

Milton Friedman (July 31, 1912 – November 16, 2006) was an American economist who received the 1976 Nobel Memorial Prize in Economic Sciences
In an article written for the March 2015 Physician Health News, the official newsletter of the Federation of State Physician Health Programs (FSPHP) President Doris Gunderson reviews the history of the organization in honor of its 25th anniversary. She writes:
“In 1990 the FSPHP was born out of a need for individual state programs to work together in discussing and promoting best practices and especially to influence national public policy.”
For the last quarter century the FSPHP has pushed a plethora of both practice and policy (legal, regulatory and healthcare) that claims to assist state physician health programs in identifying, managing and monitoring impaired physicians and protect the public from harm.It was recently suggested by the Chief Editor of American Society of Addictions Medicine (ASAM) Weekly News that this same group take the helm in influencing public policy for addiction medicine at large (i.e. not just doctors but everyone from our kids to our pregnant mothers to our elderly) on a national organizational level.
It is time we examined both the authority and the knowledge claims on which they are based.
In her rebuttal to Pauline Anderson’s August 2015 Medscape article ‘Physician Health Programs: More Harm Than Good? Gunderson dismissed criticisms as “allegations rather than facts” and “second hand anecdotes.”
In response to allegations that PHPs have no oversight Gunderson comments:
“In fact, we operate under a microscope, answering to individual practitioners, medical boards, malpractice carriers, defense attorneys, state attorneys, medical societies, hospitals, medical schools and residency training programs. We are also accountable to patient safety entities and a Board of Directors.”
The list of organizations Gunderson has to “answer” to appears to be many of the organizations and societies that physician health programs interact with. She might as well add Blockbuster for getting her videos back on time. This is not meaningful oversight. Oversight equates with accountability and that requires answerability (the provision of information) and justification for one’s actions. It also requires the presence of an outside organization truly independent of the group that is able to sanction or punish individuals for wrongdoing or misconduct. No such organization exists for state physician health programs. Period. There is no organization that exists that is able to investigate a complaint of misconduct and provide sanctions. The same applies to their primary business associates, the assessment and treatment centers (because they are private pay and out-of-pocket) and drug and alcohol testing labs (because they use non-FDA approved tests). The entire racket is unaccountable and unexamined.
Kathryn Pyne Addelson warned that what we should fear most is “unexamined” authority. “Illegitimate politicization and rampant irrationality find their most fruitful soil when our activities are mystified and protected from criticism.”
This group has been protected from criticism for the better part of a generation. They have enjoyed making authoritative pronouncements as unexamined authority. Their power depends entirely on not being questioned as what is behind the curtain is flimsy and dredged, a Potemkin village. The recent Medscape and BMJ articles are revealing that confrontation with direct and precise questions results in nothing but logical fallacy, distortions and lies. They are utterly incapable of responding with a direct and precise answer. Gunderson’s response to absent oversight is just another example of this logical fallacy and distortion. This is not how rational authority responds. This is not how legitimate authority responds. I kindly invite her to debate this. I would like a back-and-forth to clarify. It is a simple question that deserves a simple answer and I know she follows my blog as she used her own name and e-mail address.
The cumulative comments on the articles critical of these programs are revealing a system of oppressions, injustices and illusions. A more recent article on Medscape, “One-Man Fight: MD Takes on State Medical Board, PHP” reports the same pattern of coercion, absence of due process and diagnosis rigging for sham peer review that I am hearing from doctors across the country. The comments section to this article are also overwhelmingly critical of PHPs. They are pertinent, articulate and precise and missing from them is any semblance of a rebuttal by the FSPHP, their apologists or anyone else. The writing is on the wall as they say. And for that reason we call upon all those of good will in both the medical profession and the public at large to join us in this confrontation with illegitimate, irrational and immoral authority.
- Gunderson D. Message From the President Twenty-Five Years: A Remarkable Journey. Physician Health News. 2015;20(March).
- Addelson KP. The Man of Professional Wisdom. In: Fonow MM, Cook JA, eds. Beyone Methodology: Feminist Scholarship as Lived Research. Bloomington: Indiana University Press; 1991:16-35.
Illegitimate Authority



A Call for Allies– Astute Comment Speaks for Itself– Question Authority!

Despite not being a physician, I have read many posts on your blog and I am horrified by what I have read. While I believe that physicians are being treated inhumanely by the PHPs, I do not think that the source of the problem is unique to their experience. In fact, I think the basis for this ideological takeover of “health” began in the 1980s when modern psychology became the predominant belief system (religion) in American society.
Many new ideas, based on the personal writings of psychologists, were introduced at that time. Their purpose was to tell us how to best live our lives. In order to get the public to buy into their agenda, the proposed ideas were formalized by pseudo-scientific “studies,” allegedly “proving” their worth.
For instance, can you remember anyone claiming to have had an “unhealthy relationship” in the 1970s? Not likely. In the 1970s no one had “relationships.” We had relatives (a word we can no longer use), friends, classmates, boyfriends, girlfriends, husbands, wives, colleagues, acquaintances, etc. And now what do we have? Relationships. Every connection we have to another human is now termed a relationship – family relationships, intimate relationships, work relationships, and so on. Now that everything is a relationship, the word has lost its meaning, and so has the specificity of human connections. Unfortunately, this change ushered in an era which can be defined by the imposition of superficiality on things which were once substantive.
I believe that living in such a superficial environment has led to nearly universal self-absorption and apathy. That may explain why so few people appear to be interested in your message, despite the fact that ignoring it will cause enormous harm to them in the future.
It is not only those with substance abuse or psychological problems who will be affected by the Religion of Psychology movement. Everyone will lose their rights and their freedom. But since most people have become stupid sheep, blindly following along instead of thinking for themselves and standing up for their rights, it will be difficult to prevent this loss.
Young people used to be the ones who championed causes. Youth and idealism went hand in hand. That was until political correctness made independent thought a “sin.” Like relationship theory, political correctness tells us who we are, what to think, and how to act. There is no room for individuality, no room for questioning, no room for discussion. This is very sad. It will not make for a more humane world. Instead, it will create a world where uniformity and blind conformity are mandatory. What was once life will be mere existence. And what was once meaningful will be perfunctory.
The leaders of the PHPs, and others like them, as overlords of the realm of modern psychology will force their religion on the world and will obtain control of every aspect of our lives in the name of health. This trend has driven me away from conventional medicine and has made me a loner. I have, however, found some hope from Bernie Sanders’ presidential campaign. Not only is he advocating for a more humane and equal society, and telling people to stand up to the one percent, but he has managed to get a lot of young people to support him.
I do not expect Sanders to win the nomination. But, I am holding out hope that the young people who agree with his message will take up his cause on their own and will fight for their future.
Perhaps you could appeal to those young people to join you in your fight. You would do well to join forces since you are both fighting for human rights and for a future which will still contain Humanity.

Share this:

Maneuvering



Share this:

The “Impaired Physician”–Increasing the Grand Scale of the Hunt

“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.” Father Cornelius Loos ( 1592 )

How Impaired Physicians Can be Helped–Medscape Business of Medicine Article Published February 24, 2015. Click on image to access
How can impaired Physicians be helped?
1. Impairment among physicians is growing: Why?
Answer: It is not. State Physician Health Programs (PHPs) are “diagnosing” impairment when there is no impairment. They are pathologizing the normal and expanding in scope to increase the grand scale of the hunt.
2. What’s the Prognosis for Impaired Physicians?
Answer: Not Good. Those who need help (the truly impaired) are afraid to get help for fear of being monitored by their state PHP while many of those ensnared by PHPs are not impaired. There is absolutely no oversight, regulation or accountability. This needs to be evaluated in the context of physician suicide. The system is one of institutional injustice and abuse of power.
3. Is your knowledge of physician impairment up-to-date?
Answer: No. This will only occur after an evidence-based Cochrane type review separates information from misinformation; An objective non-biased investigation by outside actors identifying any conflicts-of-interest, misconduct or lack of evidence-base in the current system and separating the art and science of the medical profession from the politicalization and exploitation of the medical profession.
The list of doctors on Like-Minded Docs solves the final piece of a puzzle. It explains why so many doctors across the country are claiming fabrication and manipulation of personality and cognitive tests to support nonexistent diagnoses at these “PHP-approved” assessment centers. The relationship between the state PHP’s and the “PHP-approved” assessment centers is the same as it is between the state PHPs and the corrupt labs.
As Drs. John Knight and J. Wesley Boyd note in Ethical and Managerial Considerations Regarding State Physician Health Programs, published in the Journal of the American Society of Addiction Medicine, this is what is known as “tailoring a diagnosis”–a euphemism for the political abuse of psychiatry. According to the Global Initiative on Psychiatry “Political abuse of psychiatry refers to the misuse of psychiatric diagnosis, treatment and detention for the purposes of obstructing the fundamental human rights of certain individuals and groups in a given society.” The shoe fits here. In fact it fits very well.

The Global Initiative on Psychiatry opposes the Political_Abuse_of_Psychiatry wherever it may occur and “supports those psychiatrists and psychiatric organizations that pressure the offending states to discontinue the practice and lobby vigorously those organizations which are wavering. The main way for individuals and organizations to work is through diplomatic channels. It is necessary to expose the practice and to embarrass countries that are at fault by expelling them from organizations such as the World Psychiatric Association. This can only be ensured by properly organized open investigation of psychiatric practice and interviews with the alleged victims”
Political abuse of psychiatry in the profession of medicine needs to be treated in the same way.
An evidence based Cochrane type assessment of their “research” and an Institute of Medicine Conflict of Interest review are long overdue.
In evaluating a physician for “impairment” or being “disruptive” the Physician Health Programs (PHPs) under the Federation of State Physician Health Programs (FSPHP) are not gathering data to form a hypothesis. They are making data fit a hypothesis that arrived at the out-of-state “PHP-approved” assessment center well before the alleged miscreant doctor.
With guilt assumed from the start, no due process, no appeal, and no way out physicians are being bullied, demoralized, and dehumanized to the point of hopelessness, helplessness and despair.
This needs to end now.
Medicine is predicated on competence, good-faith, and integrity.
Medical ethics necessitates beneficence, respect, and autonomy.
The scaffold erected here is designed for coercion and control.
Exposure, transparency, and accountability are urgent.
The emperor has no clothes.
Sunshine is the best disinfectant.
https://artbylisabelle.wordpress.com/2015/03/01/three-shells-and-a-pea-asam-fsphp-and-lmd/

Share this:

Question Authority: The Need for Anti-Authoritarians in the Medical Profession
 To evaluate the legitimacy of an authority it is necessary to:
To evaluate the legitimacy of an authority it is necessary to:

If one looks behind the curtain there is not much there. 
Historical, political, economic and social analysis can all show how the construct that exists today came to be. This can be factually ascertained by simple reasoning and examination of the documentary evidence.
Any one of these analyses would reveal that the “PHP-blueprint” is a false-construct built on circumnavigation and obfuscation.
An evidence-based scrutiny of the literature would reveal it to be invalid and of little probative value. A public policy analysis would reveal the logical fallacies involved in trumpeting their positions including exaggerated rhetoric and fear monitoring strategies designed to inspire moral panics and exploit fears to further an underlying political agenda
Any critical analysis would reveal cherry picking. proof by anecdote, deceptive propaganda, double talk, contradictory, illogical and incomprehensible jabber, unprovable and un-disprovable statements and a panoply of logical fallacy.
These groups misrepresent, censor and suppress. They nit pick and split hairs.  The concept of denial is not just used to force people into treatment and justify abuse during treatment but to suppress specific questions and deliberately avoid key facts.
The concept of denial is not just used to force people into treatment and justify abuse during treatment but to suppress specific questions and deliberately avoid key facts.
So why are we not questioning this “authority?” They have been left alone and basically thrown in the backyard left to proliferate like feral cats.

We need anti-authoritarians and we need them now.
I need allies before the door closes for good. And that door may be closing a lot sooner than you think!


Share this:

“Addiction Medicine” is not recognized by the American Board of Medical Specialties (ABMS)–It is a “self-designated-practice specialty” (SDPS) and indicates neither knowledge nor expertise.
 Educational and Professional Standards in Medical Specialties and Subspecialties
Educational and Professional Standards in Medical Specialties and Subspecialties
The increasingly rapid growth and complexity of medical knowledge in twentieth century American medicine resulted in the creation of specialties and subspecialties.
A related development was the creation of “boards” to “certify” physicians as knowledgeable and competent in the specialties and subspecialties in which they claimed to have expertise. The American Board of Ophthalmology, organized in 1917, was the first of these.
As the number of medical specialties proliferated an umbrella organization was formed to accomplish this task. The Advisory Board for Medical Specialties was created in 1933 and reorganized as the American Board of Medical Specialties (ABMS) in 1970. This non-profit organization oversees board certification of all physician specialists and sub-specialists in the United States.
The ABMS recognizes 24 medical specialties in which physicians can pursue additional training and education to pursue Board Certification.
In 1991 the American Board of Medical Genetics was approved as the 24th ABMS board and these 24 boards grant the 37 general certificates and 88 subspecialty certificates available to medical specialists today.
The ABMS Member Boards are responsible for developing and implementing the educational and professional standards for quality practice in a particular medical specialty or subspecialty and evaluate physician candidates for Board Certification. They set the bar of knowledge and competence for their given area of expertise.
All of the ABMS Member Boards are:
“committed to the principle of examining doctors based on six general competencies designed to encompass quality care: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice.”These areas have been collectively identified by the ABMS, the American College of Graduate Medical Education (ACGME) and the Institute of Medicine (IOM) in order to standardize graduate medical education in any specialty from medical school graduation through retirement.1
One of the 24 medical specialties ABMS recognizes in which physicians can pursue additional training and education and pursue Board Certification is Psychiatry.
Founded in 1934, The American Board of Psychiatry and Neurology (ABPN) is one of the 24 ABMS specialty boards. In 1959, the ABPN issued its first subspecialty certificate in Child and Adolescent Psychiatry and was the only ABNP subspecialty until 1991 when the first examination in Geriatric Psychiatry was administered.4 Addiction Psychiatry became a subspecialty of ABPN in 1993.
The ABPN governs the specialty of Psychiatry, of which Addiction Psychiatry is a subspecialty. Board Certification in Addiction Psychiatry requires a four-year psychiatric-residency program for training in the prevention, diagnosis and treatment of mood, anxiety, substance-abuse as well as other psychological and interpersonal problems followed by an additional year of training in one of the 40 accredited Addiction Psychiatry Fellowship programs. The Accreditation Council for Graduate Medical Education (ACGME) is the professional organization responsible for the accreditation residency education programs in the US for ABMS specialty and subspecialty areas of medicine. Addiction Psychiatry training programs are governed by the ACGME and graduates are eligible for ABPN Certification in Addiction Psychiatry.
When this rigorous education and training is complete a candidate is Board Eligible and can then take the subspecialty certification exam. The exam assesses competency in the dand consultation, pharmacotherapy, pharmacology of drugs, psychosocial treatment and behavioral basis of practice to be Board Certified in the subspecialty of Addiction Psychiatry by the ABPN.
Candidates must then be assessed in a number of areas including psychiatric evaluation and consultation, pharmacotherapy, pharmacology, toxicology, psychosocial treatment, behavioral basis of practice, and many other areas in which for the past half-decade they where taught and apprenticed.
The current structure of residency training is little changed from when it was conceived originally by William Stewart Halsted in the late 19th Century. Physicians acquire knowledge and skills necessary to safely and competently manage patients through apprenticeship. Training in a specialty area provides a comprehensive platform that allows medical school graduates to apply a body of knowledge to patient care and the treatment of disease. This forms the foundation of our Guild–undifferentiated and general but pluripotential.
The American Academy of Addiction Psychiatry (AAAP) is the only professional organization in the US focused on the subspecialty of Addiction Psychiatry. The AAAP Mission Statements are to: 2
-
PROMOTE HIGH QUALITY EVIDENCE-BASED SCREENING, ASSESSMENT AND TREATMENT FOR SUBSTANCE USE AND CO-OCCURRING MENTAL DISORDERS.
-
TRANSLATE AND DISSEMINATE EVIDENCE-BASED RESEARCH TO CLINICAL PRACTICE AND PUBLIC POLICY.
-
STRENGTHEN ADDICTION PSYCHIATRY SPECIALTY TRAINING AND FOSTER CAREERS IN ADDICTION PSYCHIATRY.
-
PROVIDE EVIDENCE-BASED ADDICTION EDUCATION TO HEALTH CARE TRAINEES AND HEALTH PROFESSIONALS TO ENHANCE PATIENT CARE AND PROMOTE RECOVERY.
-
EDUCATE THE PUBLIC AND INFLUENCE PUBLIC POLICY FOR THE SAFE AND HUMANE TREATMENT OF THOSE WITH SUBSTANCE USE DISORDERS.
-
PROMOTE PREVENTION AND ENHANCE ADDICTION TREATMENT AND RECOVERY ACROSS THE LIFE SPAN.
-
PROMOTE RESEARCH ON THE ETIOLOGY, PREVENTION, IDENTIFICATION AND TREATMENT OF SUBSTANCE USE AND RELATED DISORDERS.
Self-Designated Practice Specialty : An AMA Census Term Indicating What a Group of Doctors are Calling Themselves.
 The American Medical Association records a physician’s Self-Designated Practice Specialty (SDPS) in response to an annual credentialing survey. According to the AMA, SDPS are “historically related to the record-keeping needs of the American Medical Association and do not imply ‘recognition’ or ‘endorsement’ of any field of medical practice by the Association. SDPS refers to a self-designated specialty and this is not equivalent nor does it imply ABMS [American Board of Medical Specialties] Board Certification.
The American Medical Association records a physician’s Self-Designated Practice Specialty (SDPS) in response to an annual credentialing survey. According to the AMA, SDPS are “historically related to the record-keeping needs of the American Medical Association and do not imply ‘recognition’ or ‘endorsement’ of any field of medical practice by the Association. SDPS refers to a self-designated specialty and this is not equivalent nor does it imply ABMS [American Board of Medical Specialties] Board Certification.
“The fact that a physician chooses to designate a given specialty/area of practice on our records does not necessarily mean that the physician has been trained or has special competence to practice the SDPS.”3
Physicians have been able to list addiction medicine as a self-designated area of practice using the specialty code “ADM” since 1990.
In contrast to these accepted board credentials, American Board of Addiction Medicine (ABAM) certification requires only a medical degree, a valid license to practice medicine, completion of a residency training in ANY specialty, and one year‘s full time involvement plus 50 additional hours of medical education in the field of alcoholism and other drug dependencies. The majority of American Society of Addiction Medicine (ASAM) physicians meet these requirements by “working in a chemical dependency treatment facility, taking continuing medical education courses in addiction, or participating in research.”6
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments,, physicians, purchasers, and consumers of health care products, and the general public.’5 They have succeeded in doing this as many consider them to be the experts in addiction medicine including regulatory agencies.
addiction medicine as a specialty recognized by professional organizations, governments,, physicians, purchasers, and consumers of health care products, and the general public.’5 They have succeeded in doing this as many consider them to be the experts in addiction medicine including regulatory agencies.
The goal of the American Board of Addiction Medicine (ABAM) Foundation is to “gain recognition of Addiction Medicine as a medical specialty by the American Board of Medical Specialties (ABMS).”
But Addiction Medicine is currently not recognized by the ABMS. It is still a a Self-Designated Practice Specialty and the ABAM is a Self-Designated Board. So too is the American Academy of Ringside Medicine and Surgery, the American Academy of Bloodless Medicine and Surgery and the Council of Non-Board Certified Physicians. But these Self-Designated Boards do not have the multi-billion dollar drug and alcohol testing and treatment industry supporting them. Addiction Medicine has deep pockets, and if the November 2014 issue of the Journal of the American Medical Association (JAMA) is a harbinger of what’s to come, this self-designated practice specialty currently being certified by a self-designated Board and bereft of anything resembling the the educational and professional standards for quality practice in a particular medical specialty or subspecialty may soon robber baron its way into acceptance by the American Board of Medical Specialties.
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model. The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the drug and alcohol testing and 12-step treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.

- Stevens RA. In: Stevens R, Rosenberg C, Burns L, eds. History and Health Policy in the United States: Putting the Past Back in: Rutgers University Press; 2006:49-83.
- American Association of Addiction Psychiatry Website http://www.aaap.org/about-aaap/mission-statement (accessed 4/2/2014).
- American Medical Association. List & Definitions of Self-Designated Practice Specialties. August 21, 2012 http://www.ama-assn.org/ama.
- Juul D, Scheiber SC, Kramer TA. Subspecialty certification by the American Board of Psychiatry and Neurology. Academic psychiatry : the journal of the American Association of Directors of Psychiatric Residency Training and the Association for Academic Psychiatry. Spring 2004;28(1):12-17.
- http://www.asam.org/about-us/mission-and-goals.
- Tontchev GV, Housel TR, Callahan JF, Kunz KB, Miller MM, Blondell RD. Specialized training on addictions for physicians in the United States. Substance abuse : official publication of the Association for Medical Education and Research in Substance Abuse. Apr 2011;32(2):84-92.

“mail order” expertise; Diploma Mill
Share this:

American Medical Association (AMA) Seeks to Test Older Physicians: The Aging Physician–Goodbye Dr. Welby!

The AMA is seeking to test older physicians. This is no doubt due to the influence and lobbying of the “impaired physicians movement” and the “addiction medicine” specialists who brought us the “impaired” and “disruptive” physician constructs. As do all groups of this ilk, they want to expand. It is predictable and that is what we are seeing here.
Originally posted on Disrupted Physician:
The Aging Physician—Goodbye Dr. Welby!

As a specialist in geriatric medicine I have experience in taking care of a number of doctors who were referred to me for suspected memory problems. Still operating and teaching residents in his 70s, my first was a well-respected surgeon, a pioneer or Maverick who had made advances in his particular subspecialty. Known for his detailed knowledge of the history of medicine and sharp clinical acumen, he had not seemed himself for a while. His colleagues noted he appeared slower, fatigued and forgetful at times (not remembering his keys, having trouble finding the right word). An internist friend and co-worker who knew him for 50 years curb-sided me and asked if I would see him. He did not have a primary care physician or even seen a doctor professionally for decades (a common phenomenon in this age cohort of doctors).
I met him the next week and he readily admitted to having difficulty concentrating and having trouble with his short term memory. On taking his history he told me of his life and career which started as an intern in Boston in 1942 and he was on duty the night 492 people were killed in the Cocoanut Grove fire with many of the victims transported to his hospital. “I can see every detail as if it were yesterday–beautiful young women wearing fashionable dresses and gowns and young men in formal evening wear who looked as if they were sleeping but were dead.”
“Gastric reflux ” was the only medical problem he reported, adding it was well controlled for the better part of a decade with anti-reflux medications from the office sample closet. I tested his memory with several cognitive scales which showed some mild deficits in short-term memory and sent him to a neuropsychologist for more comprehensive testing. His physical examination, including a comprehensive neurological exam was normal. I ordered the usual lab work up for dementia to look for possible metabolic causes and his B12 level returned markedly low–a result of his long-term use of proton pump inhibitors. He was given an intramuscular injection and started on high doses of oral B12. As one of the “reversible’ causes of dementia he was back to his usual sprightly self several months later.
Another, a 70 old psychiatrist still teaching medical students and residents had asked a third-year psychiatric resident out on a date on two separate occasions. She reported him to administration on the second request. When I asked him about the incident he replied he didn’t see what was wrong with what he did and it was being blown out of proportion. “She’s in her 20’s” I said to which he replied “Well I’m only 36.” Still giving lectures to first year medical students without error or pause from knowledge he learned long ago, he could not identify a pencil or a watch when I pointed to them and asked what there were. He knew neither the month, season or year. After an MRI and neuropsychological testing he was given a diagnosis of probable Alzheimers disease. He had no spouse or children and his work was his life. After that he became profoundly depressed and six months later was dead.
Another elderly doctor, an internist, had a fairly sudden sudden onset of memory problems and symptoms of delirium. It turned out he was having trouble sleeping and his cardiologist prescribed him Dalmane, a benzodiazepine similar to Valium (medications that have a whole host of adverse effects in older patients including memory problems and falls). But valium has a half-life of hours whereas Dalmane has a half life of days. The medication was stopped and he was back to normal after a few days.
Aging is associated with an increased decline in many areas including cognition, motor-skills, muscle strength, and vision that can individually or cumulatively create risk to the person or others in a variety of situations (driving, living situation, occupation).
With advancing age comes advancing risk and the recognition and vigilance of others is often necessary for intervention. If the risk is recognized the problem can be addressed by the appropriate healthcare providers and specialists.
Doctors are not immune from cognitive impairment or dementia and the perspicacity of others is necessary should this occur.
Recognition and awareness are important. So too is an assessment by a qualified physician Board Certified in Neurology, Geriatrics or Geriatric Psychiatry who has education and experience in the diagnosis and treatment of memory disorders.
Recognition, Insight and Education Essential
In 2009 Dr. Ralph Blasier, M.D, J.D., published an article in the Journal Clinical Orthopaedics and Related Research entitled “The Problem of the Aging Surgeon: When Surgeon Age Becomes a Surgical Risk Factor” discussing the ability of older physicians to practice medicine safely and effectively.
His primary message is that a decline in physical and cognitive abilities is associated with the aging process and that these issues are especially pertinent to the field of medicine.
An area little researched, Blasier gives anecdotal examples such as a surgeon in his late 80s who had to regularly depend on younger colleagues to finish his operations. He concludes that these anecdotal examples suggest many surgeons lack insight into the degradation of their own skills and suggests recognition, insight, and education can help facilitate retirement of the aging surgeon before a decline in competency and skill creates a problem.
The awareness, education and insight of others is necessary to identify age associated illness in doctors who can then be referred to the proper specialists for evaluation. And although no evidence base exists, anecdotal reports such as these caused some groups to see an opportunity to increase the grand scale of the hunt.
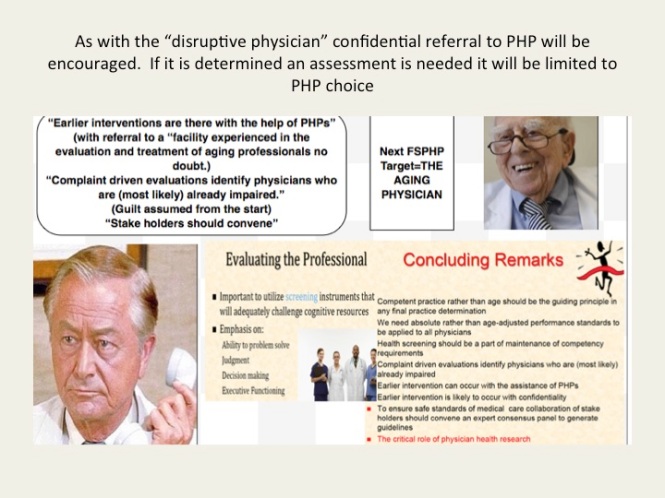
Aging Physicians Next Target of Physician Health Programs
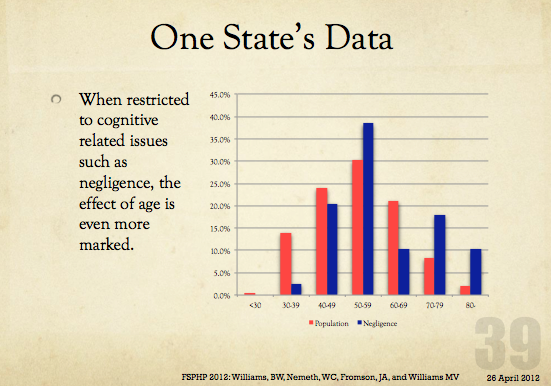
As with the “impaired” and “disruptive” physician, the “physician health and wellness movement” organized as the Federation of State Physician Health Programs (FSPHP) is linking the “aging” physician with threats to patient safety and hospital liability. “Experts say doing nothing could result in lawsuits, higher liability insurance rates, ruined reputations for practices and all involved, and even possible losses of practices and the licenses of non-reporting physicians.”
And if you look at the articles and presentations aimed at the administrative, regulatory, and legal arenas of medicine it appears a new moral panic is percolating in the “physician wellness” cauldron.
Labelling a group dangerous and creating fear in those responsible for that group is an effective means to sway policy and opinion.
With absolutely no evidence base these groups have acted as “moral entrepreneurs ” and used this same methodology to successfully change policy and regulation in the medical profession and advance their goals. The methodology is to
1. Label a group and link that group to danger
2. Offer to assist in identifying and eliminating that danger
3. Corner the market and control all aspects including assessment, testing and monitoring by swaying those in authority to make it public policy and regulation. 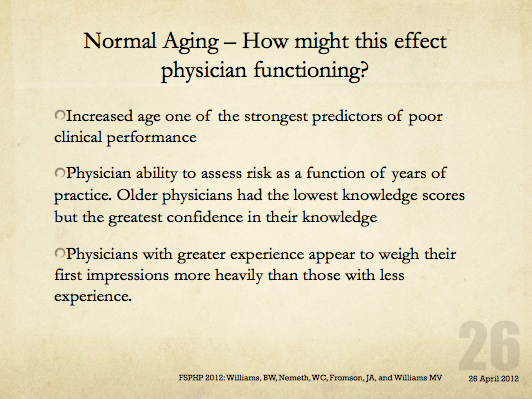
The methodology is not new–witches are real, witches are dangerous and witches need to be identified and exterminated at all costs. Convince the authorities to assist you in protecting the public from harm and advance the greater good
In this manner the FSPHP has convinced state medical boards to adopt and enforce policies that have incrementally and systematically increased their autonomy, scope and power since they first cultivated a relationship with the Federation of State Medical Boards (FSMB). This occurred in 1995 when they took an uninvited seat at the table of power by offering a non-disciplinary “safe harbor” as an alternative to discipline for doctors impaired by drugs or alcohol.
Since then they have increased their scope from the “impaired” to the “disruptive” to everything else. Arising from the “impaired physicians movement” as “addiction specialists” these doctors whose specialty of addiction is not even recognized by the American Board of Medical Specialties have now become the “experts” in all matters related to physician health. Jacks of all trades covering neurology, psychiatry, geriatrics, and occupational medicine.
A 2011 updated FSMB Policy on Physician Impairment states that Medical Boards should recognize the state Physician Heath Program (PHP) as their experts in all matters relating to licensed professionals with “potentially impairing illness,” and these include those potentially impairing maladies that increase as we age.
They are also using “everyone else does it why don’t we?” logical fallacy. According to a Washington Post article “other professions are subject to age-related regulations. For example, airline pilots must undergo regular health screenings staring at age 40 and must retire at age 65. FBI agents must retire at age 57.”
Proposing drug testing in doctors a JAMA article uses this same logic stating when sentinel events occur in the airline, nuclear power and railway industry the get drug tested. However all of these industries use FDA approved tests, certified labs, strict chain-of-custody and MRO review in their drug testing. One of the authors of the JAMA paper, Dr. Greg Skipper, introduced the non-FDA approved and unvalidated Laboratory Developed Tests currently used in PHPs such as EtG. He claims no conflicts-of-interest. Comparing drug testing to industries that use the highest quality of testing and safeguards to protect the donor from false-positives to the junk science used in PHPs is comparing apples to oranges. Which one do you think they’s be using in the random drug testing of doctors?
Furthermore, airline pilots, railway engineers and nuclear power plant employees have a choice of assessment and treatment centers should they get a positive test. Doctors do not. They are mandated to “PHP-approved” facilities. This is enforced by state medical boards as they adhere to an ASAM Public Policy Statement recommending only “PHP approved” treatment centers be used for assessment and treatment and a recent audit found the PHP in North Carolina could not provide any measurable indices or qualitative indicators of how an assessment center is stamped “approved.” The best they could come up with is “reputation” and other ‘informal sources. What the audit missed is all of the 19 out-of-state “PHP-approved” centers Medical Directors can be found on this list.
And what will happen with the “aging physician” is the same. Doctors will be forced into “assessments” at “PHP-approved” facilities where they will be misdiagnosed, over-diagnosed and forced into monitoring contracts under threat of loss of licensure. Goodbye Dr. Welby!



Share this:

Making the Data fit the Hypothesis is not Science: The American Society of Addiction Medicine (ASAM), “Weasel Phrases,” “Framing” and “Data-Dredging.”
This is an example of language framing. Language framing uses words and phrases to direct attention to a point of view to advance a vested interest.
In this case the use of the phrase “honest and denial free” in the context of physician reporting imparts associative meaning to the reader.
As denial is a recurring motif and cardinal attribute of physician addiction according to the paradigm, the connotation is that the reports by physicians may have been influenced by dishonesty and denial while face-to-face interviews done by “trained” interviewers were not.
“Framing” is another propaganda technique designed to tell the audience how to interpret the information given through context. The message here is that the somewhat less lifetime prevalence of substance abuse and addiction in physicians found by anonymous mail survey may be underreported as a result of both methodology and denial.

AMSA is now known as the ASAM
But in actual fact there is a large body of research regarding “social desirability bias” that shows the converse to be true.

 Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Principles of Addiction Medicine devotes a chapter to Physician Health Programs. Written by Paul Earley, M.D., FASAM,1 Earley states that the lifetime prevalence of substance abuse or addiction in physicians found by Hughes2 is “somewhat less than the percentage in the general population reported by Kessler” of 14.6%.3
Although he specifies the numerical percentage “in physicians at 7.9%,”3 he avoids the use of numbers (14.6%) in the general population. He instead uses the qualifier “somewhat less.” Why is this?
My guess is because it understates the statistical fact that the prevalence found by Kessler in the general population was almost twice that found by Hughes in physicians.
You see, “Somewhat less” is a “detensifier.” It creates an impression of a small disparity between doctors and the general population.
In propaganda this is what is known as a “weasel phrase.” Weasel phrases are used to obfuscate the…
View original post 645 more words
Share this:

How False Constructs Come to Be Regarded As Irrefutable Truth: The Malleus Maleficarum, Demonologists and Witch-Prickers–Let’s See if She Floats!
From the mid 1980s until present day a confederacy of “authorities” calling themselves “addiction medicine” specialists assisted in identifying disruptive physicians. Shaping clinical and legal orthodoxy they set the standards that cooperating regulatory authorities could follow in criminalizing, persecuting and punishing heretics.imgres
Behavioral manifestations included not answering pages on time, untimely or illegible chart notes, being late for meetings and questioning hospital authority. Disruptive physicians were blamed for everything—patient morbidity and mortality, increasing malpractice costs and decreased hospital revenue.
Using the nebulous “disruptive physician” label, anyone with a grudge or suspicious could accuse anyone of misbehavior, malice and mayhem.
Propaganda, threats, misinformation, guild assumed from the start, PHP oversight of disruptive physician persecution was standard.


“The belief that there are such things as witches is so essential a part of the faith that obstinately to maintain the opposite opinion manifestly savors of heresy.”
So begins Malleus Maleficarum , a witch hunters manual published in 1486 that launched a new paradigm for all those concerned with the identification and extirpation of witches. Used as a judicial case-book the Malleus set forth definitions of witchcraft, rules of evidence, and the canonical procedures by which suspected witches were tortured and put to death. Written by Inquisitors for Inquisitor, the Malleus construct came to be regarded as irrefutable truth and contributed to the identification and execution of as many as 60,000 “witches”, predominantly women. The 29th and last edition was published in 1669.

Although there was a general belief in witches at the time theas published they were not regarded as evil or life threatening. Society did not…
View original post 682 more words
Share this:

The Brain Disease Model of Addiction: is it Supported by the Evidence and has it Delivered on its Promises?

The brain disease model of addiction: is it supported by the evidence and has it delivered on its promises?
Published Online: 11 December 2014
Sign up for Lancet Psychiatry to read the full article. An overview is below.
We need a similar critique of the American Society of Addiction Medicine (ASAM) and its affiliates on this side of the Atlantic as “addiction medicine” is slated to be approved by the American Board of Medical Specialties in 2016 even though the discipline falls far short of the educational and professional standards for quality practice developed and implemented by all other ABMS member boards. According to the ABMS these 24 boards are:
“committed to the principle of examining doctors based on six general competencies designed to encompass quality care: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice.”These areas have been collectively identified by the ABMS, the American College of Graduate Medical Education (ACGME) and the Institute of Medicine (IOM) in order to standardize graduate medical education.
Any critique of the ASAM would find a number of issues antithetical to the six general competencies which stress “learning and improvement.” In contrast the ASAM rests on the conviction that their views are absolutely certain and patently rejects open-minded inquiry. An academic analysis of addiction medicine from the vantage point of the ASAM would reveal false assumptions, bias, dogmatism, and data-dredging. It would also reveal that those claiming expertise are in fact illegitimate and irrational authority who believe in an ends-justifies-the-means approach to push forth the chronic relapsing brain disease with lifelong abstinence an d imposed 12-step recovery. These are false experts who rationalize unethical, unprofessional and even criminal behavior as zeal for the faith if it aligns with the brain disease model of addiction (BDMA) Their viewpoints are fixed and final.
They have not been held to truly objective judging, analysis, evaluation or outside critique. The purpose of critique is the same as the purpose of critical thinking: to appreciate strengths as well as weaknesses, virtues as well as failings. Critical thinkers critique in order to redesign, remodel, and make better. This direly needs to be done. The evidence-base for both the BDMA and the drug and alcohol testing, assessment and treatment is poor. They are claiming physician health programs are the crown jewel of addiction treatment– a replicable model to be replicated in other populations. It is all hyperbole and propaganda. In reality they are using medical assessment and treatment as tools to repress and punish doctors. Those running the state physician health programs are typically morally disengaged bullies with Machiavellian egocentricity. And all the congratulatory backslapping is based on a singe poorly designed opinion piece.
Science and medicine need to be predicated on competence, thoughtfulness, good faith, civility, honesty, and integrity. This is universally applicable. What they are doing betrays the trust of society and breaches the most basic ethical obligations of not only doctors but human beings.
But no one seems to be challenging them. Why is no one questioning this self-appointed authority. If people do not start talking, writing, discussing and debating the current paradigm then what Robert Dupont describes in the ASAM White Paper on Drug Testing will be ushered in. As with doctors you won’t know it until it hits you. If the ASAM becomes an ABMS medical specialty then it will be too late. They will impose their authority on you as a patient and their won’t be a damn thing you will be able to do about it.
Once illegitimate and irrational authority are sanctified by the American Board of Medical Specialties there will be nothing left to do except watch the profession of medicine go up in flames.
Right now it’s just doctors and pilots. What you need to see is that you are next. I base that prediction on past public-policy, regulatory, administrative and medical practice tinkering as well as the documented paper trail of “research” and opinion. And even though all of this can be explained using documentary evidence, fact and critical analysis no one seems alarmed.
If you map it out you will see the trajectory is aimed at the transportation industry, students with federal loans, high school athletes, schools, gun owners, and eventually schools.
If you have something to lose that is affiliated with a state or federal agency they will hold it hostage if you get a positive hair, nail, sweat blood, or urine test at your doctors visit. The positive test is the golden ticket for them and a ticket to an assessment facility in Kansas, Arkansas, Mississippi and some other places for you on your dime. And these are one-way tickets. No return to normality available. One way ticket. No return flight.
See full article through the following link:
http://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(14)00126-6/fulltext
Proponents of the brain disease model of addiction (BDMA) have been very influential in setting the funding priorities of NIDA, and by extension the bulk of publicly supported research on addiction. In 1998, Leshner testified that NIDA supports more than 85% of the world’s research on drug abuse and addiction.3 The American Society of Addiction Medicine has defined addiction as a “primary, chronic disease of brain reward, motivation, memory, and related circuitry”.4 In July, 2014, newly appointed Acting Director of US National Drug Control Policy, Michael Botticelli, launched a reformist strategy nationally, claiming decades of research have demonstrated that addiction is a brain disorder—one that can be prevented and treated.5 The BDMA has also been widely discussed in leading scientific research journals3, 6 and most recently in a positive editorial in Nature.7
In the USA, proponents of the BDMA have argued that it will help to deliver more effective medical treatments for addiction with the cost covered by health insurance, making treatment more accessible for people with addictions.1, 2, 6 An increased acceptance of the BDMA is also predicted to reduce the stigma associated with drug addiction by replacing the commonly held notion that people with drug addiction are weak or bad with a more scientific viewpoint that depicts them as having a brain disease that needs medical treatment.
In this Personal View, we critically assess the scientific evidence for the BDMA reported in leading general scientific journals and the extent of the social benefits that advocates of the BDMA claim it has produced, or is likely to produce, with its widespread acceptance among clinicians, policy makers, and the public. The BDMA is not co-extensive with neuroscience-based explanations of addiction. This review is not intended as a critique of all neuroscience research on addiction. We focus instead on the popular simplification of work in this specialty that has had a major influence on popular discourse on addiction in scientific journals and mainstream media.
 Conclusions
Conclusions

Considerable scientific value exists in the research into the neurobiology and genetics of addiction, but this research does not justify the simplified BDMA that dominates discourse about addiction in the USA and, increasingly, elsewhere. Editors of Nature were mistaken in their assumption that the BDMA represents the consensus view in the addictions specialty,7 as shown by a letter signed by 94 addiction researchers and clinicians (including one of the authors of this Personal View).74Understanding of addiction, and the policies adopted to treat and prevent problem drug use, should give biology its due, but no more than it is due. Chronic drug use can affect brain systems in ways that might make cessation more difficult for some people. Economic, epidemiological, and social scientific evidence shows that the neurobiology of addiction should not be the over-riding factor when formulating policies toward drug use and addiction.
The BDMA has not helped to deliver the effective treatments for addiction that were originally promised by Leshner and its effect on public health policies toward drug addiction has been modest. Arguably, the advocacy of the BDMA led to overinvestment by US research agencies in biological interventions to cure addiction that will have little effect on drug addiction as a public health issue. Increased access to more effective treatment for addiction is a worthy aim that we support but this aim should not be pursued at the expense of simple, cost effective, and efficient population-based policies to discourage the whole population from smoking tobacco and drinking heavily. Nor should the pursuit of high technology cures distract from the task of increasing access to available psychosocial and drug treatments for addiction, which most people with addictive disorder are still unable to access.
Our rejection of the BDMA is not intended as a defence of the moral model of addiction.65 We share many of the aspirations of those who advocate the BDMA, especially the delivery of more effective treatment and less punitive responses to people with addiction issues. Addiction is a complex biological, psychological, and social disorder that needs to be addressed by various clinical and public health approaches.65 Research into the neuroscience of addiction has provided insights into the neurobiology of decision-making, motivation, and behavioural control in addiction. Chronic use of addictive drugs can impair cognitive and motivational processes and might partly explain why some people are more susceptible than others to developing an addiction. The challenge for all addiction researchers—including neurobiologists—is to integrate emerging insights from neuroscience research with those from economics, epidemiology, sociology, psychology, and political science to decrease the harms caused by drug misuse and all forms of addiction.46

References
- Leshner, A. Addiction is a brain disease, and it matters. Science. 1997; 278: 45–47
- Dackis, C and O’Brien, C. Neurobiology of addiction: treatment and public policy ramifications.Nat Neurosci. 2005; 8: 1431–1436
- US Government Printing Office. Senate Hearing 105-573. Drug addiction and recovery.http://www.gpo.gov/fdsys/pkg/CHRG-105shrg49670/html/CHRG-105shrg49670.html. ((accessed Sept 26, 2014).)
- American Society of Addiction Medicine. Public policy statement: definition of addiction. Chevy Chase, MD. http://www.webcitation.org/62jXWo8dq; 2011. ((accessed July 15, 2014).)
- Botticelli, M. National blueprint for drug policy reform released today in Roanoke, VA. Office of National Drug Control Policy media release July 9, 2014.http://www.whitehouse.gov/blog/2014/07/09/national-blueprint-drug-policy-reform-released-today-roanoke-va. ((accessed July 15, 2014).)
- Volkow, N and Li, T. Drug addiction: the neurobiology of behaviour gone awry. Nat Rev Neurosci.2004; 5: 963–970
- Animal farm. Nature. 2014; 506: 5
- Ahmed, S. The science of making drug-addicted animals. Neuroscience. 2012; 211: 107–125
- Koob, G. The neurobiology of addiction: a neuroadaptational view relevant for diagnosis.Addiction. 2006; 101: 23–30
- Feltenstein, M and See, R. The neurocircuitry of addiction: an overview. Br J Pharmacol. 2008;154: 261–274
- Hyman, S, Malenka, R, and Nestler, E. Neural mechanisms of addiction: the role of reward-related learning and memory. Annu Rev Neurosci. 2006; 29: 565–598
- Koob, G and Le Moal, M. Neurobiology of addiction. Academic Press, New York; 2006
- Panlilio, L and Goldberg, S. Self-administration of drugs in animals and humans as a model and an investigative tool. Addiction. 2007; 102: 1863–1870
- Vanderschuren, L and Ahmed, S. Animal studies of addictive behavior. Cold Spring Harb Perspect Med. 2013; 3: a011932
- Volkow, N, Wang, G, Fowler, J, Tomasi, D, and Baler, R. Neuroimaging of addiction. in: P Seeman, B Madras (Eds.) Imaging of the human brain in health and disease. Elsevier, San Diego; 2014: 1–26
- Volkow, N, Fowler, J, Wang, G, Teland, F, and Baler, R. Imaging dopamine’s role in drug abuse and addiction. in: L Iversen, S Iversen, S Dunnett, A Bjorklund (Eds.) Dopamine handbook. Oxford University Press, Oxford; 2010: 407–417
- Volkow, N and Baler, R. Addiction science: uncovering neurobiological complexity.Neuropharmacology. 2014; 76: 235–249
- Volkow, N, Fowler, J, Wang, G, Baler, R, and Telang, F. Imaging dopamine’s role in drug abuse and addiction. Neuropharmacology. 2009; 56: 3–8
- Reske, M and Paulus, M. A neuroscientific approach to addiction: ethical issues. in: J Illes, B Sahakian (Eds.) Oxford handbook of neuroethics. Oxford University Press, Oxford; 2011: 177–202
- Kendler, K, Chen, X, Dick, D et al. Recent advances in the genetic epidemiology and molecular genetics of substance use disorders. Nat Neurosci. 2012; 15: 181–189
- Ball, D. Addiction science and its genetics. Addiction. 2008; 103: 360–367
- Satel, S and Lilienfeld, S. Brainwashed: the seductive appeal of mindless neuroscience. Perseus Books Group, New York; 2013
- Heyman, G. Addiction: a disorder of choice. Harvard University Press, Cambridge, MA; 2009
- Kincaid, H and Sullivan, J. Medical models of addiction. in: D Ross, H Kincaid, D Spurrett, P Collins (Eds.) What is addiction?MIT, Cambridge, MA; 2010: 353
- Robins, L, Helzer, J, Hesselbrock, M, and Wish, E. Vietnam veterans three years after Vietnam: how our study changed our view of heroin. Am J Addict. 2010; 19: 203–211
- Kleiman, M. When brute force fails: how to have less crime and less punishment. Princeton University Press, Princeton; 2009
- Bachman, J, Wadsworth, K, O’Malley, P, Johnston, L, and Schulenberg, J. Smoking, drinking, and drug use in young adulthood: the impacts of new freedoms and new responsibilities. Lawrence Erlbaum, Mahwah, NJ; 1997
- Ahmed, S, Lenoir, M, and Guillem, K. Neurobiology of addiction versus drug use driven by lack of choice. Curr Opin Neurobiol. 2013; 23: 581–587
- Alexander, B, Coambs, R, and Hadaway, P. The effect of housing and gender on morphine self-administration in rats. Psychopharmacology (Berl). 1978; 58: 175–179
- Hall, WD, Gartner, CE, and Carter, A. The genetics of nicotine addiction liability: ethical and social policy implications. Addiction. 2008; 103: 350–359
- Gartner, CE, Barendregt, J, and Hall, WD. Multiple genetic tests for susceptibility to smoking do not outperform simple family history. Addiction. 2009; 104: 118–126
- Roberts, N, Vogelstein, J, Parmigiani, G, Kinzler, K, Vogelstein, B, and Velculescu, V. The predictive capacity of personal genome sequencing. Sci Transl Med. 2012; 4: 133ra58
- Button, K, Ioannidis, J, Mokrysz, C et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013; 14: 365–376
- Ioannidis, J. Excess significance bias in the literature on brain volume abnormalities. Arch Gen Psychiatry. 2011; 68: 773–780
- Ioannidis, J, Munafò, M, Fusar-Poli, P, Nosek, B, and David, S. Publication and other reporting biases in cognitive sciences: detection, prevalence, and prevention. Trends Cogn Sci. 2014; 18: 235–241
- Hall, WD, Gartner, CE, Mathews, R, and Munafò, M. Technical, ethical and social issues in the bioprediction of addiction liability and treatment response. in: A Carter, W Hall, J Illes (Eds.)Addiction neuroethics: The ethics of addiction research and treatment. Elsevier, New York; 2012:116–138
- Lingford-Hughes, A, Welch, S, Peters, L, and Nutt, D. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP. J Psychopharmacol. 2012; 26: 899–952
- Ersche, K, Williams, G, Robbins, T, and Bullmore, E. Meta-analysis of structural brain abnormalities associated with stimulant drug dependence and neuroimaging of addiction vulnerability and resilience. Curr Opin Neurobiol. 2013; 23: 615–624
- Hyman, S. The neurobiology of addiction: implications for the voluntary control of behaviour. in:J Illes, B Sahakian (Eds.) Oxford handbook of neuroethics. Oxford University Press, Oxford; 2011:203–217
- Goldstein, R and Volkow, N. Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat Rev Neurosci. 2011; 12: 652–669
- Volkow, N, Wang, G, Fowler, J, and Tomasi, D. Addiction circuitry in the human brain. Annu Rev Pharmacol Toxicol. 2012; 52: 321–326
- National Institute on Drug Abuse. Drugs, brains and behavior: the science of addiction. Washington, DC. http://www.drugabuse.gov/publications/science-addiction; 2007. ((accessed July 15, 2014).)
- Nutt, D and Lingford-Hughes, A. Addiction: the clinical interface. Br J Pharmacol. 2008; 154: 397–405
- Volkow, N and Li, T. Drugs and alcohol: treating and preventing abuse, addiction and their medical consequences. Pharmacol Ther. 2005; 108: 3–17
- Lingford-Hughes, A, Watson, B, Kalk, N, and Reid, A. Neuropharmacology of addiction and how it informs treatment. Br Med Bull. 2010; 96: 93–110
- Kalant, H. What neurobiology cannot tell us about addiction. Addiction. 2010; 105: 780–789
- Koob, G, Lloyd, G, and Mason, B. Development of pharmacotherapies for drug addiction: a Rosetta Stone approach. Nat Rev Drug Discov. 2009; 8: 500–515
- Cahill, K, Stead, L, and Lancaster, T. Nicotine receptor partial agonists for smoking cessation.Cochrane Database Syst Rev. 2011; 2 (CD006103.)
- Rösner, S, Hackl-Herrwerth, A, Leucht, S, Lehert, P, Vecchi, S, and Soyka, M. Acamprosate for alcohol dependence. Cochrane Database Syst Rev. 2010; 9 (CD004332.)
- Minozzi, S, Amato, L, Vecchi, S, Davoli, M, Kirchmayer, U, and Verster, A. Oral naltrexone maintenance treatment for opioid dependence. Cochrane Database Syst Rev. 2011; 4 (CD001333.)
- Kosten, T, Domingo, C, Shorter, D et al. Vaccine for cocaine dependence: a randomized double-blind placebo-controlled efficacy trial. Drug Alcohol Depend. 2014; 140: 42–47
- View in Article
- | Summary
- | Full Text
- | Full Text PDF
- | PubMed
- | Scopus (3)
- Hartmann-Boyce, J, Cahill, K, Hatsukami, D, and Cornuz, J. Nicotine vaccines for smoking cessation. Cochrane Database Syst Rev. 2012; 8 (CD007072.)
- Hall, WD and Gartner, CE. Ethical and policy issues in using vaccines to treat and prevent cocaine and nicotine dependence. Curr Opin Psychiatry. 2011; 24: 191–196
- Paul, S, Mytelka, D, Dunwiddie, C et al. How to improve R&D productivity: the pharmaceutical industry’s grand challenge. Nat Rev Drug Discov. 2010; 9: 203–214
- Djulbegovic, B, Hozo, I, and Ioannidis, J. Improving the drug development process: more not less randomized trials. JAMA. 2014; 311: 355–356
- Prinz, F, Schlange, T, and Asadullah, K. Believe it or not: how much can we rely on published data on potential drug targets?. Nat Rev Drug Discov. 2011; 10: 712
- Tsilidis, K, Panagiotou, O, Sena, E et al. Evaluation of excess significance bias in animal studies of neurological diseases. PLoS Biol. 2013; 11: e1001609
- Hall, WD. Stereotactic neurosurgical treatment of addiction: minimising the chances of another ‘great and desperate cure’. Addiction. 2006; 101: 1–3
- Luigjes, J, van den Brink, W, Feenstra, M et al. Deep brain stimulation in addiction: a review of potential brain targets. Mol Psychiatry. 2012; 17: 572–583
- Stephen, J, Halpern, C, Barrios, C et al. Deep brain stimulation compared with methadone maintenance for the treatment of heroin dependence: a threshold and cost-effectiveness analysis.Addiction. 2012; 107: 624–634
- Rouaud, T, Lardeux, S, Panayotis, N, Paleressompoulle, D, Cador, M, and Baunez, C. Reducing the desire for cocaine with subthalamic nucleus deep brain stimulation. Proc Natl Acad Sci USA.2010; 107: 1196–1200
- Carter, A and Hall, WD. Proposals to trial deep brain stimulation to treat addiction are premature. Addiction. 2011; 106: 235–237
- Baltuch, G and Stern, M. Deep brain stimulation for Parkinson’s disease. Informa Healthcare,New York; 2007
- Rose, G. The strategy of preventive medicine. Oxford University Press, Oxford; 1992
- Carter, A and Hall, WD. Addiction neuroethics: the promises and perils of neuroscience research on addiction. Cambridge University Press, London; 2012
- National Institute on Drug Abuse. Fiscal Year 2015 Budget information—congressional justification for National Institute on Drug Abuse. Rockville, MD. http://www.drugabuse.gov/about-nida/legislative-activities/budget-information/fiscal-year-2015-budget-information-congressional-justification-national-institute-drug-abuse; 2014. ((accessed July 15, 2014).)
- White, V, Hill, D, Siahpush, M, and Bobevski, I. How has the prevalence of cigarette smoking changed among Australian adults? Trends in smoking prevalence between 1980 and 2001. Tob Control. 2003; 12: ii67
- Pierce, J, Gilpin, E, Emery, S, White, M, Rosbrook, B, and Berry, C. Has the California tobacco control program reduced smoking?. JAMA. 1998; 280: 893
- Hall, WD, Madden, P, and Lynskey, M. The genetics of tobacco use: methods, findings and policy implications. Tob Control. 2002; 11: 119–124
- Doran, C, Hall, WD, Shakeshaft, A, Vos, T, and Cobiac, L. Alcohol policy reform in Australia: what can we learn from the evidence. Med J Aust. 2010; 192: 468–470
- Miller, P, Carter, A, and De Groot, F. Investment and vested interests in neuroscience research of addiction: why research ethics requires more than informed consent. in: A Carter, W Hall, J Illes (Eds.) Addiction neuroethics: the ethics of addiction research and treatment. Elsevier, New York;2012: 278–301
- Courtwright, D. The NIDA brain-disease paradigm: history, resistance, and spinoffs. BioSocieties.2010; 5: 137–147
- Nutt, D, King, L, Saulsbury, W, and Blakemore, C. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet. 2007; 369: 1047–1053
- Heim, D. Addiction: not just brain malfunction. Nature. 2014; 507: 40

