Deciding Whether To Refer a Colleague to a Physician Health Program
J. Wesley Boyd, MD, PhD
Physicians should exercise caution in referring a possibly impaired colleague to a physician health program (PHP), given that PHPs work closely with their state medical societies or licensing boards but often receive little oversight. The AMA Journal of Ethics is a monthly bioethics journal published by the American Medical Association.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.” The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical Society updated its mission to read:“The purposes of the Massachusetts Medical Society shall be to do all things as may be necessary and appropriate to advance medical knowledge, to develop and maintain the highest professional and ethical standards of medical practice and health care, and to promote medical institutions formed on liberal principles for the health, benefit and welfare of citizens of the commonwealth.”With a foundation and history built and based on of scholarship and critical thought we need to support the highest levels of science, fact, intelligence and reason. Stupidity tries but it should not win. Before the Boston Society for the Diffusion of Useful Knowledge in 1842, Dr. Oliver Wendell Holmes delivered two long lectures entitled “Homeopathy and Its Kindred Delusions.” He characterized one of its popular practitioners, Dr. Robert Wesselhoeft, as one of those: “Emperics [quacks], ignorant barbers, and men of that sort…who announce themselves ready to relinquish all the accumulated treasure of our art, to trifle with life upon the strength of these fantastic theories.” That “pretended science” as Holmes called it, was “a mingled mass of perverse ingenuity, of tinsel erudition, of imbecile credulity, and artful misrepresentation, too often mingled in practice…with heartless and shameless imposition.”And Holmes words are as apt and appropriate today as they were in mid 19th Century Boston! Probably more so. History has recurrently proved that false constructs and groundless concepts allow for endless error. The Massachusetts Medical Society and all of its members need to come to the realization that Physician Health Services (PHS) has paradoxically become a reservoir of bad medicine beset by corruption. The documentary evidence of professional, ethical and legal misconduct must be specifically and precisely addressed.
Accountability. Answerability and Justification Required. Accountability, or answerability, is necessary to prevent abuse and corruption. This requires both the provision of information and justification for actions. What was done and why? Professional guidelines and standards of care, ethical codes of conduct and the law are all objective benchmarks that can be used to assess the actions and decisions of others. In any free society this necessitates the existence of organizations of truly independent opinion capable of standing in this judgment.State PHPs are Non-Governmental Organizations (NGOs) over which the state health department has no supervisory oversight. There is no regulation, no transparency and no accountability. There is no public scrutiny and they police themselves. In Ethical and Managerial Considerations Regarding State Physician Health Programs Drs. John Knight and J. Wesley Boyd called for greater oversight and scrutiny of PHPs by the medical community at large. They recommended periodic auditing, national standards and regulation. They also attempted to convince the Massachusetts Medical Society to implement changes at PHS where they served as Associate Directors with over two decades of collective experience. These efforts to promote transparency and accountability at both local and national levels, however, fell on deaf ears.State PHPs have systematically removed doctors of academic integrity and moral compass. Those not conforming to groupthink were threatened with litigation if they breached “peer-review” statutes or confidentiality agreements and this has effectively silenced many from reporting misconduct, abuse or even crimes they may have witnessed.
Massachusetts PHP engaging in Procedural, Ethical and Criminal Misconduct In Massachusetts John Knight was removed in 2009 and J. Wesley Boyd in 2010. In Ethical and Managerial Considerations Regarding State Physician Health Programs they comment “if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise—tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.” So too will the clinical laboratories. Of course “tailoring” a diagnosis to support anything other than the real diagnosis is fraud. The “PHP-approved” assessment centers are willing to fabricate and misrepresent neuropsychological and cognitive testing to support “denial” and “cognitive-impairment.” Detailed examples can be seen here and here. The evidence is clear that past medical director Dr. Luis Sanchez and Director of operations Linda Bresnahan have engaged in not only unethical but criminal activity. Egregious misconduct including forensic fraud and political abuse of psychiatry can be seen in detail here, here and here. This type of inverse morality is antithetical to the history and organizational purpose of not only the MMS but the entire Profession of Medicine. Institutional injustice can have grave and far reaching consequences. Increasing reports suggest that programs just like PHS are contributing to the suicide epidemic in doctors. The patterns are the same and the same scaffold is being used. PHPs are colluding with the same drug-testing companies and “PHP-approved” assessment facilities. It is, in fact, a rigged game.
Sunshine is the best disinfectant. Very few doctors are speaking out. Most are vey afraid and remain silent.Few have obtained documentary evidence of misconduct. I have. To ignore the problem or suggest that it does not exist will only cause more damage to other doctors. The suicides will continue. Nothing will change. The majority of Massachusetts Medical Society members (as are the majority of doctors) are honest, thoughtful and responsible. Most are completely unaware of the ethical and criminal allegations concerning PHS. This is, after all, a system that depends on secrecy and silence. Most doctors are also probably unaware that the MMS has no regulatory, supervisory or investigatory oversight of PHS. They have removed themselves from scrutiny by design. The only avenue of complaint, I have been told, is by filing an ethical complaint with the MMS grievance committee and that any investigation is private, non-disciplinary, and final. This is irrespective of the severity and scope of the complaint. What this means is that any complaint against a member of PHS is behind closed doors, if the complaint is substantiated it results in “education” not “discipline,” and the decision cannot be further addressed, appealed or revisited.
Moreover, I have been hearing that ethics and grievance committees in many states have been intentionally populated by PHP apologists, supporters and friends. As with the other “point-people” they have positioned at medical boards, public health departments and law enforcement, these friends of like-mind are used to deflect, block, delay, suppress and minimize valid complaints. I do not know if this is the case in Massachusetts. However, the bottom line is that only two results are possible from any complaint 1) complaint dismissed–final answer, or 2) complaint substantiated–member educated on matter-final answer. Although this system may be applicable to some of the common ethical conundrums encountered in the medical profession it is not applicable to criminal activity and fraud.
The character of those involved in PHS can be seen in my post “Integrity and Accountability the Declining State of Physician Health and the Urgent Need for Ethical and Evidence Based Leadership.” Wayne Gavryck’s moral compass and adherence to professional and ethical standards can be seen here. My request is simple, straightforward and should be easy to answer. So to any of the apologists, supporters or defenders of PHS I have a simple request. Just answer the questions here. No reframing the question, moving the goalpost or redirecting the focus. Just register and respond. Simple request and litmus test. Ascertain or refute what you see. Can the actions of actions of Dr. Luis Sanchez, Dr. Wayne Gavryck or Linda Bresnahan procedurally, ethically or legally. Yes or No.
Accountability Requires Answerability and Justification for Actions. Accountability necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable. State PHPs such as PHS have not only removed answerability and justification but have taken steps to prevent any interference by outside actors including medical societies, medical boards, law enforcement and departments of public health. The most crucial step in solving any problem is admitting it exists. This exists. There is a solution to this. Sunshine is the best disinfectant. If the actions of Sanchez, Gavryck and Bresnahan cannot be justified or defended then it must be concluded that these individuals have violated procedure, ethics and the law. And if that is the case it is the responsibility of the MMS to acknowledge the individual and specific issues as well as the reality that there is no current avenue to address these issues. That, in and of itself, is a problem. The documents show significant and severe wrongdoing that constitute crimes committed within the walls of MMS. How far down would the moral compass have to go before the significance of this is recognized? This necessitates acknowledging the problem exists, defining the problem and addressing it directly.
Zero-Tolerance for Forensic Fraud and Political Abuse of Psychiatry Necessary. Any and all forensic fraud should be met with Zero-tolerance. State PHPs are colluding with commercial drug testing labs and “PHP-approved” assessment and treatment centers this same scaffold is being used in many states. Doctors are dying because of it. State Physician Health Programs (PHPs) are organized under the Federation of State Physician Health Programs (FSPHP). The FSPHP arose from the American Society of Addiction Medicine and the history can be seen here.
Dr. Luis Sanchez is past President and Linda Bresnahan is the current Secretary. The FSPHP does not represent doctors but the multibillion dollar drug and alcohol testing, assessment and treatment industry. This will all come out in due time. The states of North Carolina and Michigan have taken the lead in starting to expose this. Others will follow. State Auditor Suzanne Bump is currently looking into a Massachusetts Audit of PHS. But because of the scope and severity of the forensic and rehab fraud it is morally imperative that the MMS address this. Those engaging in forensic fraud must be removed. This needs to be done state by state and I am providing Massachusetts with documentary proof.of forensic fraud. This is not isolated but systemic. There are plenty of doctors of intellectual and moral integrity to take the place of those who do not. The criminal and ethical violations shown do not comport with any codes of conduct including those of the medical society. It is paradoxical here that in my battle against PHS that I am the one supporting truth and fact,medical and professional ethics, evidence-based medicine and physician rights. It is I who am fighting for the preservation of and adherence to historical ideals and moral codes of the medical profession. This is easily seen by looking at rhetoric versus actions and deeds. Those of Sanchez, Gavryck and Bresnahan are irreconcilable. As the oldest medical society in the United States whose stated purpose is to “…do all things as may be necessary and appropriate to advance medical knowledge, to develop and maintain the highest professional and ethical standards of medical practice and health care, and to promote medical institutions formed on liberal principles for the health, benefit and welfare of citizens of the commonwealth” it is morally imperative that the Massachusetts Medical Society address this urgently, directly and with full-measure. Massachusetts needs to take the lead in exposing this national problem.
In his book “Fire Lover: A True Story,” Joseph Wamnaugh profiles Fire Captain and Senior Arson Investigator for the Glendale California Fire Department John Orr. Known for his uncanny instincts in solving arson cases, Orr often astounded other investigators with his seemingly brilliant deductions in determining the causes of incendiary crime.
As it turns out, neither instinct nor brilliance played any role. Orr solved many of these cases by first-hand knowledge. He actually started many of the infernos he fought. Burning down businesses and homes for over a decade, investigators suspect Orr may have intentionally set as many as 2000 fires.
John Orr
One involved a large Pasadena hardware store that killed four people including a 3-year old toddler and his grandmother. Orr is now serving a life-sentence at Lompoc Penitentiary. Details of his arsonist acts are described in chilling detail in his own book, “Points of Origin…playing with fire.”
These cases have generally been attributed to “bad apples,” and prevention has hence been focused on identification by screening of candidates in the same manner as police departments–methods that may successfully identify and weed out criminals turned cops but not cops turned criminals.
This type of screening is unlikely to isolate those with inverted perceptions of morality for whom the normal rules do not apply. There is no test to identify individuals joining the police force “who might get so caught up in making things right or getting their guy that they would push procedural, legal or ethical boundaries.” There is no test that would have identified John Orr.
The 1991 film Backdraft illustrates this type of warped morality in portraying a firefighter turned arsonist who attempts to make a moral political statement about the dangers of reducing firefighter staffing by setting a series of explosive fires to prove the social value of firefighters. Hinds-Aldrich describes an ends-justifies-the-means occupational overzealousness in which these individuals in their efforts to do what they think is right take matters into their own hands and begin freelancing.
Occupational socialization and commitment go awry and firefighter arsonists may attempt to downplay their acts and believe the risks are manageable or even justified and necessary. They may believe they are truly providing the community a valuable service by eliminating dilapidated and crime-ridden properties-noble corruption all done for the greater good.
In a large number of cases studied by Hinds-Aldrich, at least two firefighters at the same department were involved in the fire-setting. They worked together. In Louisiana, authorities discovered that several firefighters from two rural districts were setting dozens of fires each year, mostly grassland but eventually buildings.
The majority of firefighters are individuals of integrity, good-heart and moral compass. But an estimated 100 firefighters are arrested for arson each year. Many others have avoided detection due to a confluence of factors. Hinds-Aldrich notes some have even returned to work as firefighters at a later date. Some have been let go by their department without formal investigation under the rationalization that the threat was removed. The desire to keep this behind closed-doors is understandable as the arsonist, as a firefighter, puts a stain on a noble profession. How many of these returned to their old habits is unknown. Historically no methods have been in place to detect, investigate and hold accountable those who are engaging in behavior that is the antithesis of their public responsibility and trust.
But this behavior has consequences that are sometimes grave and permanent. As Wamnaugh notes: “The damage they do in one fire can be enormous. I mean it can be a calamity, just one crime.”
Backdraft was loosely based on firefighter Ray Norton Jr who was in 1985 was convicted of conspiring with seven other “sparkies” to set 219 blazes in and around Boston during a 14-month arson spree. The group was motivated by the mistaken belief that the fires would force local governments to hire more firefighters after widespread layoffs in the 1980s. The group started with trash bins and vacant buildings but this soon escalated to burned houses, churches, factories, restaurants, a Marine Corps barracks and the Massachusetts Fire Academy. More than 300 people were injured and $22 million in property was destroyed. This illustrates the concept of so called “noble corruption” and the power of “groupthink.”
What are the motivational factors involve? Some experts previously hypothesized arsonist firefighters may have been motivated by situational factors, boredom or wanting to participate in the job they were tasked with doing –putting out fires. Others have theorized that becoming a firefighter was a direct consequence of being a firebug; a deliberate volitional choice similar to a foot fetishist becoming a shoe salesman.
This seems plausible on the surface. It makes sense in the same vein of logic as Willie Sutton’s explanation as to why he robbed banks–“that’s where the money is.” If firefighter arsonists are the product of a pyromaniacs wish fulfillment in choosing a vocation that supports and a fire fetish then screening to identify this pathology makes perfect sense. Identify and remove the threat before the damage occurs. If Florsheims wanted to extirpate all foot fetishists a screening system identifying any unusual proclivity for toes could be developed. The underlying reliability and validity of that screen, however, depends on multiple factors including the truthfulness of the potential shoe salesman. It’s much more complicated. It is a safe assumption that selling shoes does not create a fetish for feet. Some foot fetishists become shoe salesmen but I would guess few shoe salesmen become foot fetishists.
In the case of arsonist firefighters evidence suggests that it is much more complicated. Arsonist firefighters are not the simple product of a firebug choosing a vocation that provides an increased incidence of engaging in and a closer proximity to their avocation. Joining the profession does not appear to be deliberate machination to acquire an unmolested backstage pass to start fires. The personality profiles of firefighters who engage in arson seems to involve an interplay between insecurity and power. Therefore the usual screening procedures are ineffective as this type of personality predisposes these individuals to evolve into arsonists over time. It is an evolution fostered by the reinforcement of power and control. Such was the case with Orr.
According to Joseph Waughnaugh: “It’s power and control. They’ve not only created a living thing, they’ve created a living thing that is the object of massive attention.”
One of the primary motives for firefighters who commit arson was found to be the desire to be seen as a hero. Those with deep-seated insecurities and feelings of powerlessness, such as Orr, are provided with a feeling of empowerment over society. These individuals are suddenly given attention, recognition and validity they never had. Retaliation for some grievance, real or imagined, may also sometimes play a role.
“They may be the first to call in a fire, the first on the scene, and one of the most eager, excited, and enthusiastic members of the response team. Their main reason for lighting the fire is so they can appear as a hero, either by being the first to spot the flames, or by rescuing people and saving property. Extreme cases of firefighter arson involve fires set in occupied structures. When a firefighter sets fire to an occupied structure, the potential for being a life-saving hero is even greater. In North Carolina, one firefighter would set fire to an occupied house, and then return to the scene and rescue the family. His need for excitement, being worshiped, and getting attention predominated over any concern about the terrible danger to which he exposed the occupants”
Some researchers believe that firefighter arsonists undergo a mental process referred to as RPM: the arsonist rationalizes the crime, projects blame, and minimizes the consequences.
The impact of firefighter arson can be severe. People die or are seriously injured, including fellow firefighters. Homes are destroyed. An arsonist from within the fire department can disgrace the whole department, and his actions diminish public trust. Several states that have experienced the crime of firefighter arson have developed new legislation that directly impacts the prosecution of firefighters accused of arson.
The most crucial step was admitting that the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
Physician Wellness Suicides and Medical Review Officer Forensic Fraud
Multiple parallels exist between firefighter arsonists and physician wellness experts. Misuse of entrusted power occurs when those who have been given authority to carry out expected goals instead use their position and power to benefit themselves and others close to them. Abuse of power is particularly egregious when that person is doing the opposite of what he or she is supposed to do.
The firefighter who commits arson is an example of this phenomenon. So too would be a program that ostensibly promotes the health of doctors but is in reality driving them to suicide or a Medical Review Officer (MRO) ( whose sole job is to prevent the donor of a drug or alcohol test from being falsely accused of drug or alcohol use) falsely accuse a donor of drug or alcohol use by engaging in fraud.
Some of the same psychodynamics and sociocultural factors are probably involved. A disproportionate number of arsonist firefighters are volunteer firefighters (75%) who offered to help fight fires and ended up doing the opposite.. A large majority of physician wellness experts were doctors who had had their licenses revoked and were only able to practice medicine again by becoming “addiction medicine” specialists and offering to help other doctors. As a result these programs self-select for doctors who did something severe enough to lose their licenses and getting their licenses back does not necessarily mean they have changed. Many used the “salvation” card to get their licenses back. “I’ve changed.” “I want to help others.” “I’ve been redeemed.”
Designed with the dual purpose of helping sick doctors and protecting the public, many of the current state Physician Health Programs (PHPs) do neither. Paradoxically they have become reservoirs of bad medicine and institutional injustice. Part of the problem is the PHPs have removed themselves from answerability and accountability. Accountability necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable. As we have seen, much of this is by intentional design. PHPs have no oversight or outside regulation. No avenue exists to file a complaint let alone investigate one. In addition those who do file complaints are targeted for retaliation and retribution via “swift and certain consequences” that can be irreversible. Because of this, few ensnared by these programs speak out and those outside dare not speak up out of fear of being targeted themselves. This provides the necessary secrecy and silence they need in order to operate.
As with firefighter arson, few people are pointing their fingers at PHPs and claiming any problems with them. Any suggestion of misconduct or wrongdoing is inevitably ignored, delayed, blocked, rationalized or justified.
Most worrisome is the fact that outside agencies who should and could be doing something about ethical violations, procedural irregularities and even crimes are doing nothing. As a result inverted systems of morality involving procedural, ethical and criminal violations against doctors are able to not only exist but thrive.
This needs to change. Everyone in the medical profession must be and should be prepared to admit that there are ethical, procedural and legal breaches being committed by State PHPs and that precise, firm methods are needed to combat the situation. To ignore the problem or suggest that it doesn’t exist will only increase the damage caused by the impaired physician movement as well as destroy the morale of good and honest doctors. We must talk to all doctors about forensic fraud, neuropsychological fraud and physician suicide. We must investigate, charge and convict the perpetrators of these crimes. No exceptions. The most crucial step in exposing firefighter arsonist was admitting the problem exists. The most crucial step in exposing physician wellness corruption is admitting the problem exists. Although we have made some gains this has not yet happened.
Defend the Medical Review Officer (MRO)
It is now over five months and no one has been able to procedurally, ethically or legally justify the actions of Dr. Wayne Gavryck and the Massachusetts PHP, Physician Health Services, Inc. I had previously offered 100 volumes of the Classics in Medicine Library to anyone who could do so. (see prior blog below). No one has.
Therefore I am going to lower the bar and increase the prizes. If anyone can think of anything that would hypothetically justify the actions of Gavryck and PHS procedurally, ethically or legally then they win my complete collection of the Classics in Medicine Library. On top of that I will add my collection of Cocoanut Grove artifacts as seen below. Just one will do.
Cocoanut Grove Artifacts including menu, wine list, and matchbook
The Cocoanut Grove was a popular nightclub and restaurant lo located at 17 Piedmont Street in Downtown Boston. On Saturday November 28, 1942 it was the scene of a tragic and deadly fire that killed 492 people and injured many more. Fourteen hospitals received the injured and the dead: Beth Israel, Boston City, Cambridge (MT Auburn St.), Cambridge City, Carney, Chelsea Naval, Faulkner,
Massachusetts General, Massachusetts Memorial, Peter Bent Brigham, St. Elizabeth’s, St. Margaret’s, and U.S. Marine. Boston City Hospital took the majority of patients (134) and Massachusetts General Hospital took 39.
Boston City Hospital merged with the Boston University Medical Center Hospital and unfortunately the majority of its records and archives have been lost. Fortunately, we know more about the practices and techniques used at Mass General as a result their excellent archives and due to the June, 1943Annals of Surgery, which was dedicated to the Symposium on the Management of the Cocoanut Grove Burns at the MGH.
While innovations in burn treatment were a major focus, burns were not the only medical problem. Upon arrival at the hospitals, it was obvious that a large number of patients had severe respiratory distress. Some patients showed evidence of obstruction to the air passages. Non-burn specialists were quickly called to the scene to perform laryngoscopes, tracheal suction and tracheotomies. Such a large number of respiratory patients at one time enabled doctors and researchers to better understand the impact of various treatments, leading to many advances in the field.
As the Medical Review Officer (MRO) for the Massachusetts state Physician Health Program (PHP), Physician Health Services, Inc. (PHS, inc.), Dr. Wayne Gavryck’s responsibility is an important one. His job is to verify that the chain-of-custody in any and all drug and alcohol testing is intact before reporting a test as positive.
Dr. Gavryck evidently did not do that here. In fact for more than a year he helped cover up an alcohol test that was intentionally fabricated at the behest of PHS Director of Operations Linda Bresnahan (who told me when I confronted her with the fact that I have never had or ever even been suspected of having an alcohol problem “you have an Irish last name–good luck finding anyone who will believe you!”
It took a formal complaint with the College of American Pathologists to get the truth out. The whole fiasco can be seen here and here.
What Gavryck and his co-conspirators did is egregious and ethically reprehensible. It shows a complete lack of moral compass and personal integrity. What was done from collection to report to coverup and everything in-between is indefensible on all levels (procedurally, ethically, and legally).
The documentary evidence shows with clarity that this was not accident or oversight. It was intentional and purposeful misconduct. I think everyone would agree that there should be zero-tolerance for forensic fraud in positions of power. Any person of honor and civility would agree.
Transparency, regulation, and accountability are necessary for these groups. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. I’ll erase my blog and vanish into the woodwork. But If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Sanchez and Bresnahan (much like Annie Dookhan) he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths.
Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
It is people just like this who are killing physicians across the country. The body count is vast and multiple. And those who are caught doing dirty deeds such as this need to be held accountable.
Please help me get this exposed, corrected, and rectified. The doctors of Massachusetts and the doctors of this entire country deserve better than this.
Integrity and Accountability—Defend the MRO Procedurally, Ethically or Legally and win 100 Volumes of the Classics in Medicine Library and Salk and Sabin Autographs!
“The incompetent or unprincipled physician, licensed to practice medicine by a too complaisant State, is the greatest menace to scientific medicine – as great a menace as all the cultists put together.” —Dr. Morris Fishbein (The Medical Follies. New York: Boni Liverlight, 1925 p. 71)
“There is no place in science for consensus or opinion, only evidence” —Claude Bernard
Sabin, Salk and the Classics in Medicine Library
Polio is nearly a thing of the past thanks to to Dr. Jonas Salk and Albert Sabin. In 1952 Salk discovered and developed the first successful vaccine for polio and combined with Albert Sabin’s 1961 oral vaccination the duo effectively obliterated the contagious polio virus. Once a deadly threat to our country and future there were 93,000 cases of polio reported in the U.S. Between 1952 and 1953 alone. But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
full body respirator or “iron lung” needed to treat patients whose respiratory muscles became paralyzed by polio
October 23, 2014 was the centenary of Jonas Salk’s birth and in honor of his 100th birthday I am sponsoring a contest to win framed autographs of both Jonas Salk andAlbert Sabin as seen above. In addition, you will receive 100 volumes of the Classics in Medicine Library published by Gryphon Editions whose “mission is the preservation of the literary and intellectual heritage of the noble professions that we serve”
These are exact facsimiles of the original classics bound in leather and include works by William Osler, Harvey Cushing and Paul Dudley White.
Background
According to British sociologist G. V. Stimson the “impaired physician movement” is characterized by a “number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by involvement in medical society and treatment programs.” Their “authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
In this regard Dr. Wayne Gavryck, M.D. is a prototypical example.
An ex-alcoholic with a history of malpractice, Gavryck quit drinking through Alcoholics Anonymous, became “board certified” in “Addiction Medicine” and became involved with the Massachusetts PHP, Physician Health Services, Inc. (PHS) where he has been an Associate Director since 1988. He serves as their Medical Review Officer (MRO).
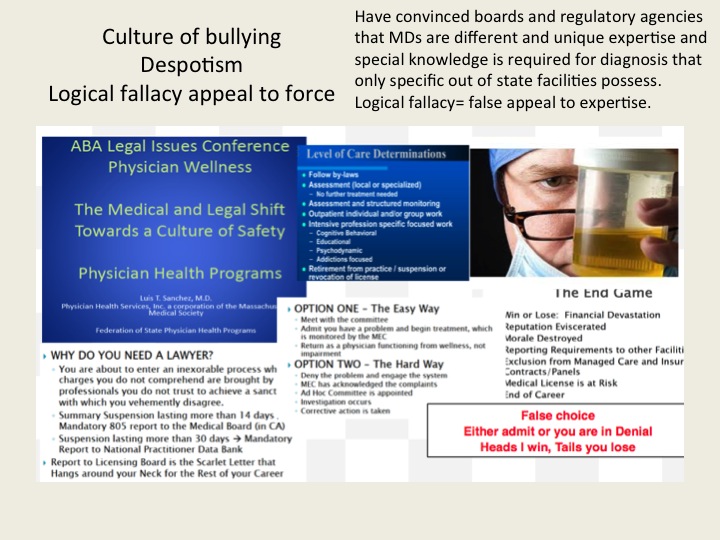
The “impaired physician movement” has gained tremendous sway through the American Society of Addiction Medicine and the Federation of State Physician Health Programs. The ASAM is not a valid medical specialty but a “special interest group” that represents the chronic relapsing brain disease with lifelong abstinence and 12-step recovery model of addiction and the companies that profit from it financially ( drug and alcohol testing labs, 12-step inpatient assessment and treatment centers) and politically (Drug War advocates, Anti -Medical Marijuana advocates). The impaired physician movement gained a seat at the table of power in medicine by bamboozling regulatory and administrative medicine. This illegitimate and irrational authority is in charge of almost every state PHP in the United States. ASAM physicians joined their state PHPs, gained power, and then removed those who did not agree with the groupthink and doublethink. Blind obedience and control are favored over fairness, truth and evidence-base. As with other states under the FSPHP, blindly obedient doctors are kept on while those who question the science and ethics of the groupthink are removed. The PHP-Drug Testing Laboratory and “PHP approved” assessment and treatment center industrial complex requires a Medical Review Officer of blind faith who places the goals of the FSPHP above all other considerations including the Hippocratic Oath. The system requires doctors who are willing to participate in “moral disengagement” of wrongdoing including professional, ethical and legal violations. To erect this scaffold they have put in place barriers to exposure and accountability. By declaring themselves “experts” they have used logical fallacy to temporize deflect and otherwise stifle accountability. With no oversight or regulation they are, in fact, accountable to no one. The appeal to authority and esoteric knowledge is an effective means of extinguishing valid concerns. Complacent that this is a group of benevolent organizational purpose those who should know better and could do something about it rationalize their apathy and indifference. A necessary step in exposing and addressing this problem is imposing accountability. If an organization is able to engage in conduct that is the antithesis of accepted professional guidelines and standards of care, in violation of professional and societal mores and codes-of-conduct and is illegal then there is a systemic problem. This problem can fortuitously be addressed by examining standards of care, conduct and criminal codes for breaches. If a breach is found then it needs to be explained and justified. One of the tactics of the FSPHP is to deflect criticism under the logical fallacy of appeal to authority. We are the experts. We know better. That is where it usually ends. But accountability requires both the provision of information and justification of actions. My hypothesis is that this group is committing fraud, violating ethics and flouting the law in an irrefutable manner. If this is not true then my hypothesis should be able to be refuted. It cannot. And for that reason I am putting my money where my mouth is.
Accountability
In all fairness, If Gavryck can justify his actions either procedurally, ethically or legally and back it up by any written protocol, guideline or standard then he wins and I will refrain from any more criticisms. In addition I will hand deliver to him the Salk and Sabin autographs and 100 volumes of the classics in medicine, apologize and remove this entire blog.
Accountability requires both the provision of information and justification of actions. One way of examining this is to look at the body professional and ethical standards and state and federal law. The FSPHP has blocked the provision of information regarding drug-testing. Although it has taken over three years I have obtained the all of the information pertaining to a July 1, 2011 test that should have immediately been rejected by the MRO. It is an invalid test.
Dr. Gavryck violated every conceivable procedural guideline and standard-of-care there is for an MRO, the Medical Review Officer Certification Council’s Codes of Ethical Conduct and both State and Federal Law. This can be ascertained by looking at the documentation. I have done this and found hundreds of documents that support the accusation that as an MRO Wayne Gavryck breached protocol, engaged in unethical behavior and broke the law. Prove me otherwise with just one credible source and the prizes are yours.
Contest Rules
Your job is to review the documentary evidence and records from PHS, Quest Diagnostics and USDTL and assess the actions and decisions made by the MRO)
If you can show that these decisions were the result of legitimate reasoning based on published guidelines or protocol, ethically defensible or did not break any laws and cite one credible source that concurs with this point of view then you have won.
If you can show that these decisions were the product of legitimate and thoughtful reasoning in accordance with established guideline, ethical codes then I will hand-deliver the items to you.
If you can justify, support or defend the actions of the Medical Review Officer (MRO):
Procedurally;
Ethically;
or Legally;
You win all of the prizes! Simple as that!
In fact, If you can support just one of these the entire lot is yours.
If you can show Dr. Gavryck did not breach any and all published Standards-of-Care andProfessional Protocols and Guidelines regarding drugs-of-abuse testing, OR that he did not violate any and all Codes of Conduct and Ethical Guidelines of the Medical Profession from Hippocrates to the American Medical Association OR that he did not violate multiple State and Federal Laws you win Salk and Sabin autographs and all of the books.
All of the documents and details regarding the forensic fraud, concealment, coverup and deliberate misrepresentation to a state agency under color of law can be seen here:
To Review: Any and all drug testing requires chain-of-custody. “Forensic” drug testing differs from “clinical”drug testing because the consequences of a falsely positive test can be grave and far reaching. Because the results of a positive test can result in the loss of rights and liberties of the person taking the test it is essential that it be done correctly. False-positive tests are unacceptable so strict chain-of-custody procedure and MRO review assure specimen integrity. This provides accountability and the custody
The custody-and-control form records chain-of-custody and is given the status of a legal document as it has the ability to invalidate a test that lacks complete information. The job of the MRO is to invalidate specimens without intact chain-of-custody.
The MRO job is fairly simple. If a lab reports a positive test for any substance the MRO must check that the signatures, dates, times and other information on the custody-and-control form are correct and per protocol. Chain-of-custody must be accurate and complete. The MRO looks for “fatal flaws” on the chain-of-custody form. If a “fatal flaw is present then the test is invalidated and the test is not reported as “positive” but “invalid.”
The sole job of the MRO is to ensure that the drug testing process and chain-of-custody procedure is followed to the letter. The MRO reviews the Custody and Control form for accuracy and completeness. The MRO also rules out any other possible explanations for a positive test (such as legitimately prescribed medications). Only then is a test reported as positive.
“the sole responsibility of the MRO is to”ensure that his or her involvement in the review and interpretation of results is consistent with the regulations and will be forensically and scientifically supportable.”
Corruption is misuse of entrusted power. It occurs when those who have been given authority to carry out expected goals instead use their position and power to benefit themselves and others close to them. Abuse of power is particularly egregious when that person is doing the opposite of what he or she is supposed to do.
Accountability is necessary to prevent corruption and necessitates both the provision of information and justification for actions; what was done and why? The other defining factor of accountability is the ability of outside actors to punish and sanction those who commit misconduct or wrongdoing. Without these constraints corruption is inevitable.
Although Gavryck may serve PHS, it is not in the capacity of a certified medical review officer; by my count the documentary evidence alone shows that he violated four of the seven Medical Review Officer Certification Council Codes of Ethical Conduct. In addition to violating the MRO Ethical Conduct he violated every other code I can think of from the Hippocratic Oath to the AMA Code of Ethics. and everything in between.
As the MRO for PHS Gavryck’s responsibility is simple. He is supposed to verify that the chain-of-custody of the sample was intact before reporting a test as positive.
This is indefensible on all levels (procedurally, ethically, and legally). The documents show with clarity that this was not accident or oversight, but intentional and purposeful misconduct
There should be zero-tolerance for forensic fraud of this sort. Those of integrity and moral compass would agree. Transparency, regulation, and accountability are necessary. It is an issue that needs to be acknowledged and addressed not ignored and covered up.
If Dr. Gavryck can give a procedural, ethical, or legal explanation of what was done then I stand corrected. Just one will suffice. If he cannot then this needs to be addressed openly and publicly. And whether he was involved in the original fraud or not is irrelevant. As the MRO for PHS it is his responsibility to correct it–however late the hour may be.
Perhaps Dr. Gavryck needs to see some of the damage he has caused in order to take this responsibility. Known as a “bag man” who simply rubber stamps positive tests at the request of Linda Bresnahan, much like Annie Dookhan, he does not see the damage that is caused. Forensic fraud has grave and far reaching effects and in this case has severely impacted many people and include patient deaths. Perhaps Dr. Gavryck needs to take a “moral inventory” and see that this this type of behavior causes real damage to real people and put a face on it.
Please help me get this exposed, corrected, and rectified. The physicians of Massachusetts deserve better than this.
In 2012 Robert Dupont delivered the keynote speech at the Drug and Alcohol Testing Industry Association annual conference and described a “new paradigm” for addiction and substance abuse treatment of zero tolerance for alcohol and drug use that is enforced by monitoring with frequent random drug and alcohol tests. Detection of any substances is met with swift and certain consequences. He proposed expansion of this paradigm to other populations including workplace, healthcare, and schools. Based on the state Physician Health Program model of “contingency management,” with frequent testing and a point of “leverage,” such as a medical license in doctors, that is used as a behavioral incentive.
The ASAM White Paper on drug testing seems to indicate a desire to liberalize drug testing by utilizing health care providers in the process. Currently forensic drug testing uses a strict chain-of-custody protocol with Medical Review Officer (MRO) review. But if the result of a positive test is “therapeutic” rather than “punitive” this is unnecessary. In the “new paradigm” a positive test simply requires an evaluation at a “PHP-approved” facility.
Accountability needs to be rooted in organizational purpose and public trust.
A recent article in JAMA, “Identification of Physician Impairment” suggests that undetected physician impairment may be contributing to medical error and that sentinel-event and random alcohol-drug testing could be implemented to address the problem as is being done in the current “Physician Health Program (PHP)” system.
The most consequential and critical issue for physicians, if this comes to fruition, is who will be in organizational and managerial control of the system and what ideological influences will be guiding policy and practice. It is concerning that one of the co-authors of this article, Greg Skipper, is a Fellow of the American Society of Addiction Medicine with strong ties to the 12-step treatment industry and drug testing industry.
History shows Lord Acton’s aphorism on absolute power to be repeatedly true. Corruption is a virtually inevitable consequence of unchecked power. The only two factors that constrain corruption are moral virtue and deterrence.
Disregard for standards of care and violations of codes of conduct are common. So too is the use of anything that furthers the agenda. Pseudoscience, such as polygraph testing, previously deemed by the American Medical Association as an unscientific game of “chance,” and psychometric testing of dubious validity are being used for confirmation of diagnoses.
They introduced and brought to market junk science like the Ethyl Glucuronide (EtG) biomarker for detecting alcohol use. The EtG was introduced by an FSPHP physician, marketed, and proselytized as an accurate and reliable test for alcohol. After setting an arbitrary cutoff of 100 to prove drinking he ruined countless careers and lives.
As the disaster toll increased it became clear the test was not very good. It became apparent the test was, in fact, very flawed and misguided as using an ultra sensitive poorly specific test for a substance environmentally ubiquitous precludes its forensic applicability.
Hand sanitizer, cosmetics, sauerkraut, and myriad other products were shown to result in an elevated EtG. Sensibly, the majority of drug testing and monitoring programs abandoned it. The market for the test decreased dramatically as the only customers left were drug monitoring programs in which the testers had absolute power and those being tested were absolutely powerless–programs like those run by the PHP.
This group has now introduced the Phosphatidylethanol (PEth) test as a confirmation test for EtG and USDTL marketed it as the PEthStat. State Physician Health Programs are now using the EtG and adding the PEth to confirm alcohol ingestion. And just as they did with the EtG the claims of reliability are grand but without foundation. All speculative A=B oversimplified thinking that ignores the myriad other factors involved. The science is empty if you remove the dregs of filler and puff. And the conflicts of interest are mind-boggling.
Corporate Front Groups and Corruption in Medicine-Forensic fraud, conflicts of Interest and the Erosion of Trust The ASAM and FSPHP are corporate front groups that have infiltrated organized medicine and gained tremendous sway. Advancing the multi-billion dollar 12-step rehab and drug testing industry agenda control has replaced conduct and ideology has trampled science and reason. As organizations without transparency, accountability, or regulation they have become reservoirs of bad medicine and corruption.
Accountability is rooted in organizational purpose and public trust. Unfortunately, humanitarian ideals have been trampled by the imposition of corporate front groups who advance hidden agendas under guises of science and scholarship and patinas of benevolence. Rife with conflicts of interest, these groups obfuscate, mislead, and exploit us to further an underlying political agenda. Healthcare and medicine has been infiltrated by various groups that pose a serious threat to both the humanitarian and evidence based aspects.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.” The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical Society updated its mission to read:
“The purposes of the Massachusetts Medical Society shall be to do all things as may be necessary and appropriate to advance medical knowledge, to develop and maintain the highest professional and ethical standards of medical practice and health care, and to promote medical institutions formed on liberal principles for the health, benefit and welfare of citizens of the commonwealth.”
With a foundation and history built and based on of scholarship and critical thought we need to support the highest levels of science, fact, intelligence and reason. Stupidity tries but it should not rein. Before the Boston Society for the Diffusion of Useful Knowledge in 1842, Dr. Oliver Wendell Holmes delivered two long lectures entitled “Homeopathy and Its Kindred Delusions.” He characterized one of its popular practitioners, Dr. Robert Wesselhoeft, as one of those:
“Emperics [quacks], ignorant barbers, and men of that sort…who announce themselves ready to relinquish all the accumulated treasure of our art, to trifle with life upon the strength of these fantastic theories.” That “pretended science” as Holmes called it, was “a mingled mass of perverse ingenuity, of tinsel erudition, of imbecile credulity, and artful misrepresentation, too often mingled in practice…with heartless and shameless imposition.”
And Holmes words are as apt and appropriate today as they were in mid 19th Century Boston! Probably more so.
History has recurrently proved that false constructs and groundless concepts allow for endless error.
The Massachusetts Medical Society needs to come to the realization that Physician Health Services is engaging in procedural, ethical and legal breaches. The evidence is clear that past medical director Dr. Luis Sanchez and Director of operations Linda Bresnahan are engaging in not only unethical but criminal activity within the walls of the MMS. Egregious misconduct including forensic fraud and political abuse of psychiatry can be seen in detail here, here and here.This is not a matter of opinion but a matter of fact. It has been ascertained by outside agencies and can also be confirmed by two former associate directors at PHS. What more does the MMS need? This type of misconduct can have grave and far reaching consequences for referred doctors and needs to be addressed urgently with precise, firm methods. To ignore the problem or suggest that it does not exist will only cause more damage.The majority of Massachusetts Medical Society members are honest, thoughtful and responsible. Most are unaware of the ethical and criminal allegations concerning PHS.. It is time they become aware as sunshine is the best disinfectant. As the most crucial step in solving a problem is admitting it exists I am requesting this be ascertained or refuted based on the documents and examined procedurally, ethically and legally. If there is no problem then the MMS should have no problem supporting or justifying the actions of Dr. Luis Sanchez, Dr. Wayne Gavryck and Linda Bresnahan. If the MMS cannot justify, support or defend these actions then it must be concluded that these individuals have violated professional protocol,, professional and community ethics and the law. And if that is the case it is the responsibility of the MMS to admit the problem exists, define it and address it. It is the responsibility of the MMS to facilitate exposure and that those engaged in wrongdoing be held appropriately accountable for their actions. I am sure no one at the MMS would disagree that forensic fraud be met with Zero-tolerance. The criminal and ethical violations shown here do not comport with any codes of conduct including those of the medical society. Those engaging in forensic fraud must be removed.
Good leadership requires correct moral and ethical behavior of both the individual and the organization. . Integrity is necessary for establishing relationships of trust. It requires a true heart and an honest soul. People of integrity instinctively do the “right thing” in any and all circumstances. Adherence to ethical codes of the profession is a universal obligation. It excludes all exceptions. Without ethical integrity, falsity will flourish.
The documentary evidence here shows fraud. It is intentional. All parties involved knew what they were doing, knew it was wrong but did it anyway. The schism between pious rhetoric and reality is wide.
One measure of integrity is truthfulness to words and deeds. These people claim professionalism, ethics and integrity. The documents show a reality of hypocrisy and sanctimony. But the hypocrisy seen here is also a danger because the careers and lives of doctors in Massachusetts are in these peoples hands.
As the oldest medical society in the United States the Massachusetts Medical Society can count some of the greatest minds in the history of American medicine as members. My how far we have fallen. This same author has previously unintelligibly compared the field of medicine to Barbra Streisand’s face and shamelessly and opportunistically blamed the Boston Marathon bombing on “marijuana withdrawal.”The sophomoric mnemonics are neither clever nor illuminating. Unworthy of Readers Digest circa 1957, this dumbing down of doctors needs to end. The very soul and practice of medicine is being castrated and lobotomized by the same dull and very very blunt instrument. How does one reconcile the fact that the very same medical society that publishes the New England Journal of Medicine is allowing this type of tripe and rabble to get past editorial review? In 1969, through an act of the state legislature, the Massachusetts Medical…
Good leadership requires correct moral and ethical behavior of both the individual and the organization. . Integrity is necessary for establishing relationships of trust. It requires a true heart and an honest soul. People of integrity instinctively do the “right thing” in any and all circumstances. Adherence to ethical codes of the profession is a universal obligation. It excludes all exceptions. Without ethical integrity, falsity will flourish.
The documents below show fraud. It is intentional. All parties involved knew what they were doing, knew it was wrong but did it anyway. The schism between pious rhetoric and reality is wide.
One measure of integrity is truthfulness to words and deeds. These people claim professionalism, ethics and integrity. The documents show a reality of hypocrisy and sanctimony. But the hypocrisy seen here is also a danger because the careers and lives of doctors are in these peoples hands.
Dr. Clive Body in his book Corporate Psychopaths writes that “Unethical leaders create unethical followers, which in turn create unethical companies and society suffers as a result.” And according to Dr. Robert Hare in Without Conscience “If we can’t spot them, we are doomed to be their victims, both as individuals and as a society. ”
Abuse under the utility of medical coloration is especially egregious. It violates the fundamental ethical principles of Medicine -Autonomy, Beneficence, Nonmaleficence and justice. Intentionally falsifying a laboratory or diagnostic test to refer for an evaluation or support a diagnosis or give unwarranted “treatment” is unconscionable.
Similar fraud is occurring across the country.
This is an example of the institutional injustice that is killing physicians. Finding themselves entrapped with no way out, helpless and hopeless they are feeling themselves bereft of any shade of justice and killing themselves. These are nothing more than bullies and accountability is essential.
Accountability, or answerability, is necessary to prevent abuse and corruption. This requires both the provision of information and justification for actions. What was done and why?
Professional guidelines and standards of care, ethical codes of conduct and the law are all objective benchmarks that can be used to assess the actions and decisions of others. In any free society this necessitates the existence of organizations of truly independent opinion capable of standing in this judgment.
State PHPs are Non-Governmental Organizations (NGOs) over which the state health department has no supervisory oversight. There is no regulation, no transparency and no accountability. There is no public scrutiny and they police themselves.
In Ethical and Managerial Considerations Regarding State Physician Health Programs Drs. John Knight and J. Wesley Boyd call for greater oversight and scrutiny of PHPs by the medical community at large. They recommended periodic auditing, national standards and regulation. They also attempted to convince the Massachusetts Medical Society to implement changes at PHS where they served as Associate Directors with over two decades of collective experience.
These efforts to promote transparency and accountability at both local and national levels, however, fell on deaf ears.
State PHPs have systematically removed those not conforming to groupthink. Threatening them with litigation if they breached “peer-review” statutes and confidentiality agreements has effectively silenced them from reporting any misconduct, abuse or even crimes they may have witnessed.
In Massachusetts John Knight was removed in 2009 and J. Wesley Boyd in 2010. In Ethical and Managerial Considerations Regarding State Physician Health Programs they comment “if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise—tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.” So too will the clinical laboratories.
How is this any different from the case of Dr. Farid Fata, the Michigan oncologist who intentionally diagnosed healthy patients with cancer so he could charge them for unneeded chemotherapy? The U.S. Attorney called it the “most egregious” case of health care fraud ever. His acts may have contributed to one patient death. The institutional injustice of the PHP system is causing countless deaths of physicians.
To consciously “tailor” a diagnosis is fraud. To tailor a diagnosis of substance use disorder or any other psychiatric diagnosis is the political abuse of psychiatry. Misrepresentation, dishonesty, deception, and distortion play no role in the Profession and Guild of Medicine. To do so violates the basic moral principles of Medical Ethics–Autonomy, Beneficence, Non-Maleficence and Justice.
The “PHP-approved” assessment and treatment centers are all staffed by doctors of “like-mind.” It is a rigged game.
An audit of the North Carolina PHP found essentially no oversight from the Medical Board or Medical Society. The audit found that “abuse could occur without being detected,” and this is by design. By removing and blocking the provision of information necessary for accountability, restricting the liberties and freedoms of physicians, and increasing their power and control they have erected a framework of hidden abuse.
While outspoken in denouncing what they regard as unethical and unprofessional behavior by other doctors, they are resistant to apply even the most minimal standards to their own activities.
To whom are the PHPs accountable? Whom do they represent? There are legitimate concerns.
















 But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.
But thanks to Sabin and Salk the last case of naturally occurring polio in the U.S. occurred in 1979.










 Accountability needs to be rooted in organizational purpose and public trust.
Accountability needs to be rooted in organizational purpose and public trust. ce of unchecked power. The only two factors that constrain corruption are moral virtue and deterrence.
ce of unchecked power. The only two factors that constrain corruption are moral virtue and deterrence. arketed it as the PEthStat.
State Physician Health Programs are now using the EtG and adding the PEth to confirm alcohol ingestion. And just as they did with the EtG the claims of reliability are grand but without foundation.
All speculative A=B oversimplified thinking that ignores the myriad other factors involved. The science is empty if you remove the dregs of filler and puff. And the conflicts of interest are mind-boggling.
arketed it as the PEthStat.
State Physician Health Programs are now using the EtG and adding the PEth to confirm alcohol ingestion. And just as they did with the EtG the claims of reliability are grand but without foundation.
All speculative A=B oversimplified thinking that ignores the myriad other factors involved. The science is empty if you remove the dregs of filler and puff. And the conflicts of interest are mind-boggling.