Below images link to podcast.




Below images link to podcast.

Physician Health Programs (PHPs) now targeting medical students–More sheep for the slaughter
The attached article entitled “Medical school drug testing is a moral and scientific failure” opposes testing medical students for drugs and alcohol but things are going to get a whole lot worse.
In the past six-months I have been contacted by an increasing number of medical students searching for help after being trapped in quagmire of their state physician health program (PHP). Each of them had either been referred to a “PHP-approved” assessment center or had already had an evaluation recommending inpatient treatment.
Some of these students were subjected to non-FDA approved laboratory developed tests including hair testing for marijuana metabolites and the alcohol biomarker EtG. These typeof tests can detect substances that were used days, weeks and even months prior to testing.
Medical students and physicians are just as likely to have experimented with illicit substances in their lifetimes as their age and gender matched peers.1
Although medical students as a group drink slightly more alcohol than the general population, the pattern and prevalence of alcohol, dependence is consistent with their age mates in the general population.1 2
Like it or not recreational and experimental drug use is widespread in young adults and most of them “grow out of it” and the 21st Amendment repealed the Volstead Act in 1933. Alcohol is legal and those that can handle it have a right to a round of beers after a long day or imbibe a cocktail with a dinner date. But according to the prohibitionist profiteers and moral preeners any drug or alcohol use is a sign of “potentially impairing illness” that must be addressed and treated early to prevent an inexorable slide into a chronic relapsing brain disease and abstinence and lifelong adherence to the principles 12-step spirituality are the only way to do so.
An old joke asks “How does a doctor define an alcoholic?” Answer–“anybody who drinks more than he does.” How does a PHP define an alcoholic? Answer –anybody who walks through the front door.
In reality, a zero-tolerance paradigm utilizing this type of testing would be ruinous. With recreational and experimental drug use common in young adults a profession that refuses to accept anyone who tests positive for drugs will exclude large numbers of brilliant, talented individuals. Dismissing highly talented people in medicine for what might be a one-off recreational non problematic drug experience would retard its advance.
The use of these non-FDA approved tests of unknown validity should not be allowed to begin with but there needs to be a concerted direct attack on their use on medical students or the brain-drain on the profession will bring it back to the dark ages. The ASAM White Paper on Drug Testing proposes imposing this system with mandatory drug testing by the healthcare system from childhood to old age. College loans are proposed as “leverage” for college students in this “contingency management” paradigm so a lot of promising students could be weeded out before even applying to medical school. Forget GPA and MCATS as the primary criteria for medical school admission will be sobriety and clean urine screens..
Diagnosing disease without meeting the diagnostic criteria for that disease.
None of the students who contacted me seemed to fit the diagnostic criteria for the diagnosis given to them stories which were articulate, detailed and sincere. All cases involved either a naive mistake or isolated incident.
One student made the disastrous revelation to a PHP director who had just given a class lecture that she had smoked marijuana with her high school friends in her home state of Colorado. She was then called in by the PHP and referred for an evaluation at an out of state facility where she was diagnosed with “marijuana dependence” based on a positive low level THC metabolite on a hair follicle test. She was told she was in denial and inpatient treatment was recommended. Although she admitted to occasional weekend marijuana use there were absolutely no problems in any realm of her life. It is self-evident that impairment due to drugs or alcohol impacting someones capacity to work or function needs to be addressed but the penalty imposed on her for her private behavior was to end her career in medicine before it even started. The medical school administration mandated she either complete the treatment required by the PHP or she would not be able to enroll the following semester and not being able to come up with the up-front out-of-pocket cost for treatment she was not able to return to the medical school and has decided to pursue a different career.
Another student was anonymously reported to the PHP for smoking marijuana at a weekend party which resulted in a similar assessment and recommendation for inpatient treatment. After spending 3 months at a facility in Alabama he is now under monitoring contract with his PHP but returned to school.
Healthy student asks for help in his organizational skills–ends up with a psychiatric and substance abuse diagnosis
After reading an advertisement in the state medical society newsletter promoting work-life balance a second-year medical student contacted his state PHP to obtain advice on his problem with “procrastination.” Classes and working part time in the endocrinology lab left him with little time and he found himself slacking off on his exercise routine and burning the midnight oil before test nights. He told the PHP director about his history of depression after his father died immediately before his freshman year at college. That October he became overwhelmed with sadness and missed his dad and hometown. He sought help from the campus physician who prescribed prozac which was discontinued in a years time without return of any symptoms.
Realizing there were no classes in work-life balance but only a support group for “burnout” the student declined the PHP directors offer of an assessment of his “mental health.” Much to his surprise he was called in the following week by a medical school administrator and told that the PHP was requiring an assessment at one of two out of state “PHP-approved” assessment centers in Lawrence Kansas. He was at first confused at the nonsense he was hearing and then became indignant at the nonsensical and illogical request without rhyme or reason and the betrayal of trust and ethics. “Surely this must be a HIPPA violation.” He obtained an outside consultation from a psychiatrist and contacted the campus physician who confirmed his diagnosis was acute situational depression and bereavement but the PHP disregarded the information. He bartered for a local evaluation but this was refused. He arranged for the 96-hour assessment in Kansas. His mother paid the requisite out-of-pocket up-front $4,500.00 to the facility and she told him not to worry as his life would get back to normal after they confirmed he had no psychological problems. “Dysthymia, Major depressive disorder, severe, in remission and alcohol use disorder” were given as diagnoses. “Alcohol use disorder” was based on a hair test for EtG which was the result of his drinking an occasional beer or two with friends after school and on the weekends. He was told he may be “self-medicating” and playing “Russian roulette” given his history of depression. Recommendations included inpatient treatment followed by a “structured aftercare program” of abstinence and monitoring by for alcohol and drugs of abuse. Forced to sign a contract with the PHP he was understandably upset at the serious and unfounded sequelae that was the result of asking for help.
Another fourth-year student got into a bit of a shoving match with his buddy at the bar on a Saturday night and was reported to his PHP anonymously. He is awaiting evaluation.
This brings up another potential problem–sham peer review. As PHPs accept anonymous referrals what is in place to prevent inappropriate referrals based on removing a competitor and improving your academic standing.
A legitimately prescribed stimulant for ADHD bought a third year student into a PHP contract. He was forced to discontinue the medication prescribed by a psychiatrist specializing in childhood ADHD by a family practitioner in “recovery” from abusing intravenous fentanyl who had been monitored by the PHP himself for ten years then became medical director after getting board certified as an addiction medicine specialist.
This student got 99th percentile across the Board on his MCATs and may one day cure cancer but now faces an uncertain future as he recently got a positive EtG on a urine test and they are currently “sorting this out.”
The most bizarre story was from a student who sought help for sleep troubles after reading about the PHP as a referral source. He subsequently saw a sleep-specialist and was diagnosed with an oversized uvula which was surgically corrected. His sleep troubles improved but his troubles with the PHP remained. A triathlete and excellent student the PHP determined he had a “thought disorder” and discussions of “schizophrenia” were entertained by the PHP and they recommended an out of state evaluation at one of the three gulags used by the FSPHP for “disruptive physician” and behavioral exams–Vanderbilt, Acumen and the Professional Renewal Center. All of these facilities come with a guaranteed diagnosis. Polygraphs and unvalidated neuropsychological instruments designed to detect “character defects” cast a pretty wide net.
Question FSPHP with direct questions to undermine a “culture of professionalism.
It is important that medical school administrators refuse to engage in blind deference to the authority of the state PHP. Authority must always be questioned and to not do so is irresponsible. Unquestioning allegiance to an authority does not comport with the history of the medical profession or science. Faith in institutions demands mass adherence to faith in that authority and direct challenges to the status quo are needed to undermine that faith. They have bamboozled the medical boards into implementing bad policy, approving bad science and making bad decisions. They have duped state legal authorities into deference to their expertise and integrity under the notion that questioning these attributes undermines a culture of professionalism. Fact of the matter is they have no expertise, no integrity and no professionalism.
PHPs have been contaminated with an outside influence and support an agenda that has nothing to do with protecting the public or helping medical students. They are an illegitimate authority that has become an irrational authority and their recommendations mandate direct answers and justification.
If the PHP has concerns about a student then the first step should be to obtain an independent second opinion. PHPs discourage second these second opinions and disregard all outside expert opinion no matter how well qualified and experienced that expert is. Anyone outside this brood of addiction addicts is scoffed at as biased or unenlightened to the simplistic belief system with which they have contaminated the medical profession. Look into the assessment centers to which they are mandating referral. Ask what qualitative factors and quantitative measurements were used to approve that facility and why no one in Massachusetts has the ability come to a competent diagnosis. The yarn that doctors and medical student have an ability to dissemble and appear normal while harboring a “potentially impairing condition” is one of the medical urban legends they started. Ask to see the evidence base. There is none and it defies common sense, logic and science.
An increasingly bright light is being shed towards the malfunctions and corrupt practices of this unaccountable confederacy of “authorities” and at some point soon their jig will inevitably be up. In the interim, if you are referred to a PHP it would be a good idea obtain independent lab tests and two second opinions. Although the PHP will disregard this documentation it would be wise to obtain it to prove both your normality and the discrepancy between your independent evaluation results and the cherry-picked pulled out of a hat multiple diagnoses confabulated and misrepresented by the PHP.

Medical school drug testing is a moral and scientific failure
ANONYMOUS | EDUCATION | MAY 11, 2014
Before the 1980s, drug testing was uncommon. It was widely viewed as an invasion of privacy and an infringement on fourth amendment rights. Today, a medical student is likely to be drug tested before entering medical school, before clinical rotations, and/or before residency. If preventing drug use among medical students is the goal of these tests, they have failed miserably. Urinalysis drug tests are ineffective. But more importantly, they are immoral.
Drug tests are ineffective for two reasons. First, they basically just test for marijuana. A 10 panel urinalysis technically tests for 10 different drugs, but marijuana is one of the only drugs that can be detected for more than 30 days. Cocaine can be detected for 4 days. Amphetamine, methamphetamine, ecstasy, heroin, and codeine all can be detected in urine for only 2 days. This means that a user of drugs far more dangerous than marijuana needs to abstain for just a couple of days. Psilocybin mushrooms, as well as several other mind-altering drugs, are not tested for at all.
For a marijuana user, a drug test might seem like a nightmare. But here we arrive at the second reason why drug tests are ineffective, they are easily beaten. A marijuana user may choose to drink a lot of water before his drug test to dilute his urine. Alternatively, he may choose to use a friend’s urine who he knows does not use marijuana. Either one of these options might work. But fortunately for such a marijuana user, there is another option that is essentially risk free, synthetic urine. There are several companies that make synthetic urine capable of beating drug tests. The word on the Internet is that Quick Fix is a safe bet. I personally know some people who would agree. At just $30 for a bottle, it looks like the drug test is no match for the free market.
Do not just take my word for it though. In 2003, the University of Michigan conducted a study on the effectiveness of drug testing students. From nearly 900 schools, the study found that drug testing, whether routine, random, or based on suspicion, had no measurable effect on drug use among students. Put simply, drug testing accomplishes nothing.
The most important concern I have about drug testing medical students is a moral one. Regardless of their effectiveness, or ineffectiveness, the endgame of drug testing is to prevent drug users from becoming doctors. Users, not addicts; and there is a big difference. A marijuana user might use on weekends or at night to relax, much like an alcohol user. A marijuana addict, although rare, is the type of person who might show up to important occasions intoxicated. The statistics on marijuana addiction vary. They usually show that less than 10% of users become addicts, but they always show that alcohol users have higher rates of addiction. A urinalysis detects alcohol for no more than 12 hours after use. This means that medical students who use alcohol are more likely to be addicted, and they face basically no risk of failing a drug test.
Should we be worried about medical students being drunk in clinical settings? Of course. And we should also be worried about medical students being high in clinical settings. Intoxication could be disastrous and it needs to be prevented. The good news is that this is done naturally. It is highly unlikely to find medical students who are addicts of marijuana, alcohol, or any mind-altering drug. I believe it is safe to say that the rigor of medical school itself prevents drug addicts from becoming doctors. There are, however, drug users who will make it into medical school or other rigorous scientific careers. Actually, many of them thrive. Richard Feynman, Kary Mullis, and Francis Crick used marijuana and LSD, Carl Sagan used marijuana, and Oliver Sacks used several illicit drugs. When drug tests are required for every medical student, the casual drug user, no matter how much potential he has, is bullied for no reason. The potentially dangerous drug addict has already been weeded out long ago.
Medical school is supposed to be based on science. The science shows that drug testing does not work. If it did work, then many great scientists would have been removed from their professions. These facts alone should be enough to settle the issue, but it is important to look at two more moral objections we should all have.
First, drug tests are not free. Before entering medical school, I paid about $30 for one. This does not sound like much. But charging students even one penny is unacceptable, for there is not even a fraction of a penny in benefit from these tests. The nearest drug testing facility for me was a 20 minute drive from my house. I could have driven anywhere for 20 minutes and just handed $30 to any random person. Surely, that $30 would bring more value to society than $30 wasted on a drug test. Imagine if a police officer searched a person’s car for drugs against his will, found none, and then charged this person $30. That is the reality of drug testing.
Second, drug tests are an invasion of privacy. Medical students should not be forced to prove their innocence. This creates a guilty until proven innocent environment. It immediately creates resentment among students, and rightfully so. Furthermore, what about people with paruresis? The International Paruresis Association estimates that 7% of people suffer from this condition, also known as shy bladder. Type “paruresis drug test” into a search engine and spend some time reading through the horror stories that are shared. These people suffer from a medical condition, and of all places, their medical school is completely inconsiderate.
Drug testing is a moral and scientific failure. Medical schools should be too embarrassed to take part in such nonsense.
The author is an anonymous medical student who blogs at unchainedmedical.
TAGGED AS: MEDICAL SCHOOL


Are Physician Health Programs (PHPs) above the law?
Unable to get law enforcement to take cognizance of reported abuse, many doctors I have spoken with believe that the actors involved are impervious to criminal liability. Complaints of fabrication and fraud involving PHPs and their affiliates to the police, the Attorney General and other law enforcement agencies have been given no credence, tabled or dismissed with little investigation.
Believing these agencies are deliberately ignoring credible complaints and the documentary evidence placed before them, some have concluded that state PHPs have been given the power to commit crimes with impunity and immunity.
PHPs are not above the law. It is by removing themselves from and blocking the usual routes of accountability and absolute operational control of the testing, assessment and treatment process that has enabled misconduct to remain hidden, unrecognized or excused. The crimes exist but they remain undetected, unnoticed and unpunished.
Removing Accountability
The essence of accountability is answerability which means having the obligation to answer questions regarding decisions and actions. This requires the transmission of information when it is requested. The accountable actor provides the information to the overseeing actors in a transparent manner.
Accountability also requires explanation and justification for the information provided. What was done and why? Standards, rules, regulations, codes, laws and other benchmarks are then applied by the overseeing actor to determine if the information provided was appropriate or inappropriate.
The availability and application of sanctions for illegal or inappropriate actions uncovered through answerability is also a necessary component of accountability. This is necessary to impose restraint on authority and power. Lack of enforcement of sanctions contribute to the creation of a culture of impunity.
The usual mechanisms that exist to impose restraint and create incentives for appropriate behavior and actions are absent. No outside oversight exists to limit their power or subject them to a set of rules. No regulation exists to curb abuse.
A Culture of Impunity
The authority accorded PHPs and the power they exercise exist in a culture of impunity.
The key findings of the2014 North Carolina PHP Audit are below:.
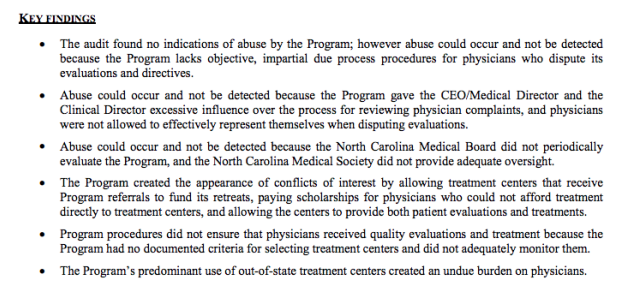
No indications of abuse were found, a point brandished by the PHP as redeeming and proving no abuse was occurring. In actual fact it is an ominous finding that also relates to their apparent ability to violate the law.
The audit found no indications of abuse but that abuse could occur and not be detected because of an absence of due process for the complainant, excessive control of the complaint process by the PHP and absence of oversight by either the medical board or medical society. What this means is that a doctor with no power is making a complaint against an unsupervised agency with enough power to influence the investigation of a complaint against itself. The reason no indications of abuse were found is because the system is specifically designed to hide abuse. That is the intent.
Absence of transparency, regulation and oversight coupled with control of information enables both censorship and doctoring of records. Strict Confidentiality is enforced by HIPAA, peer review protection, and drug and alcohol confidentiality law.
PHPs are able to suppress and conceal criminal activity but they are also able to manufacture information designed to hide misconduct.
The North Carolina Audit found no objective selection criteria for the out of state assessment and treatment centers because none exist other than ideological mindset and monetary gain. The same facilities are used by most state PHPS. They are, in fact, mandated as they are the “PHP-preferred” facilities.
In 2011 The American Society of Addiction Medicine (ASAM) issued a public policy statement on coordination between PHPs, regulatory agencies, and treatment providers. recommending only “PHP-approved” treatment centers be used and the statement specifically excludes ‘non-PHP” recognized facilities.
What the Audit diid not discover is the medical directors of all of the “PHP-approved” facilities can all be seen on this list of Like-Minded Docs. It is a rigged game Every aspect of drug-testing, assessment and treatment is kept hidden and secret and within control of the PHP.
It is a rigged game in which they have removed themselves from all aspects of accountability. They have, in effect, manufactured a culture of impunity at our expense.
“PHP-Approved Attorneys”
My survey has revealed an additional factor stacking the deck and removing accountability from PHPs. The attorneys ostensibly representing doctors are also part of the racket.
A doctor referred to a PHP will be given a list of 3 or 4 attorneys by the PHP who are “experienced in working with the medical board.” What they do not tell you is that theses attorneys are hand-picked or cultivated to abide by the rules dictated by the PHP.
They will not “bite the hand that feeds” and any procedural, ethical or criminal misconduct by the PHP will not be addressed. Laboratory fraud, false diagnoses, and Establishment Clause violations are off limits.
The primary purpose of these attorneys is to enforce payment for laboratory fees and demand compliance with whatever the PHP demands. Their primary purpose is to keep doctors powerless under the PHP and prevent misconduct, including crimes, from being discovered.
The attorney pool is currently over-served by those serving two clients and most of those outside simply do not know enough about the “physician health” legal issues related to doctors. Most of those involved in representing physicians before medical boards in these matters are former board attorneys or assistant AGOs. When those outside this cloister appear before medical boards they are like a deer in the headlights. It is a new terrain where all due process and familiar protocol have been removed. Truth and evidence are irrelevant as labyrinthine administrative procedure and protocol are used to trump all other consideration. Of course this was all facilitated by changes in administrative and medical practice acts orchestrated by the physician health movement “in the interests of protecting the public. This must be recognized and addressed. Skilled negotiators and lawyers with administrative law experience would do well to consider representation for doctors before medical boards regarding “physician health” matters. The current pool is glutted with those who will not “bite-the-hand-that feeds.” They depend on referrals from state physician health programs for their livelihood and this precludes going against the tide.

 “In the small world of drug testing, these four—Angarola, Bensinger, DuPont and Willette—are affectionately referred to as the Gang of Four. Dr. John Morgan explains, “They are the ones responsible for a good deal of drug testing’s success, and some of the fear that goes along with it. Remember these names. These men are among the most competent and knowledgeable about drug testing—scientifically and politically. They are well-informed: they have to be. Their livelihoods depend upon their credibility. Unfortunately their expertise represents the greatest threat to the civil liberties we seek to protect. Know your enemy.” 1
“In the small world of drug testing, these four—Angarola, Bensinger, DuPont and Willette—are affectionately referred to as the Gang of Four. Dr. John Morgan explains, “They are the ones responsible for a good deal of drug testing’s success, and some of the fear that goes along with it. Remember these names. These men are among the most competent and knowledgeable about drug testing—scientifically and politically. They are well-informed: they have to be. Their livelihoods depend upon their credibility. Unfortunately their expertise represents the greatest threat to the civil liberties we seek to protect. Know your enemy.” 1
Steal This Urine Test – Fighting Drug Hysteria In America – By Abbie Hoffman with Jonathan Silvers. 1986
A recent Huffington Post article written by Maia Szalavitz, The Rehab Industry Needs to Clean Up Its Act Here’s How, describes the need to radically rethink and reform American addiction treatment.. The article quotes Dr. Mark Willenbring who states
“What we simply need is a nice bulldozer, so that we could level the entire industry and start from scratch.”
Agreed, but the chances of this are slim to none if the “PHP-blueprint” becomes the “New Paradigm.” To prevent this from happening it is critical to disprove the claims, recognize the threat, and address the matter directly and collectively. We need political and social activism in the same spirit as Abbie Hoffman whose words from three decades ago are aptly accurate. His prescient warnings remain unknown, forgotten, or irrelevant to us today but their accuracy is crystal clear. Few people know the enemy.
 On April 23, 2015 Dr. Robert Dupont, MD addressed the House Subcommittee on Oversight and Investigations Combatting the Opioid Abuse Epidemic and proposed widespread application of a “New Paradigm” for substance abuse management based on the nation’s physician health program (PHP) model of care.
On April 23, 2015 Dr. Robert Dupont, MD addressed the House Subcommittee on Oversight and Investigations Combatting the Opioid Abuse Epidemic and proposed widespread application of a “New Paradigm” for substance abuse management based on the nation’s physician health program (PHP) model of care.
This model is being brandished as “gold standard for addiction treatment” to the drug and alcohol rehabilitation community and general public. The medical literature contains numerous articles claiming the high success rate of these programs4,6,9,10 and they are being promoted to set the “ standard for recovery” as a replicable model to be used for treating “other addicted populations.”11 In his speech before the House Subcommittee Dupont states critics call the expansion “utopian” but many would beg to differ. “Dystopian” would be more like it.
There has been an increasing scrutiny of these programs recently not yet covered by mainstream media. The link between the marked increase in physician suicide (which is much more than the oft quoted medical school class of 400 per year is directly related to the FSPHP takeover of PHPs). A recent Medscape article describes the coercion, control, secrecy and conflicts-of-interest between the PHPs and their “PHP-approved” assessment and treatment centers. The simple fact is the majority of doctors referred to these programs do not have a substance use disorder or psychiatric problem but are given one nevertheless. This removes their locus of control and puts the PHP in complete power. Their fate is in the hands of the PHP.
The assessment and treatment facilities used by PHPs do not take insurance and require payment up front. It is all out of pocket because if insurance was involved the fraud would have been discovered long ago. The PHPs have no accountability. There is no oversight by medical boards or medical societies and answerability and justification for actions are absent. And as we are hearing the rehabilitation industry itself is unregulated. So too are the junk-science lab tests used in PHP programs as these non-FDA lab tests and the corrupt labs that use them have no oversight form the FDA or any other agency able to hold them to account. It is a free for all.
Those ensnared in this web do know the enemy but can do nothing about it. I am hearing story after story of doctors seeking help from their medical societies, law enforcement, the media and the ACLU only to be turned away.
Their stories are remarkably similar An increasing number of complaints involving PHPs and the preferred assessment and treatment centers and contracted commercial labs are being reported. A recent lawsuit filed by a doctor against the North Carolina PHP and Medical Board reported on Medscape last week is a prototypical case. The scenario typically goes like this: An accusation is made against a doctor who has had no previous disciplinary history or concerns (alcohol on breath, throwing a surgical instrument) and referred to the state PHP; An assessment is recommended by the PHP at an out-of-state “PHP-approved” assessment and treatment center; the assessment confirms a psychiatric problem or substance use disorder and recommends typically three-months of inpatient treatment followed by a 5-year contract with the state PHP for monitoring. It is becoming clear that doctors who do not fit the diagnostic criteria for a disease are being diagnosed with a disease. There are also complaints of laboratory misconduct and forensic fraud.
It is important to recognize that State PHP programs require strict adherence to 12-step doctrine11 and limit assessments to not only ASAM facilities but to a specific constellation of 12-step assessment and treatment centers with medical directors who belong to a group called like-minded docs. It is in fact a “rigged game.”
In “Six lessons from state physician health programs to promote long-term recovery” Dupont and Dr. Greg Skipper attribute this success rate to the following factors:12
(1) Zero tolerance for any use of alcohol and other drugs;
(2) Thorough evaluation and patient-focused care;
(3) Prolonged, frequent random testing for both alcohol and other drugs;
(4) Effective use of leverage;
(5) Defining and managing relapses; and
(6) The goal of lifelong recovery rooted in the 12-Step fellowships.12
In truth the sole basis for these claims is a single retrospective cohort study of 904 physicians monitored by 16 state PHPs initially published in the British Medical Journal in 2008.2 In 2009 the same study was published in the Journal of Substance Abuse Treatment3 and deemed the “PHP-blueprint. Methodologically flawed and rife with conflicts-of-interest this study is the sole foundation of all of the claims. Of the 904 participants 102 were “lost to follow up” and of the remaining 802, 155 failed to complete the contract but despite the small numbers this study has been hashed and rehashed to brandish the claims of an 80% success rate physician including subsets of psychiatrists,4 surgeons5 and anesthesiologists6 In his address to the House Subcommittee Dupont, who is a co-author on every one of these papers, claims similar success in a subgroup of opioid addicted doctors.
None of this has been subjected to normal scientific peer-review procedures and represents a serious departure from the normal standards of scientific inquiry
The same forces that have created and sustained the current monopoly of 12-step oriented treatment in America have grand plans through links forged though government, private agencies and the drug and alcohol testing assessment and treatment industry.
Through a combination of large-scale funding, rhetorical persuasion and moral panics they have gained both tremendous sway and power in the profession of medicine and the collateral damage they have caused is widespread and permanent. They are poised to do the same to others using the same methods and the procedural protections afforded to those currently being tested for substances of abuse in Federal Workplace Drug Testing programs will be removed without your consent or knowledge. I recently heard from someone that these groups are lobbying the Nuclear Regulatory Commission into accepting this model with some resistance.
As far-fetched as all of this sounds all one has to do is look. The greatest threat to the civil liberties we seek to protect is no longer a threat but a reality.
Examine the documents below and connect the dots to see the coming Trojan horse for systemic application of a flawed substance abuse management program with no evidence base.
Medicalization of 12-step will be accomplished when “addiction medicine” becomes recognized as a bona-fide medical specialty by the American Board of Medical Specialties.(ABMS) which is slated to occur within the next couple years. At that point this group will deem 12-step ideology as best practice “evidence-based” doctor recommended care. This will “sanctify” the ideology as medical “standard of care” and can then be imposed on anyone with impunity and immunity. Medicalization subverts the Establishment clause of the 1st Amendment and the propaganda supporting this has already begun. See the 12-step “facilitation” piece below giving the reasoning they will use. This is not facilitation but coercion.
The ASAM White Paper on Drug Testing promotes random testing of everyone using the Non-FDA approved tests of unknown validity currently used in state physician health programs. This will be implemented through the healthcare system by removing procedural protections currently in place under federal guidelines. This is sure to be a boon for anyone battening and fattening off the Drug and Alcohol Testing Industry Association or rehab racket gravy train but a burden and pain for the rest of us.
The conflicts of interest are unfathomable.
Dupont and fellow “Gang of Four” member Peter Bensinger (DEA chief, 1976–1981) run a corporate drug-testing business. Their employee-assistance company, Bensinger, DuPont & Associates is the sixth largest in the nation and managing drug testing for some 10 million Americans including Kraft Foods, the FAA and even the Justice Department. They sell drug-testing management programs. The “New Paradigm” is simply a ruse to get non-FDA approved testing into the wider workplace via loopholes and workarounds. His ties to the drug and alcohol testing and treatment industry are easy to find. Drug testing is a multi-billion-dollar-a-year industry. DATIA [Drug & Alcohol Testing Industry Association] represents more than 1,200 companies and employs a DC-based lobbying firm, Washington Policy. Many of the non-FDA approved tests they are using in the “PHP-blueprint” they in fact introduced to the market themselves with no evidence base. It is reprehensible.
And the people who will suffer most in the “New Paradigm” will be those who are already marginal in American society. That’s a given. I have heard from doctors who are gay or belong to a minority group who claim they were referred to a PHP due to discrimination but had no recourse.
Medicalization of behavior removes due process as the victimized are simply put in a labeled group and via actuarial logic that safely that removes the underlying prejudice from view by categorization of risk. Discrimination is justified and rationalized. So read the documents below and connect the dots. Then do something about it. Say something. Write something. Do something. The Emperor has no clothes and this needs to be exposed. Either defend what you read below or protest this New Inquisition. We need revolt and Revolution. The Federation Of State Physician Health Programs (FSPHP) regime is simply another front-group designed to force the medical profession in line for the profits of the rehab racket. The FSPHP is the enemy and State PHPs need to be reformed and repaired with transparency and accountability. And to accomplish this the entire long running mess needs to be bulldozed and rebuilt from scratch.


Please donate here: https://www.gofundme.com/PHPReform
There is a very urgent need for a “counterpower” to state physician health programs (PHPs). On average five or six medical students, doctors or residents contact me each week and I want to continue to help them and work toward advocacy and watchdog groups. Unfortunately I am losing ground quickly. We have made tremendous advances in the last year and I am working in many different venues to expose the problems written about here. Those involved in this corrupt system are hoping that I will run out of resources and simply go away and have done everything they can to accomplish this. Without your help this will occur and it will unfortunately occur soon.

The Medscape article Physician Health Programs- More Harm Than Good? by Pauline Anderson shed some light on coercive, controlling secretive lair of Physician Health Programs. Coercive v. supportive is the question Alissa Katz presents in todays Emergency Medicine News. Supporting coercion, John Knight and J. Wesley Boyd claim that any doctor caught in the maw of their state PHP must abide by whatever the PHP requests in order to continue practicing medicine. Susan Haney concurs who notes the unwary self-referrer who unwarily steps into the lions den.
Former White House Drug Czar (1973-1977) Robert Dupont, M.D. disagrees claiming the programs are worth the price of a “lifetime of well-being.”
You don’t say? Robert Dupont’s ties to the Drug and Alcohol Testing Association (DATIA) are thick and the designs of the former National Institute on Drug Abuse Director are spelled out in the ASAM White Paper on Drug Testing as well as his keynote speech before DATIA proposing expansion of this paradigm to other populations including workplace, healthcare, and schools. He profits from both drug tests and employee assistance program management. The “PHP-blueprint” is simply Straight, inc. for doctors and the same propaganda, fabricated studies, 12-step indoctrination, coercion, control and abuse remain unfettered and just as vile.

Dupont wants to swindle the PHP system into other EAPs such as as DOT proclaiming the “need to reach more of the 1.5 million Americans who annually enter substance abuse treatment, which now is all too often a revolving door.”1 They conclude:
This model of care management for substance use disorders has been pioneered by a small and innovative group of the nation’s physicians in their determination to help other physicians save their careers and families while also protecting their patients from the harmful consequences of continued substance abuse. In fulfilling the professional admonition “physician: first heal thyself,” these physicians have created a model with wide applicability and great promise.1
“Based on abundant evidence, a “new paradigm” for substance abuse treatment has evolved that is the exact opposite of harm reduction. This paradigm enforces a standard of zero tolerance for alcohol and drug use that is enforced by monitoring with frequent random drug and alcohol tests. Detection of any drug or alcohol use is met with swift, certain, but not draconian, consequences.”
Straight, Inc. –Torture as treatment
In 1981 Dupont made similar claims about Straight, Inc., a non-profit teenage rehabilitation center. The predecessor of Straight, Inc., the Seed, was started in 1970 in Florida with a start up grant of $1 million dollars from the federal governments National Institute on Drug Abuse (NIDA). Director of NIDA, Robert L. DuPont, Jr. had approved the grant.on the antidrug cult Synanon founded in 1958. Deemed a the “family oriented treatment program,” Dupont encouraged organization and expansion. Targeting the children of wealthy white families they exploited parents fears for profit. Signs for hidden drug use such as use of Visine, altered sleep patterns, and changes in clothing style were used as indications for referral. Any child who arrived would be considered an addict in need of their services. Coercion, confrontation, command and control as the guiding principles,. Submit or face the consequences. .We know what’s right. The idea was to strip the child of all self-esteem and then build him back up again in the straight image. Abused dehumanized, delegitimized, and stigmatized-the imposition of guilt, shame, and helplessness for ego deflation and murder of the psyche to facilitate canned and condensed 12-step as a preparatory step on the path of lifelong spiritual recovery.

Children were coaxed or terrorized into signing confessions, berated, and told they were in “denial. Inaccurate and false diagnoses were given to wield greater control. Reports and witness accounts now indicate that many of the kids did not even have drug problems but by creating a “moral panic” about teenage drug use they exploited parents fears for profit. Straight, Inc. became the biggest juvenile rehabilitation center in the world. Health officials in Boston cited Straight for treating a 12 -year old girl for drug addiction when her records revealed all she did was sniff a magic marker! Pathologizing normality.

Methodologically flawed research , deceptive marketing, and propaganda were all used to support the continuation of the program. Designed to be hidden from public view. Straight, Inc. had no regulation or oversight. These programs of torture and abuse resulted in many suicides, suicide attempts, post-traumatic stress disorder and other psychological and grave psychological trauma.There is a FB page dedicated in memory to all of those who died.
Of course Dupont brandishes the “PHP-blueprint” claiming remarkable success in the same old saw we have heard ad nauseam. This paper is paraded around as ifs the holy grail but it is methodologically bottom of the barrel and the conflicts-of-interest are obscene. This retrospective five year cohort study published in 2008 is their flagship and shining star and they claim an 80% success rate in treating doctors which sounds pretty good until you consider 80% of the doctors therein do not have a substance use disorder.
The 2008 Physicians Health Program study inexplicably excluded resident physicians because they “were both younger than the average practicing physician and therefore at higher risk of substance abuse.” Other than cherry picking to favor success what is the logic behind that.

More importantly, however, is the 24 that “left care with no apparent referral” and the 48 that “involuntarily stopped or had their licenses revoked.” It is my understanding they chose these endpoints due to the large number of doctors who died by suicide so instead of identifying “suicide” they chose what they did to them as an endpoint. “left care with no apparent referral” sounds better then “left care and shot himself in the head.”
Dupont is bragging and flagging the “blueprint” as a successful model applicable to other populations and plans to bring it to you. Why? To sell long-term inpatient treatment and frequent drug testing. Dupont once recommended everyone under 40 be tested when he was 41. This man wants to test everyone. If he could he would test infants–hell he’d test fetuses if he could. One thing is for certain though–if the blinkered masses don’t wake up from their apathetic slumber they will not too far from now be waking up to pee in in a cup and won’t be able to do a damn thing about it.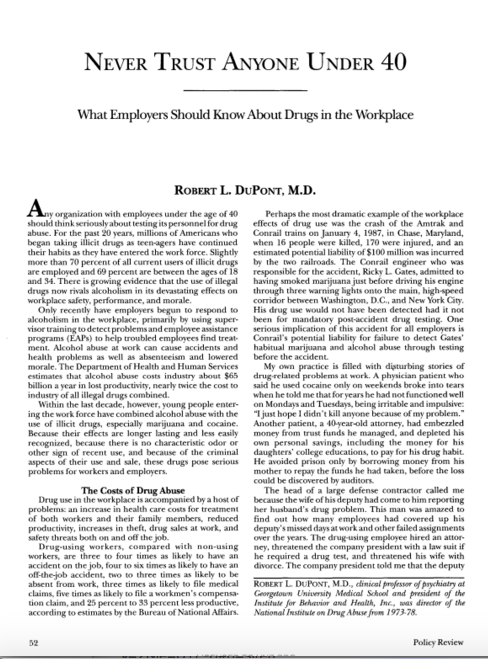

|
Emergency Medicine News:
doi: 10.1097/01.EEM.0000480794.97823.49
News
News: Physician Health Programs: Coercive or Supportive?Katz, Alissa You wouldn’t think physician health programs — designed to help doctors recover from substance abuse — would be such a contentious topic. But more than a few physicians complain that participation is “coercive” if a physician wants to retain his license. The programs are run on a state level, and have evolved into for-profit entities, according to physicians who have been through one. You can find one in all 48 states and Washington, D.C., charged with preventing “substance abuse problems among physicians and to detect, intervene, refer to treatment, and continuously monitor recovering physicians with substance use disorders.” (J Subst Abuse Treat 2009;37[1]:1.) Physician health programs (PHPs) are funded a variety of ways depending on location, including state licensing board grants, fees charged to participants, and contributions from state medical associations, according to reports. When a physician agrees to cooperate with the PHP and adhere to any and all recommendations, it decreases the probability he will be subject to disciplinary action and increases the likelihood he will be able to remain in practice, PHP proponents say. But not everyone agrees. “Participation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate if they have any intention of ever practicing medicine again,” J. Wesley Boyd, MD, PhD, and John R. Knight, MD, former PHP associate directors in Massachusetts, said in an editorial in the Journal of Addiction Medicine. (2012;6[4]:243.) Physician health programs report results of compliance, including drug test results to licensing boards, credentialing agencies, and employers whether the physician is sober, compliant with his treatment, and capable of safely practicing medicine. “Programs are generally structured to encourage professionals to get help early before the onset of problems in the workplace, but the consequences depend on the situation and the state policies,” said Warren Pendergast, MD, a psychiatrist and the CEO of the North Carolina PHP (NCPHP) Compliance MentalityNorth Carolina’s PHP was audited in 2013-2014. “There were a number of protections they wanted us to institute. There was a conflict of interest issue raised about our every-other-year retreat having a small amount of contribution from assessment and treatment centers, and we stopped that in 2012. Our policy was similar to many medical meetings sponsored by vendors,” said Dr. Pendergast. Drs. Boyd and Knight said in their editorial the programs have a compliance mentality that reports physicians to their medical board for possible disciplinary action if they don’t comply with the program’s recommendations, depriving the physicians of having a say in their own treatment. So why are physicians opting into these programs? Colleagues can recommend them for an evaluation and they have to comply, and others who self-refer just don’t know any better, said Susan Haney, MD, an emergency physician in Oregon, who went through treatment assigned by her state’s PHP. “That’s the problem. You assume, as I assumed, that the medical board is staffed with caring and competent physicians, and that the health program is there to help. So you go to them naïvely asking for help or your colleagues refer you to them thinking you’ll get help. I guess some people find help. But a lot of physicians are exploited by the system,” she said. Robert DuPont, MD, the president of the Institute for Behavior and Health and a supporter of physician health programs, said such criticisms aren’t looking at what the programs have achieved. “Outcomes are very positive, with only 22 percent of physicians testing positive at any time during the five years and 71 percent still licensed and employed at the five-year point,” according to a study Dr. DuPont co-authored. (J Subst Abuse Treat 2009;37[1]:1.) Abstinence rates among substance-abusing physicians who engage with PHPs are in the 75 to 80 percent range, which is far higher than almost any other form of substance abuse treatment. This can be attributed to PHPs’ demographic and higher socioeconomic status, compared with those in other substance abuse programs, and the risk-to-reward ratio is often higher for PHP participants. (BMJ2008;337:a2038.) “Programs have no leverage. They have no punishment; they have no consequences. The consequences are all kneaded out by other organizations, by the medical boards or the hospitals. I think all these critics have gotten it mixed up. The physicians who are coming to the PHPs have big problems; they’re under a lot of pressure, not from the PHP but from somewhere else.” Costly TreatmentDr. DuPont’s study said PHPs don’t provide formal addiction treatment, either, but instead function as long-term case managers and monitors for participants. Evaluations through PHP-recommended treatment centers aren’t usually covered by insurance, for example, and can cost as much as $4,500 for a 96-hour evaluation, if not more, and can go as high as $39,000 for a typical three-month length of stay. “If treatment is priced so high that it is out of the reach of potential physician-patients, it does not serve the purpose for which it was created and thus represents an administrative and management failure on the part of the PHP,” Drs. Boyd and Knight wrote. (J Addict Med 2012;6[4]:243.) Because many centers that specialize in evaluating health care professionals also provide costly treatment, Drs. Boyd and Knight said they are left wondering whether financial incentives play a role in the recommendation. Reports argue that physicians charge a lot for their time and services, so they are financially able to pay more than a non-physician would for the same treatment. “In our experience, it is far more common for physicians to simply stay at the same facility for treatment rather than packing up and moving elsewhere,” they wrote. Evaluation and treatment centers support PHPs financially, too, adding to a potential conflict of interest between the two. Dr. DuPont said he thinks the price to pay for assessments and treatment, however, is small compared with the perspective of a lifetime of well-being. “My experience is that PHPs are certainly willing to work with physicians on cost issues. I think it’s not realistic to think the people in the programs are not going to need treatment. To me it goes without saying the treatment is part of the package,” he said. North Carolina has a scholarship program administered through the state’s Medical Society Foundation, and the several-thousand-dollar assessments are part of the reason the program screens. “We don’t send everybody for assessment,” said Dr. Pendergast. Share this article on Twitter and Facebook. Access the links in EMN by reading this on our website or in our free iPad app, both available at www.EM-News.com. Comments? Write to us at emn@lww.com. Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. |


I am looking for a few honest and credible statisticians, biostatisticians or epidemiologists who want to make a difference in the spirit of service and helping others. I can’t pay you but you would be combating injustice, corruption and dishonesty. You would be doing your part in helping the Medical Profession, honest and decent doctors, our country and perhaps our future.
It is only a few public policy steps and minor changes in state regulatory statutes before what is described in the ASAM White Paper on Drug Testing comes to fruition. Before we know it the Drug and Alcohol Testing Industries “New Paradigm” as described here by Robert Dupont will be ushered in as it did with doctors; not with a bang but a whimper. From the ASAM white Paper:
“THIS WHITE PAPER ENCOURAGES WIDER AND “SMARTER” USE OF DRUG TESTING WITHIN THE PRACTICE OF MEDICINE AND, BEYOND THAT,BROADLY WITHIN AMERICAN SOCIETY. SMARTER DRUG TESTING MEANS INCREASED USE OF RANDOM TESTING* RATHER THAN THE MORE COMMON SCHEDULED TESTING,* AND IT MEANS TESTING NOT ONLY URINE BUT ALSO OTHER MATRICES SUCH AS BLOOD, ORAL FLUID (SALIVA), HAIR, NAILS, SWEAT AND BREATH WHEN THOSE MATRICES MATCH THE INTENDED ASSESSMENT PROCESS. IN ADDITION, SMARTER TESTING MEANS TESTING BASED UPON CLINICAL INDICATION FOR A BROAD AND ROTATING PANEL OF DRUGS RATHER THAN ONLY TESTING FOR THE TRADITIONAL FIVE-DRUG PANEL.”To prevent this future drug testing dystopia, that includes testing schoolchildren, we need to take a step back and analyze the reliability and credibility of the “evidence-base” behind these multiple non-FDA approved forensic drug and alcohol tests and testing devices the ASAM proposes be used on the population at large utilizing the Medical Profession as a urine collection agency and bypassing forensic drug testing protocol by calling this “evaluation” and treatment rather than “monitoring” and punishment. New definitions, loopholes, secrecy and subterfuge are the bread and butter of these prohibitionist profiteers.
Amazingly, there has been no Academic review of these tests, let alone a Cochrane type critical analysis. It is essentially untapped territory. In addition there has been no Institute of Medicine type Conflict of Interest Analysis. And that is why I am asking for help from statisticians, biostatisticians and epidemiologists. The task would entail a review of the literature prior to the introduction of these tests for evidence base of forensic applicability (there essentially is none) and a review of the literature peri-and post marketing of these devices to assess the reliability and credibility of the underlying methodology and ascertain the evidence-base. The goal would be publication in both academic journals and presentation to the general public through media publication with the assistance of investigative journalists and other writers. The goal is to get the truth out about these tests and allow both the medial profession and public at large to awaken to the menace this presents to medicine, our society and our future.I am no epidemiologist or statistician but as with pornography I know junk-science when I see it. Almost all of these tests were introduced with little or no evidence-base and, as with most of their endeavors, they did it below board via loopholes and cutting corners.
The overwhelming majority of papers are small, methodologically flawed, non-randomized, non-blinded retrospective studies in that appear to make the data fit the hypothesis. The authors can invariably be linked to those profiting from the tests of the testing process ( the patent holder, doctors associated with the drug testing labs, ASAM or FSPHP, Robert Dupont, Greg Skipper, etc.)
Ethyl Glucuronide (EtG) was introduced in 1999 as a biomarker for alcohol consumption,1 and was subsequently suggested as a tool to monitor health professionals by Dr. Gregory Skipper because of its high sensitivity to ethanol ingestion.2
Described as the “innovator of EtG as an alcohol biomarker,” Skipper and Friedrich Wurst, “convinced” NMS labs in Pennsylvania “to start performing EtG testing in 2002.
The study most often cited as 100% proof that there is 100% accuracy in EtG testing proving alcohol consumption involved a mere 35 forensic psychiatric inpatients in Germany that was published in 2003.3
Shortly thereafter the Physician Health Programs began using it in monitoring doctors and other professional monitoring programs soon followed.
 Laboratory Developed Tests -A Loophole to Avoid FDA Approval and Accountability
Laboratory Developed Tests -A Loophole to Avoid FDA Approval and Accountability
Up until the birth of the EtG tests used for forensic drug and alcohol monitoring had to go through the arduous, expensive and necessary FDA approval process. The LDT pathway was designed to develop simple tests with little risk that have low market potential (i;e. the cost of the normal FDA approval process would prohibit them from coming to market). The LDT pathway was designed to improve patient care and help improve diagnosis and treatment. It was not designed for forensic tests. LDT approval does not require in vivo testing. It is essentially an honor system and to develop an LDT it is not even necessary to prove that the test is actually testing what it is purportedly testing for (validity).
So with little to no evidence base they introduced the EtG, had it developed and marketed as a LDT in collusion with unscrupulous labs, and then began using it on physicians being monitored by State PHPs. This then spread to other monitoring organizations in which there was a large power-differential between those ordering the tests and those being tested (criminal-justice, other professional monitoring programs). These biomarkers have never been used in Federal Drug Testing, SAMHSA approved, DOT, and other organizations where unions or other organizations are present and looking out for the best interests of those being tested.
Another example of how this group removes accountability. There has been essentially no oversight or regulation of LDTs. Although there was a recent push for regulation of these tests the Drug and Alcohol Testing Industry Association lobby made sure that forensic tests would be exempt.They then began publishing “research” on the EtG using the physicians being monitored as subjects. Many of the studies promoting the EtG and other biomarkers can be found in Journals that are linked to organizations that are linked to AA and were organized to educate the medical community.
 These small, methodologically flawed studies amount to little more than opinion pieces but This “evidence-base” is predominantly in biased journals published by biased medical “societies.
The EtG was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8 Sauerkraut and bananas have even been shown to cause positive EtG levels.9
The United States Substance Abuse and Mental Health Services Administration warned against using a positive EtG as primary or sole evidence of drinking for disciplinary or legal action.10 The Wall Street Journal in 2006 reported the problems with the EtG to the general public.11
These small, methodologically flawed studies amount to little more than opinion pieces but This “evidence-base” is predominantly in biased journals published by biased medical “societies.
The EtG was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8 Sauerkraut and bananas have even been shown to cause positive EtG levels.9
The United States Substance Abuse and Mental Health Services Administration warned against using a positive EtG as primary or sole evidence of drinking for disciplinary or legal action.10 The Wall Street Journal in 2006 reported the problems with the EtG to the general public.11
 As any rational authority would do, the majority of monitoring agencies abandoned the EtG after these flaws were revealed. The PHPs did not. They continued to use the EtG on doctors uninterruptedly by telling them to avoid any products that could potentially contain alcohol; a ubiquitous substance in the environment. Since that time they have justified and rationalized (EtG)2,12 13 use by sequentially raising cutoff levels from 100 to 250 to 500 to 1000 to 2000 to now unknown and adding other LDTs as “confirmation tests such as Ethyl Sulfate (EtS)14,15 Phosphatidyl-Ethanol ( Peth)16 17 and other devices such as the Subcutaneous Remote Alcohol Monitoring Bracelet (SCRAM) and, their newest device the Cellular Photo Digital Breathalyzer (CPDB) that has recently been launched, just like the EtG
As any rational authority would do, the majority of monitoring agencies abandoned the EtG after these flaws were revealed. The PHPs did not. They continued to use the EtG on doctors uninterruptedly by telling them to avoid any products that could potentially contain alcohol; a ubiquitous substance in the environment. Since that time they have justified and rationalized (EtG)2,12 13 use by sequentially raising cutoff levels from 100 to 250 to 500 to 1000 to 2000 to now unknown and adding other LDTs as “confirmation tests such as Ethyl Sulfate (EtS)14,15 Phosphatidyl-Ethanol ( Peth)16 17 and other devices such as the Subcutaneous Remote Alcohol Monitoring Bracelet (SCRAM) and, their newest device the Cellular Photo Digital Breathalyzer (CPDB) that has recently been launched, just like the EtG  with little to no evidence base other than a pilot study done by Greg Skipper and Robert Dupont.18
A 2013 article published in an ASAM incubated journal Alcoholism: Clinical and Experimental Research promotes the Phosphatidyl-ethanol (PEth ) test to confirm drinking.16 The study was done on physicians being monitored by the Alabama Physician Health Program who tested positive for EtG/EtS alcohol biomarkers. It is co-authored by Robert Dupont, Greg Skipper, and Friedrich Wurst and involved 18 subjects who tested positive for EtG/EtS of whom 7 claimed they did not drink. After finding that 5 of the 7 tested negative for PEth they concluded that “positive PEth testing following positive EtG/EtS results confirms recent drinking. Hard to wrap your head around the science in that one.
with little to no evidence base other than a pilot study done by Greg Skipper and Robert Dupont.18
A 2013 article published in an ASAM incubated journal Alcoholism: Clinical and Experimental Research promotes the Phosphatidyl-ethanol (PEth ) test to confirm drinking.16 The study was done on physicians being monitored by the Alabama Physician Health Program who tested positive for EtG/EtS alcohol biomarkers. It is co-authored by Robert Dupont, Greg Skipper, and Friedrich Wurst and involved 18 subjects who tested positive for EtG/EtS of whom 7 claimed they did not drink. After finding that 5 of the 7 tested negative for PEth they concluded that “positive PEth testing following positive EtG/EtS results confirms recent drinking. Hard to wrap your head around the science in that one. Skipper is also using both Scram ankle bracelets and the CPDB monitoring in pilots in the Human Interventional Motivational Study (HIMS) Program that was developed in 2009 to “identify, treat and, eventually, re-certify airline pilots with substance abuse problems.
Skipper is also using both Scram ankle bracelets and the CPDB monitoring in pilots in the Human Interventional Motivational Study (HIMS) Program that was developed in 2009 to “identify, treat and, eventually, re-certify airline pilots with substance abuse problems.

The Cochrane Collaboration does systematic reviews of the literature using conscientious, explicit, and judicious criteria to in order to produce and disseminate only high quality and evidenced based health care, exclude bias, and enhance transparency. The Cochrane database is a current and evolving database that includes the accuracy of diagnostic tests and is internationally recognized as the standard in evidence based health care. This benchmark for evidence based health care and systematic reviews, records just 5 controlled trials under the topic ethyl glucuronide.8,19-21 These 5 studies represent the only high-quality evidence regarding EtG applying to EtG. Information provided by the five studies suggests the following, and only the following:
Notably, there are no studies that fit Cochrane Criteria, other than non-alcoholic wine, that look at the pharmacokinetics of EtG or EtS in terms of dose-response curves, cut-off levels, specificity drug and food interactions, or modes of ingestion.
SAMHSA notes that there is little research on PEth and that EtG, EtS, and PEth “do not have a strong research base,” and that “it is not known at this time how the test results might be affected by the presence of physical diseases, ethnicity, gender, time, or the use of other drugs. Until considerable more research has occurred, use of these markers should be considered experimental.”
Phosphatidylethanol (PEth), SCRAM, and the yields no data as a test in the Cochrane library.
SAMHSA notes that there is little research on PEth and that EtG, EtS, and PEth “do not have a strong research base,” and that “it is not known at this time how the test results might be affected by the presence of physical diseases, ethnicity, gender, time, or the use of other drugs. Until considerable more research has occurred, use of these markers should be considered experimental.”
Evidence based medicine (EBM) can be defined as the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.22
Medical progress and scientific advancement is occurring so fast that the volume of medical literature is expanding at a rate of greater than 7% per year.23
Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.22
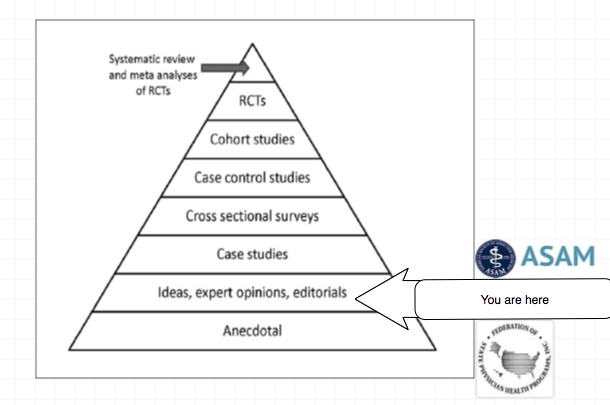
Expert opinion is the lowest level of evidence available in the EBM paradigm.24,25
Fortunately, the scientific method is a tool to help people progress toward the truth despite their susceptibilities to confirmation bias and other errors.26
Unfortunately, due to a confluence of factors (including political) this has not been done. But, unless we want a future as envisioned by Robert Dupont and explained in the the ASAM White Paper on Drug Testing we need to act now. This is not a “New Paradigm” but a “New Inquisition.”




The Ability for Hospitals to Hide behind the Immunity of HCQIA and the Abuse and Coercion by the PHP: my story and caveats.
I have been asked to write a guest blog and whole heartedly agreed. I am not afraid to tell my story and indeed, I feel that physicians need to know my story, so they don’t become yet another victim. This story really isn’t any different that a lot of other physician’s experiences. I want to be certain it is understood that my story is two-fold; violation of due process, breach of contract, and a sham peer review on the hospital’s part and a myriad of violations including roughshod disregard for civil liberties, committed by the North Carolina Physicians’ Health Program. Unfortunately, most physicians have no idea about many of the legal aspects that surround our careers, nor do they have any idea the power a hospital or PHP can wield.
In 1986, HCQIA (Health Care Quality Improvement Act) passed into law. On the outside, this act looked like a good thing because it tried to reign in escalating medical malpractice cases, and to protect people from those physicians. Quite generally, it allows physicians to be reviewed by their peers without the threat of civil litigation by the physician being reviewed. There are many points that have to be met in order for a peer review organization to stand behind HCQIA and earn its immunity. Again, unfortunately, because of this immunity, doctors can become the victim of a Sham Peer Review.
Lawyer, Gregory Piché, who has experience representing not only physicians but also hospitals in these matters, has written an excellent book, Sham Peer Review: The Power of Immunity and Abuse of Trust. While the book duly notes that it is very hard for physicians to fight back against a perceived sham peer review, it is not impossible. There are a multitude of reasons why a doctor might be targeted, for example, professional jealousy or competition. In the second chapter of his book he outlines 12 signs that you may be a victim of a sham peer review. I won’t enumerate those here but, they are eye opening. In my story, I was able to check off 10 of the 12 warning signs.
So enough background for now, let’s get on with my personal example. In November 2013, I was accused of misbehavior at the outpatient surgery center associated with Johnston Medical Center (Smithfield, North Carolina). Four staff members, who were kept anonymous from me, accused me of throwing an instrument and later that same day, striking a patient. Heinous behavior. I didn’t recall anything special from the day in question, I still stand by my side of the events. The instrument I was accused of throwing was a retractor. We were doing an arthroscopic case and thus no retractors were being used. All I can guess is that when we converted to an open procedure, I may have gently tossed the arthroscopic cannula onto the back table. The second accusation, again most heinous, was in a large man who was having hand surgery under a Bier block with sedation. He repeatedly moved and fidgeted, at one point sitting bolt upright on the operating table. I forcibly grabbed his wrist, still attached to a lead hand, and placed it firmly on the operating table, making a thudding sound. I certainly did not strike this patient, that violates my personal rules of honor and integrity. Skipping way ahead for a moment, I eventually had a Fair Hearing through the hospital’s administrative remedies, at which time only one of the accusers showed up. She was not a credible witness and in the end stated that the others hadn’t witnessed anything visually.
Mind you, these events supposedly took place in November of 2013. I was not made aware of it until December and didn’t go before the MEC until January. This is where it is very important to know the bylaws or to review them should you find yourself in a similar position. Under the bylaws I was to have been notified in writing and provided with details concerning the accusastion. Yet, I received only a phone call and then was not told any details of the accusations. Additionally, as a first time report, this should have gone to the head of the surgery department, not directly to the MEC. It should have been handled internally. This was the first violation of their bylaws. In North Carolina, failure to follow your bylaws is considered a breach of contract. From this point on they were violating my rights of due process. Because of the violations of their bylaws, due process, and their breach of contract, they have no right to stand behind the immunity of HCQIA. I wish I knew then what I know now. I should have looked at my bylaws and hired counsel before attending a meeting with the MEC. However, I figured that my explanation would ring true with my “peers.” Another mistake. I did ask about having a lawyer present but I was told that would not be allowed, which is probably true under the bylaws, but certainly is another personal violation of representation.
I presented myself to the MEC and gave my side of the story but I was rebuffed. They investigated and told me they believed my accusers, the same accusers that DID NOT show up to my fair hearing eight months later. I was told that I would be “voluntarily required,” an oxymoron, to go the North Carolina Physicians’ Health Program to be evaluated. The oxymoron was explained as such: if they made it required, they would have to immediately report me to the NPDB. However, it was not voluntary in that my privileges were threatened if I didn’t attend. As I was planning to move out of North Carolina within six months, I agreed simply to keep the peace and move on without issue. I was given assurances by the Vice President of Medical Affairs that the evaluation would be kept confidential and that if anything came of the visit, it would be recommendations only. I, like many others, had never heard of the PHP before.
Due to scheduling issues, I was unable to be evaluated until late February, meanwhile still practicing and working out of this hospital; I was covering their ER, performing consults, and bringing them surgical cases (revenue). I presented for my evaluation, confirmatory email in hand, only to be told that I didn’t have an appointment that day and would need to reschedule. Fine, although I was convinced that was a test of my patience something that has been confirmed by others. Again, due to scheduling issues, (travel for interviews, death of a friend, and on call requirements), I didn’t get seen until early April. I was eventually accused, by the hospital, that I was purposefully delaying my evaluation. Much to my amazement, upon presenting, I was told that I would have to have a urine drug screen and that I would have to pay for it! This was not mentioned ahead of time, although the receptionist who had erred with my initial appointment, commented that I had been told. I was also told, by the psychiatrist, that there was no doctor-patient relationship and he could report me to any authorities he saw fit. Despite me signing a release, I feel that without a doctor-patient relationship, he never had the authority to see my subsequent test results. Certainly, an argument can me made about a HIPAA violation on his part. To this point I have had my 5th and 14th Amendment rights violated by the hospital. NCPHP is probably guilty of illegal search and seizure as well as invasion of privacy.
We haven’t even started the evaluation. We began our talk. Not more than 15 minutes into the evaluation, he was trying to strong-arm me in to a contract with the PHP which would follow me to any future state where I might work. I refused, as I had been guaranteed that I was there for recommendations only. I answered all questions voluntarily, wanting to present myself as open and willing, not an “angry person.” I never refused a question, answering some of the most intimate questions possible. During this evaluation, I was never asked the 20 Questions of Johns Hopkins nor the CAGE questions. I was simply asked about consumption of alcohol which I didn’t deny. I have never been accused of coming to work impaired nor have I had any legal issues related to the social use of alcohol.
As the evaluation ended, I was escorted to and joined in the restroom by the psychiatrist, who was present as I provided a sample. Humiliating and violating. I then asked what drugs it tested for; I was told 12 drugs and alcohol. I balked as I had told him that I used alcohol socially. The urine was in his possession and I was told “not to worry about it.” Of course, the test came back positive for ethanol metabolites. As my evaluation was on Friday, the test result was communicated to me on Monday. At this point, the NCPHP recommended to the hospital that I undergo an evaluation for anger management as well as substance abuse. Remember, I had never been accused of impairment and this was a single isolated test. The courses were expensive and out-of-state. I refused anything to do with substance abuse evaluation or monitoring – which required the out-of-state evaluation or six months of draconian monitoring. I was especially concerned about travel restrictions under the monitoring contract as my daughter was getting married back in the Midwest. I was told they couldn’t guarantee that I could travel for her wedding. Obviously, that was a deal breaker.
At this point, I appealed to the hospital, offering to attend local anger counseling for which I would pay and I even offered to undergo urine testing at the hospital. The hospital continued to rebuff my concessions and attempts at coming to an amicable middle-of-the-road solution. I finally hired a lawyer who made it plain that signing a contract with the NCPHP was not a good thing. It was roughly at this time that the State Auditor in North Carolina released her report on the NCPHP. With all of the stories I know, it’s hard to believe that they didn’t find more evidence of malfeasance in reviewing 100 charts. They did find conflict of interest issues and recommended that physicians be allowed to seek their own care. Despite this recommendation, I was not afforded that opportunity. I presented this information to the MEC along with position statements from SAMHSA (they are against use of an isolated positive test and don’t believe the EtG test should be used as the sole forensic test especially when dealing the career of a professional), as well as reports condemning the EtG test (it is not approved by the FDA). Again, I was rebuffed.
In early May, after failing to sign the contract, I was summarily suspended from the hospital. Again, the bylaws were violated as I did not meet any of the definitions for a summary suspension. Why after six months was I suspended summarily? If they were so concerned, I should have been suspended the previous November. After 30 days, by federal mandate, I was reported to the NPDB and subsequently investigated by the NCMB. I was released from my contract at Duke University. Although my license was never suspended, revoked, or restricted, I have been unable to get even a locums job. I have been rejected by at least three hospitals in Iowa. I’m working towards a Texas license but I’m finding that to be quite difficult. The hospital and PHP have continued to hide behind the veil of immunity. The violations of due process and breach of contract cannot be questioned which eliminates that immunity. The bigger concern is violation of civil liberties committed by both institutions.
Interestingly, the NCMB investigated and asked that I seek another evaluation, for anger management, with a counselor. They gave me a short list of providers in Iowa City, where I had relocated with my family. I went to one visit and she found no issues, other than an adjustment disorder stemming from the way I had been treated. I thought one visit rang hollow, so I pretty much begged the counselor to give me some recommendation. She said I could possibly benefit from a course in communication. Again, from a list of their choosing (the NCMB), I completed an at home course that dealt with communication and anger management.
Meanwhile, the hospital continued to hide behind the recommendations of the NCPHP. They would not back down from that. I eventually was given a Fair Hearing. After three nights of testimony in August and September of 2014, I was vindicated. The panel said that there was not enough evidence to have sent me for an evaluation in the first place, making everything following that moot. One of them has called it a witch hunt; a sham peer review. This decision was remanded by the MEC back to the panel who stuck to their initial decision. However, the MEC refused to overturn my suspension, which is allowed according to the bylaws. An appellate review also fell on deaf ears.
I think this story has many take home points. It never hurts to get a lawyer involved, the earlier the better. I firmly believe that had I involved a lawyer in January of 2014, I may never have had to go for an evaluation at the PHP. Know or review your hospital bylaws if you are ever in any situation with a hospital. Although I was given assurances that only recommendations would be made, the hospital hid behind their HCQIA immunity and the PHP, both entities holding my license/privileges over my head. Get everything in writing. Avoid any PHP, unless you feel you truly need their help, voluntarily. Even then, consider an evaluation by a trusted community colleague. The NCPHP is very typical of these organizations throughout the country, its modus operandi is addiction medicine. They base all of their recommendations on the spiritual 12-step program of alcoholics anonymous and the disproven belief that physicians need more intense treatment, junk science as most people call it. Like most of these institutions, they do not treat patients. They evaluate and refer you to an expensive out-of-state course, where you will most likely be entrapped in a prolonged, never ending contract with the PHP. It has been well documented that if you attend a substance abuse evaluation, you will most likely be labeled an abuser, ending up with 90 days of inpatient treatment. Lastly, be aware of the warning signs of a sham peer review, especially if you are just starting in a new position. Physicians are proud and territorial and they are not always “their brother’s keeper.”
I continue to fight for my professional career but the road blocks are enormous. Finding a lawyer to file suit, on a contingency basis, has also been impossible. As physicians, we need to stand up to these inequities. We need to support each other and contemplate the future when we may need to band together in a class action lawsuit. Maybe it’s time the ACLU becomes truly involved and excited about this opportunity.
Daniel Vande Lune, M.D.


“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.” Father Cornelius Loos ( 1592 )

How Impaired Physicians Can be Helped–Medscape Business of Medicine Article Published February 24, 2015. Click on image to access
How can impaired Physicians be helped?
1. Impairment among physicians is growing: Why?
Answer: It is not. State Physician Health Programs (PHPs) are “diagnosing” impairment when there is no impairment. They are pathologizing the normal and expanding in scope to increase the grand scale of the hunt.
2. What’s the Prognosis for Impaired Physicians?
Answer: Not Good. Those who need help (the truly impaired) are afraid to get help for fear of being monitored by their state PHP while many of those ensnared by PHPs are not impaired. There is absolutely no oversight, regulation or accountability. This needs to be evaluated in the context of physician suicide. The system is one of institutional injustice and abuse of power.
3. Is your knowledge of physician impairment up-to-date?
Answer: No. This will only occur after an evidence-based Cochrane type review separates information from misinformation; An objective non-biased investigation by outside actors identifying any conflicts-of-interest, misconduct or lack of evidence-base in the current system and separating the art and science of the medical profession from the politicalization and exploitation of the medical profession.
The list of doctors on Like-Minded Docs solves the final piece of a puzzle. It explains why so many doctors across the country are claiming fabrication and manipulation of personality and cognitive tests to support nonexistent diagnoses at these “PHP-approved” assessment centers. The relationship between the state PHP’s and the “PHP-approved” assessment centers is the same as it is between the state PHPs and the corrupt labs.
As Drs. John Knight and J. Wesley Boyd note in Ethical and Managerial Considerations Regarding State Physician Health Programs, published in the Journal of the American Society of Addiction Medicine, this is what is known as “tailoring a diagnosis”–a euphemism for the political abuse of psychiatry. According to the Global Initiative on Psychiatry “Political abuse of psychiatry refers to the misuse of psychiatric diagnosis, treatment and detention for the purposes of obstructing the fundamental human rights of certain individuals and groups in a given society.” The shoe fits here. In fact it fits very well.

The Global Initiative on Psychiatry opposes the Political_Abuse_of_Psychiatry wherever it may occur and “supports those psychiatrists and psychiatric organizations that pressure the offending states to discontinue the practice and lobby vigorously those organizations which are wavering. The main way for individuals and organizations to work is through diplomatic channels. It is necessary to expose the practice and to embarrass countries that are at fault by expelling them from organizations such as the World Psychiatric Association. This can only be ensured by properly organized open investigation of psychiatric practice and interviews with the alleged victims”
Political abuse of psychiatry in the profession of medicine needs to be treated in the same way.
An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
In evaluating a physician for “impairment” or being “disruptive” the Physician Health Programs (PHPs) under the Federation of State Physician Health Programs (FSPHP) are not gathering data to form a hypothesis. They are making data fit a hypothesis that arrived at the out-of-state “PHP-approved” assessment center well before the alleged miscreant doctor.
With guilt assumed from the start, no due process, no appeal, and no way out physicians are being bullied, demoralized, and dehumanized to the point of hopelessness, helplessness and despair.
This needs to end now.
Medicine is predicated on competence, good-faith, and integrity.
Medical ethics necessitates beneficence, respect, and autonomy.
The scaffold erected here is designed for coercion and control.
Exposure, transparency, and accountability are urgent.
The emperor has no clothes.
Sunshine is the best disinfectant.
https://artbylisabelle.wordpress.com/2015/03/01/three-shells-and-a-pea-asam-fsphp-and-lmd/



A lawsuit was filed in Federal Court in March against the organization that monitors impaired professionals for the Michigan State Board of Medicine, alleging constitutional violations, financial conflicts, lack of oversight, and due process. Three mid-level providers are claiming damages as a result of actions taken by the Health Professional Recovery Program (HPRP), originally established to provide health professionals with a confidential and non-disciplinary approach to dealing with substance abuse disorders and mental health issues.
The HPRP, administered by a private contractor, was initially designed to monitor treatment of health professionals referred to them by providers. But plaintiffs claim the program’s administrators are overruling treatment decisions by board-certified and licensed physicians in favor of coercion of individuals into a small group of selected treatment facilities that are also charged with providing an initial evaluation of the need for treatment. Treatment facilities are expensive, and in most cases, insurance companies don’t consider these admissions to be medically necessary.
In one case cited in the court filing, the plaintiff was told she would have to stop taking pain medication prescribed by her treating physician for a period of two years. This decision was made after a short evaluation during which the evaluator did not contact the treating provider, and when the plaintiff refused to agree, her nursing license was summarily suspended. Her suspension was later dissolved in court. This is one small example, but it’s telling, Last time I checked, doctors had the right to choose a healthcare provider. It is surprising that the Michigan Medical Board would support a policy that essentially declares many of their own licensees inadequate to provide a treatment plan.
Unfortunately, this is not the only professional health program faced with backlash for financial double dealing and coercion. North Carolina physicians’ complaints promoted the North Carolina State Auditor to investigate oversight by the medical board in that state, and she found evidence of lack of oversight and the appearance of conflict of interest. Money flowed directly from the “impaired physician program” to their “approved providers” in the form of scholarships for the doctors they referred.
A common pattern has emerged in the treatment of doctors for mental illness or substance abuse. Agencies that were originally installed as volunteer boards aimed at helping doctors return to practice safely have been populated with a new group of professionals – doctors who are closely tied to treatment facilities or drug testing companies who frequently have their own history of substance abuse issues.
A recent string of posts on SERMO, the world’s largest physician-only social network, received a lot of attention. It is clear there have been a lot of abuses, sharing of confidential information, and lack of due process for participants. Many object to the religious overtones of every program that is “approved” for doctors by the Federation of State Physician Health Committees, the parent organization that has formed to keep all state committees notified of talking points. Physicians are currently subjected to polygraph tests, a practice most Americans would never accept. The term “disruptive physician” is an easy way to target those who speak out against a system that has become adversarial.
There are 400 suicide deaths annually among US physicians. Many of these doctors suicide when under investigation or contract with the committees originally designed to help them return to health. Other doctors are afraid to speak out, for fear of reprisal, particularly when in a contract with their PHP.
Have you heard of a colleague who has self-reported or has been reported for mental health or substance issues? Perhaps you have experienced a period of mental health crisis in your own life. How did you handle reporting requirements? What rights should doctors enjoy?

|September 24, 2015
R. Jeffrey Goldsmith, MD, DLFAPA, FASAM; Gary D. Carr, MD FAAFP, FASAM, DABAM
To the Editor:
We are writing on behalf of the American Society of Addiction Medicine (ASAM) regarding the Medscape 08/19/15 article “Physician Health Programs: More Harm than Good?” authored by Pauline Anderson. ASAM is a professional society representing more than 3,600 physicians and associated professionals dedicated to increasing access and improving the quality of addiction treatment. We have a robust body of policy statements supporting the role of physician health programs and an active Physician Health Committee, which includes current and past directors of state physician health programs (PHPs), as well as current past leadership of the Federation of State Physician Health Programs (FSPHP). ASAM believes this article does not fully represent the outstanding, professional, ethical and honest work done by our states’ PHPs.
This recent Medscape article reviews the complaints of several individuals who, in one fashion or other, have become dismayed with their state Physician Health Program (PHP). The article reviews their allegations in some depth and goes on to discuss investigations of PHPs in Michigan and North Carolina, with emphasis on the latter. The article reviews concerns over lack of due process, out of state treatment requirements, cost of treatment, “expensive contracts,” treatment center demands for payments, lack of PHP oversight, conflicts of interest, etc. All in all it presented a very disparaging view of state PHPs.
Physician Health Programs were created in the 1970s after an article featured the high numbers of suicides among Oregon physicians following licensure revocation for addictive illness. Both the AMA and the Federation of State Medical Boards (FSMB) called on individual states to develop programs to assist these physicians. Early PHP work involved addiction alone and later grew to include all psychiatric illness when PHPs identified significant psychiatric comorbidity among their addiction participants. Some PHPs with expertise and funding also assist with the “disruptive” or more accurately, the “distressed physician,” typically a physician in need of interpersonal coaching to improve communication. Others assist physicians who have engaged in sexual boundary violations and for whom there is an underlying, untreated psychiatric disorder at play.
The author failed to note the national study of PHPs called project Blue Print. This study revealed that nationally, PHP participants demonstrate a 78% success in recovery without relapse at an average of 7.2 years of monitoring. If we consider those who suffer a brief relapse and then enjoy success, that number exceeds 90%. The only other organization that shows that level of effectiveness is the airline industry, which, like medicine, employs safety sensitive professionals. These organizations have raised the bar for those treating addictive illness around the country. Is there a reason the author failed to even mention this?
The author communicates that those involved in a PHP have no due process. This is a mischaracterization. Before PHPs, physicians with these illnesses dealt directly with their state medical boards and were often disciplined merely for being ill. The PHPs have, in effect, been allowed to serve as a “buffer” to this system. The PHP offers the physician with potentially impairing illness an opportunity for a multidisciplinary evaluation at a choice of nationally recognized facilities. If treatment is indicated, they are given options for centers equipped to provide treatment. If they disagree with the evaluation, they are given the option of a second opinion evaluation. The PHP itself, with one exception, does not independently diagnose or treat. At any time — from the initial contact with the PHP and thereafter — the physician has the right to present their case directly to the state Medical Board. If they are being mistreated or unfairly diagnosed, they have complete due process with their Medical Board. PHPs do not exist to judge “guilt and innocence” or to determine what medical practice act statutes were violated. They exist to provide assistance and support to a physician who is ill and to support that physician’s restoration to wellness and a safe return to practice.
One of the author’s sources highlighted the North Carolina Audit — an exhaustive investigation. The Audit reviewed the NC program from stem to stern, including the details of over 100 cases. Their findings were released in April 14, 2015. There were NO instances of abuse by the program, misappropriations of funds or conflicts of interest identified by two subject experts employed by the State and independent of the PHP. The auditor made recommendations which the program has since instituted to protect itself and protect against even the appearance of impropriety. That’s it. To me, that feels pretty close to exoneration.
The author’s sources allege PHPs can be heavyhanded or demanding, “forcing” doctors into expensive out of state treatments, requiring
“expensive” contracts and the like. If you are a physician with addictive illness characterized by denial of that illness due to fear and shame, the process of evaluation and the introduction to treatment, when indicated, can feel intimidating. When a physician is afflicted with a potentially impairing illness, the privilege to practice medicine may be lost, in the absence of restorative treatment. While Medical Boards employ discipline to protect the public, PHPs offer an alternative to discipline. Namely, PHPs support physicians by directing them to evaluators and treatment programs with the requisite expertise to care for professionals in safety sensitive employment. Physicians, when they are patients, should not expect to dictate where, when and how their treatment will take place. Selfdiagnosis and selftreatment is uniformly discouraged in the medical profession. However, physicians may pursue second opinion consultations, just as patients in the general population are encouraged to do.
Once successfully treated, the physician engages in a contract with the PHP which entails careful monitoring of the health condition and accountability. In turn, the PHP can confidently advocate for the physician’s return to practice before their regulatory board, hospital credentialing bodies, malpractice carriers and others. Is it too much to ask that a physician recovering from illness be accountable to a PHP and in doing so, obviate the Medical Board’s need to discipline? If a doctor is going to take my daughter to surgery, I would appreciate the assurance that the doctor is safe to do so.
PHPs are highly effective. Were it otherwise, they would have ceased to exist years ago. Are they accountable? They are held to account every day by their state medical boards and professional associations, their state hospitals and the partners of every doctor they work with. A single incident of patient harm by a PHPmonitored doctor would result in public outrage, and in all likelihood fuel onesided, misleading articles like that produced by Ms. Anderson. There would be tremendous pressure on the medical boards to abandon the PHP model and start revoking licensure. That could easily happen. It would take us back to the licensure revocations observed in the 1970s, destroying the careers of physicians and denying the public access to an important resource, particularly at a time we are encountering physician shortages.
We submit, you will find no group of professionals in the country who have done more for physicians with potentially impairing illness than the state PHPs who comprise the FSPHP. They devote their careers to the task of assisting colleagues who, without their help, would certainly no longer be practicing medicine and in many instances would be dead of their disease. They are most often led by professionals who are devoted to helping those colleagues who are suffering and at risk for suicide. Day after day, they man the gate of help and hope and do all they can for the doctors who need them while fending off detractors, including organizations in favor of abolishing PHPs and shaming ill physicians through public discipline. In my view, the loss of PHPs and the safety they provide to physicians in crisis would do “More Harm than Good.” PHPs exist because they work. For every doctor the author interviewed to disparage their work, there are thousands who would attest to the benefit derived from their involvement with a PHP.
ASAM believes this article was not representative of the outstanding, professional, ethical and honest work done by our states PHPs. We, and all our patients, are fortunate to have them. Their success rate with complicated illnesses raises the bar for our entire field. They remind us that such success in treating these illnesses should not be the exception — it should be our expectation for all our patients.
Sincerely,
R. Jeffrey Goldsmith, MD, DLFAPA, FASAM
President, American Society of Addiction Medicine
Gary D. Carr, MD FAAFP, FASAM, DABAM Chair, ASAM Physician Health Committee
Cite this article: ASAM Responds to ‘Physician Health Programs: More Harm Than Good?’. Medscape. Sep 24, 2015.



Hi Mr.Goldsmith,
Currently, these ‘PHP approved evaluation’ centers are the exact same facilities as the PHP ‘treatment’ centers. There centers also have financial relationships with PHP programs and PHP directors.
They charge upwards of $5,000 dollars to the physician plus travel and lodging expenses, because they are often out-of-state.
Former ASAM leader and PHP director Dr.Talbott owned such a facility with a judge as a co-investor. Dr.Talbott was convicted by a jury in a US court of law of coercing a doctor into unnecessary ‘treatment’ for financial gain. How many of these 78% recovery rate come from physicians falsely diagnosed? Dr.Fata, the Michigan doctor convicted of giving false cancer diagnoses, also touted his high ‘treatment success rate’
We’d like you to correct these current questionable practices by ASAM and PHPs. A true independence of diagnosticians and PHPs is a good place to start, with strict oversight and auditing to eliminate all and any financial ties and conflicts of interest. PHP leadership and directors should be replaced by physicians with demonstrated commitment to ethics and personal rights.
Do these steps sound reasonable to you?