Dictatorships can be indeed defined as systems in which there is a prevalence of thinking in destructive rather than in ameliorative terms in dealing with social problems. The ease with which destruction of life is advocated for those considered either socially useless or socially disturbing instead of educational or ameliorative measures may be the first danger sign of loss of creative liberty in thinking, which is the hallmark of democratic society. All destructiveness ultimately leads to self-destruction—Leo Alexander
The importance of recent articles published on Medscape and in the British Medical Journal critical of state Physician Health Programs (PHPs) cannot be overemphasized. Physician Health Programs- More Harm Than Good? by Pauline Anderson broke new ground as it was the first mainstream medical publication to address the serious concerns so many of us are aware of but can do nothing about. Jeanne Lenzer’s “Physician health programs under fire” published in the British Medical Journal (BMJ) shines further light on state physician health programs and discusses the lack of transparency, oversight and accountability and profit motive of these programs. Direct and serious questions that deserve direct and serious answers. What we need now is fuel for the fire. We need a conflagration and we need to name the enemy and that enemy is the Federation of State Physician Health Programs (FSPHP). The FSPHP is both an illegitimate authority and an irrational authority and this is easily proved.
Physician Health Programs (PHPs) were Originally funded by medical societies and staffed by volunteers and existed in every state by 1980., The equivalent of Employee Assistance Programs (EAPs) for other occupations. Their purpose was to help sick doctors and protect the public from harm. Over time, however, these programs have been subverted by special interest groups representing the drug and alcohol testing, assessment and treatment industries whose primary agenda is to sell the “PHP-Blueprint” to other occupations and groups. This is being done by falsely claiming unparalleled success for doctors treated by PHPs and they are touting it as , the “new paradigm” when in reality this model. subjects doctors to all manner of abuse in a system of institutional injustice and a culture of harm. Many of these horror stories were told in the comments section of the Medscape article and a subsequent article by Dr. Pamela Wible, MD entitled Do Physician Health Programs Increase Physician Suicides?
The stories we have heard are articulate, consistent, believable and very sad. Many of those who were previously silent out of fear and due to threats have now come forward. It can no longer be ignored or deflected. The Federation of State Physician Health Programs (FSPHP), however, has remained silent. We are hoping this will garner some interest in the mainstream media. The FSPHP needs to be held accountable for their actions. This includes both answerability and justification for their actions. The silence and inane answers of FSHPH and its President Doris Gunderson speaks volumes.
“Science under dictatorship becomes subordinated to the guiding philosophy of the dictatorship.” So begins Medical Science Under Dictatorship1 written in 1949 by Leo Alexander and published in the New England Journal of Medicine. Alexander acted as consultant to the Secretary of war and the Chief Counsel for the Nuremberg trials.
The guiding philosophic principle is Hegelian or “rational utility” and “corresponding doctrine and planning”, Alexander said “replaced moral, ethical and religious values” and Nazi propaganda was highly effective in perverting public opinion and public conscience. He explains how this expressed itself in a rapid decline in standards of professional ethics in the medical profession. This all “started from small beginnings” with subtle shifts in the attitudes of physicians to accept the belief that there is such a thing as “a life not worthy to be lived.”
In 1985 the British Sociologist G.V. Stimson wrote of a new form of professional control in the United States that had emerged in the preceding decade whose “success rests on the ability to take certain areas of conduct such as alcoholism and drug abuse (which are formally disciplinary issues) and handle them as diseases.”2
Stimson writes:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”2
Among these authoritative pronouncements was the use of specialized treatment centers. Many professionals were critical of these programs including Assistant Surgeon General John C. Duffy who criticized the “boot-camp mentality”4toward doctors and American Society of Addiction Medicine President Leclair Bissel who when asked in a 1997 interview when the field began to see physicians as a specialized treatment population replied “when they started making money..”.” 5
Amid reports of abuse, coercion and control in facilities using a doctor’s medical license as “leverage,” the Atlanta Journal Constitution ran a series of reports in 1987 documenting the multiple suicides of health care practitioners at one of these programs (5 while in the facility and at least 20 after discharge).6 Neither these suicides nor a large settlement against the same facility (finding a non-alcoholic doctor was intentionally misdiagnosed as an alcoholic and forced into months of treatment) for fraud, malpractice, and false imprisonment involving intentional misdiagnosis7 generated any interest among the medical community at large.
And by 1995 the door had closed as the Federation of State Physician Health Programs ( FSPHP ) relationship with the Federation of State Medical Boards (FSMB), the national organization responsible for the licensing and discipline of doctors, was forged. A 1995 Journal of Medical Licensure and Discipline(Vol82N3) contains articles outlining the high success rates of these programs in 8 states with an editorial comment from the FSMB that concludes:
“cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.”8
The Federation of State Medical Boards (FSMB) has approved any and all policy and regulation put forth by the impaired physician movement then organized under the Federation of State Physician Health Programs (FSPHP) with no apparent inquiry or opposition.
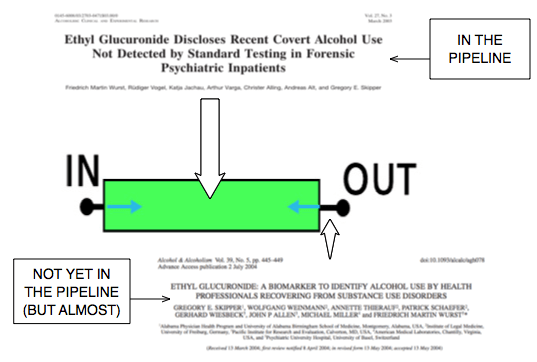
In 2003 Dr. Gregory Skipper, one of the key players of the impaired physician movement partnered with NMS labs to develop the alcohol metabolite ethyl-glucuronide (EtG) as a laboratory developed test13 14 he proposed be used as a monitoring tool for covert alcohol use in physicians after a pilot study involving just 14 psychiatric inpatients.15
The policy entrepreneurship this group so effectively uses to advance their goals can be seen in the August 25, 2004 Journal of Medical Licensure and Discipline which contains articles both presenting the problem 11 and providing the solution.11 The EtG was then introduced as an accurate and reliable indicator of covert alcohol use and the impact of this cannot be underestimated as it introduce to the market not only unregulated non FDA approved tests for forensic use but tests reaching further back into history then those used by workplace drug-testing programs.
 The limitations of any test needs to be understood both in the forensic and clinical context but there is a lot less flexibility in the forensic context when people’s liberties, freedoms or property rights ( as with a medical license) are in jeopardy.
The limitations of any test needs to be understood both in the forensic and clinical context but there is a lot less flexibility in the forensic context when people’s liberties, freedoms or property rights ( as with a medical license) are in jeopardy.
Sensitivity and specificity need to be carefully considered. The positive predictive value of a test is the true positives over the true positives plus false positives. If you are going to sanction somebody as a result of a single test that test needs to have 100% sensitivity.
When workplace drug testing was introduced debates over both the accuracy and scope of tests occurred. The employees right to privacy and the employers right to have a drug-free workplace were discussed with the general consensus being testing for impairment was a legitimate concern but preservation of private life should remain.
What was done here dissolves both.
PHP programs require abstinence from all substances including alcohol and strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Requiring abstinence from drugs and alcohol while using non-FDA approved Laboratory Developed Tests in monitoring programs is a dangerous combination. The suicides reported by the Atlanta Journal Constitution in 1987 were prior to the introduction of these tests. Adding these tests of unknown validity to an already abusive program of coercion and control would only worsen the situation.
I have been hearing of multiple suicides involving both the fear of results and false results. I have also been hearing of doctors who have killed themselves because they were suffering from depression but did not seek help as their fear of being ensnared into the PHP outweighed the need to get help.
Three decades after G.V. Stimson so accurately defined the impaired physician movement the impaired physician movement defines the professional control of medicine.. Their involvement in medical society physician health programs (PHPs) and treatment programs has evolved into absolute control of both. Pronouncements on physician impairment have evolved from insider’s claims to written edict. And their reach has extended from impairment due to drugs and alcohol to “potential impairment” and “relapse without use.” Their reach has extended from drug and alcohol impairment to all other aspects of medicine and the impact has been profound. Medicine has been subordinated to the guiding philosophy of the impaired physician movement and doctors are dying in droves du to institutional injustice.
How does the profession of medicine reconcile the fact that we have allowed an as yet non ABMS recognized “self-certification” specialty full reign over those who are ABMS recognized? How is it that we allow non-FDA approved Laboratory Developed Tests (LDTs) of unknown validity on doctors coerced into state Physician Health Programs (PHPs)? A recent debate in Washington calling for regulation of “clinical” LDTs just took place and the fact that they are being used for “forensic” purposes in doctors is incomprehensible. Has anyone noticed it is the same people introducing the tests who are claiming PHPs are the “gold standard,” trying to push them on other EAPs and calling for more widespread use of these tests?
The use of non-FDA approved Laboratory Developed Tests (LDTs) for drug and alcohol testing is currently limited to PHPs and the criminal justice system. (i.e. monitoring programs in which those doing the testing have power and those being tested have no power). That may soon change. See Drug Testing and the Future of American Drug Policy and The American Society of Addiction Medicine White Paper on Drug Testing describing the plans for widespread expansion of this drug testing to other groups including kids.
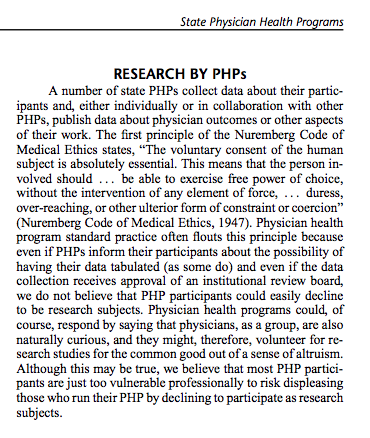
Those involved in the Massachusetts General Hospital Laboratory Medicine, Toxicology and addiction medicine departments looked critically at these tests and decided hands down against using them. Why? Because no evidence base exists and the potential harm far outweighs any perceived benefit. “Research” has been done on those being monitored by PHPs and the criminal justice system and Drs. J Wesley Boyd, M.D., PhD, and John Knight, M.D. of Harvard Medical School who collectively have over two decades of experience as Associate Directors with the Massachusetts PHP, Physician Health Services, Inc. addressed this research in a 2012 article published in the Journal of the American Society of Addiction Medicine entitle Ethical and Managerial Considerations Regarding State Physician Health Programs. The allegations that PHPs are engaging in research in violation of the Nuremberg code ( that was a direct result of the Nuremberg trials for which Dr. Alexander acted as consultant ) should have raised some eyebrows. It hasn’t.
If the ASAM becomes recognized by the ABMS as is now occurring “addiction medicine” specialists will inevitably join hospital formulary, clinical laboratory and ethics committees to erect the same scaffold seen in the PHPs and those with hidden agenda will be able to outvote those of good conscience and critical reasoning. Patient care will then be subordinated to the guiding philosophy of the impaired physicians movement.
This system of institutional injustice is killing doctors by suicide as the medical societies and Departments of Public Health have given PHPs full autonomy and authority and it is poised to impact patient care.
I challenge you to name any other company, organization, group or agency within or related to the profession of medicine and the field of science that is bereft of absolutely all transparency, regulation or oversight? It does not exist.
The PHP scaffold has deliberately removed themselves from all aspects of accountability including answerability, justification of actions and the ability of outside actors to hold them in judgment of any information provided by answerability. Heads I win, tails you lose. That is a big red flag in itself. and those not currently being held accountable may very well be after you next as their grand plan includes expansion to many other groups including workplace employee assistance programs (EAPs), the Department of Transportation, athletes, students and even kids!
Doctors have been afraid to talk about this for fear of being ensnared themselves. Those already in these programs have remained silent out of fear, threats and punishment. It is my hope that the articles published by Paula Anderson, Pamela Wible and Jeanne Lenzer will open the door to mainstream media coverage and result in the outrage this deserves. As Leo Alexander states in the closing words of this paper–“Yes, we are our brother’s keepers.
In The Argument of Fascism Ludwig von Mises wrote:
It cannot be denied that Fascism and similar movements aiming at the establishment of dictatorships are full of the best intentions and that their intervention has, for the moment, saved European civilization. The merit that Fascism has thereby won for itself will live on eternally in history. But though its policy has brought salvation for the moment, it is not of the kind which could promise continued success. Fascism was an emergency makeshift. To view it as something more would be a fatal error.








 The excerpt above is taken from the 2006
The excerpt above is taken from the 2006 














 and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability. PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.
PHCU Board counsel were additionally afforded the power to act as both “hearing-officers” on cases and present these same cases to the Board and recommend disciplinary action. This was by design also.