

“Let it be considered, too, that the present inquiry is not concerning a matter of right, if I may say so, but concerning a matter of fact.”–Adam Smith
“Most men endure the sacrifice of the intellect more easily than the sacrifice of their daydreams. They cannot bear that their utopias should run aground on the unalterable necessities of human existence” -Ludwig von Mises
The guiding philosophic principle is Hegelian or “rational utility” and “corresponding doctrine and planning”, Alexander said “replaced moral, ethical and religious values” and Nazi propaganda was highly effective in perverting public opinion and public conscience. He explains how this expressed itself in a rapid decline in standards of professional ethics in the medical profession. This all “started from small beginnings” with subtle shifts in the attitudes of physicians to accept the belief that there is such a thing as “a life not worthy to be lived.”
In 1985 the British Sociologist G.V. Stimson wrote of a new form of professional control in the United States that had emerged in the preceding decade whose “success rests on the ability to take certain areas of conduct such as alcoholism and drug abuse (which are formally disciplinary issues) and handle them as diseases.”2
Stimson writes:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”2
Among these authoritative pronouncements was the use of specialized treatment centers. Many professionals were critical of these programs including Assistant Surgeon General John C. Duffy who criticized the “boot-camp mentality”4 toward doctors and American Society of Addiction Medicine President Leclair Bissel who when asked in a 1997 interview when the field began to see physicians as a specialized treatment population replied “when they started making money..” .” 5
Amid reports of abuse, coercion and control in facilities using a doctor’s medical license as “leverage,” the Atlanta Journal Constitution ran a series of reports in 1987 documenting the multiple suicides of health care practitioners at one of these programs (5 while in the facility and at least 20 after discharge).6 Neither these suicides nor a large settlement against the same facility (finding a non-alcoholic doctor was intentionally misdiagnosed as an alcoholic and forced into months of treatment) for fraud, malpractice, and false imprisonment involving intentional misdiagnosis7 generated any interest among the medical community at large.
And by 1995 the door had closed as the Federation of State Physician Health Programs ( FSPHP ) relationship with the Federation of State Medical Boards (FSMB), the national organization responsible for the licensing and discipline of doctors, was forged. A 1995 issue of The Federal Bulletin: The Journal of Medical Licensure and Discipline, contains articles outlining the high success rates of these programs in 8 states with an editorial comment from the FSMB that concludes:
“cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.”8
The Federation of State Medical Boards (FSMB) has approved any and all policy and regulation put forth by the impaired physician movement then organized under the Federation of State Physician Health Programs (FSPHP) with no apparent inquiry or opposition.
In 2003 Dr. Gregory Skipper, one of the key players of the impaired physician movement partnered with NMS labs to develop the alcohol metabolite ethyl-glucuronide (EtG) as a laboratory developed test13 14 he proposed be used as a monitoring tool for covert alcohol use in physicians after a pilot study involving just 14 psychiatric inpatients.15
The policy entrepreneurship this group so effectively uses to advance their goals can be seen in the August 25, 2004 Journal of Medical Licensure and Discipline which contains articles both presenting the problem 11 and providing the solution.11 The EtG was then introduced as an accurate and reliable indicator of covert alcohol use and the impact of this cannot be underestimated as it introduce to the market not only unregulated non FDA approved tests for forensic use but tests reaching further back into history then those used by workplace drug-testing programs.
The limitations of any test needs to be understood both in the forensic and clinical context but there is a lot less flexibility in the forensic context when people’s liberties, freedoms or property rights ( as with a medical license) are in jeopardy.
Sensitivity and specificity need to be carefully considered. The positive predictive value of a test is the true positives over the true positives plus false positives. If you are going to sanction somebody as a result of a single test that test needs to have 100% sensitivity.
When workplace drug testing was introduced debates over both the accuracy and scope of tests occurred. The employees right to privacy and the employers right to have a drug-free workplace were discussed with the general consensus being testing for impairment was a legitimate concern but preservation of private life should remain.
What was done here dissolves both.
PHP programs require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring abstinence from drugs and alcohol while using non-FDA approved Laboratory Developed Tests in monitoring programs is a dangerous combination. The suicides reported by the Atlanta Journal Constitution in 1987 were prior to the introduction of these tests. Adding these tests of unknown validity to an already abusive program of coercion and control would only worsen the situation.
I have been hearing of multiple suicides involving both the fear of results and false results. I have also been hearing of doctors who have killed themselves because they were suffering from depression but did not seek help as their fear of being ensnared into the PHP outweighed the need to get help.
Three decades after G.V. Stimson so accurately defined the impaired physician movement the impaired physician movement defines the professional control of medicine.. Their involvement in medical society physician health programs (PHPs) and treatment programs has evolved into absolute control of both. Pronouncements on physician impairment have evolved from insider’s claims to written edict. And their reach has extended from impairment due to drugs and alcohol to “potential impairment” and “relapse without use.” Their reach has extended from drug and alcohol impairment to all other aspects of medicine and the impact has been profound. Medicine has been subordinated to the guiding philosophy of the impaired physician movement and doctors are dying in droves du to institutional injustice.
How does the profession of medicine reconcile the fact that we have allowed an as yet non ABMS recognized “self-certification” specialty full reign over those who are ABMS recognized? How is it that we allow non-FDA approved Laboratory Developed Tests (LDTs) of unknown validity on doctors coerced into state Physician Health Programs (PHPs)? A recent debate in Washington calling for regulation of “clinical” LDTs just took place and the fact that they are being used for “forensic” purposes in doctors is incomprehensible. Has anyone noticed it is the same people introducing the tests who are claiming PHPs are the “gold standard,” trying to push them on other EAPs and calling for more widespread use of these tests?
The use of non-FDA approved Laboratory Developed Tests (LDTs) for drug and alcohol testing is currently limited to PHPs and the criminal justice system. (i.e. monitoring programs in which those doing the testing have power and those being tested have no power). That may soon change. See Drug Testing and the Future of American Drug Policy and The American Society of Addiction Medicine White Paper on Drug Testing describing the plans for widespread expansion of this drug testing to other groups including kids.
Those involved in the Massachusetts General Hospital Laboratory Medicine, Toxicology and addiction medicine departments looked critically at these tests and decided hands down against using them. Why? Because no evidence base exists and the potential harm far outweighs any perceived benefit. “Research” has been done on those being monitored by PHPs and the criminal justice system and Drs. J Wesley Boyd, M.D., PhD, and John Knight, M.D. of Harvard Medical School who collectively have over two decades of experience as Associate Directors with the Massachusetts PHP, Physician Health Services, Inc. addressed this research in a 2012 article published in the Journal of the American Society of Addiction Medicine entitle Ethical and Managerial Considerations Regarding State Physician Health Programs. The allegations that PHPs are engaging in research in violation of the Nuremberg code ( that was a direct result of the Nuremberg trials for which Dr. Alexander acted as consultant ) should have raised some eyebrows. It hasn’t.

What do you think will happen when ASAM gets recognized by the ABMS in 2 years as is expected? These “addiction medicine” specialists will inevitably join hospital formulary , clinical lab, toxicology and ethics panels to do the same thing they have done to get where they are today. They will do the same thing they have done with state PHPs. Those with a hidden agenda will be able to outvote those of good conscience and thoughtful intelligence and patient care will then be subordinated to the guiding philosophy of the impaired physicians movement.
This system of institutional injustice is killing doctors by suicide as the medical societies and Departments of Public Health have given PHPs full autonomy and authority and it is poised to impact patient care.
I challenge you to name any other company, organization, group or agency within or related to the profession of medicine and the field of science that is bereft of absolutely all transparency, regulation or oversight? It does not exist.
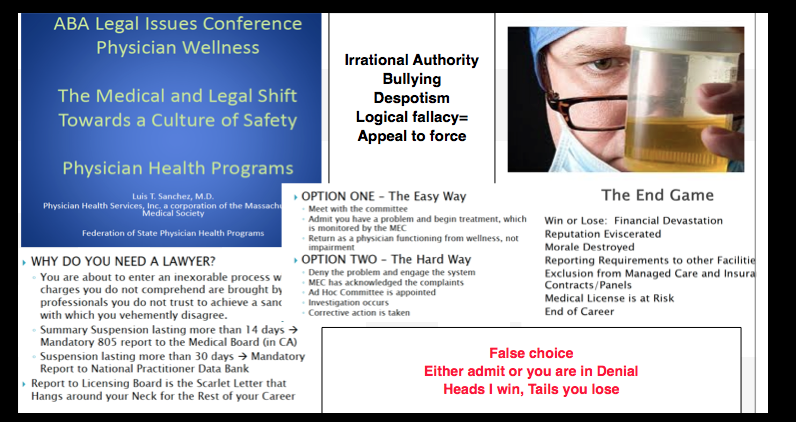
The PHP scaffold has deliberately removed themselves from all aspects of accountability including answerability, justification of actions and the ability of outside actors to hold them in judgment of any information provided by answerability. Heads I win, tails you lose. That is a big red flag in itself. and those not currently being held accountable they may very well be after you next as their plans include expansion to other groups includes EAPs, the Department of Transportation, athletes, students and even kids!
Doctors are afraid to talk about this for fear of being ensnared themselves. Those already in these programs will not speak for fear of punishment. This is a legitimate concern and needs to be discussed openly and publicly. I need allies!
Help me get the word out –too many doctors are dying. Three died by suicide in one month alone who were being monitored by the Oklahoma PHP and these suicides did not even make the local papers let alone national news! They need to.
In The Argument of Fascism Ludwig von Mises wrote:
It cannot be denied that Fascism and similar movements aiming at the establishment of dictatorships are full of the best intentions and that their intervention has, for the moment, saved European civilization. The merit that Fascism has thereby won for itself will live on eternally in history. But though its policy has brought salvation for the moment, it is not of the kind which could promise continued success. Fascism was an emergency makeshift. To view it as something more would be a fatal error.















 “Spirituality can go hand-in-hand with ruthless single-mindedness when the individual is convinced his cause is just”
“Spirituality can go hand-in-hand with ruthless single-mindedness when the individual is convinced his cause is just”









Wow! Thank you for this! This article may very well be far beyond its time, and thus, that much more impactful. There is so much to be added to the discussion of the mental and physical state of the modern day physician. It could provide so much more insight not only into the lives of physicians, but also their patients. Much like the police, there is a code of silence among the medical and scientific community; one so static and unwavering, it is much of the cause of the staggering amount of deaths and illnesses abound in our current society. Because by default, everyone is either a patient or a physician, by building the platform for this conversation, pieces of writing like this may prove to be the key to saving every single person in the world. Literally. Again, thank you!
Thanks! The problem is the mainstream medical bloggers will not address the role of physician health programs and physician suicide. In fact many of my comments on these blogs regarding this have been removed as “spam.” This barrier has been very hard to break for various reasons. How do we solve a problem most doctors will not even mention? To address the problem we need to acknowledge it and that is just not happening.
Liked by you and 2 other people
So, so true! Please, just don’t stop what you’re doing. No matter how much blow back and obstacles you face, keep getting this message out there. People are watching and waiting for the courage to join in the conversation. People like you, with the courage to be the first on the dance floor, so to speak, are the reason the party gets started. No matter how long it may seem that you’re dancing alone, you’re not. And right when you last expect it, the whole world will begin acknowledging the significance of physician health and physician suicide, as if it’s been around as long as sliced bread. People like you and I rarely get the credit we deserve, but what’s credit, compared to saving lives. I can’t emphasize enough how important research, data and discussions like this are for the necessity of literally, saving lives. I get it. I really, really do. I’ve personally seen what can and continues to happen as a result of us ignoring what the lacking physician health programs and growing physician suicide. So, yea, just keeping going, please. For the children who may never meet you, but will live longer lives from the sacrifices you’ve made. Much peace, love and blessings be to you always! A’se (and so it is)!
Liked by you and 1 other person
So is it suicide or accidental overdose? I had a physician who was found dead by his wife, overdosed on a prescription med. It has bothered me all these years, wondering if it was deliberate or an accident. I tell myself it was accidental, because that’s what I want to believe, and yet, you all have so much responsibility weighing on your shoulders. How do you cope?
Liked by you
The 400 figure is an underestimate as death certificates and other traditional sources of information have proven unreliable. In addition most of these deaths are not investigated –especially if there was a PHP involved. Last August 3 doctors died by suicide in a 30 day period who were under monitoring by the state PHP and it did not even make the local news. In many cases it is difficult to determine if death is a result of suicide or an accident and suicides are often underreported to protect the victim or family from stigma or insurance investigations. An insurance company will more easily pay on a claim due to a “drug misadventure” than a suicide.
Liked by 2 people
That’s understandable, but so sad. Everything seems to boil down to insurance now, what they will or will not pay for. From a patient’s point of view, it gets frustrating that we all pay because of the ones who abuse the system, and from your side, it means extra work because some of the patients abuse the system, so all patients must be subjected to the same embarrassing testing. And you suffer because the patients hold you responsible, so it is an uphill battle all the way. I’m glad the COD is not included in obits that are seen in newspapers, and also glad autopsies are not required in every case. I can remember when they were, and how hard it was on families. In the case of my doctor, an autopsy was ordered and it was all over the front page of the local paper. Not a good thing for his family to live with.
Liked by you and 1 other person
[…] http://disruptedphysician.com/2015/02/25/the-elephant-in-the-room-physician-suicide-and-physician-he…; […]
Liked by you
(forgive if this is a redundant entry – left one yesterday but didn’t get posted.)
Another brilliantly incisive piece, Michael!
In what is sure to be a seminal work, Tom Bourne and colleagues examined the psychiatric impact of board complaint investigations on physicians in Britain (the GMC there is the equivalent of state licensing boards here) and found a 100% increase from baseline in depression, anxiety and suicidal ideation. Hmmm … any possible link between board “investigations,” PHP sham “diagnoses” and physician suicide?
(see: Bourne T, et al. BMJ Open 2015;4:e006687. doi:10.1136/bmjopen-2014-006687)
You would have expected medical boards (consisting of physicians who took an oath, for godsakes!) and PHPs (with their “oh-so-concerned-about-physician-health” mantra) to have shuddered at this finding and rushed out to investigate whether this could possibly be true.
Now, optimists that you are, brace yourself … not one medical board or PHP member has responded to the Medscape article which announced this, nor apparently countered the finding in any other forum. (As in “oh, board and PHP inquiries are really benign … see all our happy campers … our studies show everybody’s doing well and what great work we’re doing.”
Have you heard of any investigation by FSPHP or FSMB into whether this finding might be true? Or at least an expression of concern? Nah ….
Or perhaps the AMA …? Nah.
Oooh, oooh, maybe the APA which by all rights should be concerned about the illicit activities of unlicensed PHPs operating as “public charities” conducting career and life altering psychiatric and substance abuse evaluations under the sham rubric of “peer review,” referring, under board order based on their pontifical findings (whose report they adamantly refuse to provide to the subject physician), to pre-selected “preferred institutions” with whom there is a prearranged “understanding” of the admission diagnosis and impairment severity and the gross abuse of the field of psychiatry by the denial of due process and ensuing torture these programs commit…? Maybe they’d be concerned, right??? … nah. Multiple parties have emphatically tried to rouse them from their institutional slumber to utterly no avail but an insulting response implying that the complainer is nothing but a personality-disordered whiner who’s unhappy with “the program.” (Yes, the “program.” That’s like telling a Jew in 1940’s Germany that he shouldn’t be complaining about the free train ride the government is offering.)
As has been explicitly documented by the NC State Auditor in its comprehensive performance evaluation report on the NCPHP (see NCOSA Performance Evaluation of NCPHP April 2014, available online), NCPHP systematically violated the due process rights of over 1,140 physicians over the preceding decade. (Even the writing of the phrase does not convey the extremity of the violation – one has not only been denied justice and screwed by one’s own pathetically impotent lawyers, one has lost one’s career and even personal identity – all in one fell swoop by an agency with no oversight or accountability.)
Now, answer me this: if you were falsely accused of something, falsely diagnosed, had laboratory data falsified in order to both reinforce the false diagnosis and punish you for your defiant challenge, and had your due process rights violated, and you then were entirely deprived of your career and then so publicly shamed by the published proceedings based on the false but incontestable findings, and your practice was abruptly upended, and you then were forced to witness your patients’ suffering as a result of the disruption of their care with you, and you then were forced to bear the news of one of your patients committing suicide as a direct result of this abusive disruption of care, would you be … upset?
Keep up the extraordinary work, Michael. While there are innumerable docs who have been utterly obliterated by this combined board / PHP abuse and their manipulation of their privilege – and, yes, some have tragically taken their lives being put in such an impossible bind, there are a few of us who are determined to confront this abuse and demand that protections be put in place so that it never occurs again, without severe consequences ensuing to the offending party.
Liked by you
Two examples of the misinformation and propaganda this group is putting out.
http://www.medscape.com/viewarticle/840112
http://www.thefix.com/content/what-if-we-really-treated-addiction-disease-it
Like
[…] The Elephant in the Room: Physician Suicide and Physician Health Programs. […]
Like
(From a resident physician who wishes to remain anonymous)
Dr. Langan:
Thank you for your articles and research regarding PHPs and “impaired” physicians. I have become involved in this issue after someone close to me struggled with depression during residency. Sadly, they lacked the resources, support and coping skills and ended up committing a crime with a misdemeanor charge. Despite their treatment and rehabilitation, they were dismissed from residency. Not sure if they will ever get to practice clinical medicine. It is very sad. they are very smart, great doctor and very empathetic towards patients.
After their situation, I started looking on blogs and found that many residents had shared similar instances. Many reported struggling with depression and the stresses of residency put them over the edge– like the perfect storm of stress, fatigue, and loneliness that could exploit anyone’s weaknesses. It seems like during residency, we are emotionally as well as legally vulnerable. Many of these residents have never been able to resume training at their institutions despite their demonstration of clinical competence and emotional maturation. According to that medscape article, that is a huge loss to society, socially and financially.
Sadly, there still so much stigma surrounding mental health, and I think it may be worse in our profession.
I am very concerned regarding the future of our profession. We are becoming robots in a health care factory. Our own personal lives are being compromised as well as quality patient care.
I appreciate all you are doing to shed light on this very important issue.
Thank you for your time and consideration
Liked by 2 people
Reblogged this on Chaos Theory and Human Pharmacology and commented:
“How do we solve a problem most doctors will not even mention? To address the problem we need to acknowledge it and that is just not happening.” — Dr. Michael L. Langan.
Re: Happening now (i.e., reblog).
Liked by you
I was sent the letter below by e-mail. Dr. Roop has specifically requested that it be published here with his contact information and I applaud his courage.
On Mar 5, 2015, at 4:04 PM, Jonathan Crane Roop MD wrote:
Name: Jonathan Crane Roop MD
Email: jonathanroop@hotmail.com
Comment: I am Board Certified in Internal medicine. I have endured years of emotional, psychological and spiritual abuse at the hands of the Washington Physician’s Health Program. I have suffered through a long list of injustices without recourse. They include, but are not limited to discrimination, abuse of power, breach of contract and repeated and WILLFUL medical negligence.
Because the actions of the WPHP have been SO egregious, I assumed what was happening to me must be extraordinarily rare.
I have nothing to hide. And I have shared my story with any and all who would listen. To date, my voice, my rights and now my life have been dismissed as unimportant. MY LIFE!! It’s apparently better that I die than my tormentors be questioned and compelled to defend their indefensible and evil behavior.
I am meeting with one last attorney tomorrow. I fully expect him to ignore the basic, indisputable and well documented facts of my case. Namely, there is massive and systematic malfeasance being committed by a tax payer funded agency in the State of Washington who act with omnipotence and without oversight. I have no reason to believe he will respond any differently than the others with whom I have met. HE WON’T CARE! HE WILL NOT BE MOVED. He will make statements that suggest I DESERVE this treatment. And that my life, as well as my imminent death, is unworthy of his time or efforts.
Once my assumptions about this last meeting are officially confirmed, I am committed to the only course of action available to me. The only thing which will put an end to this nightmare.
Today I stumbled upon your website. And today, for the first time, I have learned that my case is not rare. I suspect the other physician victims in this matter have occasionally allowed themselves to dream wistfully of justice. Justice which they have seen thwarted at every turn. Perhaps they, like me, have dreamily imagined the relief and joy and LIFE they would experience if the truth were simply presented and the perpetrators held accountable. I have imagined standing up in court and triumphantly affecting justice for myself as well as all of the other current and future victims. I deliver a powerful defense of justice. My ‘dream speech’. I have imagined that I might still live. And then I wake up.
And so today, imagine my shock, when I found my ‘dream speech’ here. My speech. Reasonable. Honest. Consistent. And based firmly in truth, justice and defense of the powerless against the (arbitrarily) powerful. My speech, it seemed, but authored by another.
Thank you, Dr. Langan. You have given a voice to my struggles. Please never stop speaking for me, and people like me, many of whom, I fear, will not survive to see justice.
Despite my intention to die, I actually WANT TO LIVE! And I will live and fight on if I ever believe that there is even a small chance of justice for me and the other innocent victims of PHP’s and the ‘treatment’ centers with whom they contract (Talbott in my case. Purely evil and loathsome human beings, for the record).
So, because I do WANT to live…PLEASE HELP ME, SIR!
Can you refer me to attorneys, individuals or groups who might advocate for me and the other victims? Do you have any specific words of hope or encouragement?
Please note my name. Please add me to the list of innocent victims of these power hungry, narcissistic BULLIES.
I don’t expect to live through this. And in a way, the PHP, Talbott and the addiction ‘experts’ with whom I have been tragically acquainted are correct…My life is worth very little. But this issue is so much larger than I. I can die with some serenity if I believe there will be meaningful justice for others like me. And that those responsible will be held to account.
Thank you Dr. Langan. Thanks to all of those involved in the creation and maintenance of this website. Although your shining beacon is barely perceivable through the darkness of injustice which surrounds and seeks to extinguish it…it is the only glimmer of hope I have found during my slow death by PHP.
Jonathan Crane Roop MD
811 S Cowley St #48
Spokane WA 99202
509-710-4641
Liked by 1 person
These miscarriages of justice remind one of nothing so much as Victor Hugo’s “Les Miserables”. That was, of course, a mere novel. Sadly, the experiences described here are real. The loss of capable physicians is doubly tragic — not only for the physicians involved, but for society at large. I would add only that God is capable of giving our lives purpose, even after what is most precious to us has been taken. Life can be worth living, despite great loss.
Like
I have been hearing from 2 or 3 every day. Nearly all of them are afraid to leave comments here (even anonymously) for fear the PHP will find out. There is a “learned helplessness” because there is no lifeline. The Medical Boards are complicit, The Medical Societies have no oversight, Law enforcement turns a deaf ear because the perpetrators have convinced them it should be kept within the medical profession. Attempting to report valid crimes are refused and they are often reported back to the Board or PHP and further punished. The media is not interested because they have been labeled “impaired”or “disruptive” and no matter how strong the truth, evidence or facts are they take the PHPs word over theirs. And almost all of the doctors I have talked to are good doctors who are kind hearted and honest. But bad doctors are rarely sanctioned by medical boards; they have to do something so egregious that turning a blind eye would be noticed. And doctors who are bad people who have engaged in terrible behavior often get reinstated by claiming they were “helpless” over that behavior but are now “in recovery.” They go to extremes to protect sexual violators in these programs and also believe they can monitor pedophiles with polygraphs and treat them with 12-step. Just look at the case below. An adolescent psychiatrist gets arrested with child pornography and admits to a longstanding attraction to young boys. The PHP gives him a polygraph test “proving” he’s a looker not a toucher and he is back practicing medicine in no time. The PHP speaks as if he is a Saint. Perhaps they had a slot to fill in the “sexual addiction” department in one of the “PHP-approved” assessment and treatment centers.
http://www.psychsearch.net/montana-psychiatrist-james-h-peak-convicted-of-child-porn-wants-license-back/
http://billingsgazette.com/news/local/peak-s-medical-license-reinstated-on-lifetime-probationary-status/article_fab77fef-188c-5f29-8013-4a86c87d32a8.html
Like
[…] “Physician Suicide and Physician Health Programs: The Elephant in the Room (http://disruptedphysician.com/2015/02/25/the-elephant-in-the-room-physician-suicide-and-physician-h… 😉 […]
Liked by you
Reblogged this on Disrupted Physician.
Like
Doctors, I can sympathize with your pain although I am not a physician. I was trained at a university medical facility in laboratory medicine and during my sophomore year it was found that I was suffering from what their psychologist called “delayed grief” from the loss of my mother. Long story short, they pushed me out of school until I could get it together. I am a disabled, Christian and pastor of a small church now and not in laboratory technology practice anymore. My website http://thelivingmessage.com, is my way of bringing the hope of Jesus to those who are searching for answers in a world that seems not to want to hear them. Please feel free to refer any of your friends to my site or even to email me through it. I will be glad to pray with and for any or all of you in your time of pain and suffering. God gave you your talents and abilities so please don’t throw them away if possible.
Like
Thanks Gordon, I appreciate your comments and I will.
Liked by 1 person
The list really touched me….I have been close to just ending it before. I used to think it was something only “other” people experienced. This is so sad !!
Liked by you
Reblogged this on diploctor and commented:
This article and video are so important !
Liked by you
[…] require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring […]
Liked by you
[…] require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring […]
Liked by you
[…] system is also the unspoken and hushed major contributor to physician suicide-the elephant in the room. Those who really need help for mental health, substance abuse or other issues are afraid to get […]
Liked by you
[…] require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring […]
Liked by you
[…] is also killing physicians by driving them to hopelessness, helplessness, and despair. The general medical community needs to awaken to the reality of the danger and expose and dismantle […]
Like
[…] for suicide. The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical […]
Like