



Doctored Wechsler IQ–Boilerplate subtraction of subsets -diagnsosis = cognitive impairment
In May 1999, Dr. G. Douglas Talbott stepped down as president of the American Society of Addiction Medicine (ASAM) down as a jury awarded Dr. Leonard Masters a judgment of $1.3 million in actual damages and an undisclosed sum in punitive damages for malpractice, fraud, and false imprisonment. The fraud finding required that the errors in the diagnosis were intentional.
The lawsuit apparently resulted in some changes in the evaluation process. The errors were deemed intentional in the Masters case as the charts lacked sufficient data for the false diagnosis. Judging by what we see here they are generating intentionally erroneous tests to support an intentionally erroneous diagnosis.
In 2008 I went to Talbott Recovery Center in Atlanta for a 96-hour evaluation due to a positive urine test reported for a substance closely related to a medication I was prescribed. Despite obtaining a letter from the pharmaceutical manufacturer stating that the drug found in my urine was, in fact, the parent compound of the drug I was prescribed and despite a negative forensic fingernail test (done by USDTL) I was forced by Linda Bresnahan to have an “assessment.”
I arrived with 4500.00 which was about 500 dollars short for the evaluation. I had requested a forensic hair test and did not realize they were so expensive. The primary concern for most of the morning I arrived was when the remaining 500 dollars would arrive. In fact I was told that I would not be able to be admitted until I paid in full.
I had an appointment with an internist, Dr George MacNabb that he cancelled when he found out I had not yet paid in full. I have to admit that I, nor anybody I know at MGH, has refused care to a patient based on pre-payment.
The 96-hour assessment included the physical exam, neuropsychological and cognitive testing in addition to drug and alcohol testing by urine and hair. After finding out my hair test and toxicology screens were negative and in light of my supporting negative nail tests and letter from the pharmaceutical manufacturer I was pretty confident I was good to go but ended up wishing they would have told me the hair test didn’t count before I paid the extra cash.
At the completion of the 96-hour assessment I was brought to their conference room and told by Dr. Paul Earley and his his assessment team that I needed to stay for treatment. “I don’t understand,” I said..”I have negative hair (3 months) and nails (6 months), an explanation for the positive test and have never had any problems at work. I was then told that based on my neuropsychological and cognitive testing I was in denial and “cognitively impaired” and that they could not advocate for my safely practicing medicine.
I was then taken to accounting to see how I would come up with the 18-25K for treatment. On the last page of my assessment report it states that “Dr Langan agreed with this assessment and recommendations and requested to return home to collect his funds to return for treatment at the Talbott Recovery Campus.”
It is well documented that Talbott will “keep you until the money runs out.”
I had given them a list of people to contact who could verify my work performance was excellent and there were no concerns from anyone including nurses, patients and students. I asked why they had not contacted my Chief, nurse practitioner or any of my coworkers and was told they had enough information from the PHP Besides, one of them told me “they might cover for you so we can’t put much weight in their opinions.”
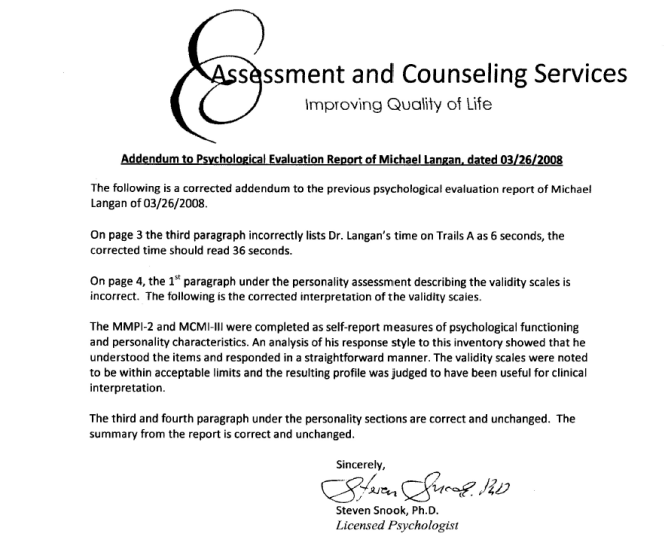
My first impression when I started reading the report was that it was another persons assessment given to me by mistake. The neuropsychology report indicating “denial” I knew was wrong as I recognized the language reporting an elevated L-scale. Thinking at the time it was an unintentional mistake I asked it be looked at as it was impossible. The L-scale or “Lie-scale” is a “validity” scale that picks up someone trying to portray himself in a positive light so you have to take the rest of the results with a grain of salt. It only works in unsophisticated naive individuals who answer blanket questions related to essentially good an bad behaviors or traits (such as “have you ever lied?”) believing that is what the audience is looking for. As a result, only people bereft of enough common sense to understand that concrete blanket statements are implausible.
Dr. Snook wrote an interpretation of my L-scale as if it were positive ( > 65). It was later confirmed to be 49 (as normal as normal can be on this) after obtaining the scoring sheet and raw data but even confronted with this he refused to correct it and only did so after the Georgia Psychological Association forced him to. He engaged in intentional fraud at the request of PHS to show pathology where there is none and in terms of medical ethics there should be zero tolerance for this. Zero! Political abuse of psychiatry to give a false diagnosis for economic or political gain is antithetical to both medical and societal ethics. It is unconscionable in light of all of the doctors who have killed themselves after being evaluated by these programs.
And although I can’t prove it, the IQ test above was also doctored as I have taken it before and “comprehension” was my best score. The computer shaves off points to lower comprehension and reasoning subscales and they give a diagnosis of “cognitive impairment.” I subsequently took it in Boston two weeks later and went back up again! I wonder what happened in Atlanta? I could not disprove this one however as there is no raw data generated to prove whether I incorrectly interpreted a proverb or couldn’t tell him what I would do if I found a stamped envelope on the street.
Neuropsychological Misconduct –Making the Data fit the Diagnosis Part 1: Denial
“To further complicate matters, many evaluation/treatment centers are dependent on state PHP referrals for their financial viability. Because of this if, in its referral of a physician, the PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnoses and recommendations in a way that will support the PHP’s impression of the physician.” -John Knight and J. Wesley Boyd. in “Ethical and Managerial Considerations Regarding State Physician Health Programs,” Journal of Addiction Medicine 2012

Dr. Stephen Snook, PhD
Confirmatory Distortion
“Confirmatory distortion” is the process by which an evaluator, motivated by the desire to bolster a favored hypothesis, intentionally engages in selective reporting or skewed interpretations of data thereby producing a distorted picture. It is an “indisputable conscious endeavor to find and report information that is supportive of one’s favored hypothesis.10
In other words it is a conscious decision and not an unconscious bias..
I requested Talbot and Dr. Snook address the fraud and rewrite the interpretation and recommendations. I then complained to PHS not knowing at the time that they were the ones who requested it. The requests were ignored.
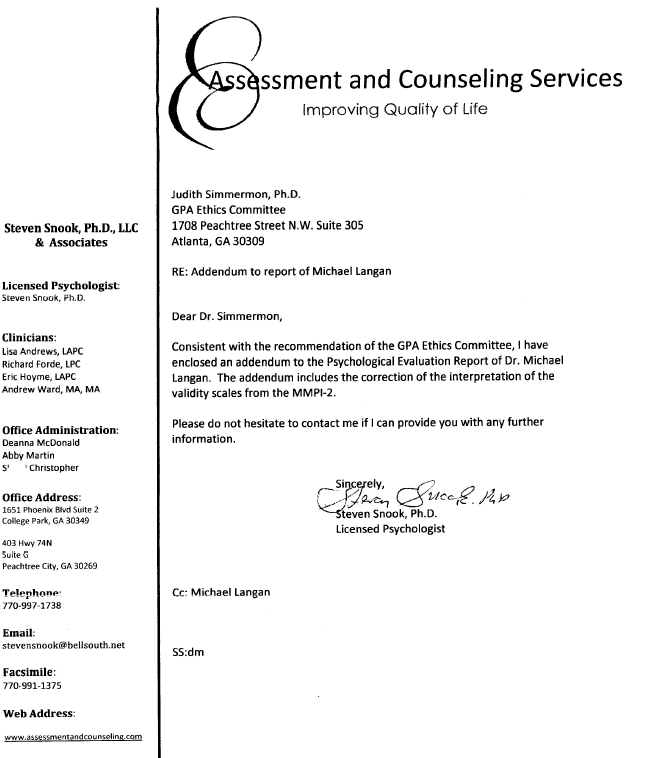
I then filed a complaint with the Georgia Psychological Association. They confirmed the fraud and forced Dr. Snook to correct the test. Below is his apology. An apology received only because his back was to the wall. “Profound apologies”–Give me a break. There would not be one if the Georgia Psychological Association did not force him to.
I have since spoken to a couple dozen doctors who have the same template on their evaluations. An elevated L-scale would be unusual in any doctor even if he were an alcoholic or addict. It is only the very naïve and unsophisticated who would think they can show themselves in a positive light by answering questions of obvious attempt such as “I never lie.” And if a class action lawsuit comes about this is one of the items that could be used to prove the systemic fraud. Obtain the score sheets from the facilities on anyone with this same interpretation and it will most likely show fabrication in the same manner.
Next up is the cognitive impairment piece. Just like the MMPI they manipulate the IQ tests to show cognitive impairment by shaving off points in the executive function subcategories.
Snook is one cog in this system of fraud. He and others like him should have their licenses revoked permanently. There is no excuse. How many careers have ended because of his contribution to this scam? How many have died?
As always with my posts, if he cares to contest it and can disprove the fraud I’ll take the post down. As with all the others they can’t. If they could’ve they would’ve.
And this is the reason I was targeted by Linda Bresnahan. Upset that I got one of their own in trouble she threatened retribution. “You won’t be a doctor in five years” she said. “Dead, relapsed or in jail I don’t care.” “Dead?” I said.
“Either that or you’ll wish you were”. And when Drs. John Knight and J. Wesley Boyd were removed from PHS and were no longer there to protect me she made good on her threat. She and Luis Sanchez fabricated an alcohol test in retribution for calling out one of their own.








 This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.
This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.




