
In “Ethical and Managerial Considerations Regarding State Physician Health Programs, ” Dr.’s J Wesley Boyd and John Knight note the significant and multiple conflicts of interest that exist between State Physician Health Programs and the referral treatment centers that they use. They state:
“To further complicate matters, many evaluation/treatment centers depend on state PHP referrals for their financial viability. Because of this, if, in its referral of a physician, the PHP highlights a physician as particularly problematic, the evaluation center might—whether consciously or otherwise—tailor its diagnoses and recommendations in a way that will support the PHP’s impression of that physician.”
There is an obvious difference between impartially evaluating evidence in order to come to an unbiased conclusion and building a case to justify a conclusion already drawn. To consciously “tailor” a diagnosis of addiction or relapse based on anything other than the objective evidence violates the basic principles of medical ethics.
A state audit of the North Carolina Physicians Health Program that was released in 2014 documented the conflicts of interest and lack of quality assurance in referrals to out of state “PHP-approved” assessment and treatment programs. The same centers are used in most states including Massachusetts. and the the medical directors of the “PHP-approved” facilities can all be found on this list of “Like-Minded Docs.” The financial and political conflicts-of-interest are obvious between the PHPs and the “PHP-approved” assessment and treatment centers. And there is no choice in the matter.
In 2011 the ASAM issued a Public Policy Statement on Coordination between Treatment Providers, Professionals Health Programs, and Regulatory Agencies recommending physicians in need of assessment and treatment be referred only to “PHP approved” facilities and also that PHPs need the full cooperation of the board if they deem a monitored physician noncompliant as “criticism or doubt could unintentionally undermine the PHP” In addition the ASAM wants regulatory agencies to recognize the PHP their expert in all matters relating to licensed professionals with “potentially impairing illness.” You read that right, “potentially impairing illness.” The Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting and approved the concept of “potentially impairing illness” and “relapse without use.”
And what might signal a potentially impairing illness you ask? According to Physician Health Services, Inc. (PHS), not having “complete, accurate, and up-to-date records” could be a red flag as “when something so necessary is not getting done, it is prudent to explore what else might be going on.”
Boyd writes in Psychology Today that when he and John Knight published this paper, reviewers at 2 different journals said that the issues raised were very important but it “should not be published, essentially because doing so might bring unwanted outside attention to PHPs” and —one of them wrote the paper should be withdrawn and instead be presented at the national federation of PHPs’ annual meeting. Boyd recommends more state audits and national standards and that “because PHP practices are largely unknown to physicians until they themselves are referred to one, physicians who do register complaints about standard PHP practice are often dismissed as bellyaching”
On July 1st 2011 I was asked to have a blood test for alcohol. 19 days later it was reported at an impossibly high level and I was reported to the Board of Registration in Medicine and asked to have an evaluation at one of the “PHP-approved” facilities.
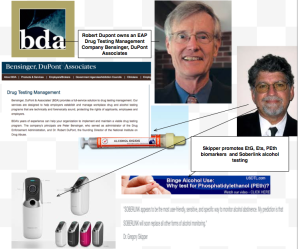
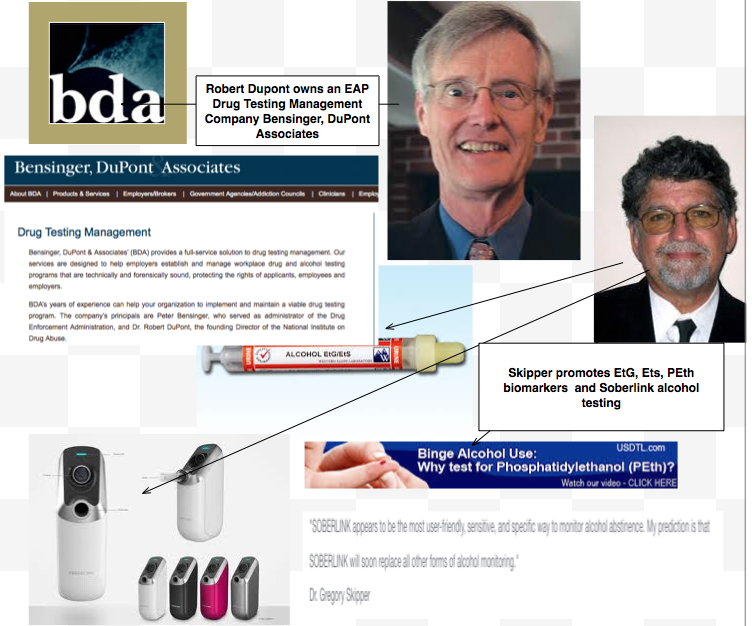
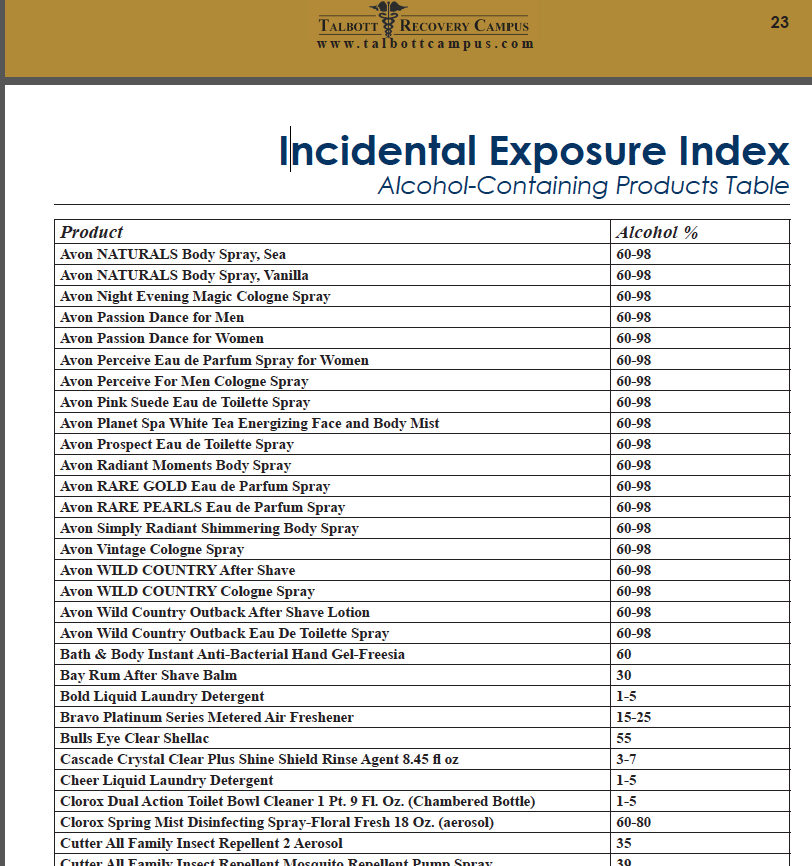
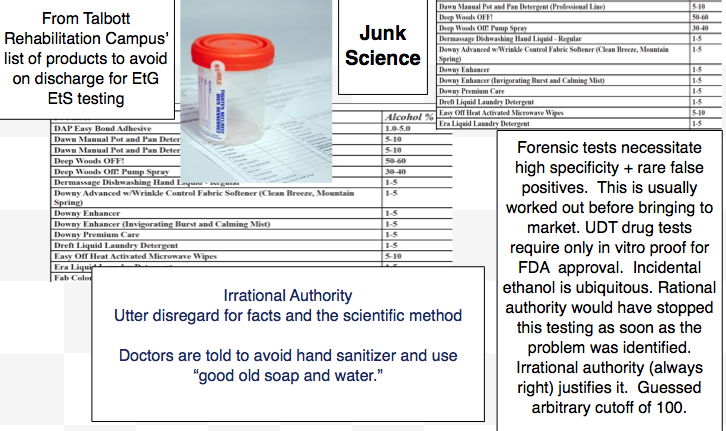
One potential conflict-of-interest that has not been entertained is that between the PHP and the contracting labs. Just like the assessment and treatment centers there is a lot of money involved in drug and alcohol testing and the FSPHP is a big referral source. In addition, some of the tests these labs are using on physicians were actually introduced by an ASAM/FSPHP doctor and developed as Laboratory Developed Tests (LDTs). LDTs do not require the stringent FDA approval process. In actual fact , you don’t even have to show that it is even detecting the substance you claim it to be testing for. Some internal protocol has to be provided but other than that it is an honor system. And without FDA oversight, the labs can claim anything they want as far as validity, sensitivity, and specificity. Once these tests were developed as LDTs they were pitched to the Federation of State Medical Boards as reliable and valid. The PHPs then contracted with the labs to use the tests they introduced for monitoring physicians in the programs. The EtG was introduced with essentially no evidence-base other than a small study on less than 20 psychiatric inpatients in Europe with an arbitrary cutoff of 100. Countless lives were ruined with lost medical and nursing licenses, incarceration, loss of custody of children and most programs abandoned it in 2006. A SAMHSA advisory was issued that it was unreliable. The Wall Street Journal wrote an article about the “flawed test.” Most monitoring programs abandoned it. The PHPs did not and continued to use it on doctors without pause. The PHPs put the responsibility on the monitored physicians to avoid hand sanitizer, cologned, sauerkraut, and hundreds of other products as ethanol is ubiquitous in our environment. Irrational authority. The EtS, and PEth were also introduced by an FSPHP physician.
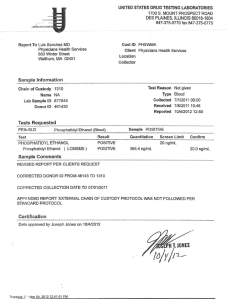
It was just discovered that after 7 days and under unknown conditions my PEthStat Forensic test was changed to “clinical” with specific instructions to USDTL to run it as “clinical.” PHS then misrepresented it to the Board as forensic for the last three years. PHS is not a “clinical” provider.
USDTL-Litigation Packet(selected)
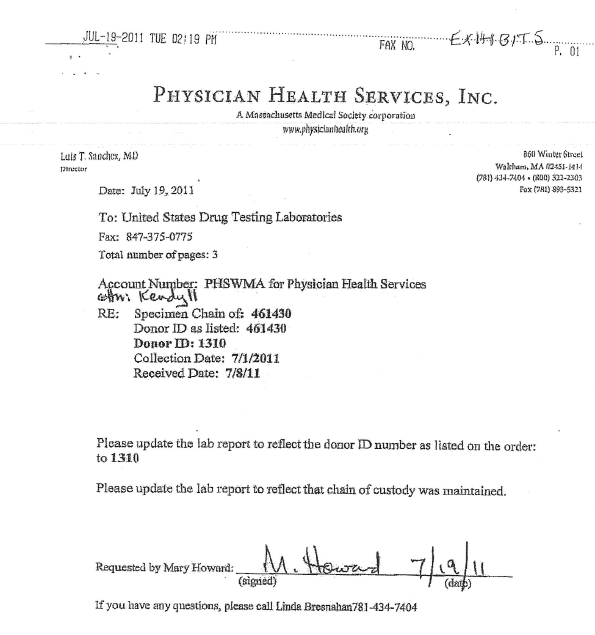
What we see here is a letter from Luis Sanchez reporting a positive test for phosphatidylethanol (PEth) from July 19th, 2011 to the Board of Registration in Medicine. I have also attached documents from the “litigation packet” received from USDTL that is generated with any forensic drug test as a record of chain-of-custody. This document ensures the integrity of the drug testing by recording the specimens whereabouts at all times. The Medical Review Officers job is to make certain everything was done correctly by confirming that everything was documented and their were no breaks in the chain-of-custody. If a donor disagrees with a positive test then the litigation packet is used to check the integrity of the specimen. It is a quality control measure that protects both parties.
The litigation packet contains all of the information that the MRO reviews when reporting the results of a positive specimen. If the custody and control form contains all of the information it is supposed to and confirms chain of custody then it is reported as a positive. If the chain-of- custody contains so called “fatal flaws” (lacking collectors signature, missing date and time, mismatched ID #’s, specimen not sealed, etc.) then it is deemed “invalid.” it must be thrown out by protocol. That is standard operating procedure, standard of care, and required. This is the MROs sole and simple responsibility.
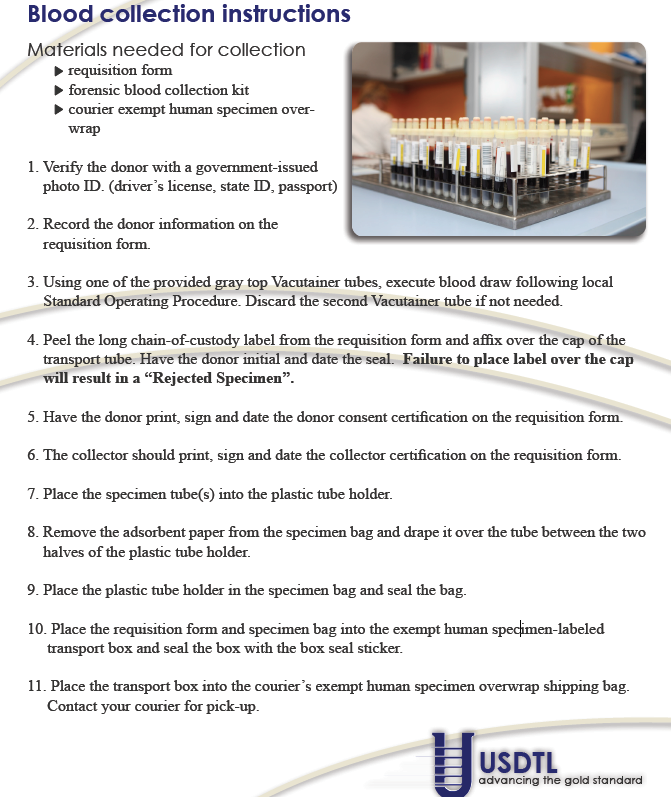
collectioninstructions_PEth_ FD_021810
In my case I disagreed with the positive result and requested the litigation packet on the specimen. This was at first refused by PHS. Linda Bresnahan and the PHS attorney Deb Grausbaum then tried to dissuade me from obtaining it deeming it complicated and costly. But I insisted on obtaining it and sent the $500.00 fee and when I did so was told that there would be “unintended consequences” as a result of my request. I finally received it in December of 2011 and it included a “summary of results” dated December 3, 2011 and signed by the director of Laboratory operations, Joseph Jones, supporting it as a true positive. (even though it contradicts his own written protocol on forensic collection procedure.) what he preaches apparently does not apply when it comes to pleasing a big client such as the FSPHP. $$
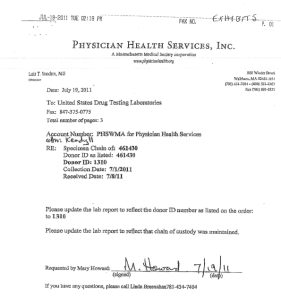
So what do we see here in the litigation packet? Evidence of deliberate forensic fraud perpetrated by PHS, drylabbing, and intentional misrepresentation of lab data. It shows clear and deliberate falsification of lab data at the request of PHS and includes a memo from Linda Breshahan on July 19th requesting that the ID# on a positive specimen with no collection date be “updated” to my ID # 1310 and that it be updated to show “chain-of-custody” be maintained. Well that would seem highly unusual as a “chain-of-custody” cannot be backdated and “correcting” a unique identifier on forensic specimen is prohibited. In actual fact there was no chain-of-custody and not even a custody and control form the collecting lab (Quest Diagnostics)! When this complete absence of external chain of custody was pointed out to PHS they pleaded ignorance but eventually produced a letter from Quest Diagnostics dated March 22, 2012 that appears to be written in language suggesting legitimacy but in actuality documents all of the fatal flaws.
A six-month investigation was done by CAP and USDTL was forced to change the test from “positive” to “invalid” on October 4th 2012. This was reported to PHS but not conveyed to anyone else. The Chief Investigator for CAP called me in December of 2012 to make sure the test had been corrected. It had not. Instead PHS reported me to the Board for “noncompliance” the 2nd week of October for damage control. They apparently did this as a pre-emptive strike thinking I would never find out!
It does not take a forensic toxicologist or chemist to interpret the attached documents. They show collusion to commit fraud with USDTL, collusion to cover up fraud with Quest Diagnostics, misrepresentation of facts to a State Agency, and obstruction of the truth when the test was mandated by CAP to be corrected by USDTL. These documents show conspiracy, fraud, and corruption. What they show is procedurally, ethically, and legally indefensible.


The distinction between “forensic” and “clinical” drug and alcohol testing is black and white. Forensic testing is done to detect illicit substances. Pre-employment, random monitoring, or for cause drug testing is done in individuals to see if they are using drugs or alcohol when they should not be. Because the consequences of a positive test can be significant and even permanent, forensic drug and alcohol testing requires strict procedure and protocol to prevent harming the innocent. A custody and control form documenting the chain-of-custody and review by a Medical Review Officer (MRO) before reporting a positive test are necessary to ensure the validity of the test. It is the responsibility of the MRO to make sure no other explanations exist for the positive test (such as a prescribed medication) and check chain-of-custody. If the chain-of-custody contains any “fatal flaws” (specimen not sealed with sticker and signed by donor, missing date or collector signature, etc.) it is rejected as an invalid specimen.
A clinical test is used in patient care. Ordered by a doctor, it is use for purposes of treating a patient. A clinical test does not have the strict requirements of a forensic test. I could send a sample of fluid from a tin of pickled herring or Jagermeister to the clinical lab for electrolytes and would still get a result back.
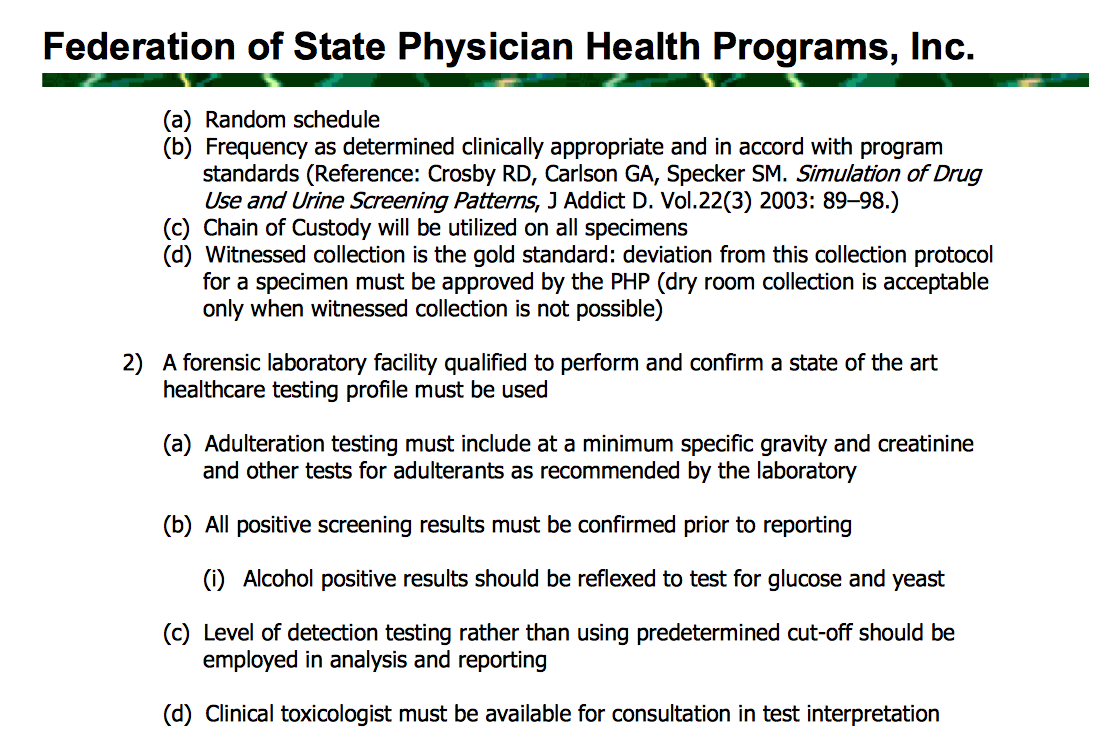
PHS is a monitoring program not a treatment provider. According to PHS documentation they follow NIDA drug and alcohol testing protocol. Guidelines for both the Federation of State Medical Boards (FSMB) and the Federation of State Physician Health Programs (FSPHP) state chain-of custody and MRO review on all specimens. In addition to MRO review the guidelines also specify that the PHP Medical Director confirm all positive tests. PHS has an MRO, Wayne Gavryck.
I have multiple emails sent to Gavryck asking him to correct this and inquiring why as an ardent 12-step zealot he was not practicing what he preaches by promptly admitting his wrong and making amends for it. He ignored me. Can’t wait to hear him have to explain his doublethink and hypocrisy publicly.
MRO Code of Ethics
The fact that a monitoring agency with an MRO asked the lab to process and report it as a clinical sample and then used it forensically is an extreme outlier in terms of forensic fraud. The fact that they collected it forensically, found out it was collected wrong with no chain of custody and the wrong tube 7 days after it was drawn and then changed it from forensic to clinical deepens the malice. The fact that they then reported it to the Board as a forensic sample and maintained it was forensic up until now makes it egregious. But the fact that the test was changed from “positive” to “invalid” on October 4th, 2012 and they then reported me to the Board on October 8th 2012 for “noncompliance,” suppressed it and tried to send me to Kansas for damage control makes it wantonly egregious. (they didn’t think I’d ever find out but the CAP investigator called me in December. Add on that the fact that I’ve been questioning the validity of the test since day 1 and they violated the HIPAA Privacy Rule over and over and this is reckless and major health care fraud.
Like other front groups the primary motive is profit for the drug testing and rehab industry, and “recovered” physicians like Dr. Gavryck have become “willing gulls” in all sorts of fraud and chicanery. Ideology trumps science and control usurps conduct. including Dr. Gavryck, are “in recovery” themselves and, having only a hammer, see everything as a nail. PHS, inc. is a non-profit NGO that has become corrupt. This occurred under the leadership of the prior Medical Director Luis Sanchez, MD who has since retired. The director of operations, Ms. Linda Bresnahan is engaging in fraud with apparent impunity. Forensic (in contrast to clinical) drug testing mandates strict adherence to protocol including proper collection procedures, unbroken chain-of-custody, and Medical Review Officer (MRO) review prior to reporting a forensic test as a true positive. It is held to a higher standard because the potential consequences can be grave and far reaching. There are no exceptions. The Federation of State Medical Boards and the Federation of State Physician Health Programs require chain-of-custody and MRO review for any and all drug testing according to their guidelines. PHS, inc has an MRO, Dr. Wayne Gavryck, who has holds this responsibility. I have attached the MRO Code of Ethics and an explanation of the importance of chain-of-custody.
Medical Review Officers need to have honorable values and follow the same standards as everyone else.
If an individual’s identity is tied to a sub-group that is unregulated, unaccountable, and with no oversight, such as PHS, fraud may be committed even though they have excellent knowledge about cultural norms and values on a more general level. So called “noble cause corruption is quite common and one someone gives up their integrity in lock step with the other members of the group, no matter how small the enticement, the potential for continued and more severe forms of corruption is increased.
collectioninstructions_PEth_ FD_021810
PHS provided a letter from the New England Compliance Manager, Nina Tobin, on March 22, 2012 in response to my persistence in obtaining the absent Quest “chain-of-custody.” After going into great detail about the faxed document from PHS, she states “the collector was unfamiliar with collecting blood samples for PHS and did not have a “chain-of custody” form designed for blood tubes.” “The collector used the faxed letter request, which included the test code and the collection information, as the chain of custody form.” This is analogous to not receiving an item you requested by express mail and having them reply the person was “unfamiliar with the postal system in the United States and did not have a postage stamp, she wrote U.S. Postal Service on a piece of paper and wrote “express mail” on the flat side and folded it into an envelope.” The very nature and purpose of both are removed. You cannot manufacture a chain-of-custody any more than you can manufacture a stamp.
MLLv3finalJacob Hafter Esq
ThePhysician suicide has increased dramatically across the country and as Pamela Wible observes in the Washington Post it is “often hushed up.” It is only going to get worse. Heightened perceptions of defeat and entrapment are known to be powerful predictors of suicide.
Quest lists “accountability” as one of six company values on their corporate website claiming “as a company and as individuals, we accept full responsibility for our performance and acknowledge our accountability for the ultimate outcome of all that we do.” Quest lists “integrity” as a value noting all “decisions and actions ultimately are driven by integrity,” and an Integrity Commitment Pledge. The Quest Code of Business Ethics includes compliance with laws, rules, and regulations. confidentiality in release of test results and protected health information (PHI), avoidance of Conflicts of Interest (COI), and fair dealing; “no person may take unfair advantage of anyone through manipulation, concealment, abuse, or privileged or confidential information, misrepresentation of facts or any other unfair dealing practice.” Quest “actively promotes honest and ethical behavior in all its business activities,” and require employees to report violations to, among others with supervisory capacity, a “Compliance Officer.”

i














 This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.
This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}