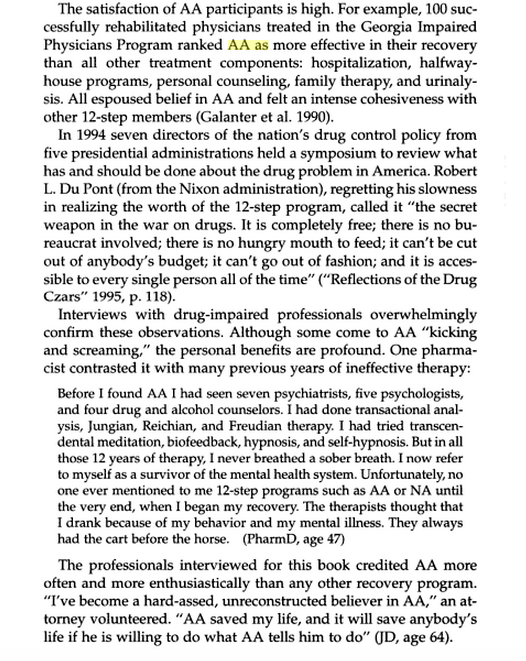
The FSPHP mandates 12-step ideology on all doctors in a zero-tolerance system of abuse and control while at the same time putting out misinformation that the PHP programs are the “new paradigm.” The page below is from the book Drug-Impaired Professionals by Robert Holman Coombs.
This is they type of propaganda these groups have propagated. What is described above is absurd and unrealistic but it is reported, reproduced and repeated to the point that it is accepted as the truth.
The majority of physicians referred to these programs are not even addicts. These programs of Zero-tolerance and 12-step indoctrination are based on coercion and control. They are causing many doctors to die by suicide as they are feeling hopeless, helpless and defeated. This portrayal of a group of blissful 12-stepping doctors over the moon because they found spirituality is nonsense.
But you will not find many doctors speaking out against them for fear of “contingency management.” Disagreeing or even questioning PHP practices including the validity of 12-step can literally cost you your license.
I have spoken to multiple physicians and nurses and have encouraged them to tell their stories here but they are afraid of retribution and “unintended consequences.” And who can blame them?
They can send you back to one of the “PHP-approved” facilities for “stinkin thinkin.”
Unfortunately the ASAM and FSPHP have successfully bamboozled others into believing they are true experts with noble intent. They have bamboozled the Federation of State Medical Boards (FSMB) to the point where they have gained autonomy and unrestrained managerial prerogative. They essentially use the state Boards to impose sanction on doctors who they report doctors for “noncompliance” which includes disagreeing with or questioning mandated A.A or refusing to admit you have a chronic relapsing brain disease when you in fact do not. They are in fact imposing A.A. on doctors and forcing them to accept their thinking under threat of loss of licensure. This violates the Establishment Clause and is a very serious problem that is being ignored. It is a slippery slope we are on.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness” that predates impairment often by many years.”
It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A. A. language –stinking thinking.”
The ASAM has monopolized addiction treatment in the United States. But what the FSPHP arm has done is far more sinister. A.A. has effectively taken over regulatory medicine and the private lives of doctors as a form of social control. A doctor can be referred to a PHP for virtually anything and if the PHP believes he or she is in need of an assessment it will be done by a “PHP-approved” facility which means it will be done by a 12-step facility. The PHP selects who will be monitored and dictates every aspect of what that entails and the entire process is done within the confines of A.A. ideology. It is a, in fact, a rigged game as the medical directors of the PHP approved facilities can all be seen on this list of like-minded docs who refer to theselves as “trusted servants” and “believe that evidence from extensive, well-designed studies demonstrates the great benefits of Twelve-Step recovery modalities including Twelve Step Facilitation in promoting long-term recovery.”
A.A. is imposed on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. And the bottom line is that A.A. has taken over all aspects of “physician health” and is forcing doctors to accept doctrine that is perhaps helpful to a few, useless or unneeded for many, and harmful and sometimes lethal to others. This is unacceptable and it needs to be recognized.
“New Paradigm” of Zero-Tolerance and 12-step Spirituality Based on “success” of PHP to Move to Other Occupations and Kids.
To move this “new paradigm” to other populations they had to gain control of the doctors first. They have not only created a monopoly but buffered themselves from physicians who may disagree with what they are doing to others. This current system essentially stifles them.
The power, immunity and impunity this group yields over doctors was done silently and with no opposition. It was done by sequential public-policy steps. This is why anyone interested in civil liberties and human rights should recognize the menace this presents to society. The scaffold is in place and they are just adding more nooses. Just ask the airline pilots. They plan to impose similar systems on teachers, students and athletes.
And this is all spelled out in the ASAM White Paper on Drug Testing. What people need to realized is what is described therein is just a few public policy steps away from them. The only organization they have to convince is the organization that regulates any type of professional license, employment or benefit.
Gaining regulatory sway in the medical field and control over individual doctors was necessary to move this model to other populations. It is merely a stepping stone for things to come. It is only a few public policy steps from us to you.
This impacts us all. It enables control of research, public policy and public health. It is a system that suppresses dissent and shapes conformity. The FSPHP encourages the confidential referral of outliers.
The ASAM is pro-drug war and anti-medical marijuana. This essentially silences most doctors for fear of being recognized and being brought in. I know many doctors who will not even talk about it in public.
This is fixed doctrine and will not change.
That is why the ACLU and other groups who promote civil rights, those who are against the drug war and anyone involved in Medical Marijuana need to step in. These groups need to recognize the reality of who these people are, what they have planned and understand why they need to be stopped. They are currently not even in the public eye and by outward appearances they appear to be benign. In truth they are malignant and rapidly metastasizing without any symptoms.
In Order to Stop This the Following Must be Done
1) get a team of epidemiologists/statisticians to attack the “evidence-base” and “research” that the ASAM/FSPHP has used to support their claims (junk science, pseudoscience, success of 12-step, etc) and do a Cochrane type meta-analysis that will show there is little to no basis for it.
2) Demand accountability of the PHPs. Assign accountability to the Medical Societies and Departments of Public Health. Demand they be accountable for state-contractors with the Medical Boards (many of whom are complicit–in Massachusetts the Board of Registration in Medicine is simply an extension of the state PHP-i.e. Like-minds.
3) Demand that the criminal activity taking place within these PHPs be addressed by law enforcement.
4) Demand the Attorney General enforce the rampant Establishment Clause Violations occurring with mass 12-step coercion.
5) Identify and expose the backgrounds of many of the individuals involved including felons and double felons who reinvented themselves as “addiction medicine” doctors. Many of these individuals are repeat offenders with a history of manipulating the system who should have never had their licenses returned. In my opinion the ASAM/FSPHP/LMD rigged system is an example of corporate psychopathy. While corporate level psychopathy is estimated at around 3% the numbers here appear to be much higher if one looks at the moral disengagement, unethical decision making, lack of empathy and externalization of blame evident in their personal histories.
6) Correctly identify that this system of institutional injustice is responsible for the astronomical suicide rate in physicians. This is due to the fact that doctors who need help are not getting it for fear of being ensnared by the state PHP and those already ensnared are being subject to coercion, abuse, institutional injustice, degradation, dehumanization, delegitimization and civil and human rights abuses and that this is a public health emergency that needs to be addressed.
7) reveal the scam set up between the PHPs, rogue labs, and “PHP-preferred” assessment and treatment gulags.
8) show how this is only a few public policy steps from Doctors to Pilots to Teachers to students to kids. etc. etc.
This necessitates that we get the conversation going before it is too late.
Please listen to this podcast interviewing Dr. Michael Langan. This is very important to understand. AA is a dangerous cult and even doctors are not safe. Either join the cult or your license is in jeopardy. This is the opposite of help. This is abuse and indoctrination. This must stop. Thank you to Dr. Langan for his bravery.
The article below was published in the now defunct magazine Gray Areas almost twenty years ago. (Vol. 4, No. 1, Spring 1995 pp. 75-77). Antipolygraph.og founder George Maschke noted in 2008 that article “makes a good introduction to the pseudoscience of polygraphy” and “the criticisms of polygraphy remain valid today.” They still do.
The Art of Deception: Polygraph Lie Detection
By Michael Lawrence Langan, M.D.
I’d swear to it on my very soul, If I lie, may I fall down cold.”
– Rubin and Cherise
(Hunter/Garcia)
The accuracy of polygraphic lie detection is slightly above chance. Nevertheless, State and local police departments and law enforcement agencies across the United States are devoted proponents of this unscientific and specious device. In addition, the American public seems to lend an implicit credence to the “lie detector” as evinced by its ubiquitous use on television crime shows and in “whodunit” literature. It is given overt attributions of credibility on tabloid type talk shows and news shows. For example, in the highly publicized case of Tonya Harding a reporter stated, not with removed objectivity but with sardonic grin and mocking emphasis, that the accused had failed two polygraph tests. The implied assumption is that if the person has failed the polygraph test, then therefore he or she is guilty regardless of other evidence. Bottom line. Culpa ex machina. End of story.
Lie detection by the polygraph is based on the premise that the act of telling a lie causes specific, universal, and reproducible physiological responses as manifested by the autonomic nervous system. (Saxe, 1991) These physiological responses, which are largely outside the influence of voluntary control, are then measured by the polygraph instrument. The polygraph itself is simplistic in design. It consists of several devices which are attached to the subject to record blood pressure, pulse, respiration, and galvanic skin response (which is related to perspiration). The results are then recorded on a moving paper by a “kymograph.” Hence any change of one of the autonomic nervous system variables will be recorded on the paper as a change from baseline. The polygraph examiner then interprets the tracing. A characteristic change from baseline on a relevant question is interpreted as a lie.
In fact, the polygraph test does measure autonomic nervous system activity. The role of the autonomic nervous system with its sympathetic and parasympathetic branches is well defined within the field of medicine, and was well described by the French physician Claude Bernard over a century ago. The primary role of the autonomic nervous system is to maintain bodily homeostasis to allow the individual to exist in a changing environment.
Simplistically described, the autonomic nervous system is a part of the peripheral nervous system which consists of a variety of outgoing nerve pathways that regulate important physiological functions generally outside of voluntary and conscious control. Thus, respiration, body temperature, heart rate, digestion, sweating, and blood pressure are all, partly or entirely, regulated by the autonomic nervous system. It is divided into sympathetic and parasympathetic branches which have contrasting functions in terms of effect. The sympathetic branch increases heart rate, respiratory rate, blood pressure, and perspiration. It is active at all times but varies with the constantly changing environment, and is especially active during rage or fright and prepares the body for the so called “fight or flight” phenomenon. Many of these reactions are caused by the release of epinephrine. The parasympathetic nervous system, on the other hand, is primarily involved with conservation and restoration. It is the sympathetic branch of the autonomic nervous system that the polygraph measures in terms of its activity. Thus, from a medical perspective it is entirely valid that the polygraph will accurately measure sympathetic nervous system activity with its instrumentation.
The false assumption of the polygraph test is that dishonesty is the sole cause of sympathetic arousal during a polygraph examination. Deception is a cognitive phenomenon that cannot be measured. Indeed, throughout the entire history of medicine there has not been a single scientific study that demonstrated evidence that a cognitive phenomenon (such as love, hatred, truth, altruism, jealousy) could be measured. Since, in the complex realm of truth and deception, there is no known physiological response that correlates with lying, then there is no validity to the test. Although the act of lying can elicit fear and anxiety via the sympathetic nervous system, so can multiple other confounding and complex emotional factors including stress, embarrassment, anger, and fear. “Deception itself cannot be measured directly.” (Steinbrook, 1992) In addition, each individual differs in autonomic lability. Some people stay calm with a gun at their head. While others get autonomically excited, with heart thumping and palms sweating at simply shaking someone’s hand.
In reality, the examination itself is inherently designed to elicit fear and anxiety. It is an interrogation. If this fear and anxiety are recorded on a relevant question, then you have failed that question according to the polygraph “experts.”
The polygraph technique begins with a pre-test. After a sixth-grade level lecture on the nervous system and a proclamation of the test’s infallibility, the examiner will go over all of the questions that have been formulated.
These questions consist of control questions, relevant questions, and irrelevant questions. The subject will then be attached to the polygraph equipment and the formal testing begins.
The most crucial questions on the polygraph examination, or “Control Question Test,” are the control questions and relevant questions. The control questions are garnered from the suspect by asking him an innocuous question which could not be truthfully denied. For example, “Have you ever thought of hurting someone?” or “Have you ever lied to anyone?” The responses to the control questions will elicit some degree of autonomic activity which can then serve as a baseline for which to compare subsequent questions. The relevant questions pertain to the actual investigation at hand. The magnitude of responses to relevant questions and control questions as compared with the irrelevant questions is then interpreted, in a non-blinded manner, by the examiner. The assumption is, that if you are prevaricating, the relevant questions will cause a greater response than the control questions. So if the question “Have you ever been late for an appointment?” (control question) elicits less of an emotive response on the polygraph equipment than “Did you murder and rape your girlfriend?” (relevant question) you have failed the test. And, according to the American Polygraph Association (APA) you are lying. Assuming the subject is innocent, it is fairly obvious that he would respond with more emotional autonomic activity to a question regarding a recently deceased loved one than he would an inquiry about punctuality. Obvious to everyone, that is, but the APA.
The APA is a professional organization for polygraph examiners who have complete faith in the accuracy of the test. They have their own trade journalPolygraph in which they report scientifically worthless studies and brandish anecdotes of the wonders of their trade. The majority of these members can pride themselves on completing a 6 week to 6 month post- high school training course in the art of polygraphy. They have no formal training in medicine, psychology, physiology, or behavior; the very disciplines on which the testing is based. The majority of them cater to the legal system wherein their economic livelihood depends.
Since they are primarily paid to identify guilty suspects, motivational factors may play a part in their eagerness to find the guilty suspect. (Kleinmuntz, 1987)
The accuracy of any test is determined by that test’s sensitivity (ability to find a positive) and specificity (ability to find a negative). A polygraph examiner will ardently tell you that the exam has somewhere in the neighborhood of a 95% sensitivity rate. This means that if 100 guilty suspects are given a polygraph exam, 95 of them will be detected through the test. Only five of the 100 will be a false negative and not be detected by this miraculous method. Likewise they will claim a similar specificity rate, and state that if you are telling the truth then you have almost a 100% chance of being cleared by the test. John Reid, the inventor of the Control Question Test claimed 99% accuracy. (Reid and Inbau, 1977)
This is clearly not accurate. The polygraph was not subjected to much critical and scientific investigation until the last two decades. (Saxe, et al., 1983) Since this time there have been a number of studies of sound scientific design and methodology which clearly refute the high specificity and sensitivity that polygraph advocates claim. These studies have appeared in reputable peer-reviewed journals and not trade publications. Horvath, for example, reported a sensitivity of 76 percent and a specificity of 52 percent. (Horvath, 1977) This means that out of 100 liars 76 of them will be detected by the polygraph. What is astonishing though is the specificity of 52 percent. This means that out of 100 people who are not lying, 52 will be identified as telling the truth while 48 of the honest individuals will be branded as liars. The odds are similar to that of a coin toss which would have a specificity of 50 percent. Barland and Raskin’s study actually demonstrated a specificity of 45%. Worse than a coin toss. (Barland and Raskin, 1976) Multiple other studies have shown similar results. (Brett, et al., 1986, Kleinmuntz and Szucko, 1984, Lykken, 1984).
The polygraph examiner likens his “skill” to that of the radiologist reading a chest X-Ray or a cardiologist interpreting an EKG. (Barefoot, 1974) This analogy is not only ridiculous but, in fact, if a medical test had a similar sensitivity and specificity to that of the polygraph examination it would simply not be used in the field of medicine. They will cite the fact that the polygraph has been used in the United States for greater than 70 years as if longevity is directly related to validity. They will state that they have personally administered hundreds or thousands of these tests, and have almost never been wrong, as if total number of tests given constitutes accuracy.
They are so convinced of the accuracy of the polygraph that they regard opponents of polygraphy as communists and do-nothing professors. (Arther, 1986) It doesn’t occur to them that someone with a Ph.D. and years of research experience, in the very subjects they ignorantly dabble in, may know something more than they do.
It is astounding that the criminal justice system has institutionalized and perpetuated a so called “technology” that lacks scientific evidence and is in fact rejected by the scientific community. It is as ludicrous as procuring the so called “love meter” machine from the amusement park which measures galvanic skin response and placing it in the courtroom. But in a backward legal system which has been known to use psychics to help with unsolved murders and has allowed the mentally retarded to serve as jurors, it is not entirely surprising.
The tool is useful to them, however, in that 25 to 50 percent of examinees will, under the tense psychological pressure of the exam, confess to the misdeed at hand. (Lykken, 1981, Lykken, 1991) Persuaded that they have been proven dishonest by “scientific” means they give up hope. It is usual for the polygraph examiner to interrogate the subject who has failed the test. They will state that there is no way now to deny the objective guilt demonstrated by this impartial and unbiased scientific device, and that the only available option is to confess.
The assessment by the polygrapher is genuinely convincing because, sadly, he believes it himself. Thus the instrument is clearly useful as a confession inducing device. One wonders, over the past 70 years, how many false confessions have been obtained in this way from innocent persons.
In summary, the polygraph is a ludicrous implementation of pseudo-science at its worst. The members of the APA are non-scientists practicing science, and the consequences are often dire. Lykken reports the cases of three men who were convicted of murder largely due to the polygraph examiner’s testimony that in their “expert opinion” they had failed the test. All three were subsequently found to be innocent. (Lykken, 1991) Polygraph examiners ignore such cases or rationalize that they are due to the rare incompetence of some examiners.
The continued use of polygraphic lie detection has the potential to cause much harm to those who are judged dishonest by its results. The specificity and sensitivity are not dissimilar to that of a coin toss. Innocent suspects have about a 50/50 chance. One failure is all it takes to ruin your life. Since the 1923 Federal Court decision of Frye vs United States (293 F 1013 [DC Cir 1923]), polygraph evidence has not been admissible in federal court cases because there was deemed a lack of scientific validity to the test. This travesty however is still used widely by the state court system. Furedy characterizes the continued use of polygraphy as a serious “social disease.” (Furedy, 1987) State laws regarding abuse of the polygraph must change, and it is time for the medical and scientific communities to educate lawmakers and policy makers about the true validity of this perversion of science. It must be forever banished to the same realm of parapsychology as the Ouija Board, phrenology, and palmistry. The relatively conservative American Medical Association’s Council on Scientific Affairs recommended that the polygraph not be used in pre-employment screening and security clearance. (Council on Scientific Affairs, 1986) It is time to extend this recommendation across the board, and put the greater than 3000 anachronistic polygraph examiners in the United States out of business.
Meanwhile, if you are asked to take a polygraph test–don’t do it. Those involved in the criminal justice system, including lawyers, are largely uneducated in the realm of scientific scrutiny and experimental methodology.
They may not separate science and pseudo-science, and erroneously believe that the polygraph is an accurate scientific instrument. Their interactions are with polygraph examiners who proselytize its use, and they have little or no interaction with scientists, psychologists, and physicians who refute its use. Refuse to take the test and educate them. Cite the Frye doctrine, go to the medical library, copy the scientific articles which belie its validity, and present them to whomever requested you to take the test. State that the principles and assumptions underlying polygraphy are not supported by our understanding of psychology, neurology, and physiology. Then put the burden of proof on their heads. Tell them to present you with scientific evidence that corroborates the validity of the test. There is simply no rational basis for a machine to detect liars.
References
Arther RO. 1986. The polygraph’s enemies: An update. Journal of Polygraph Science. 20: 133-136.
Barefoot J. 1974. The Polygraph Story. Cluett Peabody and Co., New York.
Barland, G, Raskin D. 1976. Validity and reliability of polygraph examinations of criminal suspects (Report 76-1, Contract 75 NI-99-0001).
Brett AS, Phillips M, Beary JF. 1986. Predictive power of the polygraph: Can the “lie detector” really detect liars? The Lancet. 1: 544-547.
Council on Scientific Affairs. 1986. Polygraph. Journal of the American Medical Association. 256: 1172-1175.
Furedy JJ. 1987. Evaluating polygraphy from a psychophysiological perspective: a specific-effects analysis. Pavlovian Journal of Biological Sciences.22: 145-151.
Horvath F. 1977. The effect of selected variables on interpretation of polygraph records. Journal of Applied Psychology. 62: 127-136.
Kleinmuntz B. 1987. The predictive power of the polygraph: The lies lie detectors tell. Journal of the American Medical Association. 257: 189-190.
Kleinmuntz B, Szucko J. 1984. A field study of the fallibility of polygraphic lie detection. Nature. 308: 449-450.
Lykken D. 1984. Polygraph Interrogation. Nature. 307: 681-684.
Lykken DT. 1981. A tremor in the blood: Uses and abuses of the lie detector. McGraw-Hill, New York.
Lykken DT. 1991. Why (some) Americans believe in the lie detector while others believe in the guilty knowledge test. Integrative Physiological and Behavioral Science. 26: 214-222.
Reid JE, Inbau FE. 1977. Truth and deception: The polygraph (“lie detector”) technique. Williams & Wilkins, Baltimore.
Saxe L. 1991. Science and the CQT polygraph: A theoretical critique. Integrative Physiological and Behavioral Science. 26: 223-231.
Saxe L, Dougherty D, Crosse T. 1983. Scientific validity of polygraph testing: a research review and evaluation. Conference: OTA-TM. U.S. Congress Office of Technology Assessment.
Steinbrook R. 1992. The polygraph test – A flawed diagnostic method. The New England Journal of Medicine. 327: 122-123.
“The incompetent or unprincipled physician, licensed to practice medicine by a too complaisant State, is the greatest menace to scientific medicine – as great a menace as all the cultists put together.” —Dr. Morris Fishbein (The Medical Follies. New York: Boni Liverlight, 1925 p. 71)
“There is no place in science for consensus or opinion, only evidence” —Claude Bernard
Sabin, Salk and the Classics in Medicine Library
Polio is nearly a thing of the past thanks to to Dr. Jonas Salk and Albert Sabin. In 1952 Salk discovered and developed the first successful vaccine for polio and combined with Albert Sabin’s 1961 oral vaccination the duo effectively obliterated the contagious polio virus. Once a deadly threat to our country and future there were 93,000 cases of polio reported in the U.S. Between 1952 and 1953 alone. But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
full body respirator or “iron lung” needed to treat patients whose respiratory muscles became paralyzed by polio
October 23, 2014 was the centenary of Jonas Salk’s birth and in honor of his 100th birthday I am sponsoring a contest to win framed autographs of both Jonas Salk and Albert Sabin as seen above. In addition, you will receive 100 volumes of the Classics in Medicine Library published by Gryphon Editions whose “mission is the preservation of the literary and intellectual heritage of the noble professions that we serve”
These are exact facsimiles of the original classics bound in leather and include works by William Osler, Harvey Cushing and Paul Dudley White.
Background
According to British sociologist G. V. Stimson the “impaired physician movement” is characterized by a “number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by involvement in medical society and treatment programs.” Their “authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
In this regard Dr. Wayne Gavryck, M.D. is a prototypical example.
An ex-alcoholic with a history of malpractice, Gavryck quit drinking through Alcoholics Anonymous, became “board certified” in “Addiction Medicine” and became involved with the Massachusetts PHP, Physician Health Services, Inc. (PHS) where he has been an Associate Director since 1988. He serves as their Medical Review Officer (MRO).
The “impaired physician movement” has gained tremendous sway through the American Society of Addiction Medicine and the Federation of State Physician Health Programs. The ASAM is not a valid medical specialty but a “special interest group” that represents the chronic relapsing brain disease with lifelong abstinence and 12-step recovery model of addiction and the companies that profit from it financially ( drug and alcohol testing labs, 12-step inpatient assessment and treatment centers) and politically (Drug War advocates, Anti -Medical Marijuana advocates). The impaired physician movement gained a seat at the table of power in medicine by bamboozling regulatory and administrative medicine. This illegitimate and irrational authority is in charge of almost every state PHP in the United States. ASAM physicians joined their state PHPs, gained power, and then removed those who did not agree with the groupthink and doublethink. Blind obedience and control are favored over fairness, truth and evidence-base. As with other states under the FSPHP, blindly obedient doctors are kept on while those who question the science and ethics of the groupthink are removed. The PHP-Drug Testing Laboratory and “PHP approved” assessment and treatment center industrial complex requires a Medical Review Officer of blind faith who places the goals of the FSPHP above all other considerations including the Hippocratic Oath. The system requires doctors who are willing to participate in “moral disengagement” of wrongdoing including professional, ethical and legal violations. To erect this scaffold they have put in place barriers to exposure and accountability. By declaring themselves “experts” they have used logical fallacy to temporize deflect and otherwise stifle accountability. With no oversight or regulation they are, in fact, accountable to no one. The appeal to authority and esoteric knowledge is an effective means of extinguishing valid concerns. Complacent that this is a group of benevolent organizational purpose those who should know better and could do something about it rationalize their apathy and indifference. A necessary step in exposing and addressing this problem is imposing accountability. If an organization is able to engage in conduct that is the antithesis of accepted professional guidelines and standards of care, in violation of professional and societal mores and codes-of-conduct and is illegal then there is a systemic problem. This problem can fortuitously be addressed by examining standards of care, conduct and criminal codes for breaches. If a breach is found then it needs to be explained and justified. One of the tactics of the FSPHP is to deflect criticism under the logical fallacy of appeal to authority. We are the experts. We know better. That is where it usually ends. But accountability requires both the provision of information and justification of actions. My hypothesis is that this group is committing fraud, violating ethics and flouting the law in an irrefutable manner. If this is not true then my hypothesis should be able to be refuted. It cannot. And for that reason I am putting my money where my mouth is.
Accountability
In all fairness, If Gavryck can justify his actions either procedurally, ethically or legally and back it up by any written protocol, guideline or standard then he wins and I will refrain from any more criticisms. In addition I will hand deliver to him the Salk and Sabin autographs and 100 volumes of the classics in medicine, apologize and remove this entire blog.
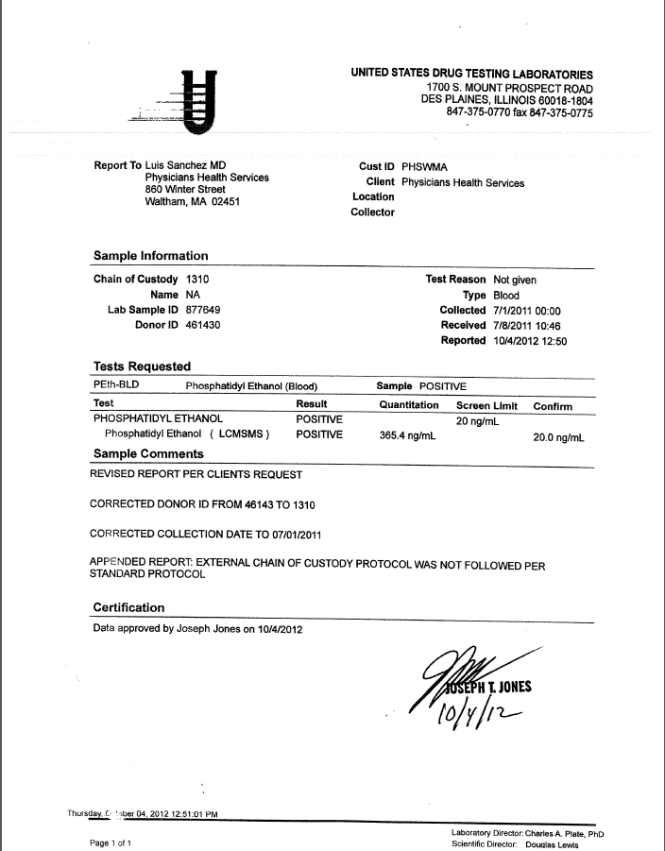
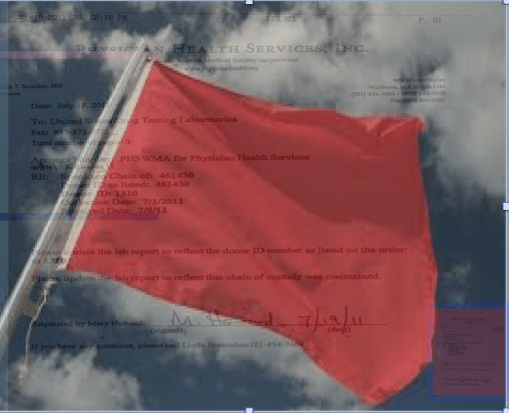
Accountability requires both the provision of information and justification of actions. One way of examining this is to look at the body professional and ethical standards and state and federal law. The FSPHP has blocked the provision of information regarding drug-testing. Although it has taken over three years I have obtained the all of the information pertaining to a July 1, 2011 test that should have immediately been rejected by the MRO. It is an invalid test.
Dr. Gavryck violated every conceivable procedural guideline and standard-of-care there is for an MRO, the Medical Review Officer Certification Council’s Codes of Ethical Conduct and both State and Federal Law. This can be ascertained by looking at the documentation. I have done this and found hundreds of documents that support the accusation that as an MRO Wayne Gavryck breached protocol, engaged in unethical behavior and broke the law. Prove me otherwise with just one credible source and the prizes are yours.
Contest Rules
Your job is to review the documentary evidence and records from PHS, Quest Diagnostics and USDTL and assess the actions and decisions made by the MRO.S)
If you can show that these decisions were the result of legitimate reasoning based on published guidelines or protocol, ethically defensible or did not break any laws and cite one credible source that concurs with this point of view then you have won.
If you can show that these decisions were the product of legitimate and thoughtful reasoning in accordance with established guideline, ethical codes then I will hand-deliver the items to you.
If you can justify, support or defend the actions of the Medical Review Officer (MRO):
Procedurally;
Ethically;
or Legally;
You win all of the prizes! Simple as that!
In fact, If you can support just one of these the entire lot is yours.
If you can show Dr. Gavryck did not breach any and all published Standards-of-Care and Professional Protocols and Guidelines regarding drugs-of-abuse testing, OR that he did not violate any and all Codes of Conduct and Ethical Guidelines of the Medical Profession from Hippocrates to the American Medical Association OR that he did not violate multiple State and Federal Laws you win Salk and Sabin autographs and all of the books.
All of the documents and details regarding the forensic fraud, concealment, coverup and deliberate misrepresentation to a state agency under color of law can be seen here:
To Review: Any and all drug testing requires chain-of-custody. “Forensic” drug testing differs from “clinical”drug testing because the consequences of a falsely positive test can be grave and far reaching. Because the results of a positive test can result in the loss of rights and liberties of the person taking the test it is essential that it be done correctly. False-positive tests are unacceptable so strict chain-of-custody procedure and MRO review assure specimen integrity. This provides accountability and the custody
The custody-and-control form records chain-of-custody and is given the status of a legal document as it has the ability to invalidate a test that lacks complete information. The job of the MRO is to invalidate specimens without intact chain-of-custody.
The MRO job is fairly simple. If a lab reports a positive test for any substance the MRO must check that the signatures, dates, times and other information on the custody-and-control form are correct and per protocol. Chain-of-custody must be accurate and complete. The MRO looks for “fatal flaws” on the chain-of-custody form. If a “fatal flaw is present then the test is invalidated and the test is not reported as “positive” but “invalid.”
The sole job of the MRO is to ensure that the drug testing process and chain-of-custody procedure is followed to the letter. The MRO reviews the Custody and Control form for accuracy and completeness. The MRO also rules out any other possible explanations for a positive test (such as legitimately prescribed medications). Only then is a test reported as positive.
“the sole responsibility of the MRO is to”ensure that his or her involvement in the review and interpretation of results is consistent with the regulations and will be forensically and scientifically supportable.”
Corruption is misuse of entrusted power. It occurs when those who have been given authority to carry out expected goals instead use their position and power to benefit themselves and others close to them. Abuse of power is particularly egregious when that person is doing the opposite of what he or she is supposed to do.
Accountability is necessary to prevent corruption and necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable.
Although Gavryck may serve PHS, it is not in the capacity of a certified medical review officer; by my count the documentary evidence alone shows that he violated four of the seven Medical Review Officer Certification Council Codes of Ethical Conduct. In addition to violating the MRO Ethical Conduct he violated every other code I can think of from the Hippocratic Oath to the AMA Code of Ethics. and everything in between.
As the MRO for PHS Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody of the sample was intact before reporting a test as positive.
This is indefensible on all levels (procedurally, ethically and legally). The documents show with clarity that this was not accident or oversight, but intentional and purposeful misconduct
There should be zero-tolerance for forensic fraud of this sort. Those of integrity and moral compass would agree. Transparency, regulation, and accountability are necessary. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Linda Bresnahan, much like Annie Dookhan, he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths. Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
Please help me get this exposed, corrected, and rectified. The physicians of Massachusetts deserve better than this.
Thank you for the Reblog–this is a topic the majority of practicing physicians are completely unaware of and we need to start the discussion, take a step back to see how we arrived here and hopefully address the errors made in judgment along the way.
Medicine is predicated on competence, good-faith, and integrity. Medical ethics necessitates beneficence, respect, and autonomy. The scaffold erected here is designed for coercion and control. Exposure, transparency, and accountability are urgent. An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements…
“The biggest problem Straight has is knowing how good it is.”–Dr. Robert Dupont, M.D., 1981
In 2012 former Nixon Drug Czar Robert Dupont, MD delivered the keynote speech at the Drug and Alcohol Testing Industry Association annual conference and described a “new paradigm” for addiction and substance abuse treatment. He advocated zero tolerance for alcohol and drug use that is enforced by monitoring with frequent random drug and alcohol tests. Detection of any substances is met with swift and certain consequences. He proposed expansion of this paradigm to other populations including workplace, healthcare, and schools.
Robert Dupont was a key figure in launching the “war on drugs” which is now widely viewed as a failure that has turned the US into the largest jailer in the world.
As the founding director of the National Institute on Drug Abuse (NIDA), he administered a 1.8 million dollar grant in 1972 to an experimental drug rehabilitation program in Florida called “The Seed,” that was later investigated by congress who noted the methods used by Seed were similar to those employed on American POW’s by North Korean Communists.
After leaving NIDA he became a paid consultant for a non-profit “family oriented treatment center, “Straight, Inc. praised by Dupont as the “best in the country.” …”the biggest problem Straight has is knowing how good it is. And I have taken it upon myself to do what I can to expand it nationally.” (Sarasota Herald-Tribune, Feb 9, 1981).
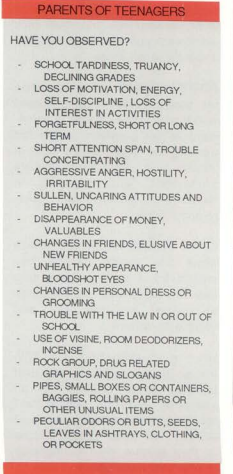
Straight did not treat addicts but “troubled teens,” mostly referred by concerned parents. When authorities closed Straight in Massachusetts they were cited for treating a 12 year old girl for drug addiction when Straight’s own record showed that the only drugs she had used was that she had once sniffed a magic marker! Straight, inc.., torture as treatment. and indoctrination that killed scores of kids by dehumanization, humiliation, and abuse leading to helplessness, hopelessness, and despair. These moral preening profiteers exploited parents fears to admit children to these inpatient boot-camp money trees. Propaganda, disinformation, junk science, and overt fraud as standard operating procedure. Dupont championed these programs as the paradigm of drug abuse treatment and used misinformation, junk science, and propaganda to promote them.
Straight executive Christopher Yarnold stated that “anybody that is using a drug that is mood-altering has a problem. Okay. He has a problem. From now until eternity he will be chemically dependent,” and must be treated with “holistic” care. Drug use in any form is harmful and requires treatment.
Once referred to these programs these children were subject to mental, psychological, and physical abuse and indoctrinated into 12-step prohibitionist dogma at the hands of unqualified zealots. The legacy of this program of coercion, control, 12-step indoctrination and abuse can be seen on this facebook page in memory of those who died.























 But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.