Just over a year ago, I wrote about the curious marketing of addiction treatment centers online, which used what I believed to be deceptive marketing practices. The email that arrived on Oct. 2, 2013 piqued my curiosity yet again. It was promoting a self-made infographic about “porn addicted” communities online. It came from a website called “Project Know.” Sounds interesting, right? The email started my second investigation into the seedy underbelly of the online marketing practices of rehab and addiction treatment centers. You know the ones, as you’ve probably seen at least one of their advertisements on TV, too. For most people, recovering from addiction is a difficult and trying process — marked by failure as much as it is success. Lack of scientific evidence aside, residential treatment centers (also known as addiction recovery centers or rehab centers) purport to offer a safe, supportive treatment environment for a person to detox from their addiction, typically for up to 30
The debate focused on the reliability and validity of a number of clinical tests currently marketed with unverified claims of accuracy such as those used for prenatal screening and Lyme disease. Notably absent from the discussions are the vast number of Laboratory Developed Tests tests being used for “forensic” drug and alcohol testing with the current FDA draft guidance stating simply:
“At this time, FDA will continue to defer oversight of the use of these tests in the forensics (law enforcement) setting to the existing system of legal controls, such as the rules of evidence in judicial proceedings and other protections afforded through the judicial process.”
The debate focused on the unreliability of lab tests such as those for Lyme disease but simply glossed over forensic drug and alcohol tests. Let’s think about this critically for a moment as a false positive test for Lyme disease can result in unneeded treatment and costs but a false drug or alcohol test can result in consequences far more grave such as loss of a child, loss of a professional license, and imprisonment. The results of a positive forensic test for drugs can be far reaching and permanent. So how did this happen?
The answer is simple. Money and profit. Lobbying groups such as the Drug and Alcohol Testing Industry Association (DATIA) ( which represents more than 1,200 companies involved in the drug and alcohol testing industry simply said “How dare you interfere with our war on drugs?” and the tests were off the table. The DATIA even employs its own DC based lobbying firm, Washington Policy Associates, and money talks. How dare anyone interfere with the profiteering ambitions to utilize junk-science in the mainstream population as specifically and explicitly spelled out in Robert Dupont’s 2012 keynote speech before the Drug and Alcohol Testing Industry Association and in the American Society of Addiction Medicine’s (ASAM’s ) White Paper on Drug Testing. These two documents should be required reading for anyone interested in civil liberties and fundamental freedoms. That they have been disregarded by most is incomprehensible and worthy of exploration. These documents both propose random mandatory and unnecessary and insurance paid drug-testing utilizing the medical profession (pediatricians to obstetricians to geriatricians) as a drug-testing collection agency using not only urine samples but also blood , oral fluid (saliva), hair, nails, sweat and breath.” It is all spelled out concisely-just read the papers.
Questions about the accuracy and marketing of Laboratory Developed Tests (LDTs) led to last years debate on whether or not the U.S. Food and Drug Administration (FDA) should regulate a subset of diagnostic tests currently exempted from oversight. Designed to bring clinical tests to market such as those for rare diseases that the costly FDA process would otherwise preclude, the LDT pathway bypasses Federal regulation and oversight. The LDT pathway additionally bypasses any semblance of accountability. It is an honor system and, as with any honor system, it is a system that can be exploited by the dishonorable.
Questions about the validity of these tests raised concerns over patient safety and this led to a call for oversight. Among those asking for regulation were Massachusetts Senators Edward J. Markey and Elizabeth Warren.
Opponents of regulation argued that the LDT pathway enables new and pioneering tests to be developed quickly and improve patient care. A viewpoint piece published in JAMA opposing regulation noted such advances have occurred “in large part because of the nimbleness of relatively small clinical and academic laboratories that can quickly respond to new medical findings and patient needs by rapidly and safely developing and improving laboratory-developed tests.”
But the LDT pathway does not require proof of test validity, that the test is actually testing for what it claims to be testing, and with no FDA oversight a lab can claim any validity it wants in marketing the test. There is no accountability. Proponents of regulation argue that this lack of oversight is a direct threat to patient safety and, as an opposing viewpoint piece in JAMA notes, a “patient’s life or death could hinge on whether a single, unregulated diagnostic test result is meaningful.”
The debate focused on the reliability and validity of a number of clinical tests currently marketed with unverified claims of accuracy such as those used for prenatal screening and Lyme disease. Notably absent from the discussions are the vast number of Laboratory Developed Tests tests being used for “forensic” drug and alcohol testing with the current FDA draft guidance stating simply:
“At this time, FDA will continue to defer oversight of the use of these tests in the forensics (law enforcement) setting to the existing system of legal controls, such as the rules of evidence in judicial proceedings and other protections afforded through the judicial process.”
The debate focused on the unreliability of lab tests such as those for Lyme disease but simply glossed over forensic drug and alcohol tests. Let’s think about this critically for a moment as a false positive test for Lyme disease can result in unneeded treatment and costs but a false drug or alcohol test can result in consequences far more grave such as loss of a child, loss of a professional license, and imprisonment. The results of a positive forensic test for drugs can be far reaching and permanent. So how did this happen?
The answer is simple. Money and profit. Lobbying groups such as the Drug and Alcohol Testing Industry Association (DATIA) ( which represents more than 1,200 companies involved in the drug and alcohol testing industry simply said “How dare you interfere with our war on drugs?” and the tests were off the table. The DATIA even employs its own DC based lobbying firm, Washington Policy Associates, and money talks. How dare anyone interfere with the profiteering ambitions to utilize junk-science in the mainstream population as specifically and explicitly spelled out in Robert Dupont’s 2012 keynote speech before the Drug and Alcohol Testing Industry Association and in the American Society of Addiction Medicine’s (ASAM’s ) White Paper on Drug Testing. These two documents should be required reading for anyone interested in civil liberties and fundamental freedoms. That they have been disregarded by most is incomprehensible and worthy of exploration. These documents both propose random mandatory and unnecessary and insurance paid drug-testing utilizing the medical profession (pediatricians to obstetricians to geriatricians) as a drug-testing collection agency using not only urine samples but also blood , oral fluid (saliva), hair, nails, sweat and breath.” It is all spelled out concisely-just read the papers.
The Birth of EtG: The Introduction and Marketing of Laboratory Developed Tests for “Forensic” Drug Testing Via a Lucrative Loophole
Numerous “forensic” tests of unknown validity using urine, blood, hair, fingernails breath and saliva have been developed and brought to market as LDTs since the first one was introduced in 2003 when ASAM physician Dr. Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.”1 With essentially no evidence base Skipper then claimed the alcohol biomarker “appeared to be 100 percent specific” in detecting covert use of alcohol for several days after ingestion based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male2
Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.
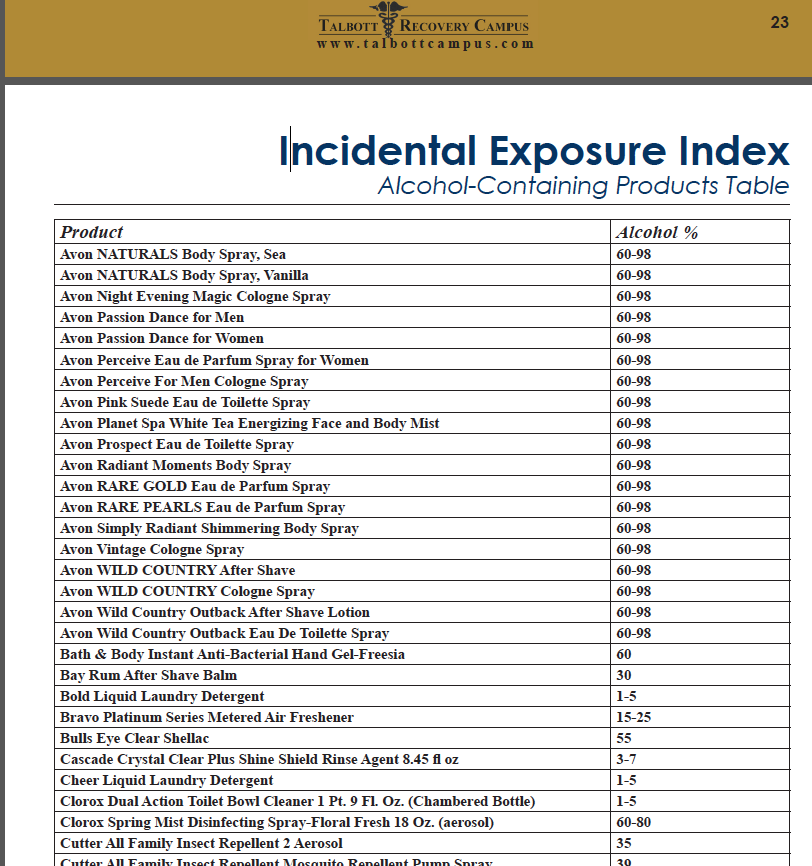
The test was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash3,4, hand sanitizer gel5, and nonalcoholic wine.6 Sauerkraut and bananas have even been shown to cause positive levels.7
Shortly after the EtG debuted, complaints began to accumulate from individuals testing positive who adamantly proclaimed they did not drink. Steadfast in their trust of expert opinion and the claimed accuracy of EtG, the complaints of the accused were largely disregarded by those doing the monitoring. People lost their licenses, jobs, careers, and reputations. Others lost their freedom or had their children taken away. It is unknown how many died by suicide.
There have been multiple lawsuits filed since the introduction of the EtG including a class-action suit, but these were inevitably met with a well-funded and deep legal defense and their “experts.” The labs have taken a “stand your ground” position yielding either dismissals or in favor of the defense. As a new to the market lab with no prior evidence-based research in forensic testing prior to its implementation and use for forensic testing, the proponents of EtG testing had no meaningful opposition in terms of a scientific body of facts and evidence and no credible voice to present it. With the only “experts” in EtG validity being those who introduced and promoted its use there were no counter-forces. Those suffering the consequences of a false-positive test had no recourse. But as the toll of mayhem increased it eventually reached a tipping-point where others began to take notice.
In 2006 the Wall Street Journal reported the problems with the EtG to the general public,8 and SAMHSA issued an advisory stating that “legal or disciplinary action based solely on a positive EtG…. is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”9
But this did not stop the Federation of State Physician Health Programs from using the EtG on physicians being monitored. Instead they instructed doctors to avoid anything potentially containing alcohol including hand sanitizer which a 2011 study found could result in EtG concentrations of almost 2000 ug/L. 10 To continue to justify the use of EtG they added other LDTs as confirmation tests of LDTs such as EtS and PEth– Junk Science to confirm junk science. Nonsensical smoke-and-mirrors antithetical to science and evidence-based medicine.
Since the birth of the EtG a variety of tests have been introduced and marketed as LDTs utilizing nails, blood, hair, breath and urine—all with unknown validity but marketed without constraint. No regulation, oversight or accountability exists.
Expanding Laboratory Developed Tests to Test Everyone: The ASAM White Paper on Drug-Testing and the “New Paradigm”
Although the current use of these tests is limited to the criminal justice system and professional monitoring programs this may soon change as the American Society of Addiction Medicine is proposing a “new paradigm” of zero-tolerance random widespread drug and alcohol testing. This is outlined in the ASAM White Paper on Drug Testing and described by Robert Dupont in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) annual conference in 2012.
As the consequences of a single unregulated “forensic” test result can be grave, far-reaching and even permanent it is critical that these tests be included in the debate on regulation of LDTs.
Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.11
Expert opinion is the lowest level of evidence available in the EBM paradigm.12,13Fortunately, the scientific method and Cochrane type critical analysis of the available evidence is a tool to help people progress toward the truth despite their susceptibilities to unconscious confirmatory bias or conscious confirmatory distortion .14 Unfortunately, no one has used these tools address they panoply of tests of unknown validity that have already entered the market ; poised to be used on virtually everyone.
It has now been 18 months since my Open Letter to Elizabeth Warren and the response thus far has been silence. Not a word since then.
Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcohol Clin Exp Res. Mar 2003;27(3):471-476.
Costantino A, Digregorio EJ, Korn W, Spayd S, Rieders F. The effect of the use of mouthwash on ethylglucuronide concentrations in urine. Journal of analytical toxicology. Nov-Dec 2006;30(9):659-662.
Reisfield GM, Goldberger BA, Pesce AJ, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. Journal of analytical toxicology. Jun 2011;35(5):264-268.
Rosano TG, Lin J. Ethyl glucuronide excretion in humans following oral administration of and dermal exposure to ethanol. Journal of analytical toxicology. Oct 2008;32(8):594-600.
Hoiseth G, Yttredal B, Karinen R, Gjerde H, Christophersen A. Levels of ethyl glucuronide and ethyl sulfate in oral fluid, blood, and urine after use of mouthwash and ingestion of nonalcoholic wine. J Anal Toxicol. Mar 2010;34(2):84-88.
Musshoff F, Albermann E, Madea B. Ethyl glucuronide and ethyl sulfate in urine after consumption of various beverages and foods–misleading results? Int J Legal Med. Nov 2010;124(6):623-630.
Helliker K. A test for alcohol–and its flaws. The Wall Street Journal2006.
Administration SAaMHS. The role of biomarkers in the treatment of alcohol use disorders. In: Advisory SAT, ed2006:1-7.
Reisfield GM, Goldberger BA, Crews BO, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after sustained exposure to an ethanol-based hand sanitizer. Journal of analytical toxicology. Mar 2011;35(2):85-91.
Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. Jan 13 1996;312(7023):71-72.
Shaneyfelt TM, Centor RM. Reassessment of clinical practice guidelines: go gently into that good night. JAMA. Feb 25 2009;301(8):868-869.
Straus SE, Green ML, Bell DS, et al. Evaluating the teaching of evidence based medicine: conceptual framework. BMJ. Oct 30 2004;329(7473):1029-1032.
Haack S. Defending Science–Within Reason: Between Scientism and Cynicism. Amherst, N.Y.: Prometheus Books; 2003.
Are the ends or purposes of those managing physician health programs the same as or in accordance with those being managed by these programs?
Moreover, will the ends and purposes of the physician health model of care be in accordance with the ends and purposes of those who will potentially be managed by this model of care in the “New Paradigm?
Employee assistance programs (EAPs) evolved from the “industrial” or “occupational” alcohol programs (OAPs) of the 1940s that were developed by companies to address alcohol abuse and its impact on the workplace. The first of these programs was developed by Dupont de Nemours and Company from 1941-1944 followed by Kodak in 1945 (Royce and Scratchley, 1989). These programs were typically staffed by a recovering alcoholic employee working in cooperation with corporate medical departments or a union health clinic and the sole referral source was to the recently formed self-help group Alcoholics Anonymous (AA). The primary intervention was to “confront the alcoholic’s job performance decline and denial using possible job loss as leverage toward seeking help.”
With time these programs broadened to include other issues that could potentially impact job performance. Worker Assistance Programs (WAPs) emerged in the 1950s when companies such as Consolidated Edison, Standard Oil of New Jersey, and American Cyanamid extended their alcoholism programs to also address mental health issues in their employees (Roman, 1981; Steele, 1995).
In the 1970s EAP-related legislation was passed and this markedly increased the number of these workplace programs. The Hughes Act ( Public Law 91-616 ) established the National Institute of Alcohol Abuse and Alcoholism (NIAAA) as part of the United States Department of Health and Human Services (USDHHS) and these organizations subsequently developed guidelines applicable to both the public and private sectors. Public Law 92-255 mandated their existence at all federal agencies and military institutions and in 1972 the Hughes Act was amended to also include drug abuse (Public Law 92-255 ). The amendment also required USDHHS Guidelines serve as the model for all federal programs. On September 15, 1986 President Ronald Reagan signed Executive Order 12564 stating a desired goal of achieving a Drug-Free Federal Workplace. This use of drug testing by governmental agencies then led to an increase in drug-testing by private employers and by 1986 more than a quarter of Fortune 500 companies were drug-testing job applicants
Another significant development was the formation of private EAP firms that began to offer EAP services and drug-testing via contracts with employers. One such example is Bensinger, DuPont & Associates (BDA) which was founded in 1982 by former DEA Chief Peter Bensinger and National Institute on Drug Abuse (NIDA) founding director Robert Dupont. BDA became the sixth largest employee assistance program (EAP) provider in the United States and provided workplace drug testing and other services to some 10-million employees of companies such as Kraft Foods, American Airlines, Johnson & Johnson and the Federal Aviation Administration (FAA). On December 1, 2015 Bensinger, DuPont & Associates was acquired by the Canadian firm of Mourneau Sheppel which employs 4000 plus individuals and has approximately 20,000 clients ranging from small businesses to some of the largest corporations in North America.
The company now known as BDA Moreau Sheppel represents the largest employee assistance program (EAP) provider in the entire world.
Ethical Considerations in Workplace Drug-Testing and EAP Management
EAPs can be managed internally by staff employees of a company or organization who contract with outside vendors for drug-testing or externally by an EAP provider such as BDA Moreau Sheppel. The primary goal is to address an employees problem (such as a substance abuse or mental health issue) before that given problem impacts job performance. In this way EAPs are viewed as mutually beneficial; they provide timely help to an employee experiencing a problem in addressing that problem and at the same time potentially avert absenteeism, poor work performance, accidents and termination of a valuable employee. They are designed to help both the employee and the employer in a “win-win” situation. The goals, therefore, should be identical. The goals should be convergent.
Although many of these programs offer mental health counseling and other such services, the core function of EAPs does not include diagnosis or treatment but to facilitate and ascertain diagnosis and treatment. Those referred to EAPs (either through self-referral or by someone else) are assessed and referred to outside sources, either individual practitioners or institutional agencies, that have expertise and experience in assessing and diagnosing the presenting problem. It is the EAP’s function to oversee and make sure that the presenting problem is not only properly assessed, addressed, diagnosed and treated (if indicated) but that the presenting problem remains managed and under control. This requires a period of monitoring or oversight to provide reassurance; progress reports from supervisors, compliance reports from treatment providers, and periodic drug and alcohol testing (if the problem involved substance use) are all part and parcel of a typical EAP.
EAPs have two primary business relationships: 1) a network of individuals and/or programs to which they refer individuals for assessment and treatment, and 2) laboratories capable of performing drug and alcohol testing. The integrity of an EAP is therefore dependent on the integrity and quality of its referral sources and laboratory operations. Those assessing, testing and treating must have education, experience and expertise in assessing, testing and treating the problems presented to them. They must be valid and reliable and it goes without saying that any and all assessment, testing and treatment must be objective, honest and without any conflicts-of-interest.
This topic is addressed in the book Employee Assistance Programs: What Works and what Doesn’t by Lawrence Mannion in which he discusses the notion of “control” in the context of managed mental health care. For those wishing to control any direction, entity or circumstances pertaining to these types of services Mannion states:
“..if the ends or purposes of those doing the controlling are in accord with the ends or purposes intrinsic or inherent in the thing being managed there is no conflict.”(page 133).
A 2001 study that looked at EAP professionals perceptions of ethical issues related to their business practices found that 22% of those surveyed identified “referrals” and “ownership structures” as among the most important and critical ethical issues facing the industry (Sharar, White, and Funk, 2001). Many of the respondents expressed concerns that the organizations owning and operating EAPs expected them to generate treatment revenue via a pattern of preferential referral to specific programs or practitioners and were concerned that this financial conflict-of-interest undermined the fundamental obligation of providing “neutral” and “objective” assessments to individuals with problems. To prevent the appearance of unethical conduct the recommendation below were made.
-Fully disclosing (to both employer and client) any affiliations with proposed referral options;
.-Offering an “objective” presentation of more than one referral option to the client;
-Providing clinical justification that the referral is in the best interests of the client;
-Refusing to accept any direct gain or financial remuneration for referring clients;
-Instituting a peer review program to monitor and evaluate the quality and appropriateness of referrals; and
-Developing a utilization/service summary report for employers containing detailed information on patterns of referral for continuing care and treatment.
In 1998 the American Medical Associations Council on Ethical Affairs suggested that incentive programs should be based on quality (rather than quantity) of services or referrals and that linking financial incentives to individual treatment decisions should be avoided (AMA, 1988). In summary any and all referrals need to be objective, honest and fair. They need to be reliable and valid. So too does any and all drug-testing. Most employee drug-testing follows a standardized protocol. Although errors do occur, the procedures followed by the vast majority of employee assistance program providers aim to minimize error. Most programs were implemented and evolved in collaboration with unions or other groups working on behalf of the best interests of the employee.
When drug testing initially entered the workplace many issues had to be worked out. Those in favor of drug-testing insisted that they had the right to demand a drug-free workplace and pointed to decreased productivity, increased accidents and absenteeism as potential consequences of drug abuse. Opponents challenged the constitutionality and reliability of drug-testing and also emphasized the necessity of distinguishing work life from private life. If a person smoked a joint on the weekend, they reasoned, it is no concern of management so long as they performed competently come Monday. Many in the medical community dismissed mandatory drug testing at the time as “chemical McCarthyism.” Nevertheless, drug-testing for better or for worse did enter the workplace. Most of these programs were implemented with the oversight and collaboration of unions or some other group advocating for the rights and interests of those being tested. Procedures and protocols were discussed, deliberated and had to be agreed on before implementation. In his 1984 book Designing Employee Assistance Programs, David Masi emphasizes the need for the close involvement of unions in workplace drug-testing and other EAP services in order to “protect employee rights”as well as the employers responsibilities in doing so (Masi, 1984). Most programs simply followed the already established Federal Workplace Drug Testing Guidelines and this is still the case for most EAPs today. The Mandatory Guidelines for Federal Workplace Drug-Testing Programs provide strict procedure and protocols specifically designed to protect the rights of those being tested. The Department of Transportation (DOT), United States Nuclear Regulatory Commission, and many other safety-sensitive organizations follow these stringent guidelines which include only using certified labs, strict chain-of-custody procedures and Medical Review Officer (MRO) assessment of all positive tests to rule out alternative explanations or “innocent-positives” (such as a prescribed drug). It is also the job of the MRO to verify that strict chain-of-custody was maintained from the collection of the sample to its final analysis. Additionally, only FDA approved drug-testing methods are utilized. This strict protocol assures a high level of validity and reliability (although mistakes can and do occur) to reduce the risk of someone being falsely labeled as a drug or alcohol user. False-positive-tests are absolutely unacceptable as the results of a positive drug-test can be grave, far-reaching and sometimes even permanent.
Physician Health Programs (PHPs)
Physician health programs (PHPs) are basically just employee assistance programs (EAPs) for doctors. They evolved from 1970’s “impaired physicians programs” much like EAPs evolved from the occupational alcohol programs (OAPs) of the 1940s. These programs were designed to both help sick doctors and protect the public in the same manner EAPs were designed to help sick employees and protect a company. The mechanics and mentality should be exactly the same. If the PHP feels a doctor is in need of an assessment he or she is then referred to an outside facility for evaluation (and treatment if that is indicated and in this system “treatment” is virtually guaranteed. The PHP then monitors the doctor for a period of time (typically five-years) to make sure that the problem remains under control. Monitoring inevitably includes at least weekly abstinence based substance abuse testing (including alcohol) using non-FDA approved laboratory developed tests (LDTs) no matter what the presenting problem. As with EAPs, one can self-refer to these programs or be referred by someone else and the latter can be done anonymously and with guaranteed confidentiality for the referrer.
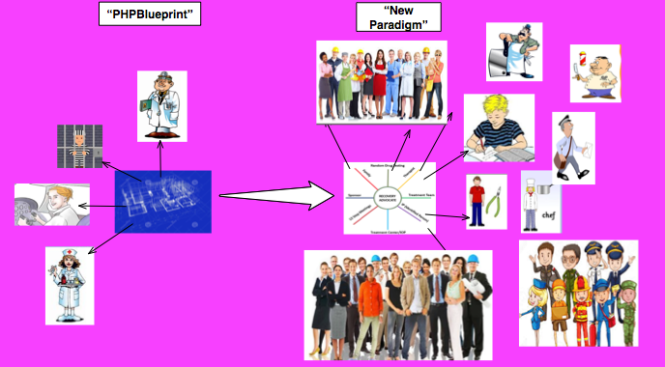
Although this model of EAP management is currently just being used on doctors, nurses, and other health care professionals; parts of the criminal justice system; and some areas of the airline industry, the grand plan is to move this model of care to other populations. Moving the “PHP-blueprint” to other occupations and populations is what is being deemed the “New Paradigm.”
The “PHP-blueprint” and the “New Paradigm”
The American Society of Addiction Medicine (ASAM) White Paper on Drug Testing describes the current practice of drug-testing in various contexts and explains how physicians and other healthcare providers can “use drug-testing to discourage non-medical drug use and ‘diversion’ of controlled substances” to “encourage appropriate entry into addiction treatment,” identify relapse and “improve outcomes of addiction treatment” through the use of “long-term post treatment monitoring.” The paper proposes random mandatory drug-testing by medical professionals (pediatricians to obstetricians to geriatricians) using not only urine but blood, oral fluid (saliva), hair, nails, sweat and breath.”
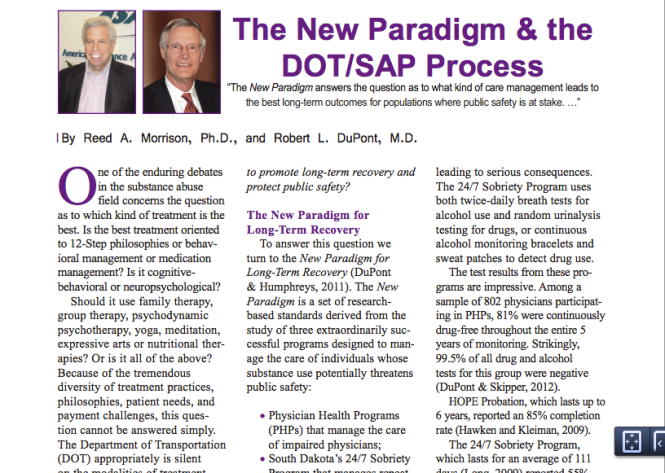
The White Paper’s writing Committee Chair, Dr. Robert Dupont, described this “New Paradigm” in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) in 2012 and claimed this model “sets the standard for effective use of drug testing” (Dupont, Drug Testing and the Future of American Drug Policy 2012) Dupont then proposed the “PHP-blueprint” be expanded to other workplace populations, healthcare students and schools. His audience, the Drug and Alcohol Testing Industry Association (DATIA) represents more than 1,200 companies involved in the drug and alcohol testing industry for profit and even employs their own DC-based lobbying firm, Washington Policy Associates.
“This model of care management for substance use disorders has been pioneered by a small and innovative group of the nation’s physicians in their determination to help other physicians save their careers and families while also protecting their patients from the harmful consequences of continued substance abuse. In fulfilling the professional admonition “physician: first heal thyself,” these physicians have created a model with wide applicability and great promise.” (Dupont, R., Skipper, G. 2012)
These six lessons are:
(1) zero tolerance for any use of alcohol and other drugs;
(2) thorough evaluation and patient-focused care;
(3) prolonged, frequent random testing for both alcohol and other drugs;
(4) effective use of leverage;
(5) defining and managing relapses; and
(6) the goal of lifelong recovery rooted in the 12-Step fellowships.
The “PHP-blueprint” is being promoted as “Gold standard” and a “New Paradigm” of recovery. In other words it is being proposed that the model of care management currently being used on doctors and managed by the FSPHP replace your current EAP. And like a faulty smoke-detector or a misfired Epipen you won’t realize or possibly even care about it until it happens.
The question for us, then, is this:
Are the ends or purposes of those managing physician health programs the same as or in accordance with those being managed by these programs?
Moreover, will the ends and purposes of the physician health model of care be in accordance with the ends and purposes of those who will potentially be managed by this model of care in the “New Paradigm?
The answer to the first question is a resounding “NO.” Complaints of coercion, abuse and other misconduct and fraud are rampant. Doctors are, in fact, being diagnosed with substance use disorder and other problems when they do not meet the diagnostic criteria for substance use disorder or other problems and being forced into unnecessary and unneeded treatment while those who do have substance use disorders and mental illness are being provided cookie-cutter treatment that is often inappropriate and inadequate treatment. Why? The money of course. Do the homework and follow the money.
It is necessary that we conform our thinking and behavior to objective reality rather than an illusion and the version of the physician health model being put forth by those promoting the “PHP-blueprint” and the “New Paradigm”is at marked variance to those being managed by the model and for further reading start with the following:
In Employee Assistance Programs: What Works and what Doesn’t, Mannion states:
“We need to spend less time making hyperbolic statements about change and entertaining grandiose ideas about strategic alliances and more time developing criteria or standards to determine what does and what does not belong under the canopy of employee assistance. More specifically what is that principle or principles on the basis of which we can develop a criterion or criteria to determine those activities that could legitimately come under the heading of employee assistance?” (page 165-166)
.
REFERENCES
American Medical Association, Council on Ethical and Judicial Affairs. Reports on Ethics in ManagedCare.Chicago, Ill.: American Medical Association Press, 1998
Dupont, R and G. Skipper “Six Lessons from State Physician Health Programs to Promote Long Term Recovery” Journal of Psychoactive Drugs 44 (1) 2012 (72-78)
Dupont, R. “Drug Testing and the Future of American Drug Policy” Presentation at the DATIA Annual Conference. San Antonio, Texas. April 19, 2012.
Jett K. Employee Assistance Programs–Government’s Role in an Expanding Field. In: Mecca AM, ed. Prevention 2000–A Public/Private Partnership: CHRF:69-81.
Manion, L. “Employee Assistance Programs: What Works and What Doesn’t” Praeger, Westport, CT. 2004
Massi, D. Designing Employee Assistance Programs. American Management Associations, New York, NY 1984
Roman P. From Employee Alcoholism to Employee Assistance. Journal of studies on alcohol. 1981;42(3):244-272.
Royce JE, Scratchley D. Alcoholism and Other Drug Problems: A Revised Edition of Alcohol Problems and Alcoholism. New York, NY: Simon & Schuster, Inc.; 1989.
Sharar D, W White, and R. Funk. “Business ethics and employee assistance/managed behavioral healthcare: A national survey of issues and challenges.” Journal of Behavioral Health Services and Research (submitted for peer review and publication April 2001).
Sharar, D., and W. White “Referrals and Ownership Structures: The first of two articles on the need for a revised ethic in employee assistance considers whether ownership structures can improperly influence EAP professionals.”
Steele P, Trice H. A History of Job Based Alcoholism Programs: 1955-1972. Journal of Drug Issues. 1995;19:511-532.
The New Paradigm for Recovery Making Recovery-and Not Relapse-the Expected Outcome of Addiction Treatment. Washington, D.C. March 2014 2014.
Making some serious gains. Let’s not lose the momentum. Please donate to my Gofundme here
The article below regarding one of my personal hero’s Dr. Oliver Sacks was published by my friend Dr. Bharani Padmanabhanm in the Valley Patriot Ledger. Thank God the current inept and illegitimate regime was not in place during Dr. Sacks’ formative years. His sympathetic and disruptive brilliance would have surely been snuffed out at its inception. How many Oliver Sacks are we losing today? One can only wonder.
The article below regarding one of my personal hero’s Dr. Oliver Sacks was published by my friend Dr. Bharani Padmanabhanm in the Valley Patriot Ledger. Thank God the current inept and illegitimate regime was not in place during Dr. Sacks’ formative years. His sympathetic and disruptive brilliance would have surely been snuffed out at its inception. How many Oliver Sacks are we losing today? One can only wonder.
Choose Dr. Oliver Sacks over Lucian Leape or Alice Newton
Dr. Oliver Sacks passed away last week from melanoma of the eye. He was best known for awakening people frozen into catatonic parkinsonism by the Spanish Flu and forgotten at the Beth Abraham Home for the Incurables. All they needed to awaken into normal life was a bit of levodopa. It was Dr. Sacks who thought of it and put his professional life on the line to give it to them. If you haven’t…
The essay below found on 123HelpMe.com entitled The “Doctor Who Saved Boston.” is about Dr. William J. Morgan, the brilliant hand surgeon who helped the Red Sox win the World Series for the first t…
The essay below found on 123HelpMe.com entitled The “Doctor Who Saved Boston.” is about Dr. William J. Morgan, the brilliant hand surgeon who helped the Red Sox win the World Series for the first time in 86 years. Morgan performed surgery on Curt Schilling’s severely damaged ankle that allowed him to pitch in game 6 of the ALCS against the Yankees when we were down three games to two.
No known medical or surgical options existed to allow Schilling the functionality to pitch. But just as things were looking bleak Dr. Morgan miraculously performed an unprecedented procedure he invented that allowed Schilling to pitch seven innings winning the game 4-2. He created a wall of stitches to hold Schillling’s torn tendon sheath in place before game 6’s win and again before game 2 of the World Series that we also won.
The memories of the Red Sox run to the 2004 World Series championship this year will remain in the minds of Sox fans forever. It is about Dr. William J. Morgan, a brilliant hand surgeon who performed a risky
Whether it is David Ortiz’s walk off performances against the Angels and Yankees, Manny Ramirez’s tape measure home runs, or Derek Lowe winning the clinching games of all three playoff series, Red Sox nation will not soon forget the memories that the “bunch of idiots,” as centerfielder Johnny Damon dubbed this year’s Sox club,provided them, nor will they forget the Sox all out assault on baseball and Boston sports history.
But of all the images the fans retain, of all the feelings they experienced, of all the heroes Sox nation put on an altar and worshipped – the most memorable has to be Curt Schilling pitching three games on an inured ankle, blood from broken sutures seeping through his sock and a look of obvious discomfort on his face, winning two, and capturing the heart’s of every member of Red Sox nation. images-37
But to understand the elation of the Nation and the reason that it has turned Curt Schilling into a God in the church that Cy Young, Ted Williams, and Carl Yaztremski built, we have to take a step back and remember the predicament that the Red Sox were in just over two months ago.
It was October 12, and the Yankees had beaten the Red Sox in Game one of the ALCS. It was only one game, but that familiar feeling was back. That familiar feeling that Red sox fans have of doom and gloom lingering just over the horizon returned.
Curt Schilling, the hired gun, the man who Sox management had brought in to beat the Yankees in just this situation, had not only lost the game, but looked utterly ineffective in doing so, allowing six runs in just three innings of work and the media was reporting that Schilling may not pitch again.
On June 10, reports came out on ESPN and in the Boston papers that Schilling had a minor injury to his ankle but that he would pitch through it and make his start that night and would not have to go on the disabled list.What came out later on in the papers was that Schilling had made the majority of his starts in the 2004 season only after undergoing shots of marcaine, which sportsinjuries.com describes as a long lasting local anesthesia that is used for pain management and works by blocking nerve sensations.The attitude that the Red Sox seemed to take toward Schilling’s injury was no harm, no foul, and after June little was heard about Schilling’s ankle, that is until October 5.October 5 was the beginning, and almost the end, of the Red Sox 2004 playoff run. It was a glorious, and infamous, day in Red Sox history. Curt Schilling pitched 6 and 2/3 strong innings at Anaheim, allowing just two runs and scattering nine hits as the Red Sox cruised to a 9-3 victory.
But late in the sixth inning, Schilling pulled up lame after fielding a slow roller down the first base line and throwing the ball over first baseman Kevin Millar’s head. He was favoring that same right ankle that had been hurting him all year.
Back to October 12, and the feelings of anxiety that every Sox fan from Maine to Rhode Island no doubt had in the pit of their stomachs. Questions were swirling around Boston. Just how serious was Schillings injury? Could he pitch again? Would he pitch again? Is there a God?
Jamie Musler, an assistant clinical specialist at Northeastern, put the injury into perspective.
Musler said that Schilling tore the tissue that covers his peroneal tendon, which sits in a small groove in the fibula and is partly responsible for moving and planting the foot. Musler said that this type of injury is caused by a traumatic event to the foot or ankle, like a significant ankle sprain, and when Schilling was moving his foot, the tendon was slipping out and causing an uncomfortable, but not necessarily painful, snapping sensation because the tendon was snapping across the fibula. This, Musler said, would directly affect foot mechanics and cause a huge problem in Schilling’s delivery.
And it would present a huge road block in Boston’s attempt to win a World Series title.
Schilling meant more to the 2004 Red Sox club than any other player. He was the tone setter and the ace, and without him the Sox would have no chance against the hated Yankees.
The Red Sox needed Schilling, because number two starter Pedro Martinez is not the fire balling Dominican dandy he used to be. And the Yankees, it seemed, had his number of late after he lost two late season starts to them, prompting Pedro to say in a press conference after one of those losses that he could “just tip my hat and call the Yankees my daddy.”
After Pedro, things got even bleaker, with inconsistent and fragile Derek Lowe, aging and unpredictable knuckleballer Tim Wakefield, and young, playoff inexperienced Bronson Arroyo filling out the rotation. These four hurlers are serviceable and talented major league pitchers, but they were not the automatic win that Schilling had proved himself to be in postseason’s past, especially in 2001, when he garnered co-MVP honors after defeating the Yankees in the World Series.
So in comes the man from behind the scenes. The man who would help the Red Sox end 86 years of playoff futility, Red Sox team doctor Bill Morgan, who talked about the injury and treatment in “Faith Rewarded,” the DVD that the New England Sports Network (NESN) recently released.
“It was a very unique situation. Either we did this or (Schilling) didn’t pitch,” Morgan said. “And he was determined that he was going to pitch, no matter what it took.” But what could Morgan do?
What followed was possibly the most publicized treatment of a sports injury in history. One could not turn on a New England news program or open up a New England paper without the top story being about Curt Schilling’s right ankle.
First, according to boston.com, the Red Sox front office brought in Dr. George H. Theodore, chief of foot and ankle service at Massachusetts General Hospital, to help Dr. Morgan try to create a brace to immobilize Schilling’s ankle while he pitched. The idea was that by eliminating movement of the ankle he would eliminate movement of the tendon and eliminate the sensation. But the problem, Schilling insisted, was that the sensation was altering his delivery, and that became apparent after his struggles in Game one of the ALCS. File that idea in the circular cabinet.
Next on the block, according to boston.com, was pair of customized cleats. Morgan had Reebok play around with different styles of cleats, from high tops to low tops, raised bottoms to lowered bottoms, in an attempt to find Schilling a comfortable medium. No dice. Schilling still could not get comfortable.
According to the Massachusetts Medical Board’s website, Dr. William Morgan is an orthopedic surgeon who specializes in hand surgery. He has his own private practice in Brighton, but his primary work setting is in hospitals. Morgan works out of several area hospitals and rehabilitation centers, including St. Elizabeth’s Medical Center of Boston and New England Baptist Hospital, New England Rehabilitation Services of Central Massachusetts, Worcester Medical Center, and University of Massachusetts Memorial Medical Center. Morgan also works out of the Massachusetts Hospital School.
Morgan got his degree from the Texas Medical College and Hospital in Galveston, Texas. He received post graduate training at the University of Massachusetts Medical Center. He continued his post grad training in hand and upper extremity surgery at the Roosevelt Hospital in New York, Brigham and Women’s Hospital, New England Baptist Hospital, and the Kantonspittal in Basle, Switzerland.
Morgan performed successful wrist surgery on one former Boston Red Sox superstar shortstop Nomar Garciaparra, allowing him to come back from what could have been a career altering injury as the All Star he was before he was injured.
The point is that Morgan is not some shaky med student on his first hospital residency. He has been around the block a few times and he knows his orthopedic surgery.
Musler said that with any injury, a doctor has to analyze it by thinking “what is the injury? What can we do to keep the tendon in place? If the feeling is throwing (Schilling) off, how do we help that?”
Morgan, it would seem, did just that, and came up with a new treatment, which he based off of the usual treatment for Schilling’s injury. Musler said that the usual treatment for the injury is to go in and deepen the groove that the peroneal tendon sits in. Musler showed me a video of the procedure in which surgeons cut away the tissue surrounding the tendon and the tendon sheath and then used a surgical drill and chisel to physically deepen the groove in the fibula that the tendon sits in. The surgeons then sutured the sheath back in place and closed the opening.
But Morgan and the Sox didn’t have that much time. They had four days. They went in, did the procedure, gave Schilling another marcaine shot, and, as they say, the rest is history.
Schilling came back and won game six against the Yankees. After the game, Morgan took out the sutures, Musler said, to avoid infection.
Morgan did the procedure again before Game two of the World Series, and Schilling would later say that had the series gone past four games he and Morgan had decided not to do the procedure again and that Schilling would shut it down for the rest of the series.
This time, Schilling was pitching on what is the biggest stage in sports, the World Series, against the best hitting team in baseball, the St. Louis Cardinals, whose line up featured Albert Pujols, the best young hitter in baseball and an MVP candidate, Scott Rolen, the RBI leader in the NL during the regular season, hard hitting and speedy shortstop Edgar Renteria, and two probable Hall of Famers in outfielders Larry Walker and Jim Edmonds.
Schilling was dominant. He made the heralded and hyped Cardinal offense look like a team of Little Leaguers as he pitched six strong innings allowing no earned runs and only four hits.
The rest, as they say, is history. The Sox would go on to sweep the Cardinals in four games, ending their 86 year dry spell of World Series titles and sending New England into a euphoria that it has still not recovered from.
But one has to wonder if there will be any lingering effects from the injury. Will Schilling be alright to pitch next year as the Sox try to repeat as champs?
Mary J. Hickey, an Assistant Clinical Specialist in the Northeastern department of Physical therapy, thinks so.
“Curt made an informed choice about his ankle. I don’t think there will be any long lasting damage,” Hickey said.
But Schilling is not out of the woods yet. Hickey said that Schilling faces at least four to six weeks in a cast, during which he will be seen often by Morgan and the Red Sox medical staff, and Musler said that Schilling faces five to six months of rehab to get back his range of motion, endurance, strength, and sports’ skill. Musler said that this could risk further injury if Schilling is not properly prepared for next season and presses when he is not ready.
Regardless of rehab and healing time, Curt Schilling and Red Sox fans are on cloud nine. The Red Sox are World Series champions for the first time in 86 years, and Sox fans have a new hero and new memories.
The memory of Curt Schilling, of him pitching hurt, grimacing in the dugout, bloody sock and all, will remain with everyone who saw it, even Yankees fans, forever. Schilling billed himself as the hired gun, a man who said in an interview with the Boston Herald before the ALCS that “he was not sure of any scenario more enjoyable than making 55,000 people from New York shut up.” But in the end he was so much more than just a hired gun, he was a hero in real red socks. And he made more than 55,000 people from Boston stand up and applaud as he became the newest Red Sox player to be canonized in the church of Red Sox nation, alongside Yaz, the Kid, Pudge and Cy.
And not to be forgotten is the man behind the scenes, the quiet and unassuming surgeon who made it all possible, Dr. William Morgan, whose name will be forever linked to Curt Schilling, the Red Sox and the 2004 World Series. He may not have thrown a pitch or swung a bat, but William Morgan saved the 2004 Boston Red Sox from being another team that just missed. And he saved Red Sox fans from finally having to utter those awful words – “wait ‘til next year.” But because of Bill Morgan and the entire Red Sox medical staff, next year is this year.
Please donate to my fund at: https://www.gofundme.com/PHPReformWe have dealt some significant blows and I would like to keep throwing some direct punches at the enemy but at this point it is getting difficult as financial issues…
These programs are a funnel for sociopaths and without restarting the problem will only get worse. This is what John Nash described would happen without counter-forces to keep their numbers low.


 Just over a year ago, I wrote about the curious marketing of addiction treatment centers online, which used what I believed to be deceptive marketing practices. The email that arrived on Oct. 2, 2013 piqued my curiosity yet again. It was promoting a self-made infographic about “porn addicted” communities online. It came from a website called “Project Know.” Sounds interesting, right? The email started my second investigation into the seedy underbelly of the online marketing practices of rehab and addiction treatment centers. You know the ones, as you’ve probably seen at least one of their advertisements on TV, too. For most people, recovering from addiction is a difficult and trying process — marked by failure as much as it is success. Lack of scientific evidence aside, residential treatment centers (also known as addiction recovery centers or rehab centers) purport to offer a safe, supportive treatment environment for a person to detox from their addiction, typically for up to 30
Just over a year ago, I wrote about the curious marketing of addiction treatment centers online, which used what I believed to be deceptive marketing practices. The email that arrived on Oct. 2, 2013 piqued my curiosity yet again. It was promoting a self-made infographic about “porn addicted” communities online. It came from a website called “Project Know.” Sounds interesting, right? The email started my second investigation into the seedy underbelly of the online marketing practices of rehab and addiction treatment centers. You know the ones, as you’ve probably seen at least one of their advertisements on TV, too. For most people, recovering from addiction is a difficult and trying process — marked by failure as much as it is success. Lack of scientific evidence aside, residential treatment centers (also known as addiction recovery centers or rehab centers) purport to offer a safe, supportive treatment environment for a person to detox from their addiction, typically for up to 30






 Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.
Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.







 Employee Assistance Programs (EAPs)
Employee Assistance Programs (EAPs) With time these programs broadened to include other issues that could potentially impact job performance. Worker Assistance Programs (WAPs) emerged in the 1950s when companies such as Consolidated Edison, Standard Oil of New Jersey, and American Cyanamid extended their alcoholism programs to also address mental health issues in their employees (Roman, 1981; Steele, 1995).
With time these programs broadened to include other issues that could potentially impact job performance. Worker Assistance Programs (WAPs) emerged in the 1950s when companies such as Consolidated Edison, Standard Oil of New Jersey, and American Cyanamid extended their alcoholism programs to also address mental health issues in their employees (Roman, 1981; Steele, 1995). Another significant development was the formation of private EAP firms that began to offer EAP services and drug-testing via contracts with employers. One such example is Bensinger, DuPont & Associates (BDA) which was founded in 1982 by former DEA Chief Peter Bensinger and National Institute on Drug Abuse (NIDA) founding director Robert Dupont. BDA became the sixth largest employee assistance program (EAP) provider in the United States and provided workplace drug testing and other services to some 10-million employees of companies such as Kraft Foods, American Airlines, Johnson & Johnson and the Federal Aviation Administration (FAA). On December 1, 2015 Bensinger, DuPont & Associates was acquired by the Canadian firm of Mourneau Sheppel which employs 4000 plus individuals and has approximately 20,000 clients ranging from small businesses to some of the largest corporations in North America.
Another significant development was the formation of private EAP firms that began to offer EAP services and drug-testing via contracts with employers. One such example is Bensinger, DuPont & Associates (BDA) which was founded in 1982 by former DEA Chief Peter Bensinger and National Institute on Drug Abuse (NIDA) founding director Robert Dupont. BDA became the sixth largest employee assistance program (EAP) provider in the United States and provided workplace drug testing and other services to some 10-million employees of companies such as Kraft Foods, American Airlines, Johnson & Johnson and the Federal Aviation Administration (FAA). On December 1, 2015 Bensinger, DuPont & Associates was acquired by the Canadian firm of Mourneau Sheppel which employs 4000 plus individuals and has approximately 20,000 clients ranging from small businesses to some of the largest corporations in North America.
 This topic is addressed in the book Employee Assistance Programs: What Works and what Doesn’t by Lawrence Mannion in which he discusses the notion of “control” in the context of managed mental health care. For those wishing to control any direction, entity or circumstances pertaining to these types of services Mannion states:
This topic is addressed in the book Employee Assistance Programs: What Works and what Doesn’t by Lawrence Mannion in which he discusses the notion of “control” in the context of managed mental health care. For those wishing to control any direction, entity or circumstances pertaining to these types of services Mannion states:
 These six lessons are:
These six lessons are: The “PHP-blueprint” is being promoted as “Gold standard” and a “
The “PHP-blueprint” is being promoted as “Gold standard” and a “










 No known medical or surgical options existed to allow Schilling the functionality to pitch. But just as things were looking bleak Dr. Morgan miraculously performed an unprecedented procedure he invented that allowed Schilling to pitch seven innings winning the game 4-2. He created a wall of stitches to hold Schillling’s torn tendon sheath in place before game 6’s win and again before game 2 of the World Series that we also won.
No known medical or surgical options existed to allow Schilling the functionality to pitch. But just as things were looking bleak Dr. Morgan miraculously performed an unprecedented procedure he invented that allowed Schilling to pitch seven innings winning the game 4-2. He created a wall of stitches to hold Schillling’s torn tendon sheath in place before game 6’s win and again before game 2 of the World Series that we also won.





