Physician Health Programs (PHPs) now targeting medical students–More sheep for the slaughter
The attached article entitled “Medical school drug testing is a moral and scientific failure” opposes testing medical students for drugs and alcohol but things are going to get a whole lot worse.
In the past six-months I have been contacted by an increasing number of medical students searching for help after being trapped in quagmire of their state physician health program (PHP). Each of them had either been referred to a “PHP-approved” assessment center or had already had an evaluation recommending inpatient treatment.
Some of these students were subjected to non-FDA approved laboratory developed tests including hair testing for marijuana metabolites and the alcohol biomarker EtG. These typeof tests can detect substances that were used days, weeks and even months prior to testing.
Medical students and physicians are just as likely to have experimented with illicit substances in their lifetimes as their age and gender matched peers.1
Although medical students as a group drink slightly more alcohol than the general population, the pattern and prevalence of alcohol, dependence is consistent with their age mates in the general population.1 2
Like it or not recreational and experimental drug use is widespread in young adults and most of them “grow out of it” and the 21st Amendment repealed the Volstead Act in 1933. Alcohol is legal and those that can handle it have a right to a round of beers after a long day or imbibe a cocktail with a dinner date. But according to the prohibitionist profiteers and moral preeners any drug or alcohol use is a sign of “potentially impairing illness” that must be addressed and treated early to prevent an inexorable slide into a chronic relapsing brain disease and abstinence and lifelong adherence to the principles 12-step spirituality are the only way to do so.
An old joke asks “How does a doctor define an alcoholic?” Answer–“anybody who drinks more than he does.” How does a PHP define an alcoholic? Answer –anybody who walks through the front door.
In reality, a zero-tolerance paradigm utilizing this type of testing would be ruinous. With recreational and experimental drug use common in young adults a profession that refuses to accept anyone who tests positive for drugs will exclude large numbers of brilliant, talented individuals. Dismissing highly talented people in medicine for what might be a one-off recreational non problematic drug experience would retard its advance.
The use of these non-FDA approved tests of unknown validity should not be allowed to begin with but there needs to be a concerted direct attack on their use on medical students or the brain-drain on the profession will bring it back to the dark ages. The ASAM White Paper on Drug Testing proposes imposing this system with mandatory drug testing by the healthcare system from childhood to old age. College loans are proposed as “leverage” for college students in this “contingency management” paradigm so a lot of promising students could be weeded out before even applying to medical school. Forget GPA and MCATS as the primary criteria for medical school admission will be sobriety and clean urine screens..
Diagnosing disease without meeting the diagnostic criteria for that disease.
None of the students who contacted me seemed to fit the diagnostic criteria for the diagnosis given to them stories which were articulate, detailed and sincere. All cases involved either a naive mistake or isolated incident.
One student made the disastrous revelation to a PHP director who had just given a class lecture that she had smoked marijuana with her high school friends in her home state of Colorado. She was then called in by the PHP and referred for an evaluation at an out of state facility where she was diagnosed with “marijuana dependence” based on a positive low level THC metabolite on a hair follicle test. She was told she was in denial and inpatient treatment was recommended. Although she admitted to occasional weekend marijuana use there were absolutely no problems in any realm of her life. It is self-evident that impairment due to drugs or alcohol impacting someones capacity to work or function needs to be addressed but the penalty imposed on her for her private behavior was to end her career in medicine before it even started. The medical school administration mandated she either complete the treatment required by the PHP or she would not be able to enroll the following semester and not being able to come up with the up-front out-of-pocket cost for treatment she was not able to return to the medical school and has decided to pursue a different career.
Another student was anonymously reported to the PHP for smoking marijuana at a weekend party which resulted in a similar assessment and recommendation for inpatient treatment. After spending 3 months at a facility in Alabama he is now under monitoring contract with his PHP but returned to school.
Healthy student asks for help in his organizational skills–ends up with a psychiatric and substance abuse diagnosis
After reading an advertisement in the state medical society newsletter promoting work-life balance a second-year medical student contacted his state PHP to obtain advice on his problem with “procrastination.” Classes and working part time in the endocrinology lab left him with little time and he found himself slacking off on his exercise routine and burning the midnight oil before test nights. He told the PHP director about his history of depression after his father died immediately before his freshman year at college. That October he became overwhelmed with sadness and missed his dad and hometown. He sought help from the campus physician who prescribed prozac which was discontinued in a years time without return of any symptoms.
Realizing there were no classes in work-life balance but only a support group for “burnout” the student declined the PHP directors offer of an assessment of his “mental health.” Much to his surprise he was called in the following week by a medical school administrator and told that the PHP was requiring an assessment at one of two out of state “PHP-approved” assessment centers in Lawrence Kansas. He was at first confused at the nonsense he was hearing and then became indignant at the nonsensical and illogical request without rhyme or reason and the betrayal of trust and ethics. “Surely this must be a HIPPA violation.” He obtained an outside consultation from a psychiatrist and contacted the campus physician who confirmed his diagnosis was acute situational depression and bereavement but the PHP disregarded the information. He bartered for a local evaluation but this was refused. He arranged for the 96-hour assessment in Kansas. His mother paid the requisite out-of-pocket up-front $4,500.00 to the facility and she told him not to worry as his life would get back to normal after they confirmed he had no psychological problems. “Dysthymia, Major depressive disorder, severe, in remission and alcohol use disorder” were given as diagnoses. “Alcohol use disorder” was based on a hair test for EtG which was the result of his drinking an occasional beer or two with friends after school and on the weekends. He was told he may be “self-medicating” and playing “Russian roulette” given his history of depression. Recommendations included inpatient treatment followed by a “structured aftercare program” of abstinence and monitoring by for alcohol and drugs of abuse. Forced to sign a contract with the PHP he was understandably upset at the serious and unfounded sequelae that was the result of asking for help.
Another fourth-year student got into a bit of a shoving match with his buddy at the bar on a Saturday night and was reported to his PHP anonymously. He is awaiting evaluation.
This brings up another potential problem–sham peer review. As PHPs accept anonymous referrals what is in place to prevent inappropriate referrals based on removing a competitor and improving your academic standing.
A legitimately prescribed stimulant for ADHD bought a third year student into a PHP contract. He was forced to discontinue the medication prescribed by a psychiatrist specializing in childhood ADHD by a family practitioner in “recovery” from abusing intravenous fentanyl who had been monitored by the PHP himself for ten years then became medical director after getting board certified as an addiction medicine specialist.
This student got 99th percentile across the Board on his MCATs and may one day cure cancer but now faces an uncertain future as he recently got a positive EtG on a urine test and they are currently “sorting this out.”
The most bizarre story was from a student who sought help for sleep troubles after reading about the PHP as a referral source. He subsequently saw a sleep-specialist and was diagnosed with an oversized uvula which was surgically corrected. His sleep troubles improved but his troubles with the PHP remained. A triathlete and excellent student the PHP determined he had a “thought disorder” and discussions of “schizophrenia” were entertained by the PHP and they recommended an out of state evaluation at one of the three gulags used by the FSPHP for “disruptive physician” and behavioral exams–Vanderbilt, Acumen and the Professional Renewal Center. All of these facilities come with a guaranteed diagnosis. Polygraphs and unvalidated neuropsychological instruments designed to detect “character defects” cast a pretty wide net.
Question FSPHP with direct questions to undermine a “culture of professionalism.
It is important that medical school administrators refuse to engage in blind deference to the authority of the state PHP. Authority must always be questioned and to not do so is irresponsible. Unquestioning allegiance to an authority does not comport with the history of the medical profession or science. Faith in institutions demands mass adherence to faith in that authority and direct challenges to the status quo are needed to undermine that faith. They have bamboozled the medical boards into implementing bad policy, approving bad science and making bad decisions. They have duped state legal authorities into deference to their expertise and integrity under the notion that questioning these attributes undermines a culture of professionalism. Fact of the matter is they have no expertise, no integrity and no professionalism.
PHPs have been contaminated with an outside influence and support an agenda that has nothing to do with protecting the public or helping medical students. They are an illegitimate authority that has become an irrational authority and their recommendations mandate direct answers and justification.
If the PHP has concerns about a student then the first step should be to obtain an independent second opinion. PHPs discourage second these second opinions and disregard all outside expert opinion no matter how well qualified and experienced that expert is. Anyone outside this brood of addiction addicts is scoffed at as biased or unenlightened to the simplistic belief system with which they have contaminated the medical profession. Look into the assessment centers to which they are mandating referral. Ask what qualitative factors and quantitative measurements were used to approve that facility and why no one in Massachusetts has the ability come to a competent diagnosis. The yarn that doctors and medical student have an ability to dissemble and appear normal while harboring a “potentially impairing condition” is one of the medical urban legends they started. Ask to see the evidence base. There is none and it defies common sense, logic and science.
An increasingly bright light is being shed towards the malfunctions and corrupt practices of this unaccountable confederacy of “authorities” and at some point soon their jig will inevitably be up. In the interim, if you are referred to a PHP it would be a good idea obtain independent lab tests and two second opinions. Although the PHP will disregard this documentation it would be wise to obtain it to prove both your normality and the discrepancy between your independent evaluation results and the cherry-picked pulled out of a hat multiple diagnoses confabulated and misrepresented by the PHP.
- Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
- Flaherty JA, Richman JA. Substance use and addiction among medical students, residents, and physicians. The Psychiatric clinics of North America. Mar 1993;16(1):189-197.

Medical school drug testing is a moral and scientific failure
ANONYMOUS | EDUCATION | MAY 11, 2014
Before the 1980s, drug testing was uncommon. It was widely viewed as an invasion of privacy and an infringement on fourth amendment rights. Today, a medical student is likely to be drug tested before entering medical school, before clinical rotations, and/or before residency. If preventing drug use among medical students is the goal of these tests, they have failed miserably. Urinalysis drug tests are ineffective. But more importantly, they are immoral.
Drug tests are ineffective for two reasons. First, they basically just test for marijuana. A 10 panel urinalysis technically tests for 10 different drugs, but marijuana is one of the only drugs that can be detected for more than 30 days. Cocaine can be detected for 4 days. Amphetamine, methamphetamine, ecstasy, heroin, and codeine all can be detected in urine for only 2 days. This means that a user of drugs far more dangerous than marijuana needs to abstain for just a couple of days. Psilocybin mushrooms, as well as several other mind-altering drugs, are not tested for at all.
For a marijuana user, a drug test might seem like a nightmare. But here we arrive at the second reason why drug tests are ineffective, they are easily beaten. A marijuana user may choose to drink a lot of water before his drug test to dilute his urine. Alternatively, he may choose to use a friend’s urine who he knows does not use marijuana. Either one of these options might work. But fortunately for such a marijuana user, there is another option that is essentially risk free, synthetic urine. There are several companies that make synthetic urine capable of beating drug tests. The word on the Internet is that Quick Fix is a safe bet. I personally know some people who would agree. At just $30 for a bottle, it looks like the drug test is no match for the free market.
Do not just take my word for it though. In 2003, the University of Michigan conducted a study on the effectiveness of drug testing students. From nearly 900 schools, the study found that drug testing, whether routine, random, or based on suspicion, had no measurable effect on drug use among students. Put simply, drug testing accomplishes nothing.
The most important concern I have about drug testing medical students is a moral one. Regardless of their effectiveness, or ineffectiveness, the endgame of drug testing is to prevent drug users from becoming doctors. Users, not addicts; and there is a big difference. A marijuana user might use on weekends or at night to relax, much like an alcohol user. A marijuana addict, although rare, is the type of person who might show up to important occasions intoxicated. The statistics on marijuana addiction vary. They usually show that less than 10% of users become addicts, but they always show that alcohol users have higher rates of addiction. A urinalysis detects alcohol for no more than 12 hours after use. This means that medical students who use alcohol are more likely to be addicted, and they face basically no risk of failing a drug test.
Should we be worried about medical students being drunk in clinical settings? Of course. And we should also be worried about medical students being high in clinical settings. Intoxication could be disastrous and it needs to be prevented. The good news is that this is done naturally. It is highly unlikely to find medical students who are addicts of marijuana, alcohol, or any mind-altering drug. I believe it is safe to say that the rigor of medical school itself prevents drug addicts from becoming doctors. There are, however, drug users who will make it into medical school or other rigorous scientific careers. Actually, many of them thrive. Richard Feynman, Kary Mullis, and Francis Crick used marijuana and LSD, Carl Sagan used marijuana, and Oliver Sacks used several illicit drugs. When drug tests are required for every medical student, the casual drug user, no matter how much potential he has, is bullied for no reason. The potentially dangerous drug addict has already been weeded out long ago.
Medical school is supposed to be based on science. The science shows that drug testing does not work. If it did work, then many great scientists would have been removed from their professions. These facts alone should be enough to settle the issue, but it is important to look at two more moral objections we should all have.
First, drug tests are not free. Before entering medical school, I paid about $30 for one. This does not sound like much. But charging students even one penny is unacceptable, for there is not even a fraction of a penny in benefit from these tests. The nearest drug testing facility for me was a 20 minute drive from my house. I could have driven anywhere for 20 minutes and just handed $30 to any random person. Surely, that $30 would bring more value to society than $30 wasted on a drug test. Imagine if a police officer searched a person’s car for drugs against his will, found none, and then charged this person $30. That is the reality of drug testing.
Second, drug tests are an invasion of privacy. Medical students should not be forced to prove their innocence. This creates a guilty until proven innocent environment. It immediately creates resentment among students, and rightfully so. Furthermore, what about people with paruresis? The International Paruresis Association estimates that 7% of people suffer from this condition, also known as shy bladder. Type “paruresis drug test” into a search engine and spend some time reading through the horror stories that are shared. These people suffer from a medical condition, and of all places, their medical school is completely inconsiderate.
Drug testing is a moral and scientific failure. Medical schools should be too embarrassed to take part in such nonsense.
The author is an anonymous medical student who blogs at unchainedmedical.
TAGGED AS: MEDICAL SCHOOL


 Source: Flagrant Corruption by Massachusetts PHP-Help me Hold them Accountable
Source: Flagrant Corruption by Massachusetts PHP-Help me Hold them Accountable





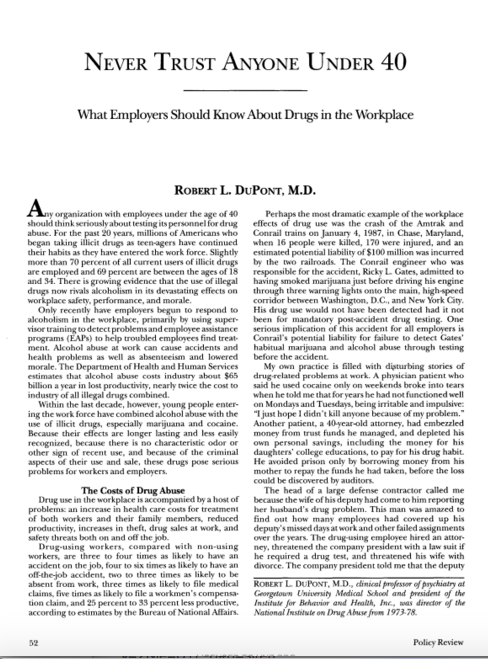
 “In the small world of drug testing, these four—Angarola, Bensinger, DuPont and Willette—are affectionately referred to as the Gang of Four. Dr. John Morgan explains, “They are the ones responsible for a good deal of drug testing’s success, and some of the fear that goes along with it. Remember these names. These men are among the most competent and knowledgeable about drug testing—scientifically and politically. They are well-informed: they have to be. Their livelihoods depend upon their credibility. Unfortunately their expertise represents the greatest threat to the civil liberties we seek to protect. Know your enemy.”
“In the small world of drug testing, these four—Angarola, Bensinger, DuPont and Willette—are affectionately referred to as the Gang of Four. Dr. John Morgan explains, “They are the ones responsible for a good deal of drug testing’s success, and some of the fear that goes along with it. Remember these names. These men are among the most competent and knowledgeable about drug testing—scientifically and politically. They are well-informed: they have to be. Their livelihoods depend upon their credibility. Unfortunately their expertise represents the greatest threat to the civil liberties we seek to protect. Know your enemy.”  On April 23, 2015
On April 23, 2015