Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
If a test’s results do not differ between alternative states of health, then the test has insignificant accuracy; if the results do not overlap with other states of health then the test has perfect accuracy. Most tests accuracies fall between these two extremes.
The intrinsic accuracy of a test is measured by comparing the test results to the “true condition status.”
‘True condition status” refers to one of two mutually exclusive states. Either acondition is present or it is absent.
We determine true condition status by means of a “gold standard” which is a source of information completely different from the test under evaluation which tells us the true condition status of the patient.
To have striven, to have made an effort, to have been true to certain ideals — this alone is worth the struggle. We are here to add what we can to, not to get what we can from, life. – William Osler
Diagnostic Medicine
Diagnostic medicine is the process of identifying the condition or disease that a patient has and ruling out conditions or diseases the patient does not have through assessment of the patient’s signs, symptoms, and results of various diagnostic tests.
Diagnostic Test Accuracy
Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
If a test’s results do not differ between alternative states of health, then the test has insignificant accuracy; if the results do not overlap with other states of health then the test has perfect accuracy. Most tests accuracies fall between these two extremes.
The intrinsic accuracy of a test is measured by comparing the test results to the “true condition status.”
‘True condition status” refers to one of two mutually exclusive states. Either acondition is present or it is absent.
We determine true condition status by means of a “gold standard” which is a source of information completely different from the test under evaluation which tells us the true condition status of the patient.
Say we want to develop a new rapid test for detecting strep throat. Strep throat is caused by the Streptococcus bacteria. Although more common in children and adolescents it can occur in people of all ages. Strep throat is one of many possible causes of sore throat and pharyngitis. It is contagious and can cause complications such as rheumatic and scarlet fever. Treatment with antibiotics can shorten the course of the disease and reduce the risk of complications.
A throat culture is obtained by swabbing the patient’s throat with a cotton swab. The sample is then sent to the lab where it is cultured. If strep is present it will grow on the culture and look as below. The bacteria either grows on the culture or it doesn’t. A throat culture is the “gold standard” for diagnosing strep throat. The problem is it may take two days to get back.
Sensitivity and Specificity
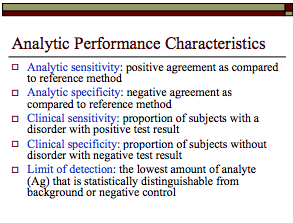
The two most important measures of diagnostic test accuracy are sensitivityand specificity.
The probability that a test will be positive in someone with the condition = Sensitivity
The Probability that a test will be negative in someone without the condition = Specificity
For diagnosing strep throat we want our test to be as close as possible to the gold standard in terms of both sensitivity and specificity.
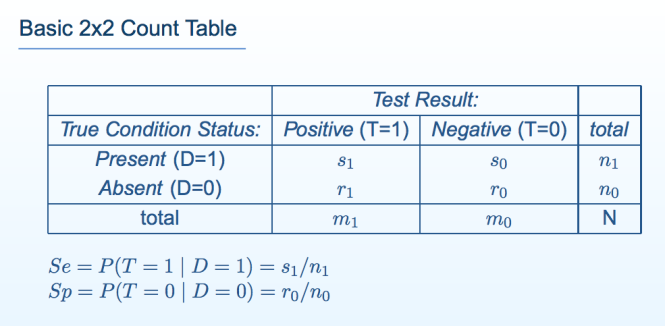
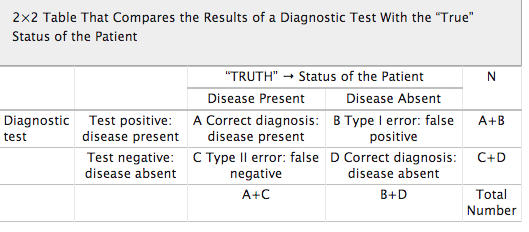
Sensitivity and specificity can be illustrated by a table with two rows and two columns. This simple Decision Matrixwhere the rows summarize the data according to the true condition status of the patients and the columns summarize the test results. This table is called a “count table” because it indicates the numbers of patients in various categories. The total number of patients with and without the condition is, respectively n\ and n0; the total number of patients with the condition who test positive and negative is respectively s\ and s0; and the total number of patients without the condition who test positive and negative is respectively r\ and ro.
The total number of patients in the study group N, is equal to N = si+so+rx+ro, or N = n\ + no·
The true condition status is symbolized by the variable D, where D = 1 if the condition is present and D= 0 if the condition is absent.
Test results indicating the condition is present are called positive; those indicating the condition is absent are called negative.
Test results are symbolized by the variable T, where T =1 denotes positive test results and T= 0 denotes negative test results.
The sensitivity (Se) of a test is its ability to detect the condition when it is present.
We write sensitivity as Se = P(T = 1 | D = 1), which is read:
“sensitivity (Se) is the probability (P) that the test result is positive (T = 1), given that the condition is present (D = 1).”
Among the n\ patients with the condition, s\ test positive; thus, Se = s\/n\.
The specificity (Sp) of a test is its ability to exclude the condition in patients without the condition.
We write specificity as Sp — P(T = 0 | D — 0), which is read:
“specificity (Sp) is the probability (P) that the test result is negative (T = 0), given that the condition is absent (D = 0).”
Among no patients without the condition, ro test negative; thus, Sp — TQ/UQ
False Negative and False Positive Tests
There are consequences associated with all test results.
False Negative Tests: If a test falsely indicates the absence of a condition in someone who truly has it then treatment can be delayed or not provided.
The consequences of a false negative strep test depend on what we do with it. Serious consequences can arise if we use our new strep test as the sole basis for subsequent decision making. Putting complete trust in the negative test result would lead to no antibiotic treatment provided to a patient with Strep and can lead to continued illness, spread of the disease and complications that would not have occurred if antibiotics were provided. The patient could potentially get rheumatic or scarlet fever.
If the new test is negative but a culture was drawn the false results could delay treatment by a couple days or so but treatment is nevertheless provided. The consequences are likely to be minimal. It is highly unlikely a patient would get rheumatic or scarlet fever as, although a little later, they are still being treated with the proper antibiotics.
False Positive Tests: If a test falsely indicates the presence of a condition in someone who does not truly have it then unnecessary tests and treatments can occur. Incorrect treatment and false labeling of patients can also occur.
In the case of a false positive strep test, a patient may undergo a course of antibiotics when they do not need them. Although the patient may suffer side-effects from the antibiotics the severity and duration of any of these consequences are minimal.
The importance of a Diagnostic Accuracy in testing is directly proportional to the tests potential to cause patient consequences and harm.
Diagnostic Medicine uses a patient’s signs, symptoms and the results of various diagnostic tests to arrive at a diagnosis.
In diagnosing strep throat a good clinician will take into account a number of variables in consideration of a differential diagnosis and base testing and treatment on the preponderance of information supporting or opposing the diagnosis.
For strep throat using the new test in addition to a throat culture, history and careful physical exam and basing the decision to prescribe antibiotics on clinical acumen based on the overall picture is the best approach. The test can be considered a piece of the puzzle but does not define it. Therefore the risk of a false positive or false negative is minimal as it is just one data point.
Diagnostic accuracy is necessary if a test is being used as the basis for further tests and treatment. If a test is being used as the sole basis for further tests and treatment it needs to be accurate. If the results of a test can cause significant patient harm or death then it needs to be either 100% accurate or combined with other highly accurate tests to confirm the diagnosis.
The specificity of a test is particularly important as a false positive can result in unneeded interventions and treatment. Stand-alone tests used in diagnosis and treatment need to be both sensitive and specific. Diagnostic accuracy is a product of consequences of false-negative and false positive tests.
Diagnostic Research Methodology
Research to discover the accuracy of a diagnostic test should be straightforward; administer the test to a group of people and see if it works.
The test being tested is the “index test”. Results of the index test are compared with the results of a “gold standard” reference test.
The research question is, “How accurately do index test results predict the (true, gold standard) reference test results?”
Diagnostic test accuracy studies require a sample of subjects who have been given the test under evaluation, some form of scoring of the tests findings and a reference or “gold standard” to which the test findings are compared. Examples include autopsy reports, surgery findings and pathology results from biopsy findings.
The gold standard for a patient’s true disease status may not always be available. A brain biopsy could be considered a gold standard for diagnosing Alzheimer’s disease but is neither practical nor humane.
The Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool is a set of fourteen questions that investigate the methodologic quality of scientific studies that quantify diagnostic test performance.
The questions identify research methodologies known to bias the accuracies research discovers.
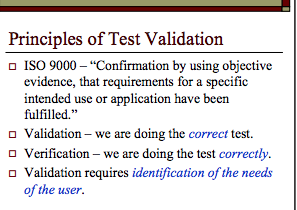
Multiple factors need to be considered in evaluating the diagnostic accuracy of a test including diagnostic validation and verification. Is the test testing what it is supposed to be testing for and are we doing it correctly?
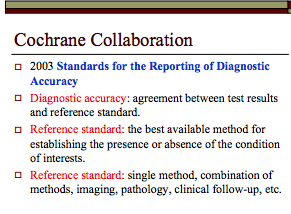
Diagnostic accuracy of a test necessitates a reference standard, The reference standard can be the best available method for establishing the presence or absence of a condition (such as the throat culture for strep throat) or a combination of methods (imaging, neuropsychological testing, clinical exam, etc. in Alzheimer’s disease.
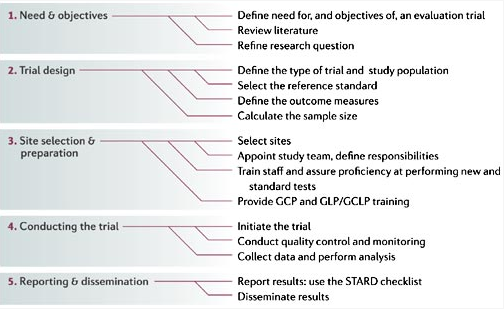
Any test that is going to be used as a basis for decisions that impact other human beings needs to be validated before it is introduced on the market. The literature needs to be reviewed critically and trials must be designed using objective evidence that validates the test is testing for what it purports to be and verifies the correct methodology of the test. Verification that the test is being collected, handled, stored, transported and processed correctly is requisite.
Cutoff levels, , cross-reactivity and myriad other issues need to be worked out prior to bringing a diagnostic test to market.
The reliability, validity and accuracy of drug test results needs to be known prior to using a test. Specificity and sensitivity must be known prior to using a test on any population.
This should go without saying as to do anything else would be irresponsible and careless.
References
Evidence-based medicine, systematic reviews, and guidelines in interventional pain management: part 7: systematic reviews and meta-analyses of diagnostic accuracy studies Pain Physician 2009, 12(6):929-963. PubMed Abstract | Publisher Full Text
Jaeschke R, Guyatt G, Lijmer J: Diagnostic tests. In Users’ guides to the medical literature: a manual for evidence-based clinical practice. Edited by Guyatt G, Rennie D. AMA Press; 2002:121-140.
Streiner DL: Diagnosing tests: using and misusing diagnostic and screening tests.J Pers Assess 2003, 81(3):209-219. PubMed Abstract | Publisher Full Text
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J: The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003., 3(25) http://www.biomedcentral.com/1471-2288/3/25webcite
GCP, good clinical practice; GCLP, good clinical laboratory practice; GLP, good laboratory practice; STARD, standards for reporting of diagnostic accuracy. See Section III, 2.13 From Nature Reviews Microbiology 4, S20–S32 (1 December 2006) | doi:10.1038/nrmicro1570
An attorney must have a factual basis for alluding to, offering or relying on evidence and that factual basis may not be wishful thinking. There are two requirements for a factual basis — an attorney’s subjective belief and objective evidence to support that belief. It has now been established that no objective evidence exists. Not a shred of it. Not a single chronologically consistent data-point!
On June 3, 2016 Governor Baker signed House Bill 4333 imposing greater accountability on state agencies when responding to public records requests. This includes shorter time frames to respond to requests (10-days for most), the provision of complete and legible records and appointing a Primary Records Access Officer to handle such requests. The new Public Records Law also subjects agencies to sanctions for failure to comply.with the new law.
On January 9, 2017 I submitted a Public Records Request through the Executive Office of Health and Human Services (EOHHS) Website for a dozen or so documents that had been submitted for board hearings but never directly addressed and containing textual content with evidence that was never weighed. Moreover, many of the documents provided direct evidence of crimes (no other is evidence needed).
All of these documents were provided to Board counsel Deb Stoller.
Oppression that is clearly inexorable and invincible does not give rise to revolt but to submission. Simone Weil
The AMA Code of Medical Ethics opinion 8.032 states:
“Physicians should disclose their investment interest to their patients when making a referral, provide a list of effective alternative facilities if they are available, inform their patients that they have free choice to obtain the medical services elsewhere, and assure their patients that they will not be treated differently if they do not choose the physician-owned facility.”
There are three ways a person can pay for health services: 1.) government Health Plans ; 2.) private health plans; and 3.) out-of-pocket
Government and private heal plans have regulations that are consistent with the AMA Code of Medical Ethics opinion 8.032 and the key concepts are: 1) No taking money for referrals 2) Referrals should be based on medical necessity 3) Referrals should be based on the best providers. Government regulations are the most restrictive. Stark Law and the Anti-kickback Statute provide very detailed “safe harbor” rules which must be followed. Congress enacted a physician self-referral law in 1993 after learning the incidence of radiology procedures and physical therapy greatly increased when the patient’s physician had an ownership interest in the facility or clinic. This law is the result of legislation introduced by Representative Fortney (Pete) Stark (D-CA), then Chairman of the U.S. House Ways and Means Health Subcommittee. An earlier self-referral law (“Stark I”) had been enacted for clinical laboratory services only. The self-referral law prohibits Medicare and Medicaid payments when a physician refers any of ten “designated health services” (DHS) to an entity where the physician has a financial relationship including clinical laboratory services and inpatient hospital services. Physician Self-Referral Law [42 U.S.C. § 1395nn] Anti-kickback regulations apply to anyone who “knowingly and willfully offers, pays, solicits, or receives remuneration in order to induce business reimbursed under the Medicare or Medicaid programs.” Anti-Kickback Statute [42 U.S.C. § 1320a-7b(b)] makes it a crime to pay for referrals in the Federal healthcare system. ( Section 1128B(b) of the Social Security Act ). False Claims Act [31 U.S.C. § § 3729-3733] makes it illegal to submit claims for payment to Medicare or Medicaid that you know or should know are false or fraudulent. Private health plans (including “self-funded” health plans) also have a restrictive set of rules and private-pay restrictions may mirror Stark Law or the Anti-kickback Statute, and will either be set forth in a provider agreement, or in a claims processing manual; compliance with which the physician may be asked to certify. Patient out-of-pocket (where the patient is solely responsible and pays out of pocket for an ancillary service) have no meaningful restrictions and this opens the door for abuse. The physician health program model is based on a simple coercive extortion scheme. In a paradigmatic case of coercion—the mugger who demands “your money or your life” the victim is better off handing over the money than losing their life. Coercion characteristically involves threats by which the coercer proposes to make the victim worse off unless they do as the coercer demands. In the 1990s some entrepreneurs within the “impaired physicians movement” discovered they could demand “your money or your medical license” and coerce doctors into paying for unneeded assessment and treatment that lasted three-times longer than normal folks and needed to be paid out-of-pocket. With no regulation from government or private insurers they could do whatever they want and they did.
The simple extortion scheme from the 1990s has now grown to around two dozen “PHP-approved” assessment and treatment centers and state boards require that only “PHP-approved” facilities be used and specifically excludes non “PHP-approved” facilities. The preferred facilities engage in “diagnosis rigging” and false diagnoses to warrant unneeded treatment. The labs are willing to engage in laboratory misconduct and will create a falsely positive test at client request. It is a closed incestuous system in which the PHP serves as the Axis of Control and everything is kept not just close-to-the-cuff” but up the sleeve. This has led to pathological opportunism and promiscuous interaction between the PHPs-assessment center-lab conglomerate, regulators and medical boards and the legal profession which includes attorneys ostensibly representing doctors who will not bite the hand that feeds them-mostly carpetbagger board attorneys and former AAGs who hopped over to the more lucrative side doctors who are actually carpetbaggers who hopped over to the other side after proving to the racket they had no scruples and the current pseudosymbiosis damages everyone but the psychopaths, bullies and clowns lining their pockets from the racket.
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model.The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the LDT drug and alcohol testing and 12-step assessment and treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.
So much for the in utero diagnostic assessment–This teratoma has been birthed!
The Second Coming
W.B. Yeats
Turning and turning in the widening gyre
The falcon cannot hear the falconer;
Things fall apart; the centre cannot hold;
Mere anarchy is loosed upon the world,
The blood-dimmed tide is loosed, and everywhere
The ceremony of innocence is drowned;
The best lack all conviction, while the worst
Are full of passionate intensity.
Surely some revelation is at hand;
Surely the Second Coming is at hand.
The Second Coming! Hardly are those words out
When a vast image out of Spiritus Mundi
Troubles my sight: somewhere in sands of the desert
A shape with lion body and the head of a man,
A gaze blank and pitiless as the sun,
Is moving its slow thighs, while all about it
Reel shadows of the indignant desert birds.
The darkness drops again; but now I know
That twenty centuries of stony sleep
Were vexed to nightmare by a rocking cradle,
And what rough beast, its hour come round at last,
Slouches towards Bethlehem to be born?
The validity and reliability of opinions lie in their underlying methodology and evidence base. Reliance on the personal authority of any expert or group of experts is the fallacy of appeal to authority and a more apt and accurate twitter caption to the photo above would be Algernon Sidney’s 1683 statement that:
“Implicit Faith belongs to Fools, and Truth is comprehended by examining Principles”
“How a healing profession heals itself #FSMB2016 partnerships #FSPHP trust and faith in oversight and system.”
Within the the allotted 140 character twitter limit this succinct observation is nevertheless very revelatory. Both systems and the oversight of systems demand accountability and answerability to outside and independent agencies. Trust and Faith are not in the equation. Why has this lesson not been learned?
Answerability requires the obligation to answer questions regarding decisions and actions. Accountability requires transparency, explanation and justification. What was done and why? Standards, rules, regulations, codes, laws and other objective benchmarks need to be applied by outside actors. This is critical. It is the very essence of…
Bertram also claims PHS has not committed any crimes because they have not been charged with any crimes. This is called denying the antecedent or inverse error. It is a logical fallacy where the consequent is an indicative conditional claimed to be false because the antecedent is false. ( A, then B; not A, therefore not B). If it is raining, then the grass is wet.It is not raining.Therefore, the grass is not wet.The argument is invalid because there are other reasons for which the grass could be wet such as spaying it with a hose. There are multiple reasons for which someone who committed a crime has not been charged with a crime.There is always a time-frame between the two and many who commit crimes never get caught. Luck, stealth, cleverness, and multiple other variables might be involved. Jimmy Savile molested and raped scores of children for decades and he was never caught. As a major fundraiser for hospitals this fiend had free rein to prey on sick and helpless little kids in hospital beds .
Stoller was provided direct evidence of crimes over five years ago. It is precise, clear and repugnant. How many careers have been derailed since that time? How many innocent people have died by suicide since that time? As a state agent it is Stoller’s duty to report a crime when she sees a crime. A criminal investigation should have ensued. Overlooking corruption allows it to fester and spread and that is exactly what she did. She concealed it. This is top-down corruption also. Sanchez is past President of the Federation of State Physician Health Pr0grams (FSPHP) and his accomplice is the VP of Laboratory Operations at the drug testing lab-an unethical tone-at-the-top if there ever was one.
Some day a real rain will come and wash all the scum off the streets- Robert De Niro
Massachusetts Public Records – House Bill 4333
On June 3, 2016, Governor Charlie Baker signed into law the first update to Massachusetts’s public records law since 1973. The law seeks to make government entities more accountable, accessible, and efficient in their management of requests for information and mandates that each state agency delegate at least one employee to be a “records access officer.” The bill also imposes a shorter timeframe to respond to record requests. Agencies have a 10-day window to produce the requested documents or to respond and if they refuse or are unable to produce a record within 10 days they must notify the requestor and if an agency agrees to provide records outside the 10 day window it only has 15 days to do so.
An attorney must have a factual basis for alluding to, offering or relying on evidence and that factual basis may not be wishful thinking. There are two requirements for a factual basis — an attorney’s subjective belief and objective evidence to support that belief.
It is now established that no objective evidence exists. Not a shred of evidence exists. Not a single date-point with a reliable timestamp is chronologically consistent with these documents being before the board.
On June 3, 2016 Governor Baker signed House Bill 4333 imposing greater accountability on state agencies when responding to public records requests. This includes shorter time frames to respond to requests (10-days for most), the provision of complete and legible records and appointing a Primary Records Access Officer to handle such requests. The new Public Records Law also subjects agencies to sanctions for failure to comply.with the new law.
On January 9, 2017 I submitted a Public Records Request through the Executive Office of Health and Human Services (EOHHS) Website for a dozen or so documents that had been submitted for board hearings but never directly addressed and containing textual content with evidence that was never weighed. Moreover, many of the documents provided direct evidence of crimes (no other is evidence needed).
All of these documents were provided to Board counsel Deb Stoller.
Today, Sunday March 12, is the beginning of daylight savings time. It also marks the beginning of Sunshine Week, a national celebration started in Florida 15 years ago to promote open government, transparency and accountability. Transparency is about shedding light. Transparency can bring accountability, and, often, meaningful reform.
In response to a request for documents submitted for specific board hearings the board has not provided a single satisfactory response. They have not been able to provide a single document that is chronologically consistent with it being considered at the board hearing for which it was submitted. I had no expectations they would and this was the precise point of my record request. These are documents that should exist but do not exist. The vault is empty. None of the documents are in the records because they were suppressed on arrival and never got to the full board. They never considered any of it. The records do not exist.
It has now been over two months and this shows how transparency is not just about shedding light on what is there but what is not there–transparency can also illuminate contrivances and lies. If these documents existed then they would have provided them long ago and this is all coming to lightas a result of Public Records Division staff enforcing new Public Records Law and they should be applauded for their integrity, honesty and genuine concern. In a culture of deference, impunity and apathy where giving allowances are the rule rather than the exception this agency deserves an A+ amidst a sea of D’s and F’s.
The majority of documents provided have illegible or missing dates. Undated documents have no value. Analyzing any dataset requires that data-points be annotated with reliable timestamps that signify when the textual content was created and this is especially important with records that accumulate over time. Documents with message content passed on to others must be annotated with reliable timestamps that signify when the textual content was received and acknowledged by the receiver.
The Board Records obtained June 2016 provided pretty clear evidence that the documents were concealed . The only documents with a decipherable date stamp included a December 15, 2011 letter requesting an attached “litigation packet” be provided to the board for consideration at a December 21, 2011 hearing, The documents are all date stamped January 17, 2012. (nearly one month after the hearing). AAG Bertram dismissed the timestamp and claimed it did not reflect when it was entered into evidence but when it was scanned into the computerized records. In truth they should be one and the same and if that is the case then where is the timestamp reflecting when it was entered into evidence? Bertram claimed this occurs after hearings not before. It all defies common sense.
The January 9, 2017 request specifically requested a copy of the documents from the “administrative record” compiled for the December 21, 2011 hearing but in response they returned the same documents provided December 15, 2011 but date stamped January 17, 2012 –nearly a month after the hearing.
The simple and straightforward request was made again and an appeal was filed requesting provision of the documents requested. Thankfully the Public Records Division staff attorneys have not accepted the logical fallacies and half-truths presented to deflect and dismiss a simple and straightforward request for documents. Supervisor of Records Rebecca Murray Ordered the board provide a revised response and we obtained every document related to the December 2011 “litigation packet” that exists and all of the materials that Bertram claims were retrieved from storage. All of it can be seen here:
It is a dataset with an N of 1. The only document retrieved from storage is the original December 15, 2011 letter requesting the “litigation packet” be submitted for consideration at the December 21, 2011 hearing and all of it is date-stamped January 17, 2012 and this precludes the existence of any earlier copies. No other copies exist!
Take a look at the letter and all of the pages of the “litigation packet” as they are pristine. No notations, initials, dates, scribbles or signatures. So how were these documents “considered” at the December 21, 2011 board hearing? At almost 50-pages did they all huddle around it or pass it around the room.
The simple fact is they were never considered by the board. They were sitting in a drawer for a month (my guess under a bunch of moon pies and diet cokes) and then put in the system well after the hearing so no one would notice.
In his cover letter RAO Dolan reiterates the ridiculous claim that the date-stamp reflects when it was “bulk-scanned ” into the electronic archives and not when it was “presented to the board.” What would be the purpose of putting timestamps on documents that have no meaning? This is a bald faced lie and I want to call him on it. Evidence presented for any hearing must be submitted and entered into the record before not after hearings. This is common sense but to put this to rest we can turn to the 2012 Manual for Conducting Administrative Adjudicatory Proceedings which outlines how administrative proceedings are conducted by professional boards. It was also edited by AAG Quinan, the Managing Attorney of the Administrative Law, Government Bureau–the Department AAG Bertram is part of The “administrative record” is listed as one of the “basic principles” in chapter 1 and is second only to “due process” M.G.L. c. 30A, § 11(8). An administrative record must be compiled for every board hearing and indexed. “The record is everything that is properly before the decision maker in rendering the decision.”
The manual makes it crystal clear that evidence must be compiled before hearings and anything not compiled before the hearing must be excluded! Bertram also claimed that “board staff” reviewed its records and minutes and retrieved from “off-site storage” the “materials” that were before the Board in December 2011.”
1 The Board’s staff has reviewed its records and confirmed this to be the case.
2 To be sure, and to put this matter to rest for the Court once and for all, the Board has retrieved from offsite storage those materials before the Board in December 2011. The documents that Dr. Langan claims were “suppressed” are in fact there—and this should not be surprising given the Board’s many orders since that time, all of which have disclaimed any reliance on the July 2011 PEth test.
3 The Board’s staff has confirmed this by reviewing its minutes and confirmed this to be the case.
It has now been confirmed that the only “materials” that exist are the documents themselves and they are dated January 17, 2012 and this does not confirm but refutes Bertram’s claims. In sum not a single data-point exists to support this document was before the board on December 21, 2011. Moreover, the document provides direct evidence of crimes (no other evidence is needed).
I have requested that Bertram either provide documentation to support his footnoted claims or reveal to the court the misrepresentations. As a government attorney he is obligated to reveal falsehood and perjury and I requested he do so. But instead of revealing no materials from off-site exist to support his claims he notified the court of his misrepresentation that by “offsite storage” he meant “basement”
He mentioned nothing about these major misrepresentations and dug his heels in deeper claiming that board staff did indeed “retrieve and review those documents” and claims his “footnote representation remains uncompromised.” His footnote representations no longer remain uncompromised. At this point I’d say they are pretty compromised–the false contrivances are in actual fact shattered.
The off-point Bertram letter can be seen here: ( Attachment B (6) ) “Uncompromised is a poor choice of words Mr. Bertram as “shattered” or “demolished” would be more appropriate. Bertram claimed agency level investigation confirmed documents were before the board in December of 2011
Bertram was also asked to address the “chain-of-custody error” misrepresentation. The documents show intentional fraud. This is no error. The laboratory fraud seen here is similar to that of Annie Dookhan but the documents here show both of the parties involved; a state physician health program and one of the labs contracted by state physician health programs nationwide. Precise and detailed documentation of forensic fraud was provided to a state attorney in 2011 but she concealed the documents. . I pointed this out to Bertram from the beginning and I also told him of all of the suicides that have occurred because of bogus tests just like this one. He did not seem to care. I notified him of another one here in Massachusetts; a good doctor and a good person who was also subject to falsified testing and injustice involving the same actors. I am hopeful that the transparency being provided here will lead to accountability. Both of these attorneys need to be held accountable.
An attorney must have a factual basis for alluding to, offering or relying on evidence and that factual basis may not be wishful thinking. There are two requirements for a factual basis — an attorney’s subjective belief and objective evidence to support that belief.
It is now established that no objective evidence exists. Not a shred of evidence exists.
Not a single date-point with a reliable timestamp is chronologically consistent with these documents being before the board.
Please donate to my Gofundme- At this point I really need funding to mount a quick and effective response to these new developments. Exposing these crooked attorneys would be a great step forward for all of PHP reform. Please help me out.


 Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).
Diagnostic test accuracy is simply the ability of the test to discriminate among alternative states of health (Zweig and Campbell, 1993).








 Oppression that is clearly inexorable and invincible does not give rise to revolt but to submission. Simone Weil
Oppression that is clearly inexorable and invincible does not give rise to revolt but to submission. Simone Weil The simple extortion scheme from the 1990s has now grown to around two dozen “PHP-approved” assessment and treatment centers and state boards require that only “PHP-approved” facilities be used and specifically excludes non “PHP-approved” facilities. The preferred facilities engage in “diagnosis rigging” and false diagnoses to warrant unneeded treatment. The labs are willing to engage in laboratory misconduct and will create a falsely positive test at client request. It is a closed incestuous system in which the PHP serves as the Axis of Control and everything is kept not just close-to-the-cuff” but up the sleeve. This has led to pathological opportunism and promiscuous interaction between the PHPs-assessment center-lab conglomerate, regulators and medical boards and the legal profession which includes attorneys ostensibly representing doctors who will not bite the hand that feeds them-mostly carpetbagger board attorneys and former AAGs who hopped over to the more lucrative side doctors who are actually carpetbaggers who hopped over to the other side after proving to the racket they had no scruples and the current pseudosymbiosis damages everyone but the psychopaths, bullies and clowns lining their pockets from the racket.
The simple extortion scheme from the 1990s has now grown to around two dozen “PHP-approved” assessment and treatment centers and state boards require that only “PHP-approved” facilities be used and specifically excludes non “PHP-approved” facilities. The preferred facilities engage in “diagnosis rigging” and false diagnoses to warrant unneeded treatment. The labs are willing to engage in laboratory misconduct and will create a falsely positive test at client request. It is a closed incestuous system in which the PHP serves as the Axis of Control and everything is kept not just close-to-the-cuff” but up the sleeve. This has led to pathological opportunism and promiscuous interaction between the PHPs-assessment center-lab conglomerate, regulators and medical boards and the legal profession which includes attorneys ostensibly representing doctors who will not bite the hand that feeds them-mostly carpetbagger board attorneys and former AAGs who hopped over to the more lucrative side doctors who are actually carpetbaggers who hopped over to the other side after proving to the racket they had no scruples and the current pseudosymbiosis damages everyone but the psychopaths, bullies and clowns lining their pockets from the racket.
 One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model.The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the LDT drug and alcohol testing and 12-step assessment and treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model.The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the LDT drug and alcohol testing and 12-step assessment and treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.





 Bertram also claims PHS has not committed any crimes because they have not been charged with any crimes. This is called denying the antecedent or inverse error. It is a logical fallacy where the consequent is an indicative conditional claimed to be false because the antecedent is false. ( A, then B; not A, therefore not B). If it is raining, then the grass is wet.It is not raining.Therefore, the grass is not wet.The argument is invalid because there are other reasons for which the grass could be wet such as spaying it with a hose. There are multiple reasons for which someone who committed a crime has not been charged with a crime.There is always a time-frame between the two and many who commit crimes never get caught. Luck, stealth, cleverness, and multiple other variables might be involved. Jimmy Savile molested and raped scores of children for decades and he was never caught. As a major fundraiser for hospitals this fiend had free rein to prey on sick and helpless little kids in hospital beds .
Bertram also claims PHS has not committed any crimes because they have not been charged with any crimes. This is called denying the antecedent or inverse error. It is a logical fallacy where the consequent is an indicative conditional claimed to be false because the antecedent is false. ( A, then B; not A, therefore not B). If it is raining, then the grass is wet.It is not raining.Therefore, the grass is not wet.The argument is invalid because there are other reasons for which the grass could be wet such as spaying it with a hose. There are multiple reasons for which someone who committed a crime has not been charged with a crime.There is always a time-frame between the two and many who commit crimes never get caught. Luck, stealth, cleverness, and multiple other variables might be involved. Jimmy Savile molested and raped scores of children for decades and he was never caught. As a major fundraiser for hospitals this fiend had free rein to prey on sick and helpless little kids in hospital beds .




 An attorney must have a factual basis for alluding to, offering or relying on evidence and that factual basis may not be wishful thinking. There are two requirements for a factual basis — an attorney’s subjective belief and objective evidence to support that belief.
An attorney must have a factual basis for alluding to, offering or relying on evidence and that factual basis may not be wishful thinking. There are two requirements for a factual basis — an attorney’s subjective belief and objective evidence to support that belief.

 In response to a request for documents submitted for specific board hearings the board has not provided a single satisfactory response. They have not been able to provide a single document that is chronologically consistent with it being considered at the board hearing for which it was submitted. I had no expectations they would and this was the precise point of my record request. These are documents that should exist but do not exist. The vault is empty. None of the documents are in the records because they were suppressed on arrival and never got to the full board. They never considered any of it. The records do not exist.
In response to a request for documents submitted for specific board hearings the board has not provided a single satisfactory response. They have not been able to provide a single document that is chronologically consistent with it being considered at the board hearing for which it was submitted. I had no expectations they would and this was the precise point of my record request. These are documents that should exist but do not exist. The vault is empty. None of the documents are in the records because they were suppressed on arrival and never got to the full board. They never considered any of it. The records do not exist. It has now been over two months and this shows how transparency is not just about shedding light on what is there but what is not there–transparency can also illuminate contrivances and lies. If these documents existed then they would have provided them long ago and this is all coming to light as a result of Public Records Division staff enforcing new Public Records Law and they should be applauded for their integrity, honesty and genuine concern. In a culture of deference, impunity and apathy where giving allowances are the rule rather than the exception this agency deserves an A+ amidst a sea of D’s and F’s.
It has now been over two months and this shows how transparency is not just about shedding light on what is there but what is not there–transparency can also illuminate contrivances and lies. If these documents existed then they would have provided them long ago and this is all coming to light as a result of Public Records Division staff enforcing new Public Records Law and they should be applauded for their integrity, honesty and genuine concern. In a culture of deference, impunity and apathy where giving allowances are the rule rather than the exception this agency deserves an A+ amidst a sea of D’s and F’s.