



The Plan to introduce non-FDA approved drug and alcohol tests into the Healthcare system and require doctors drug-test ALL PATIENTs including students and kids!

The ASAM plans to introduce non-FDA approved “forensic” Laboratory Developed Tests (LDTs) into mainstream healthcare via a loophole. This same group introduced most of these tests through a loophole and now they want to drug-and alcohol TEST EVERYBODY including STUDENTS AND KIDS through another loophole! These tests are of unknown reliability and accuracy. The LDT pathway does not even require proof that the test is even valid (i.e. that the test is actually testing for the substance it claims to be testing) but with no FDA oversight or regulation the labs can claim anything they want in marketing it and they do.
If a doctor collects a test on a “patient” the test is rendered “clinical” rather than “forensic” and by deeming this drug-testing “clinical” rather than “forensic” they can…
View original post 92 more words
Share this:

The Elephant in the Room: Physician Suicide and Physician Health Programs
The Elephant in the Room: Physician Suicide and Physician Health Programs.

Accountability is rooted in organizational purpose and public trust. Unfortunately, humanitarian ideals have been trampled by the imposition of corporate front groups who advance hidden agendas under guises of science and scholarship and patinas of benevolence. Rife with conflicts of interest, these groups obfuscate, mislead and exploit us to further an underlying political and corporate agenda. Healthcare and medicine has been infiltrated by various groups that pose a serious threat to both the humanitarian and evidence based aspects.


Share this:

Physician Health Programs: The Need for Integrity and Accountability of Organizations
Accountability, or answerability, is necessary to prevent abuse and corruption. This requires both the provision of information and justification for actions. What was done and why?
Professional guidelines and standards of care, ethical codes of conduct and the law are all objective benchmarks that can be used to assess the actions and decisions of others. In any free society this necessitates the existence of organizations of truly independent opinion capable of standing in this judgment.
State PHPs are Non-Governmental Organizations (NGOs) over which the state health department has no supervisory oversight. There is no regulation, no transparency and no accountability. There is no public scrutiny and they police themselves.
In Ethical and Managerial Considerations Regarding State Physician Health Programs Drs. John Knight and J. Wesley Boyd call for greater oversight and scrutiny of PHPs by the medical community at large. They recommended periodic auditing, national standards and regulation. They also attempted to…
View original post 413 more words
Share this:

“Doctors reporting crimes are turned back over to the very perpetrators of the crimes” — Dr. Michael L. Langan
“Doctors reporting crimes are turned back over to the very perpetrators of the crimes. The Medical Societies and professional organizations contribute to the problem by willful ignorance. Accusations are used to disregard the claims of the accused.” (1)
This quote describes exactly what happens to me.(2-8) I was reporting crimes and then delivered back to the criminal perpetrators, forced psychiatric treatment was prescribed by political abusers of psychiatry. This unethical act has been kept in secret and it have not been described by the official University records. Events that were executed by a member of the directive board at Universidad del Valle (the vice-dean of research: Mauricio Palacios Gomez).(9)
References
- Michael L. Langan. Bent Science and Bad Medicine: The Medical Profession, Moral Entrepeneurship and social control.
http://disruptedphysician.com/2015/02/28/bent-science-and-bad-medicine-the-medical-profession-moral-entrepreneurship-and-social-control/ - Jorge H. Ramírez. “Me gusta cuando callas porque estas como ausente” (no answers yet).
http://chaoticpharmacology.com/2015/03/02/me-gusta-cuando-callas-porque-estas-como-ausente-no-answers-yet/ - Jorge H. Ramírez. The Universal Declaration of Human Rights:…
View original post 88 more words
Share this:

Without Dr. William Morgan the 2004 Red Sox World Series win would not exist–a true Boston Hero

The essay below found on 123HelpMe.com called The “Doctor Who Saved Boston.” is about Dr. William J. Morgan, the brilliant hand surgeon who helped the Red Sox win the World Series for the first time in 86 years. Morgan performed surgery on Curt Schilling’s severely damaged ankle that allowed him to pitch in game 6 of the ALCS against the Yankees when we were down three games to two.
No known medical or surgical options existed to allow Schilling the functionality to pitch. But just as things were looking bleak Dr. Morgan miraculously performed an unprecedented procedure he invented that allowed Schilling to pitch seven innings winning the game 4-2. He created a wall of stitches to hold Schillling’s torn tendon sheath in place before game 6’s win and again before game 2 of the World Series that we also won.
And October 27. 2004 is a magical date for red sox fan. Watching it unfold with my…
View original post 2,882 more words
Share this:

The Medical Profession under Dictatorship–Revisiting Dr. Leo Alexander’s prescient warnings from 1949
“Let it be considered, too, that the present inquiry is not concerning a matter of right, if I may say so, but concerning a matter of fact.”–Adam Smith
“Most men endure the sacrifice of the intellect more easily than the sacrifice of their daydreams. They cannot bear that their utopias should run aground on the unalterable necessities of human existence” -Ludwig von Mises
The guiding philosophic principle is Hegelian or “rational utility” and “corresponding doctrine and planning”, Alexander said “replaced moral, ethical and religious values” and Nazi propaganda was highly effective in perverting public opinion and public conscience. He explains how this expressed itself in a rapid decline in standards of professional ethics in the medical profession. This all “started from small beginnings” with subtle shifts in the attitudes of physicians to accept the belief that there is such a thing as “a life not worthy to be lived.”
In 1985 the British Sociologist G.V. Stimson wrote of a new form of professional control in the United States that had emerged in the preceding decade whose “success rests on the ability to take certain areas of conduct such as alcoholism and drug abuse (which are formally disciplinary issues) and handle them as diseases.”2
Stimson writes:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”2
Among these authoritative pronouncements was the use of specialized treatment centers. Many professionals were critical of these programs including Assistant Surgeon General John C. Duffy who criticized the “boot-camp mentality”4 toward doctors and American Society of Addiction Medicine President Leclair Bissel who when asked in a 1997 interview when the field began to see physicians as a specialized treatment population replied “when they started making money..” .” 5
Amid reports of abuse, coercion and control in facilities using a doctor’s medical license as “leverage,” the Atlanta Journal Constitution ran a series of reports in 1987 documenting the multiple suicides of health care practitioners at one of these programs (5 while in the facility and at least 20 after discharge).6 Neither these suicides nor a large settlement against the same facility (finding a non-alcoholic doctor was intentionally misdiagnosed as an alcoholic and forced into months of treatment) for fraud, malpractice, and false imprisonment involving intentional misdiagnosis7 generated any interest among the medical community at large.
And by 1995 the door had closed as the Federation of State Physician Health Programs ( FSPHP ) relationship with the Federation of State Medical Boards (FSMB), the national organization responsible for the licensing and discipline of doctors, was forged. A 1995 issue of The Federal Bulletin: The Journal of Medical Licensure and Discipline, contains articles outlining the high success rates of these programs in 8 states with an editorial comment from the FSMB that concludes:
“cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.”8
The Federation of State Medical Boards (FSMB) has approved any and all policy and regulation put forth by the impaired physician movement then organized under the Federation of State Physician Health Programs (FSPHP) with no apparent inquiry or opposition.
In 2003 Dr. Gregory Skipper, one of the key players of the impaired physician movement partnered with NMS labs to develop the alcohol metabolite ethyl-glucuronide (EtG) as a laboratory developed test13 14 he proposed be used as a monitoring tool for covert alcohol use in physicians after a pilot study involving just 14 psychiatric inpatients.15
The policy entrepreneurship this group so effectively uses to advance their goals can be seen in the August 25, 2004 Journal of Medical Licensure and Discipline which contains articles both presenting the problem 11 and providing the solution.11 The EtG was then introduced as an accurate and reliable indicator of covert alcohol use and the impact of this cannot be underestimated as it introduce to the market not only unregulated non FDA approved tests for forensic use but tests reaching further back into history then those used by workplace drug-testing programs.
The limitations of any test needs to be understood both in the forensic and clinical context but there is a lot less flexibility in the forensic context when people’s liberties, freedoms or property rights ( as with a medical license) are in jeopardy.
Sensitivity and specificity need to be carefully considered. The positive predictive value of a test is the true positives over the true positives plus false positives. If you are going to sanction somebody as a result of a single test that test needs to have 100% sensitivity.
When workplace drug testing was introduced debates over both the accuracy and scope of tests occurred. The employees right to privacy and the employers right to have a drug-free workplace were discussed with the general consensus being testing for impairment was a legitimate concern but preservation of private life should remain.
What was done here dissolves both.
PHP programs require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring abstinence from drugs and alcohol while using non-FDA approved Laboratory Developed Tests in monitoring programs is a dangerous combination. The suicides reported by the Atlanta Journal Constitution in 1987 were prior to the introduction of these tests. Adding these tests of unknown validity to an already abusive program of coercion and control would only worsen the situation.
I have been hearing of multiple suicides involving both the fear of results and false results. I have also been hearing of doctors who have killed themselves because they were suffering from depression but did not seek help as their fear of being ensnared into the PHP outweighed the need to get help.
Three decades after G.V. Stimson so accurately defined the impaired physician movement the impaired physician movement defines the professional control of medicine.. Their involvement in medical society physician health programs (PHPs) and treatment programs has evolved into absolute control of both. Pronouncements on physician impairment have evolved from insider’s claims to written edict. And their reach has extended from impairment due to drugs and alcohol to “potential impairment” and “relapse without use.” Their reach has extended from drug and alcohol impairment to all other aspects of medicine and the impact has been profound. Medicine has been subordinated to the guiding philosophy of the impaired physician movement and doctors are dying in droves du to institutional injustice.
How does the profession of medicine reconcile the fact that we have allowed an as yet non ABMS recognized “self-certification” specialty full reign over those who are ABMS recognized? How is it that we allow non-FDA approved Laboratory Developed Tests (LDTs) of unknown validity on doctors coerced into state Physician Health Programs (PHPs)? A recent debate in Washington calling for regulation of “clinical” LDTs just took place and the fact that they are being used for “forensic” purposes in doctors is incomprehensible. Has anyone noticed it is the same people introducing the tests who are claiming PHPs are the “gold standard,” trying to push them on other EAPs and calling for more widespread use of these tests?
The use of non-FDA approved Laboratory Developed Tests (LDTs) for drug and alcohol testing is currently limited to PHPs and the criminal justice system. (i.e. monitoring programs in which those doing the testing have power and those being tested have no power). That may soon change. See Drug Testing and the Future of American Drug Policy and The American Society of Addiction Medicine White Paper on Drug Testing describing the plans for widespread expansion of this drug testing to other groups including kids.
Those involved in the Massachusetts General Hospital Laboratory Medicine, Toxicology and addiction medicine departments looked critically at these tests and decided hands down against using them. Why? Because no evidence base exists and the potential harm far outweighs any perceived benefit. “Research” has been done on those being monitored by PHPs and the criminal justice system and Drs. J Wesley Boyd, M.D., PhD, and John Knight, M.D. of Harvard Medical School who collectively have over two decades of experience as Associate Directors with the Massachusetts PHP, Physician Health Services, Inc. addressed this research in a 2012 article published in the Journal of the American Society of Addiction Medicine entitle Ethical and Managerial Considerations Regarding State Physician Health Programs. The allegations that PHPs are engaging in research in violation of the Nuremberg code ( that was a direct result of the Nuremberg trials for which Dr. Alexander acted as consultant ) should have raised some eyebrows. It hasn’t.

What do you think will happen when ASAM gets recognized by the ABMS in 2 years as is expected? These “addiction medicine” specialists will inevitably join hospital formulary , clinical lab, toxicology and ethics panels to do the same thing they have done to get where they are today. They will do the same thing they have done with state PHPs. Those with a hidden agenda will be able to outvote those of good conscience and thoughtful intelligence and patient care will then be subordinated to the guiding philosophy of the impaired physicians movement.
This system of institutional injustice is killing doctors by suicide as the medical societies and Departments of Public Health have given PHPs full autonomy and authority and it is poised to impact patient care.
I challenge you to name any other company, organization, group or agency within or related to the profession of medicine and the field of science that is bereft of absolutely all transparency, regulation or oversight? It does not exist.
The PHP scaffold has deliberately removed themselves from all aspects of accountability including answerability, justification of actions and the ability of outside actors to hold them in judgment of any information provided by answerability. Heads I win, tails you lose. That is a big red flag in itself. and those not currently being held accountable they may very well be after you next as their plans include expansion to other groups includes EAPs, the Department of Transportation, athletes, students and even kids!
Doctors are afraid to talk about this for fear of being ensnared themselves. Those already in these programs will not speak for fear of punishment. This is a legitimate concern and needs to be discussed openly and publicly. I need allies!
Help me get the word out –too many doctors are dying. Three died by suicide in one month alone who were being monitored by the Oklahoma PHP and these suicides did not even make the local papers let alone national news! They need to.
In The Argument of Fascism Ludwig von Mises wrote:
It cannot be denied that Fascism and similar movements aiming at the establishment of dictatorships are full of the best intentions and that their intervention has, for the moment, saved European civilization. The merit that Fascism has thereby won for itself will live on eternally in history. But though its policy has brought salvation for the moment, it is not of the kind which could promise continued success. Fascism was an emergency makeshift. To view it as something more would be a fatal error.
Share this:

Gay Doctor coerced by Physician Health Program (PHP) into mandated 12-step treatment and monitoring for sex addiction: The slippery slope begins
The civil and human rights violations remain hidden. The crimes remain hidden. So too will this. It appears the FSPHP is following the same pattern they have with the “impaired” and “disruptive” physicians–to discriminate. The targeting of gay, lesbian or transgender doctors for what they do in their private lives is predictable. I just heard from one of these doctors who was told by the PHP that if he did not cooperate with them in addition to losing his medical license the state medical board would make his sexual history part of the public record and available on their website!
It is an inevitable part of this well oiled slope of coercion, control, obedience and abuse.The import of this can not be overestimated.
Share this:

Gay Doctor coerced by Physician Health Program (PHP) into mandated 12-step treatment and monitoring for sex addiction: The slippery slope begins

State Physician Health Programs -coercion, control and abuse.
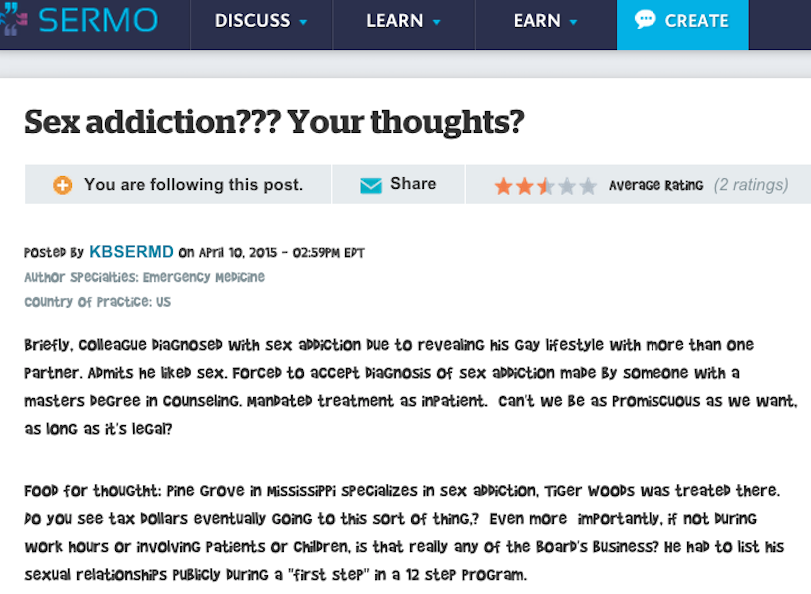
This anecdote concerning a gay doctor’s revelation he liked his non monogamous lifestyle leading to a forced acceptance of a “sex addiction” diagnosis, mandatory inpatient treatment and indoctrination into 12-step recovery was just posted on the physician social network SERMO. If the pattern looks familiar it is.
Physician Health Programs (PHPs) are non-profit NGOs that exist in every state ostensibly to help impaired doctors and protect the public from harm. PHPs have no regulation or oversight and have essentially removed all accountability. Under the ruse of protecting a doctors anonymity and providing confidentiality they have built barriers of opacity. Most doctors are unaware how they work unless they become involved with them and they are not on the radar of the public at large–they need to be.
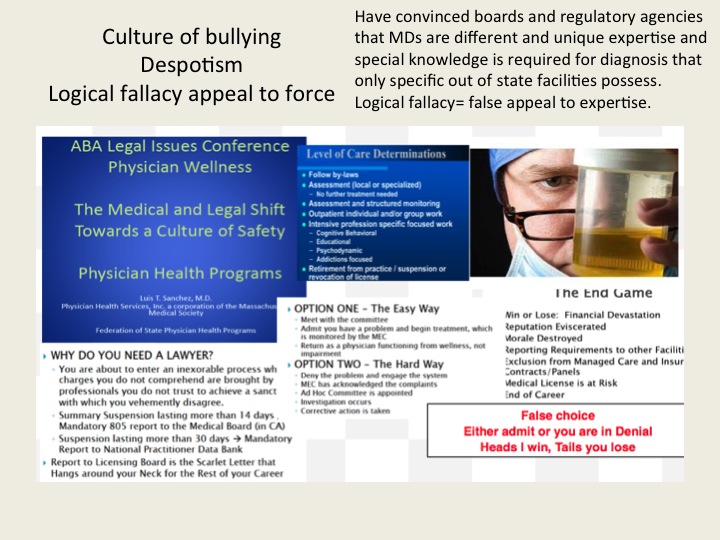
Organized under the Federation of State Physician Health Programs, (FSPHP), state medical boards have abdicated their responsibility and consider them expert authority on all things related to physician health–a logical fallacy that has placed illegitimate and irrational authority in professional control of medicine once again proving that knowledge isn’t power and ignorance often reigns.
PHPs encourage confidential referrals for “warning signs” such as those on the list below from the Massachusetts PHP, PHS, Inc. and guarantee the reporters anonymity. All semblance of due process has been removed. Medical boards have given state PHPS complete and absolute managerial control over assessment, treatment and monitoring. PHPs are not healthcare providers but monitoring agencies. If a PHP recommends an “assessment” of a reported doctor there is no choice in the matter. No allowances for a second opinion, outside support or appeal exist.
This doctor was apparently reported to his state PHP because a patient thought she smelled alcohol on his breath. As it turned out, the accusation was bogus but by being honest and forthcoming about his sexual orientation in the interview the PHP mandated an “assessment.” for unrelated issues. A not uncommon scenario as reports of behavioral issues often end up with hair tests for alcohol and other substances resulting in mandated assessments for “substance use disorder” followed by a five-year monitoring contract with the PHP and weekly urine tests.
The PHP provides a list of three or four facilities drawn from the same pool of “PHP-approved” assessment and treatment centers. However, an audit of the N.C. PHP found no written objective criteria or quantitative measurements existed on how these assessment and treatment centers are “approved” by the PHP. The common denominator seems to be that these facilities are (1) 12-step ASAM directed, and (2) willing to “tailor” an assessment to support a predetermined diagnosis. It is, in fact, a rigged game. Unfortunately the medical boards have been duped into mandating assessments at these centers under threat of loss of medical license and specifically exclude non “PHP-approved” assessments.
This scaffold is also the unspoken and hushed major contributor to physician suicide—It is the elephant in the room no one speaks of out of fear of being targeted. Doctors who really need help for mental health, substance abuse or other issues are afraid to get it for fear of being reported to the PHP. Those already monitored are subject to all sorts of psychological, financial and emotional abuse.
The Federation of State Physician Health Programs (FSPHP) has a relationship with Pine Grove. It is one of the “PHP-approved” facilities and two of their staff, Phillip Hemphill, PhD and James C. “Jes” Montgomery, MD are are listed as Program Faculty at the FSPHP annual educational conference and business meeting on April 24-27, 2015 in Fort Worth Texas.

Political Abuse of Psychiatry
Political abuse of psychiatry is the “misuse of psychiatric diagnosis, detention and treatment for the purposes of obstructing the fundamental human rights of certain groups and individuals in a society. The coercive use of psychiatry represents a violation of basic human rights in all Cultures.
What has occurred in the medical profession is no different from China or the Soviet Union under totalitarian rule where dissent is disapproved, often punished, and those perceived as threats to the existing system can be effectively “neutralized with trumped up psychiatric illness” and by this stigmatization reputations were ruined, power was diminished, and voices were hushed.

Political abuse of psychiatry involves the deliberate action of diagnosing someone with a mental condition they do not have as a means of repression or control and if you do not believe it is occurring right here today then take a look here and here to see how they are colluding with commercial drug testing companies to engage in forensic fraud and the assessment and the treatment centers to fabricate data to support non-existent diagnoses.
“Sex Addiction” used as a tool to Discriminate
There has been a lot of “chatter” in PHP circles concerning “sex addiction” and I knew they had been aligning themselves and setting up specialized programs at certain facilities. It seemed unusual as many of the key players who erected and run this scaffold have themselves been involved in sexual misconduct. 

One of the architects of the current system, Dr. Robert Walzer, M.D., J.D. who was instrumental in tinkering with administrative and medical practice laws to remove the due process and appeal rights of doctors surrendered his license in 2001 due to inappropriate sexual relationships with patients. He was the co-author of the current physician health program paradigm.
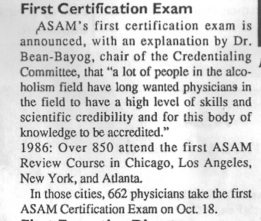
Dr. Margaret bean-Byog, M.D, Chairman of the credentialing  committee for the first certification exam and ASAM president surrendered her medical license after being accused of sexually abusing one of her patients, a Harvard medical student who subsequently died by suicide.
committee for the first certification exam and ASAM president surrendered her medical license after being accused of sexually abusing one of her patients, a Harvard medical student who subsequently died by suicide.
 And the FSPHP seems to treat doctors involved in sexually related misconduct in a favorable light. Take for instance, Dr. James Peak, M.D., a child psychiatrist who was sent to prison on a federal child pornography conviction taken under the wing of the Montana PHP. After “proving” he only ‘”looked” at pornography of young boys but never abused any using a polygraph “lie-detector” test his license was reinstated in no time at all. His treatment includes going to one AA meeting and one 12-step sex addict meeting per week. My guess is they need more staff at the PHP or one of the assessment centers.
And the FSPHP seems to treat doctors involved in sexually related misconduct in a favorable light. Take for instance, Dr. James Peak, M.D., a child psychiatrist who was sent to prison on a federal child pornography conviction taken under the wing of the Montana PHP. After “proving” he only ‘”looked” at pornography of young boys but never abused any using a polygraph “lie-detector” test his license was reinstated in no time at all. His treatment includes going to one AA meeting and one 12-step sex addict meeting per week. My guess is they need more staff at the PHP or one of the assessment centers.
I had been wondering what the motivation was behind this focus on “sex addiction” and my suspicions seem to be correct.
I have since heard of a second case of a gay doctor being forced into his state Physician Health Program (PHP) in Alabama.
Once under the control of the PHP most doctors are afraid to come forward because of the “swift and certain” consequences imposed on them. All they have to do is say the doctor was “noncompliant” to the medical board and it is over. They lose their license and there is not a thing they can do about. it. I have heard from doctors in multiple states going to law enforcement, the Attorney General, the media and the ACLU only to have the door slammed in their faces. Myself included. .
The coercion, control, ethics, and civil and human rights violations remain hidden. The crimes remain hidden. So too will this.
It appears the FSPHP is following the same pattern they have with the “impaired” and “disruptive” physicians–to discriminate. The targeting of gay, lesbian or transgender doctors for what they do in their private lives is predictable. It is an inevitable part of this well oiled slope of coercion, control, obedience and abuse.
The import of this can not be overestimated.
References:
Position Statement on Political Abuse of Psychiatry. Paper presented at: Global Initiative on Psychiatry2005.Birley JL.
Political abuse of psychiatry. Acta psychiatrica Scandinavica. Supplementum. 2000;399:13-15.

Share this:

Institutional Justice and Quality Disparity in Drug and Alcohol Monitoring–The Contrast Between MBTA Operators and Massachusetts Doctors is Shocking

In Backfire Step 1: Expose the Injustice–Forensic Fraud being committed by PHPs in Collusion with Corrupt Labs, I used documentary evidence from my own case to show how the PHPs and labs are engaging in undeniable and indefensible forensic fraud. The documents speak for themselves and it does not take a toxicologist or Medical Review Officer to understand that “Updating” a “chain-of-custody”and adding a new ID # to an already positive test breaches all procedural and professional guidelines, medical and societal ethics and state and federal law. It exemplifies how PHPs are blocking the “provision of information” required by most substance of abuse testing programs. Whereas most substance of abuse testing guidelines require not only answerability but “timely” answerability, PHPs use tactics that block and delay such information. These tactics include both refusing to provide the information and dissuading those monitored from requesting it.
In my case it took 5 months to obtain the “litigation packet” (a documentary record generated on any and all “forensic” drug and alcohol testing that records the “chain-of-custody” from initial collection to final analysis. The litigation packet I received in December of 2011 from a test collected by Quest Diagnostics can be seen here: USDTL Litigation Packet.
If you take a look at it you will see that no documentation exists regarding the specimen from when it was collected July 1st, 2011 to when it was reported as positive on July 19th, 2011 by Dr. Luis Sanchez, Medical Director of the Massachusetts PHP, Physician Health services, inc. (PHS). There is, in fact, absolutely no external chain of custody documenting the collection, handling and transport of the specimen. This in itself, according to each and every guideline ever published in the history of forensic testing invalidates the test.

But more importantly, the litigation packet revealed evidence that the reported positive test was not the result of oversight or accident but deliberate and intentional–forensic fraud by fax. Although this laboratory misconduct and fraud is undeniable and indefensible PHPs have no oversight or regulation. Neither do the labs.
Most individuals being tested for substances of abuse by employee assistance programs have a union or some other organization protecting their best interests. In the case of a suspected fraudulent or mishandled test these groups facilitate accountability by helping to obtain the information and requesting justification of actions. No such agencies exist for those being monitored by PHPs. No avenue of complaint against PHPs exist. In addition to no FDA oversight, “forensic” LDTs (unlike clinical LDTs) are exempt from Clinical Laboratory Improvement Amendments of 1988 (CLIA). The only avenue of complaint against a lab utilizing forensic LDTs is through the College of American Pathologists (CAP). As an accreditation agency, however, they are limited in what they can do as a result of an investigation. Whether the complaint involves accidental lab error or intentional fraud the only action CAP can take at the conclusion of an investigation is to threaten the lab with loss of accreditation if the lab does not come into compliance with their “Forensic Drug Testing Checklist.” They can also force the lab to “correct” these tests under threat of loss of accreditation. This is what CAP did in my case which brings us to Backfire Step 3: Reframe: emphasize the injustice, counter reinterpretation.
Drug testing that follows mandated guidelines provides procedural safeguards that protect the donor. .Accountability demands both the provision of information (answerability) and justification for ones actions. both those administering the tests and those performing the tests are held accountable by outside agencies. The system is transparent and when the validity or integrity of a test is questioned the employer and lab must provide the records and documentation.
Why are doctors allowing PHPs to use drug and alcohol testing of unknown validity? We require evidence-base and adherence to professional protocol and ethical guidelines in every other arena but this one. Using the fallacious appeal to authority, however, the impaired physicians movement doctors (FSPHP) convinced regulatory boards that these tests were valid, reliable and necessary. In fact the sensitivity and specificity is unknown so the false-positive rate is unknown. In addition, with no regulation or oversight, positive tests can be the result of deliberate misconduct and, with no agency to sanction those engaging in the misconduct, it can continue unchecked.
It is time we demand better care for our fellow doctors. It is time we debunk the mythology surrounding the required length of stay in rehabilitation facilities that is three-times longer than anyone else. There is nothing unique about being a doctor that warrants this. No evidence base exists. PHPs need to be reformed and rebuilt as programs of institutional justice. The current state of affairs is one of coercion, control and abuse.



