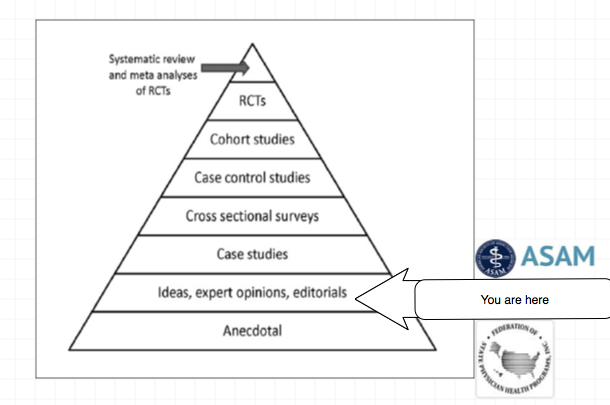
Anti-authoritarians question whether an authority is a legitimate one before taking that authority seriously. To evaluate the legitimacy of an authority it is necessary to:1. Assess whether they actually know what they are talking about. 2. Assess whether the authorities are honest in their intentions.When anti-authoritarians assess an authority to be illegitimate, they challenge and resist that authority.There is a paucity of anti-authoritarianism in the medical community concerning groups that have gained tremendous sway in the regulation of the medical profession. There is, in fact, an absence of anti-authoritarian questioning of what is essentially illegitimate and irrational authority.Most doctors are unaware of the impact these organizations have had on both the regulation of the medical profession and social control of individual doctors. Through “moral entrepreneurship” and “bent science” these groups have successfully swayed both policy-makers and the public to support an agenda not supported by reality testing or critical thinking. This acceptance without investigation has led to a deterioration of professional ethics and evidence-based decision making in the regulation of the medical profession. In order for these organizations to maintain power it is necessary that their authoritative opinion remain unquestioned and unchallenged. Consciously manufactured propaganda has persuaded regulatory and public opinion of their value and to maintain power it is necessary that this authority remain insulated from outside evaluation because the entire system is based on assumptions that can be aptly characterized as “illusions.The dogmatic statements and abusive generalizations do not conform to reality.Everything is adapted to an existing stagnant cognitive system that falls far off the map of the scientific approach to information and evidence based medicine. Perceiving only confirmations the physician health paradigm embodies and expresses preconceived ideas, values and mentalities based on certitude and absolute truth.
If one looks behind the curtain there is not much there.
Historical, political, economic and social analysis can all show how the construct that exists today came to be. This can be factually ascertained by simple reasoning and examination of the documentary evidence.
Any one of these analyses would reveal that the “PHP-blueprint” is a false-construct built on circumnavigation and obfuscation.
An evidence-based scrutiny of the literature would reveal it to be invalid and of little probative value. A public policy analysis would reveal the logical fallacies involved in trumpeting their positions including exaggerated rhetoric and fear monitoring strategies designed to inspire moral panics and exploit fears to further an underlying political agenda
Any critical analysis would reveal cherry picking. proof by anecdote, deceptive propaganda, double talk, contradictory, illogical and incomprehensible jabber, unprovable and un-disprovable statements and a panoply of logical fallacy.
These groups misrepresent, censor and suppress. They nit pick and split hairs. The concept of denial is not just used to force people into treatment and justify abuse during treatment but to suppress specific questions and deliberately avoid key facts.
So why are we not questioning this “authority?” They have been left alone and basically thrown in the backyard left to proliferate like feral cats.
We need anti-authoritarians and we need them now.
I need allies before the door closes for good. And that door may be closing a lot sooner than you think!
Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Although he specifies the numerical percentage “in physicians at 7.9%,”3 he avoids the use of numbers (14.6%) in the general population. He instead uses the qualifier “somewhat less.” Why is this?
My guess is because it understates the statistical fact that the prevalence found by Kessler in the general population was almost twice that found by Hughes in physicians.
You see, “Somewhat less” is a “detensifier.” It creates an impression of a small disparity between doctors and the general population.
In propaganda this is what is known as a “weasel phrase.” Weasel phrases are used to obfuscate the truth. Weasel phrases mislead those either without the time, or without the sense to see or look any deeper. The problem is it works.
“Methodologic differences may account for this difference,” Earley states, as the Hughes study “surveyed 9, 600 physicians by mail” and “relied on honest and denial-free reports by the physicians; the Kessler study utilized face-to-face interviews with trained interviewers.”1
This is an example of language framing. Language framing uses words and phrases to direct attention to a point of view to advance a vested interest.
In this case the use of the phrase “honest and denial free” in the context of physician reporting imparts associative meaning to the reader.
As denial is a recurring motif and cardinal attribute of physician addiction according to the paradigm, the connotation is that the reports by physicians may have been influenced by dishonesty and denial while face-to-face interviews done by “trained” interviewers were not.
“Framing” is another propaganda technique designed to tell the audience how to interpret the information given through context. The message here is that the somewhat less lifetime prevalence of substance abuse and addiction in physicians found by anonymous mail survey may be underreported as a result of both methodology and denial.
But in actual fact there is a large body of research regarding “social desirability bias” that shows the converse to be true.
One of the most consistent findings of studies of this kind is that socially desirable responding is significantly more likely with face-to-face administered data collection compared with self-administered anonymous modes.4-6
Tourangeau et al. reviewed seven studies comparing self-reports of drug use in surveys conducted in different modes. For each estimate obtained in the studies they calculated the ratio of drug use reported in self-reported surveys to the corresponding estimates in interviewer administered surveys and found that 57 of 63 different comparisons showed higher levels of reporting of drug use in the self-reported mode.7
The principal cause of social desirability bias is the level of perceived anonymity of the reporting situation.7
Evidence-based research does not support Earley’s claim that methodological differences in study design explain the difference in reported lifetime prevalence of substance abuse or addiction between physicians and the general population in these two studies.
Evidence based research would, in fact, make the findings more robust.
Moreover, I find it hard to comprehend the psychodynamics, motivation, and logic of denial and dishonesty in influencing an anonymous survey. So too would anyone else who dare peer beneath the veil. It is, in fact, a Potemkin village. In reality the emperor has no clothes.
Earley PE. Physician Health Programs and Addiction among Physicians. In: Ries R, Fiellin D, Miller S, Saitz R, eds. Principles of Addiction Medicine. 4 ed. Baltimore: Lippincott Williams & Wilkens; 2009:531-547.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Sudman S, Bradburn NM. Response effects in surveys: A review and synthesis. Chicago: Aldine Publishing; 1974.
Tourangeau R, Smith TW. Collecting sensitive information with different modes of data collection. In: Couper MP, Baker RP, Bethlehem J, et al., eds. Computer assisted survey information collection. New York: John Wiley & Sons, Inc.; 1998.
Dillman DA. Mail and telephone surveys: The total design method. New York: Wiley-Interscience; 1978.
Tourangeau R, Rips LJ, Rasinski KA. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000.
American Society of Addiction Medicine: Patient Placement Criteria. Chevy Chase, MD: American Society of Addiction Medicine; 2000.
Merlo LJ, Gold MS. Successful Treatment of Physicians With Addictions: Addiction Impairs More Physicians Than Any Other Disease. Psychiatric Times. 2009;26(9):1-8.
Physician Health Programs (PHP) claimed “gold standard” for addiction treatment. “80% success rate” being used to promote “new paradigm” to other populations.
PHPs are essentially Employee Assistance Programs (EAPs) for doctors. The vast majority of people know little or nothing about Physician Health Programs (PHPs).
Physician Health Programs (PHPs) are being called the “gold-standard” for EAPs. Claims of unparalleled success are being used to promote PHPs to other populations as a “replicable model of recovery.”
Drs. Robert Dupont and Gregory Skipper are promoting PHPs as “A New Paradigm for Long-Term Recovery” claiming an 80% success rate in doctors.
An article entitled “What Might Have Saved Philip Seymour Hoffman,” claims PHPs “ought to be considered models for our citizenry” and the “best evidence-based addiction treatment system we have going.” The author repeats the 80% success rate for doctors and claims Philip Seymour Hoffman might still be alive if he had been treated using the PHP model.
The basis for these claims is a 2009 study published in the Journal of Substance Abuse Treatment entitled Setting the Standard for Recovery: Physicians’ Health Programsand authored by Robert Dupont, A. Thomas McLellan, William White, Lisa Merlo and Mark Gold.
This study is the cornerstone of the “PHP-blueprint.” It is the very foundation on which everything else is based, a Magnum opus used to lay claim to supremacy that has been endlessly repeated and rehashed in a plethora of self-promotion and treatment community blandishment.
To date there has been no academic analysis of the “PHP-Blueprint.” There has been no Cochrane type analysis or critical review. There has been no opposition to its findings or conclusions which are paraded as fact and truth without challenge or question and there is a general lack of concern from those both within and outside the medical profession.
The Expansion of Physician Health Programs (PHPs) to Other Populations
1. Although these programs claim to help doctors they may actually be harming many and contributing to suicide.
2. The plan is to greatly expand these programs to other populations and you could be next.
In 2012 Robert Dupont delivered the keynote speech at the Drug and Alcohol Testing Industry Association annual conference and described a “new paradigm” for addiction and substance abuse treatment and proposed expansion of this paradigm to other populations including workplace, healthcare, and schools.
It is therefore critical that the “PHP-blueprint” be examined using critical reasoning and evidence base. All of this needs to be assessed in terms of legitimacy and intent.
The claim of 80% success rate in physicians is based on Setting the Standard for Recovery: Physicians’ Health Programsis unfounded. The study is a poorly designed using a single data set (a sample of 904 physician patients consecutively admitted to 16 state PHP’s).
It is non-randomized and non-blinded rendering the evidence for effectiveness of the PHP treatment model over any other treatment model (including no treatment) poor from a scientific perspective. The study contains multiple flaws in both reasoning (type I and type II errors) and statistical analysis that render its conclusions invalid.
In addition the impact of undeclared but substantial financial conflicts-of-interest (including funding by drug testing and addiction treatment industries) and personal ideological biases (including personal 12-step recovery from addictions) in the authors of this study also needs to be considered.
Moreover the misdiagnosis and over-diagnosis of addiction in physicians in this paradigm incentivized by lucrative self-referral dollars for expensive 90-day treatment programs is a significant factor.
False Endpoints and High Mortality Rate
The mean age of the 904 physicians was 44.1 years. They report that 24 of 102 physicians were transferred and lost to follow “left care with no apparent referral.”
What happened to them? These are physicians with multiple identifiers (state license, DEA, UPIN, etc) not transient drifters.
Of the 802 left in the program they report 155 failed to complete the contract. Of these, 48 involuntarily stopped or had their license revoked and 22 died with 6 of those being suicides. This study is looking at defined endpoints while being monitored so 6 killed themselves while being actively monitored by the program. But what about the 24 that left with no apparent referral? It is unlikely the just left on a whim. There must have been some precipitant event.
More importantly what happened to those 48 who were reported to the Medical Board for noncompliance and had their licenses revoked–that would be the critical time when this population would be at most risk for completing a suicide. That would be when hope was lost and the coerced physician, knowing that the fight was over, would take that step.
The outcomes they used were the last reported status of the PHP participant enrolled in the program. Measuring success of program completion in doctors compared to the general population is meaningless as the short-term outcomes are quite different in terms of the external consequences imposed. The consequence of not completing a PHP is the invariably career ending. So what happened to the 24 of who “left care with no apparent referral,” the 85 who “voluntarily stopped or retired,” and the 48 who “involuntarily stopped or license revoked.”
Whether you leave a PHP voluntarily, involuntarily, or with no apparent referral it is the end game and your career is over. Comparing this to other populations where the consequences of failing to complete the program are not so final is inappropriate. Claiming superiority over programs with a 40% success rate is unfounded because for most of those people the consequences are not so final and may mean nothing more than an increase in testing frequency.
The big question is what happened to the 157 physicians who left or stopped? How many of them killed themselves. With an average age of 44 there were 6 reported suicides 22 deaths, and another 157 no longer doctors. I would venture to say the number of suicides is a lot higher than they claim. But using the last recorded PHP status as the final outcome obfuscates this.
Due to the severity of the consequences a 20% failure rate is quite concerning. This is of particular concern because many doctors (if not most) monitored by PHPs are not addicts.
Imposed 12-step ideology and use of non-FDA Approved Drug and Alcohol Testing
As noted above, PHPs are essentially Employee Assistance Programs (EAPs) for doctors. Most EAPs, however, were developed in the presence of trade unions and other organizations working on behalf of the best interests of the employee. This collaborative effort led to EAPs that were more or less “organizationally just” with procedural fairness and transparency.
No such organizations exist for doctors. Due to the absence of oversight and accountability PHPs have been able to use non-FDA approved laboratory developed tests of unknown validity on doctors without any opposition.
The distinction between professional and private life as a fundamental value of our society and the importance of this boundary was also upheld by these groups.
In the PHP paradigm no procedural fairness or transparency exists and the boundary between professional and private life has eroded.
PHPs impose 12-step ideology on all doctors referred to these programs. State Medical Boards enforce this in violation of the Establishment Clause of the 1st Amendment yet there is little recourse for doctors as they are threatened with non-compliance and loss of licensure.
Selling the PHP Paradigm
The use of 12-step is most likely not ideologically driven but profit driven. Abstinence based 12-step programs justify the use of frequent drug and alcohol testing with ongoing lifelong assessment and treatment. As with drug-courts, PHPs provide a lucrative model to the drug and alcohol testing, assessment and treatment industry.
The plan to expand this to other populations is outlined in the ASAM White Paper.
This concerns all of us. The first step needs to be a critical appraisal ofSetting the Standard for Recovery: Physicians’ Health Programs, the foundation of their claims of an 80% success rate and a conflict-of-interest analysis of its authors. The legitimacy of the study and its claims needs to be questioned.
It does not take a Cochrane review to see that the emperor has no clothes. This is not difficult. It is straightforward and simple.
As an illegitimate and irrational authority it is necessary that this opinion remain unchallenged. We need to challenge it.
Historical, political, economic and social analysis reveals that the “PHP-blueprint” is a false-construct built on circumnavigation and obfuscation. An evidence-based scrutiny of the literature would reveal it to be invalid and of little probative value.
But if nobody speaks up it is inevitable that they will expand the “PHP blueprint” to other employee assistance programs and schools.
This is not just about doctors. You too are at risk for coercion, control, conformity and forced adherence to a lifetime of abstinence and 12-step indoctrination and if you do not speak up now it won’t be a risk but a certainty.
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
In order to comprehend the current plight of the medical profession and the dark clouds that lie ahead it is necessary to understand the history of the “impaired physician movement” and the American Society of Addiction Medicine (ASAM).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”1
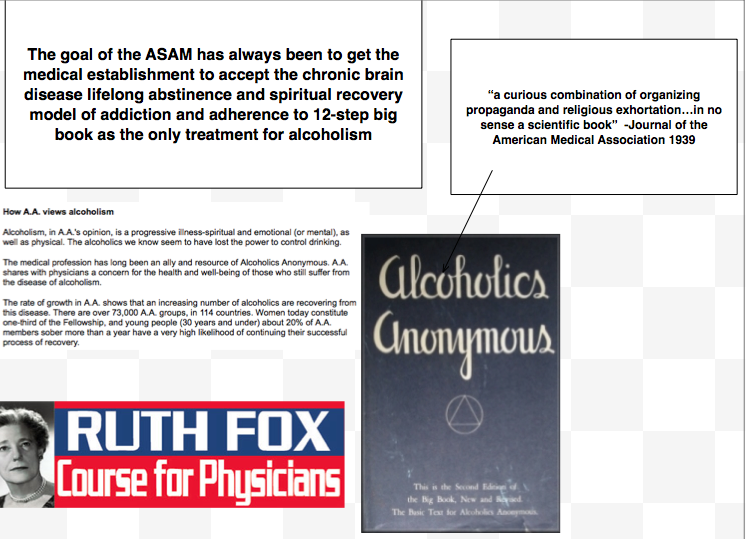
The impaired physician movement emphasizes disease and therapy rather than discipline and punishment and believes that addiction is a chronic relapsing brain disease requiring lifelong abstinence and 12-step spiritual recovery. The drug or alcohol abuser or addict is a person lacking adequate internal controls over his or her behavior; for his own protection as well as the protection of society external restraints are required including involuntary treatment.
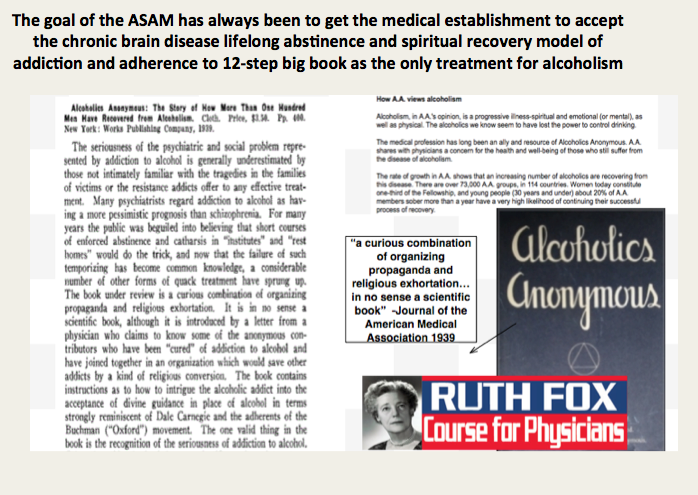
The American Society of Addiction Medicine (ASAM) can trace its roots to the 1954 founding of the New York City Medical Society on Alcoholism (NYCMSA) by Ruth Fox, M.D whose husband died from alcoholism.
Finding that alcoholics in her psychoanalytic practice did not recover when she used conventional analytic approaches, she taught her patients about alcoholism as a disease and introduced “them to AA meetings held in her living room.”2
A number of physicians in the New York Medical Society were themselves recovering alcoholics who turned to Alcoholics Anonymous for care.3
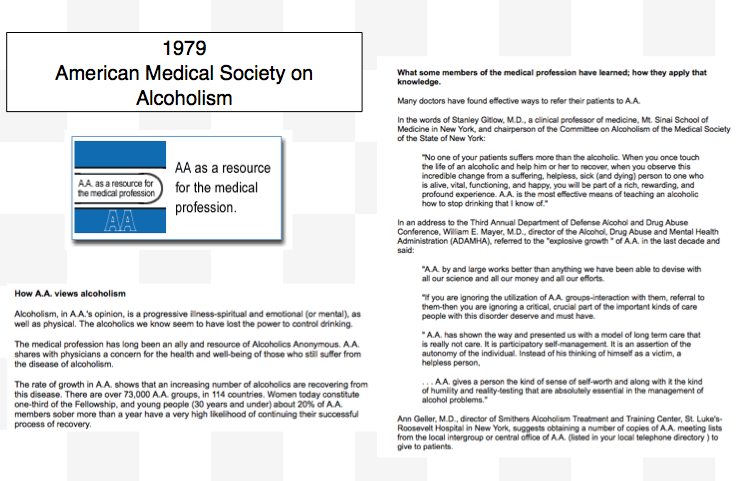
The society, numbering about 100 members, established itself as a national organization in 1967, the American Medical Society on Alcoholism (AMSA).3
The group promoted the concept of alcoholism as a chronic relapsing disease requiring lifelong spiritual recovery through the 12-steps of AA.
In 1973 AMSA became a component of the National Council on Alcoholism (NCA), now the National Council on Alcoholism and Drug Dependence (NCADD) in a medical advisory capacity until 1983.
“Abstinence from alcohol is necessary for recovery from the disease of alcoholism” became the first AMSA Position Statement in 1974.2
In 1985 ASAM’s first certification exam was announced. According to Dr. Bean-Bayog, chair of the Credentialing Committee:
“A lot of people in the alcoholism field have long wanted physicians in the field to have a high level of skills and scientific credibility and for this body of knowledge to be accredited.”2
And in 1986 662 physicians took the first ASAM Certification Exam.
By 1988 membership was over 2,800 with 1,275 of these physicians “certified” as:
“having demonstrated knowledge and expertise in alcoholism and other drug dependencies commensurate with the standards set forth by the society.”4
“While certification does not certify clinical skill or competence,” the Board explained, “it does identify physicians who have demonstrated knowledge in diagnosis and treatment of alcoholism and other drug dependencies.”5
Somehow, I don’t think this is quite what they had in mind!
Achieving “recognized board status for chemical dependence” and fellowships in “chemical dependency” are among the five-year objectives identified by the group. These are to come to fruition by “careful discussion, deliberation, and consultation” to “determine its form and structure and how best to bring it about.”5
The formation of ASAM State Chapters begins with California, Florida, Georgia, and Maryland submitting requests.6
In 1988 the AMA House of Delegates votes to admit ASAM to the House. According to ASAM News this “legitimizes the society within the halls of organized medicine.”2
In 1989 the organization changes its name to the American Society of Addiction Medicine (ASAM).2
Since 1990, physicians have been able to list addiction medicine as a self-designated area of practice using the specialty code “ADM.”
By 1993 ASAM has a membership of 3,500 with a total of 2,619 certifications in Addiction Medicine.
The Membership Campaign Task Force sets a goal to double its membership of 3,500 to 7,000 by the year 2000 to assure “the future of treatment for patients with chemicals. It represents a blueprint for establishing addiction medicine as a viable entity.”7
Ninety physicians become Fellows of the American Society of Addiction Medicine (FASAM) in 1996 “to recognize substantial and lasting contributions to the Society and the field of addiction medicine.”8
Among the honorees are Robert DuPont, G. Douglas Talbott, Paul Earley, and Mel Pohl. In addition to at least five consecutive years of membership and certification by the Society, Fellows must have “taken a leadership role in ASAM through committee service, or have been an officer of a state chapter, and they must have made and continue to make significant contributions to the addictions field.”8
The American Board of Addiction Medicine (ABAM) is formed in 2007 as a non-profit 501(C)(6) organization “following conferences of committees appointed by the American Society of Addiction Medicine” to “examine and certify Diplomats.”9
In 2009 National Institute on Drug Abuse (NIDA) Director Nora Volkow, M.D., gives the keynote address at the first ABAM board certification diploma ceremony.10
According to an article in Addiction Professional “Board certification is the highest level of practice recognition given to physicians.”
“A Physician membership society such as ASAM, however, cannot confer ‘Board Certification,’ ” but a“ “Medical Board such as ABAM has a separate and distinct purpose and mission: to promote and improve the quality of medical care through establishing and maintaining standards and procedures for credentialing and re-credentialing medical specialties.”
The majority of ASAM physicians meet these requirements by “working in a chemical dependency treatment facility, taking continuing medical education courses in addiction, or participating in research.”11
“In the United States accredited residency programs in addiction exist only for psychiatrists specializing in addiction psychiatry; nonpsychiatrists seeking training in addiction medicine can train in nonaccredited ‘fellowships,’ or can receive training in some ADP programs, only to not be granted a certificate of completion of accredited training.”11
Specialty recognition by the American Board of Medical Specialties, fifty Addiction Medicine Fellowship training programs and a National Center for Physician Training in Addiction Medicine are listed as future initiatives of the ABAM Foundation in 2014.
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers, and consumers of health care products, and the general public’12
In this they have succeeded.
And in the year 2014 G.V. Stimson’s characterization of the “impaired physician movement” remains as accurate and apt as it was in 1985. But the “number of evangelical recovered alcoholic and addict physicians” has increased dramatically (outnumbering Addiction Psychiatry by 4:1) and their involvement in “ medical society and treatment programs” has been realized and enforced through the state Physician Health Programs and their “PHP-approved’ assessment and treatment centers.
Their“ability to make authoritative pronouncements on physician impairment…based on their own claim to insider’s knowledge” has become public policy and sanctified by Regulatory Medicine -essentially the Word of the Lord.
And the 1953 Alcoholics Anonymous prophecy that “With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world” is also coming to pass.
Stimson GV. Recent developments in professional control: the impaired physician movement in the USA. Sociology of health & illness. Jul 1985;7(2):141-166.
Four Decades of ASAM. ASAM News. March-April 1994, 1994.
Freed CR. Addiction medicine and addiction psychiatry in America: Commonalities in the medical treatment of addiction. Contemporary Drug Problems. 2010;37(1):139-163.
. American Medical Society on Alcoholism & Other Drug Dependencies Newsletter. Vol III. New York, NY: AMSAODD; 1988:12.
Ursery S. $1.3M verdict coaxes a deal for doctor’s coerced rehab. Fulton County Daily Report. May 12, 1999b 1999.
. AMSAODD News. Vol III. New York, NY: American Medical Society on Alcoholism & Other Drug Dependencies; 1988.
Membership Campaign Update. ASAM News. Vol VIII: American Society of Addiction Medicine; 1993:11.
. ASAM News. Vol 12. Chevy Chase, MD: American Society of Addiction Medicine; 1997:20.
Tontchev GV, Housel TR, Callahan JF, Kunz KB, Miller MM, Blondell RD. Specialized training on addictions for physicians in the United States. Substance abuse : official publication of the Association for Medical Education and Research in Substance Abuse. Apr 2011;32(2):84-92.


 To evaluate the legitimacy of an authority it is necessary to:
To evaluate the legitimacy of an authority it is necessary to:
 The dogmatic statements and abusive generalizations do not conform to reality.
The dogmatic statements and abusive generalizations do not conform to reality.
 The concept of denial is not just used to force people into treatment and justify abuse during treatment but to suppress specific questions and deliberately avoid key facts.
The concept of denial is not just used to force people into treatment and justify abuse during treatment but to suppress specific questions and deliberately avoid key facts.






 As an illegitimate and irrational authority it is necessary that this opinion remain unchallenged. We need to challenge it.
As an illegitimate and irrational authority it is necessary that this opinion remain unchallenged. We need to challenge it.