
“Conformity is the jailer of freedom and the enemy of growth.” – John F. Kennedy.
Born – May 29, 1917
Brookline, Massachusetts,
Died- November 22, 1963
Dallas, Texas, aged 46


“Conformity is the jailer of freedom and the enemy of growth.” – John F. Kennedy.
Born – May 29, 1917
Brookline, Massachusetts,
Died- November 22, 1963
Dallas, Texas, aged 46


“The hardest thing to explain is the glaringly evident which everybody has decided not to see”
― Ayn Rand, The Fountainhead

The Birth of Junk-Science in Drug and Alcohol Testing
The attached article concerns the reliability of hair-strand tests routinely accepted in child welfare cases in Ontario as evidence of parental drug or alcohol abuse. A positive test can lead to loss of parental custody of children.
The risk for false-positive results appears to be higher in women because of the higher use of alcohol-based hair products and the limitations of these tests are addressed in the article.
Almost 98% of ingested alcohol is eliminated through the liver in an oxidation process that involves its conversion to acetaldehyde and acetic acid, but the remaining 2% is eliminated through the urine, sweat, or breath.1
Ethyl Glucuronide (EtG) was introduced in 1999 as a biomarker for alcohol consumption,2 and was subsequently suggested as a tool to monitor health professionals by Dr. Gregory Skipper, M.D., because of its high sensitivity to ethanol ingestion.3

This minor metabolite of alcohol was reported by Skipper, M.D. and Friedrich Wurst, M.D., in November 2002 at an international meeting of the American Medical Society, to provide proof of alcohol consumption as much as 5 days after drinking an alcoholic beverage, well after the alcohol itself had been eliminated from the body.
In his study Dr. Skipper arbitrarily chose a value of 100 as a cut-off for EtG. The rationale behind this value is not cited.
In 2003, because of these and other reportedly remarkable results (e.g., positive findings, confirmed by admissions by the tested individuals, after traditional urine tests had registered negative), Skipper pitched the test to National Medical Services, Inc. (NMS labs) and it was developed as a Laboratory Developed Test (LDT).
So began EtG testing began in the United States, and this paved the way for the hair tests described. The urine EtG test introduced by Skipper is the index case and prototype for an array of unproven forensic tests introduced to the market as LDTs.

The LDT Pathway was not designed for Forensic Drug and Alcohol Testing. It is an Unregulated Industry.
The LDT pathway was developed for laboratory tests that would not otherwise come to market due to the prohibitive costs of FDA approval (for example a test for a rare disease).
Bringing an LDT to market does not require testing in humans (in vivo). Nor does it require that it be shown the test is testing for what it is purportedly testing for (validity). It is essentially an honor system. It was not designed for “forensic” testing but for simple testing with low risk.
None of this testing is approved by the FDA. It is essentially an unregulated industry.
NMS became a leading proponent of EtG testing and, starting in 2003, began publishing claims promoting the absolute validity and reliability of the EtG in detecting alcohol. Akin to the vitamin and supplement industry those promoting and selling the tests could say anything they want—and they did.
NMS initially established a reporting limit or cutoff of 250ng/ml at or over which EtG test results would be reported as “positive” for drinking alcohol. This was later upped to 500ng/ml, then 1000 ng/ml.
NMS reported it as the “Gold Standard” claiming any value above 250 ng/ml indicated “ethanol consumption.”
It was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash4,5, hand sanitizer gel6, nonalcoholic beer7, and nonalcoholic wine.8
As the cutoff value got higher they added another minor metabolite of alcohol, EtS, as a “confirmatory” LDT.
The authors of a 2011 study demonstrating that hand sanitizer alone could result in EtG and EtS concentrations of 1998 and 94 mug/g creatinine concluded that:
“in patients being monitored for ethanol use by urinary EtG concentrations, currently accepted EtG cutoffs do not distinguish between ethanol consumption and incidental exposures, particularly when uine specimens are obtained shortly after sustained use of ethanol containing hand sanitizer.”9
Sauerkraut and bananas have even recently been shown to cause positive EtG levels.10
![]()
A 2010 study found that consumption of baker’s yeast with sugar and water11 led to the formation of elevated EtG and EtS above the standard cutoff. EtG can originate from post-collection synthesis if bacteria is present in the urine.12 Collection and handling routines can result in false-positive samples.13
EtG varies among individuals.14 Factors that may underlie this variability include gender, age, ethnic group, and genetic polymorphisms.
“Exposure to ethanol-containing medications, of which there are many, is another potential source of “false” positives.15
Problems Exposed by Wall Street Journal and SAMHSA
On August 12, 2006, The Wall Street Journal published a front-page article, titled “A Test for Alcohol – And Its Flaws.”.16
Quoting Dr. Skipper, among others, the article includes:
“Little advertised, though, is that EtG can detect alcohol even in people who didn’t drink. Any trace of alcohol may register, even that ingested or inhaled through food, medicine, personal-care products or hand sanitizer.”
“The test ‘can’t distinguish between beer and Purell’ hand sanitizer, says H. Westley Clark, director of the Federal Substance Abuse and Mental Health Services Administration. . . ‘When you’re looking at loss of job, loss of child, loss of privileges, you want to make sure the test is right”, he says…”
“Use of this screen has gotten ahead of the science,’ says Gregory Skipper…”
Methinks Dr. Skipper might have realized this when he initially proposed it as an accurate test after a pilot study done on only a handful of subjects. Or perhaps when he used the LDT pathway to bypass FDA approval and oversight.
On September 28, 2006, SAMHSA, a federal agency that is part of the U.S. Department of Health and Human Resources, issued an Advisory, which on the first page contained a “grey box” warning, as follows:
 “Currently, the use of an EtG test in determining abstinence lacks sufficient proven specificity for use as primary or sole evidence that an individual prohibited from drinking, in a criminal justice or a regulatory compliance context, has truly been drinking. Legal or disciplinary action based solely on a positive EtG, or other test discussed in this Advisory is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”17
“Currently, the use of an EtG test in determining abstinence lacks sufficient proven specificity for use as primary or sole evidence that an individual prohibited from drinking, in a criminal justice or a regulatory compliance context, has truly been drinking. Legal or disciplinary action based solely on a positive EtG, or other test discussed in this Advisory is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”17
Bias has been identified as a large problem with drug trials.18 Industry-sponsored research is nearly four times as likely to be favorable to the company’s product as NIH-sponsored research.19 As an example, one survey of seventy articles about the safety of Norvasc (amlodipine) found that 96% of the authors who were supportive of the drugs had financial ties to the companies that made them.20
But what about the multi billion dollar drug-testing industry and the financial ties here?
Imagine if this was a drug and not a drug-test.
Essentially Greg Skipper and the FSPHP arm of ASAM launched a very lucrative joint business venture with a commercial drug-testing lab. They introduced the test via a loophole as a laboratory developed test. An LDT has no FDA regulation so the lab was able to promote, market and sell these tests with no meaningful oversight or accountability. Quest Diagnostics and USDTL are now working with the FSPHP and engaging in the same scheme.
The lab then contracted with state licensing boards and their state PHPs (who designed, implemented and managed drug and alcohol testing programs for nurses and doctors). A mutually beneficial scheme for the labs (who collect the samples) and the PHPs (who utilize, interpret and report the results.
The PHPs develop the arbitrary cutoff levels based on alleged “scientific” research and the labs promote whatever they say. “Gold-Standard,” “accurate” and “reliable.” 
EtG, EtS, Scram, PEth, Soberlink–all unsupported junk science introduced by prohibitionist profiteers without conscience.
How many lives were ruined by this test? How many careers were lost, families shattered and futures erased. I would venture to say a lot. Just look through all of the legal cases as I have. It is unconscionable. Sociopathic profiteering.
How many committed suicide feeling helpless, hopeless and entrapped?
At the end of a talk entitled Addicted Professionals: intervention, Evaluation and Treatment, Skipper presents a slide reading “Reporting or Assisting a Troubled Peer? These doctor’s can’t help themselves….” followed by graphic images of physician suicide. (see torrance_meeting_2 (4) ). It is for shock value and morbid humor and it is grotesque. He could not care less that these were human beings with wives, husbands, children and hopes and dreams.
How many scenes like this were repeated across the country because this guy gamed the system to get an ultra-sensitive test with abysmal specificity for a ubiquitous organic compound approved and marketed as a “forensic” test?
Forensic testing needs to be as close to 100% specific as possible because the results of a positive test can be grave and far reaching. Getting this test (and all the others) approved and marketed through a loophole and then getting the state Boards and Federation of State Medical Boards to approve them by moral entrepreneurship is unconscionable. Using the LDT pathway is just another example of how the “impaired physician movement” removes accountability and culpability by bending, ignoring or otherwise making their own rules.
And the labs have taken a “stand your ground” approach. Never admit wrongdoing. Never settle.
In a February 2007 article in the magazine “New Scientist,” Dr. Skipper is quoted
that:
“…there is not yet an agreed threshold concentration that can be used to separate people who have been drinking from those exposed to alcohol from other sources. Below 1000 nanograms of EtG per millilitre of urine is probably ‘innocent’, and above 5000 booze is almost certainly to blame. In between there is a “question zone…”![]()
No Dr. Skipper—it is you who is most certainly to blame. And what of all the people whose lives you ruined by introducing junk science with no evidence base via a regulatory loophole?? “probably innocent?” Shame on you Dr. Skipper…. Shame..shame..shame.


(from http://library.duke.edu/rubenstein/scriptorium/americavotes/jfk-civilrights-flyer.jpeg)
First they came for the Socialists, and I did not speak out—
Because I was not a Socialist.
Then they came for the Trade Unionists, and I did not speak out—
Because I was not a Trade Unionist.
Then they came for the Jews, and I did not speak out—
Because I was not a Jew.
Then they came for me—and there was no one left to speak for me
I’m reminded of Martin Niemöller’s famous poem today not only because it’s Remembrance Day, but because I’ve been researching effective ways to confront oppression. Researchers have found that the motive for the oppression doesn’t determine how easily it’s stopped. Effective confrontations usually involved allies who didn’t belong to the oppressed group, so as I suspected, all oppression (or abuse) is about power.
I’m not as surprised at the obviousness of the results as I am at how long…
View original post 171 more words

 “A body of men holding themselves accountable to nobody ought not to be trusted by anybody.”
“A body of men holding themselves accountable to nobody ought not to be trusted by anybody.”
― Thomas Paine
USDTL drug testing laboratory claims to advance the”Gold Standard in Forensic Toxicology.” “Integrity: Results that you can trust, based on solid science” is listed as a corporate value. “Unlike other laboratories, our drug and alcohol testing begins and ends with strict chain of custody.” “When people’s lives are on the line, we don’t skip steps.” Joseph Jones, Vice President of Laboratory Operations explains the importance of chain-of-custody in this USDTL video presentation.
Dr. Luis Sanchez, M.D. recently published an article entitled Disruptive Behaviors Among Physicians in the Journal of the American Medical Association discussing the importance of of a “medical culture of safety” with “clear expectations and standards.” Stressing the importance of values and codes-of-conduct in the practice of medicine, he calls on physician leaders “commit to professional behavior.”
Sanchez is Past President of the Federation of State Physician Health Programs (FSPHP). According to their website the FSPHP “serves as an educational resource about physician impairment, provides advocacy for physicians and their health issues at local, state, and national levels, and assists state programs in their quest to protect the public.” In addition the FSPHP “helps to establish monitoring standards.” The FSPHP is the umbrella organization of the individual State PHPs.
Sanchez is also the previous Medical Director of the Massachusetts state PHP, Physician Health Services, Inc. (PHS). According to their website PHS is a “nonprofit corporation that was founded by the Massachusetts Medical Society to address issues of physician health. PHS is designed to help identify, refer to treatment, guide, and monitor the recovery of physicians and medical students with substance use disorders, behavioral health concerns, or mental or physical illness.”
PHPs recommend referral of physicians if there are any concerns such as getting behind on medical records. As PHS Associate DirectorJudith Eaton explains “when something so necessary is not getting done, it is prudent to explore what else might be going on.” If the PHP feels that doctor needs an assessment they will send that doctor to a “PHP-approved” facility “experienced in the assessment and treatment of health care professionals.” The physician must comply with any and all recommendations of the assessment center. To assure this the physician must sign a monitoring contract with the PHP (usually five years). USDTL is one of the labs PHPs have contracted with for forensic drug and alcohol testing.

“Forensic” drug-testing differs from “clinical” drug-testing in how the results are used. “Clinical” tests are used for medical purposes in diagnosing and treating a patient.
A “forensic” test is used for non-medical purposes. It is not used for patient care, but for detecting licit and illicit substances in those who should not be using them. Pre-employment and employee assistance and professional monitoring programs are examples.
Forensic testing is held to a higher standards because the consequences of a positive result can be grave and far reaching. A positive forensic test can result in loss of rights of the individual being tested and his or her loved ones. Mistakes are unacceptable.
The Federation of State Medical Boards Policy on Physician Impairment supports this position stating “chain-of-custody forensic testing is critical” (page 14) and the “use of a Medical Review Officer (MRO) for screening samples and confirming sample results” (page 21).
Any and all drug testing requires chain-of-custody. The custody-and-control form is given the status of a legal document because it has the ability to invalidate a test that lacks complete information. Chain-of-custody provides assures specimen integrity. It provides accountability.
 The job of the MRO is to ensure that the drug testing process is followed to the letter and reviews the Custody and Control form for accuracy. The MRO also rules out any other possible explanations for a positive test (such as legitimately prescribed medications). Only then is the test reported as positive.
The job of the MRO is to ensure that the drug testing process is followed to the letter and reviews the Custody and Control form for accuracy. The MRO also rules out any other possible explanations for a positive test (such as legitimately prescribed medications). Only then is the test reported as positive.
The legal issues involved in forensic testing mandate MRO review. According to The Medical Review Officer Manual for Federal Workplace Drug Testing Programs
“the sole responsibility of the MRO is to”ensure that his or her involvement in the review and interpretation of results is consistent with the regulations and will be forensically and scientifically supportable.”
“Fatal flaws” such as lack of chain-of-custody form, missing tamper proof seal, missing signatures, or a mismatch of the sample ID and chain of custody ID invalidate the test. It is not reported. Tight chain-of-custody and MRO review is critical for the accountability and integrity of the sample.
The Medical Review Officer Certification Council provides a certification process for MROs. They  also follow their own Code of Ethics. In accordance with these standards PHS has an MRO to review all positive tests. As added assurance the FSPHP guidelines state that all positive tests must be approved by the Medical Director.
also follow their own Code of Ethics. In accordance with these standards PHS has an MRO to review all positive tests. As added assurance the FSPHP guidelines state that all positive tests must be approved by the Medical Director.

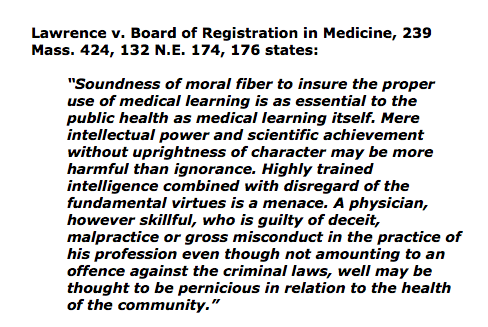
Good leadership requires correct moral and ethical behavior of both the individual and the organization. . Integrity is necessary for establishing relationships of trust. It requires a true heart and an honest soul. People of integrity instinctively do the “right thing” in any and all circumstances. The majority of doctors belong to this group.
Adherence to ethical codes of the profession is a universal obligation. It excludes all exceptions. Without ethical integrity, falsity will flourish.
The documents below show fraud. It is intentional. All parties involved knew what they were doing, knew it was wrong but did it anyway. The schism between pious rhetoric and reality is wide.

Positive Phosphatidyl Ethanol test at level of 365.4 (cutoff =20) No date of collection. place of collection or name of collector. Donor ID # = 461430 My Unique Identifier #1310 is nowhere on this document.
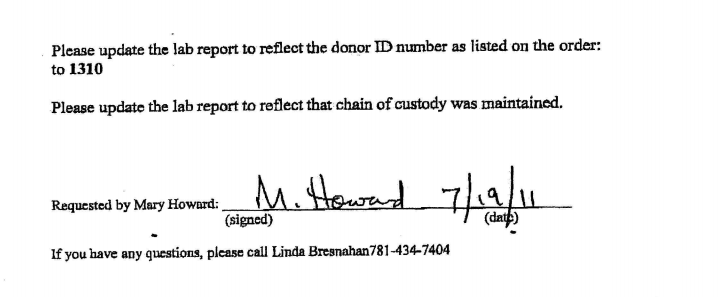
The July 19th, 2011 fax from PHS seen below is in reference to the lab report from USDTL seen above. In it PHS requests the report be “updated”to donor ID number “1310” and to “reflect that the chain of custody was maintained.”
The lab report is a positive test for the alcohol biomarker (Phosphatidyl Ethanol) or PEth, an alcohol biomarker introduced by the Federation of State Physician Health programs and marketed by USDTL and other labs to detect covert alcohol use..
There is no record of where, when or by whom it was collected.
 Both the donor ID # and chain of custody are listed as 461430.
Both the donor ID # and chain of custody are listed as 461430.
The purpose of chain-of-custody is to document the location of a specimen in real time. “Updating” it is not an option. It is prohibited. Updating the “chain of custody to reflect that chain of custody was maintained” is a clear indicator that it was not maintained.
ID #1310 is the unique identifier I was issued by PHS. It is used as a unique identifier, just like a name or social security number, to link me to any sample collected for random drug and alcohol screening. #1310 identifies me as me in the chain-of-custody. On July 1st, 2011 I had a blood test collected at Quest Diagnostics.

The sample was collected at Quest Diagnostics on July 1, 2011 but these documents were not obtained until December 3, 2011 and were included in the “litigation packet” which documents chain-of-custody and is generated on any and all forensic drug testing. It provides proof that the test was done on who it was supposed to have been done and that all required procedure and protocol was followed. It protects the donor form being falsely accused of illicit substance use. In most employee drug-testing programs the litigation-packet is provided on request immediately. It is a transparent process. This is not the case, however, at PHS.
I requested the litigation packet immediately after the positive test was reported on July 19, 2011. PHS first refused, then tried to dissuade me. They finally agreed but warned there would be “unintended consequences. The entire litigation packet can be seen here: Litigation Packet 12:3:2011
The positive sample has no chain-of-custody linked to me, no date, and no indication where it was collected or who collected it. In addition there was no “external” chain of custody for the sample. The custody-and-control form was missing.
With multiple fatal flaws (6/6) rendering it invalid, USDTL should have rejected it by their own written protocol.
6/6 Fatal Flaws–Just one invalidates the Test
USDTL did not reject it. The document below shows that USDTL added my ID # 1310 and added a collection date of July 1, 2011–the day I submitted the sample.

“REVISED REPORT PER CLIENTS REQUEST”
And in doing so the lab that claims “integrity” and “strict chain of custody” readily, and with no apparent compunction” manufactured a chain-of-custody and added a unique identifier by faxed request.
The litigation packet was signed by Joseph Jones on December 3, 2011. There was no record of where the sample was from July 1st to July 8, 2011. No external chain-of-custody or custody-and-control form was evident in the litigation packet.

The V.P. for Laboratory operations for the lab that claims “strict chain of custody” and that “doesn’t skip steps” “when “peoples lives are on the line” verified a positive test as positive with no custody and control form, no external chain of custody and 6/6 fatal flaws. What is so shocking is that this was done without compunction or pause. As a forensic test ordered by a monitoring program Jones knew full well it would result in significant consequences for someone. He knew that someones “life was on the line,” knew it was wrong, and did it anyway.
A person of conscience would never do this. It is unethical decision making that goes against professional and societal norms. A “moral disengagement” that represents a lack of empathy and a callous disregard for others. I would not consider doing something like this for any price and here it appears to be standard operating procedure.
PHS reported the positive test to the Medical Board on July 19, 2011 Positive PEth July 19, 2011-1. It was used as a stepping-stone to request an evaluation at one of three “PHP-approved” facilities (Marworth, Hazelden and Bradford). The Medical Directors of all three facilities can be seen on this list list called “Like-Minded Docs.” The MRO for PHS, Dr.Wayne Gavryck, whose job was to review the chain-of-custody and validate its integrity before reporting it as positive is also on the list. See this simplified schematic of how it works in Massachusetts. It shows how this is a rigged game.
Expecting to be diagnosed with a non-existent problem and admitted for non-needed treatment I requested an evaluation at a non-12 step facility with no conflicts-of-interest. Both PHS and the Medical Board refused this request in one of four violations of the Establishment Clause of the 1st amendment.

I chose Hazelden. The Medical Director was aware that I had just signed a patent license agreement for an epinephrine auto-injector and he had a child with a peanut allergy. We talked about the device and discussed the problems with current management. I think it was because of this added personal interaction that he did not “tailor my diagnosis” as PHS most certainly requested. Seeing me as a person rather than an object, I believe, enabled his conscience to reject it. My discharge diagnosis found no history of alcohol issues but they could not explain the positive test. Unable to rule out that I drank in violation of my PHS contract they recommended I attend AA.
PHS mandated that I attend 3 12-step meetings per week and requested that I obtain names and phone numbers of fellow attendees so they could contact them to verify my attendance. They also mandated that I discontinue my asthma inhalers (as the propellant contains small amounts of ethanol) that had been controlling my asthma and preventing serious attacks for the previous ten years. I was threatened that if I had to use the inhalers or one day late on the increased payments I would be reported to the Board and lose my license.


Sanchez states that my request for the “litigation packet” was processed on December 5, 2011 (two days after Jones signed off on it) and adds the “testing laboratory is willing to support the test results.”
In the interim I filed a complaint with the College of American Pathologists. I also requested the missing external chain of custody documents from Quest.

I never received the chain of custody from Quest. Instead I received a letter from Nina Tobin, Compliance Manager for Quest documenting all the errors but written to sound as if some sort of protocol was maintained. Tobin claimed the specimen was inadvertently logged as a clinical specimen but sent on to USDTL a week later. (See Quest Letter )

The Chief of Toxicology at MGH wrote a letter to the Board documenting all of the misconduct and irregularities stating that it was an “intentional act” perpetrated by PHS. MLLv3finalJacob_Hafter_Esq_copy.
This letter, as well as the opinions of everyone outside of PHS was ignored. So too were any opinions of my two former Associate Directors at PHS. The e-mail below dated October 10th, 2011 is to to Drs. John Knight and J. Wesley Boyd and I am referring to their article Ethical and Managerial Considerations Regarding State Physician Health Programs that was about to be published. We had hoped that it would draw more attention to the problems with PHPs.

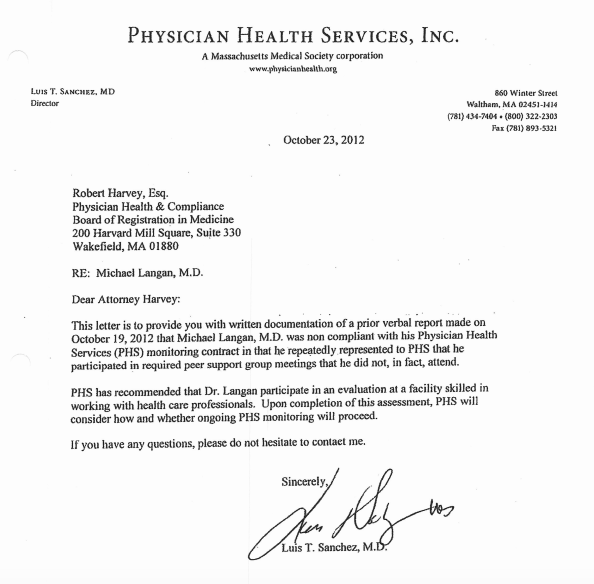
I was subsequently reported as “non-compliant” with AA meetings. They could not give any details of where or when. They then misrepresented a declaration of fact (I stated that I had started going to a specific meeting on a specific date) as an admission of guilt by saying I was referring to a different meeting. 10:23:12 PHS Letter to BORM-noncompliance.
My Chief at MGH, his Chief and others held a conference with PHS and attempted to remove me from PHS and replace the monitoring contract with one of their own. They refused. When confronted with the fabricated test they dismissed it and focused on sending me to Kansas to one of the “disruptive physician” Psikhuskas where they are using polygraphs (despite the AMAs stance that it is junk science) and non-validated neuropsychological instruments that detect “character defects” to pathologize the normal.
I refused. Had I gone to Kansas I would have been given a false diagnosis and my career would be over. This is what they do.
Amy Daniels, the investigator for the College of American Pathologists contacted me in December of 2012 to see how things were going since USDTL “amended” the test. Daniels told me that the College of American Pathologists confirmed my allegations and, as an Accrediting Agency for Forensic Toxicology mandated that USDTL correct it. (Labs can lose accreditation if they do not comply with CAP Standards for Forensic Drug Testing). This was done on October 4, 2012.
PHS denied any knowledge of an amended test. I also wrote an e-mail to Joseph Jones requesting the document but he did not reply.
I contacted CAP. On December 11, 2012 Dr. Luis Sanchez wrote a letter stating “Yesterday, December 10 2012, Physician Health Services (PHS) received a revision to a laboratory test result”
“The amended report indicates that the external chain of custody protocol [for that sample] was not followed per standard protocol]”Sanchez dismisses this test as irrelevant, rationalizing neither PHS nor the Board based any actions on the test and they would “continue to disregard” it.

The logic is that it was my behavior that resulted in any consequences. My “non-compliance” in October led to my suspension and the test had nothing to do with it. The sole reason for reporting me to the Board in 2011 was the positive test. There is no other pretext to use. It is misattribution of blame as without the test, now invalidated, there would have been no AA meetings to say I was non-compliant with.
In response to a civil complaint PHS, Quest and USDTL all took the position that the results of the fraudulent testing had absolutely nothing to do with anything.
And in response to the allegations of forensic fraud the labs claimed there was no forensic fraud because this was not a “Forensic” test but a “clinical” test. The argument was that “clinical” tests do not require chain-of-custody and it was his behavior not these tests that resulted in consequences.
As a “clinical” test I knew it was considered Protected Health Information (PHI) under the HIPAA-Privacy Rule. A patient must give written consent for any outside entities to see it. Obtaining lab tests previously required the consent of both the patient and the ordering provider. What PHS and the labs were apparently unaware of was the changes to the HIPAA-Privacy rule giving patients increased rights to access their PHI. The changes removed the ordering provider requirements. A patient has a right to obtain lab test results directly from the labs and has 30 days to do it. CAP agreed. USDTL sent me all of the documents. They can be seen below:
August 6, 2014 to Langan with health materials.
The documents sent by USDTL are notable for two things:
1. The e-mail from me to Joseph Jones dated December 10, 2012. It can be seen on page 22 of the USDTL documents. 

2. USDTL document confirming PHS knew the test was amended 67-days before they said they did.
The document shows PHS and Sanchez were aware of the invalidity of the test on October 4, 2012. Instead of correcting things they initiated machinations to throw me under the bus. They officially reported me to the Board for non-compliance on October 19, 2012.
The December 11, 2012 letter signed by Sanchez states “Yesterday, December 10, 2012, PHS received a “revised report” regarding the test. The documents show he knew about it 67-days prior.

Although USDTL complied with the HIPAA-Privacy Rule and CAP, Quest did not. Quest Diagnostics refused to send me copies of their lab reports claiming it was confidential and protected information that required PHS consent. Quest required I sign a consent form with multiple stipulations regarding PHS. I refused and contacted the Department of Justice -Office of Civil Rights. The DOJ-OCR agreed with me and I received the Quest documents
Remember a “clinical” test can only be ordered by a physician in the course of medical treatment. It requires authorization from the patient to obtain a “clinical” specimen and it requires written authorization as to who sees it. Referring physician was Mary Howard.
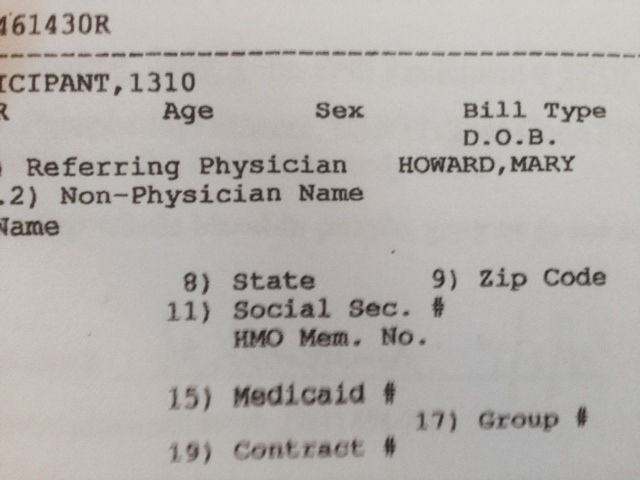
And below is the fax from PHS to Quest from July 1, 2011 also requested by Mary Howard. The signature on the front is not mine. In addition I gave the blood at 9:30 and was in my clinic at MGH at 12:23 so it couldn’t be. The WC 461430 R are dated July 2, 2011. This is a “clinical” not “forensic” sticker. The “R” indicates a red top tube. The other sticker is USDTL and indicates it was logged in on July 8, 2011.

What does it all mean? Blood left in a red top tube ferments. This is basic chemistry. The PEth test needs to be refrigerated and shipped overnight to prevent this. In addition it needs to be collected with a non-alcohol wipe in a tube that has an anti-coagulant or preservative so that it does not ferment. It requires strict procedure and protocol.
When I gave my blood on July 1st, 2011 it was as a “forensic” test per my contractual agreement with PHS.
On July 2, 2011 it was changed to “clinical.” Why? because “forensic” protocol would have invalidated it.
The only conceivable reason for doing this was to bypass chain-of-custody procedures. My unique identifier #1310 was removed and the clinical specimen number was used for chain-of-custody. The R in 461430R indicates a red top tube.
By holding on to it for one week the blood fermented. As it was July with an average temperature close to 90 they overshot their mark a bit. My level of 365 is consistent with heavy alcohol use–end stage half-gallon a day type drinking.
Quest then forwarded it to USDTL with specific instructions to process it as a “clinical” sample. USDTL complied and processed it as a clinical specimen which was reported it to PHS on July 14, 2011.

PHS then asked USDTL to add my forensic ID # 1310 and add a collection date of July 1, 2011 so it would appear “forensic” protocol was followed. The reason Jones signed the “litigation packet” on December 3, 2011 was because that was when the “litigation packet” was manufactured. A “clinical” sample does not produce one.
USDTL willingly complied with this request.

PHS then reported this as a “forensic” test to the Medical Board on July 19, 2011 and requested a reevaluation.

The distinction between “forensic” and “clinical” drug and alcohol testing is black and white. PHS is a monitoring program not a treatment provider. The fact that a monitoring agency with an MRO asked the lab to process and report it as a clinical sample and then used it forensically is an extreme outlier in terms of forensic fraud. The fact that they collected it forensically, removed the forensic components and let it sit in a warehouse for a week is abhorrent. The fact they then specifically requested it be processed as a clinical sample deepens the malice. The fact that they then reported it to the Board as a forensic sample and maintained it was forensic up until just recently makes it egregious. But the fact that the test was changed from “positive” to “invalid” on October 4th, 2012 and they then reported me to the Board on October 8th, 2012 for “noncompliance,” suppressed it and tried to send me to Kansas where I would be given a non-existent diagnosis to delegitimize me for damage control makes it wantonly egregious. This is political abuse of psychiatry.
Accountability requires both the provision of information and justification of what was done.
For doctors it is very difficult to obtain the information. As seen here, they put up a gauntlet to prevent the provision of what is immediate in all other drug testing programs. I now have all of the information. What it shows is clear. This was intentional. It was no accident. They knew what they were doing, knew it was wrong but did it anyway.
Accountability also requires that those who commit misconduct suffer consequences. The PHPs have also put up barriers to this. With no regulation or oversight they have no apparent accountability.
My understanding is that it works this way. The Medical Board, Medical Society and Departments of Public Health have no oversight. The MMS has an ethics committee but all they can do is “educate” the person if they feel there was a violation. The DPH won’t even look at it and the Board is complicit.
My understanding is that they have convinced law enforcement that this is a “parochial” issue that is best kept within the medical community. They have also created the impression that they are “friends” of law enforcement. I have heard from many doctors that they have tried to report misconduct, civil rights violations and crimes to the police, AGO, and other law enforcement agencies only to be turned back over to the PHP. By saying the physician is “impaired” it delegitimizes and invalidates the truth. “He’s just a sick doctor, we’ll take care of him.” That physician then suffers consequences effectively silencing the rest.
PHS uses the Board to enforce punitive measures and temporize. The Board puts blind faith in PHS. Blind faith that defies common sense ( mandating phone numbers at anonymous meetings) and disregards the law (Establishment Clause violations that are clear and well established). The Board also temporizes to cause damage.
In my case they required a psychiatric behavioral evaluation. I was given the choice of Kansas and a few other Like-minded assessment centers.
After petitioning for multiple qualified psychiatrists that were summarily rejected months later for no reason one of the Board Attorneys suggested Dr. Patricia Recupero, M.D., J.D. who is Board Certified in Forensic Psychiatry and Addiction Psychiatry. The Board had used her in the past but not recently. Seeing that she had been used by the Board for fit-for-duty evaluations in the past the Board accepted my petition.
Dr. Recupero wrote an 87-page report. She concluded I was safe to practice medicine without supervision, that I had never had an alcohol use, abuse or dependence problem, and that PHS request for phone numbers was inappropriate. She also documented PHS misconduct throughout my contract and concluded it was PHS actions, not mine, that led to my suspension. What she describes is consistent with criminal harassment. She documents the falsification of neuropsychological tests and confirms the forensic fraud. What did the Board do? Ignored their very own recommended and approved evaluator.
One measure of integrity is truthfulness to words and deeds. These people claim professionalism, ethics and integrity. The documents show otherwise. The careers and lives of doctors are in these peoples hands.
Similar fraud is occurring across the country. This is an example of the institutional injustice that is killing physicians. Finding themselves entrapped with no way out, helpless and hopeless they are feeling themselves bereft of any shade of justice and killing themselves. These are nothing more than bullies and accountability is essential. The “disruptive physician” moral panic has harmed the Medical Profession.
Dr. Clive Body in his book Corporate Psychopaths writes that “Unethical leaders create unethical followers, which in turn create unethical companies and society suffers as a result.” And according to Dr. Robert Hare in Without Conscience “If we can’t spot them, we are doomed to be their victims, both as individuals and as a society. ”
Wes Boyd notes that valid complaints from physicians are often dismissed as “bellyaching” by the PHPs. Complacent that these are just good guys helping doctors and protecting the public the complaints are dismissed, tabled, deflected or otherwise ignored. Bellyaching?? Is this bellyaching.
It is my opinion that what you see here is indefensible Procedurally, Ethically, and Legally.
Procedurally it goes beyond negligence and represents fraud. It violates every procedural guideline, regulation and standard of care including their very own.
Ethically it violates everything from the Hippocratic Oath to AMA Medical Ethics to the MRO Code of Conduct.
And where was PHS MRO Wayne Gavryck? By my count he violated at least 4 of the 6 Codes of Ethical Conduct.

What was done here violates the most fundamental ethical principles of Medicine -Autonomy, Beneficence, Nonmaleficence and justice.
Intentionally falsifying a laboratory or diagnostic test to refer for an evaluation or support a diagnosis or give unwarranted “treatment” is unconscionable. Abuse under the utility of medical coloration is especially egregious.
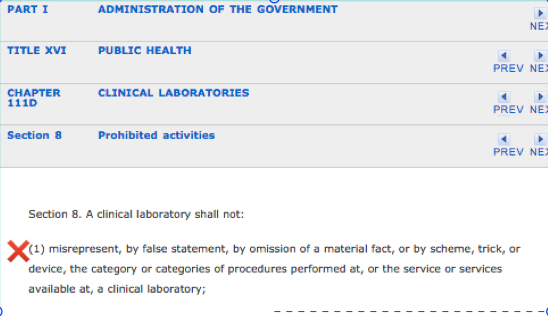
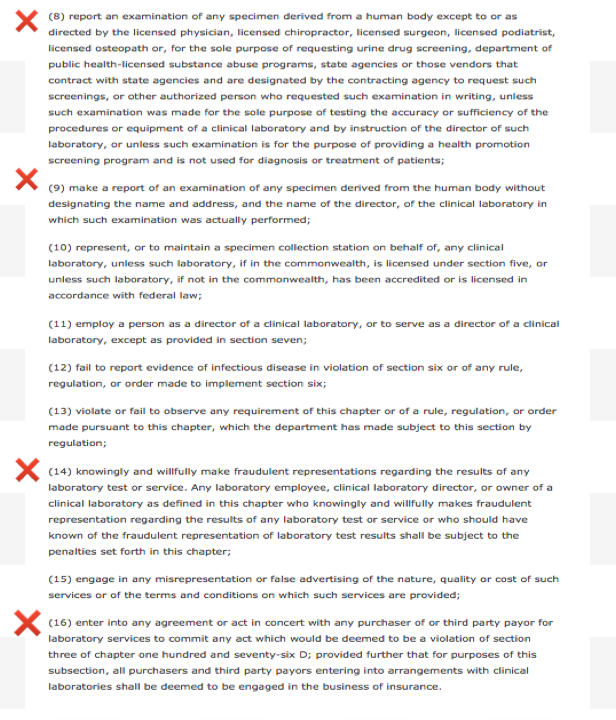
The information provided herein should negate any “peer-review” protection or immunity afforded PHS as it is undeniably and egregiously in “bad faith.” Moreover, the ordering a “clinical” test is outside PHS scope, practice, and function of PHS. According to M.G.L. c. 111, § 203 (c):
Dr. Luis Sanchez and Dr. Wayne Gavryck need to be held to the same professional standards as the rest of us.
If you can support either of them procedurally, ethically, or legally, any one of them, then I will turn in my medical license with a bow on it. If they did not commit negligent fraud by standards of care and procedural guidelines, egregious moral disengagement in violation of ALL ethical codes for the medical profession and society and break the law then disprove me. Just one will do.
But you can’t do this then I ask that you speak up and take a stand. Either defend them or help me hold them accountable. If a crime is committed it needs to be addressed. Ignoring encourages more of the same.
And if this cannot be supported procedurally, ethically or legally then I want to know what is going to be done about it?
How low does the moral compass have to go before someone takes action?
Doctors are dying across the country because of people just like this. They have set up a scaffold that removes the usual checks and balances and removed accountability. It is this institutional justice that is driving many doctors to suicide.
So the evidence is above. Either defend them or help me draw unwanted attention to this culture of bullying and abuse. So I am asking you to contemplate if what you see here is ethically, procedurally or legally sound. If you can show just one of these then I stand corrected. But if you cannot justify this on any level then I want you to help me expose this criminal enterprise. Either defend it or fight it. Silence and obfuscation are not acceptable.









Before the 2012 Drug and Alcohol Testing Industry Association (DATIA) annual conference, Dr. Robert Dupont delivered a speech entitled “Drug Testing and the Future of American Drug Policy.” He describes a “New Paradigm” for substance abuse treatment that enforces “zero tolerance for alcohol and drug use” that is enforced by monitoring with frequent random drug and alcohol tests in which positive tests are “met with swift, certain, but not draconian, consequences.” The paradigm is based on the current Physician Health Programs blueprint. Dupont states:
“…physician health programs , have set the standard for effective use of drug testing. These pioneering state programs provide services to health care professionals with substance use disorders. The programs are run by physicians, some of whom in recovery themselves. PHPs feature relatively brief but highly focused treatment followed by active lifelong participation in the 12-step fellowships of Alcoholics Anonymous and Narcotics Anonymous. The key to the success of the PHP system of care management is the enforcement of the standard of zero tolerance for any alcohol or other drug use by intensive long-term random testing for both alcohol and drugs with swift and certain consequences for even a single use of alcohol or any other drugs of abuse. PHPs use drug panels of 20 or more drugs. The PHPs commonly use EtG and EtS tests to detect recent alcohol use. Similar comprehensive programs have been developed for commercial pilots and attorneys. These innovative programs of care management produce unprecedented long-term, outcomes.”Physician Health Programs use a doctor’s medical license as “leverage” in what they call “contingency management.” What this means is that a doctor who is being monitored by a PHP must comply with any and all demands of the PHP under threat of being reported to the state Medical Board and loss of licensure. Dupont wants to extend the PHP model to other populations including kids.
The 2013 American Society of Addiction Medicine White Paper on Drug Testing describes the organizational structure of the “New Paradigm” which includes utilization of the medical profession as a urine collection agency for their drug and alcohol testing. When a doctor-patient relationship exists the testing is rendered “clinical” rather than “forensic.” Thus the consequences of a positive test can be deemed “treatment” rather than punishment. This bypasses the strict chain-of-custody and Medical Review Officer requirements designed to ensure accuracy and minimize false-positives. Forensic drug testing is tightly regulated because the results a positive test can be grave and far reaching. Erroneous results are unacceptable.

As onerous, unwarranted and unjust as this future dystopia sounds it may very well come to fruition. Across the country doctors have been going to the media, law enforcement, and the ACLU complaining of ethical breaches, civil rights violations, abuse and criminal activity only to be turned a deaf ear. The Federation of State Physician Health Programs has been able to construct this scaffold with no meaningful opposition and below the public radar. They have done this by removing accountability at all levels. By preventing access to information and erecting a system without oversight no consequences exist to deter misconduct and abuse. The same tactics and strategies will be used as they expand this to other populations.
American Society of Addiction Medicine, The Federation of State Physician Health Programs, and Like-Minded Docs
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we’d resolve their differences. Having learned to live so happily, we’d show everybody else how. Why, we thought, our Society of Alcoholics Anonymous might prove to be the spearhead of a new spiritual advance! We might transform the world”.–Twelve Steps and Twelve Traditions 1953 A.A. World ServicesThe American Society of Addiction Medicine exists to trump the 12-step chronic relapsing brain disease model of addiction as defined by A.A. The authoritarian view necessitates the authority maintain authority so everything is engineered around that goal.
The American philosopher Eric Hoffer noted:
“The only way to predict the future is to have power to shape the future. Those in possession of absolute power can not only prophesy and make their prophecies come true, but they can also lie and make their lies come true.”
The PHP model is built on the very foundation Hoffer describes.
“Addiction Medicine” not a recognized medical specialty.
This begins with the ASAM itself. “Addiction Medicine” and ABAM “board certification” is not recognized by the American Board of Medical Specialties. The requirements for this self-certification are not commensurate with ABMS certifications and only requires a medical license and board certification in ANY specialty.
Dubious Drug Testing-Not FDA approved, Conflicts-of-Interest
Federal workplace drug testing is done in accordance with mandatory guidelines. This testing is regulated using FDA approved tests with established sensitivity, specificity, and cutoff levels. FDA approval requires rigorous research and proven validity. The FDA requires valid scientific evidence (with both clinical and analytical validation) The FSPHP has introduced non-FDA drug testing via a loophole that removes accountability. The EtG, EtS, and PEth tests were introduced as Laboratory Developed Tests (LDTs) with little evidence base. The LDT pathway was developed for “clinical” tests of low market potential that would not otherwise make it to market as the FDA approval process would be prohibitive. An LDT does not even require in vivo testing or proof that the test actually tests for what it s claimed to test. Without FDA oversight, however, the labs can claim anything they want with no accountability. After getting the labs to develop the tests the FSPHP then convinced the Medical Boards they were both necessary and accurate and began using them on doctors in PHP programs.
Changing Public Policy and Regulatory Authority to Increase Power and avoid Accountability
The 2011 FSMB Policy on Physician Impairment identifies, defines, and essentially legitimizes “potential impairment” and “relapse without use.”
A PHP Should be empowered to conduct an intervention based on clinical reasons suggestive of potential impairment. Unlike the Board which must build a case capable of withstanding legal challenge, a PHP can quickly intervene based on reasonable concern."
“Empowered” to conduct an “Intervention” for reasons “suggestive” of “potential” impairment means a doctor can be pulled out of practice for anything. It essentially gives them carte blanche authority. The disregard for physician rights, due process and validity is self-evident.
in 2011 The ASAM issued a Public Policy Statement on coordination between PHPs, regulatory agencies, and treatment providers recommending that only “PHP approved” treatment centers be used in the assessment and treatment of doctors. A recent audit of the North Carolina PHP found financial conflicts of interest and no documented criteria for selecting the out of state treatment centers they used. The common denominator the audit missed was that the 19 “PHP-approved” centers were all ASAM facilities whose medical directors can be seen on this list.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness.”
According to the FSPHP, physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years.”
The policy extends PHP authority to cover physical illnesses affecting cognitive, motor, or perceptive skills, disruptive physician behavior, and “process addiction” (compulsive gambling, compulsive spending, video gaming, and “workaholism”). It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A A language –stinking thinking.” AA language has entered the Medical Profession and no one even blinked. It will get worse.
The ASAM has monopolized addiction treatment in the United States. It has imposed it on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. It selects who will be monitored and dictates every aspect of what that entails. It is a, in fact, a rigged game.
The Need for Regulation, Oversight, and Accountability
Accountability is necessary to prevent corruption and requires both the provision of information and justification for actions. What was done and why? Accountability also necessitates consequences-the ability of outside actors to punish and sanction those who commit the misconduct. Without these constraints corruption is inevitable.
In 2012 Drs. John Knight and Wes Boyd recommended the medical community outside of PHPS provide oversight and demand accountability. As with the NC PHP audit, Ethical and Managerial Considerations Regarding State Physician Health Programs generated little interest from the medical community at large.
Because addiction is currently defined as a disease, addicts must be “treated” (which in the United States is more often coercive than voluntary), and “cured” (which is defined as remaining abstinent). When the disease concept is not strictly reserve for medical conditions but is expanded to any and all drug and alcohol use.
And this is how the ASAM “New Paradigm” will encroach upon others. This is why the ACLU needs to get involved. This is not just about doctors but about the future of society.
The ASAM white paper contains the following quote minimizing the critical role of the MRO in drug testing. They feel clinical testing is good enough. And unless you want mandated random drug and alcohol testing at your physician visits using non-FDA approved testing with swift and certain consequences you will need to speak up. This occurred in the medical profession rapidly and with little notice. And that is how it will occur in other venues.
Unlike forensic drug testing where the test results must be able to meet rules of evidence in administrative, civil or criminal proceedings, clinical drug testing* is part of a patient examination performed by a clinician with whom the patient is in a therapeutic relationship. The testing is used for the purposes of diagnosis, treatment, and the promotion of long-term recovery. Clinical drug test results must meet the established standards of medical practice and benefit the therapeutic relationship, rather than meeting the formal legal requirements of forensic testing. Drug testing in medicine employs the same sound procedures, safeguards, and systems of information management that are used for all other health-related laboratory tests, tests on which life-and death medical decisions are commonly made.State Physician Health Programs have no meaningful oversight or accountability. Across the country doctors are reporting ethical and civil rights abuses and even criminal activity to law enforcement, the ACLU and the media. With the exception of North Carolina their complaints were patently ignored. Feeling hopeless, helpless, defeated and entrapped many are killing themselves. Institutional justice is a protective factor for preventing suicides. None exists here. The North Carolina PHP audit revealed conflicts-of-interest and no oversight by the state medical society or board. The audit also found that abuse could occur undetected because of this lack of accountability.
There seems to be a willful ignorance or apathy regarding PHPs. Perhaps most take the side of the PHPs complacent that these are just helping sick doctors and protecting the public the complaints are nothing more than “bellyaching.” In reality the misconduct and abuse perpetrated by the PHPs is commensurate with the behavior of Dr. Farid Fata, the Detroit Oncologist who intentionally misdiagnosed patients with cancer so he could make money off unnecessary chemotherapy treatment. Dr. Fata’s egregious betrayal of trust and unconscionable acts generated a flurry of comments. His vile acts resulted in an appropriate response.
The exact same misconduct is being perpetrated by PHPs but being overlooked, justified or otherwise ignored. Dr. Fata intentionally misdiagnosed patients with cancer who did not have cancer so he could give them chemotherapy to make money. PHPs are intentionally misdiagnosing substance abuse and behavioral disorders in physicians who do not have them in order to give them unneeded treatment and force them into monitoring contracts to both make money and gain control.
It undermines the very integrity of the profession. It is particularly vile when the betrayal of trust involves doing the opposite of what was entrusted. Abuse of positions of power, trust and influence in the field of medicine need to be both prevented, recognized and addressed. Oversight, regulation and accountability are essential if this is going to be accomplished. There are no exceptions. Policies and procedures must be enforced in a consistent manner.
The medical boards, medical societies, and departments of health have given the state PHPs carte blanche control and absolute power. They will not even investigate misconduct or even crimes.
And the PHPs have convinced law enforcement that this is a parochial matter. Doctors reporting crimes are often turned back over to the PHP.
This refusal to investigate or even acknowledge valid and factual complaints of professional misconduct has not only prevented the exposure of wrongdoing and corruption but deepened it. How does wrongdoing and corruption serve the best interests of the public or promote public health? It doesn’t. How could a culture that protects the perpetrators of unethical and indefensible misconduct yet turns a deaf ear to their victims possibly contribute to the common good? It can’t. And giving an oppressive, illegitimate and irrational tyranny absolute power and granting them unrestrained managerial prerogative over doctors is fallacy.
“Every time we turn our heads the other way when we see the law flouted, when we tolerate what we know to be wrong, when we close our eyes and ears to the corrupt because we are too busy or too frightened, when we fail to speak up and speak out, we strike a blow against freedom and decency and justice.”
― Robert F. Kennedy



Three shells and a pea–ASAM, FSPHP, and LMD.
As home to some of the countries top ranked hospitals and most prestigious medical schools, Massachusetts is an international healthcare hub with world-class teaching, research and clinical care. Two of the top three psychiatric hospitals in the United States as rated by U.S. News and World Report are found here in Massachusetts with McLean Hospital earning the top prize and Massachusetts General Hospital ranked number three. However, this medical mecca of learning and research is apparently unable to attract anyone with the competence and skill to assess a physician for substance abuse or disruptive behavior.
In Massachusetts if the State PHP feels a physician is in need of an assessment the evaluation must be done at “a facility experienced in the assessment and treatment of health care professionals.” No exceptions. And apparently these esoteric skills are only found in Georgia, Arkansas, Alabama, Kansas, and a half dozen other far-away places.
With over 20 years experience with the Massachusetts PHP, Physicians Health Services, inc., Harvard Medical Schools Dr.’s John Knight and J. Wesley Boyd wrote an article in the Journal of Addiction Medicine last year entitled “Ethical and Managerial Considerations Regarding State Physician Health Programs.”
One of the issues they discussed was the conflicts of interest between the state PHPs and the “PHP-approved” evaluation centers. The conflicts-of-interest between state Physician Health Programs and these “PHP-approved” assessment and treatment centers were also uncovered in the recent state Audit of the North Carolina PHP. What was not uncovered, however, was just how absolute these conflicts of interest are. It is a smoke and mirrors closed system of false choice An elaborate charade of verisimilitude. Carnival hucksters in medical smocks.
One comment in Knight and Boyd’s article that I was surprised got past editorial review was that the treatment centers may “consciously or otherwise” tailor diagnosis and recommendations to the PHP’s impression of that physician. “consciously” tailoring a diagnosis is fraud. It is political abuse of psychiatry. It is unethical and unconscionable. It is, in fact, a crime. Political abuse of psychiatry right here in the United States.
And if you cross-reference the medical directors of the “PHP-preferred facilities” with this list of Like-Minded Docs it is a perfect match.
Therefore when the PHP refers a physician for an evaluation and gives them a choice of an assessment facility there is no choice. It is three card monte. A shell game. Heads I win tails you lose. Isn’t it about time this unethical and unconscionable rigged referral process be exposed.



The Medical Profession, Moral Entrepreneurship, Moral Panics, and Social Control.

As a society governed by organizations, associations, institutions and regulatory bodies, the medical profession is not immune to “moral panics” and “moral crusades.”
A threat to patient care or the values of the profession can be identified and amplified. A buildup of public concern fueled by media attention ensues creating a need for governing bodies to act. Medical Professionalism and the Public Health has been assailed.
Unbeknownst to the general population and most members of the medical profession at large, certain groups have gained tremendous sway within organizational and regulatory medicine. Through moral entrepreneurship they have gained authority and become the primary definers of the governance of the medical profession and the social control of doctors. To benefit their own interests they have fostered and fueled “moral panics.” Exhorting authorities to fight these threats by any means necessary they have successfully made and enforced rules and regulations and introduced new self-serving definitions and tools that neither help doctors nor protect the public.

 The Medical Profession, Moral Entrepreneurship, and Social Control
The Medical Profession, Moral Entrepreneurship, and Social Control
Sociologist Stanley Cohen used the term “”moral panic” to characterize the amplification of deviance by the media, the public, and agents of social control.1 Labeled as being outside the central core values of consensual society, the deviants in the designated group are perceived as posing a threat to both the values of society and society itself. Belief in the seriousness of the situation justifies intolerance and unfair treatment of the accused. The evidentiary standard is lowered.
Howard Becker describes the role of “moral entrepreneurs,” who crusade for making and enforcing rules that benefit their own interests by bringing them to the attention of the public and those in positions of power and authority under the guise of righting a society evil. 2
And according to cultural theorist Stuart Hall, the media obtain their information from the primary definers of social reality in authoritative positions and amplify the perceived threat to the existing social order. The authorities then act to eliminate the threat.3 The dominant ideas or ideologies are reproduced by relying on the opinions of the defining authority and then spread through the media. The communal good has been assailed.
As a society governed by organizations, associations, institutions and regulatory bodies, the medical profession is not immune to “moral panics.” A threat to patient care or the values of the profession can be identified and amplified. A buildup of public concern fueled by media attention ensues creating a need for governing bodies to act. Medical Professionalism and the Public Health has been assailed.
Unbeknownst to the general public and most members of the medical profession at large, certain groups have gained tremendous sway within medical society. Through moral entrepreneurship they have gained authority and become the primary definers of the governance of the medical profession and the social control of doctors. To benefit their own interests they have fostered and fueled “moral panics” and “moral crusades. ” Exhorting authorities to fight these threats by any means necessary they have successfully made and enforced rules and regulations and introduced new definitions and tools with no meaningful resistance or opposition.
The Inquisition did not have to convince individual citizens or the general public of their beliefs to advance an agenda; just Ecclesiastical and Political Authority. Similarly, the “impaired physicians movement” did not have to convince individual doctors or the medical profession of their beliefs to further a self-serving agenda; just regulatory and administrative authority.
Addiction Medicine Monopoly, False Authority and Conflicts of Interest
The “impaired physicians movement” can be defined as a group of physicians with alcohol and substance abuse problems who, having found sobriety through 12-step spirituality, banded together to promote the ideology behind their personal “recovery” to other doctors and the medical community at large. In the 1980s the movement gained momentum and as their numbers grew began calling themselves specialists in “addiction medicine.” The American Society of Addiction Medicine (ASAM) is not a true specialty, but a Self-Designated-Practice-Specialty, which simply means that is what they are calling themselves. It reflects neither knowledge nor expertise.. “Board certification” by the American Board of Addiction Medicine (ABAM) is not recognized by the American Board of Medical Specialties (ABMS).
ABAM certification requires only a medical degree, a valid license to practice medicine, and completion of residency training in ANY specialty. Addiction Psychiatry, a subspecialty of psychiatry under the American Board of Neurology and Psychiatry is the only specialty recognized by the ABMS. and their specialty society is the American Academy of Addiction Psychiatry.
The ASAM is schooled in just one one uncompromising model of addiction with the majority attributing their very own sobriety to that model–the chronic relapsing “brain disease” with lifelong abstinence and 12-step spiritual recovery model. As the “voice of addiction medicine,” the ASAM has nevertheless defined the dominant treatment paradigm in the United States. ASAM doctors outnumber addiction psychiatrists by 4:1 and the movement is well funded. Because addiction is defined as a “disease”, addicts must be “treated” (more often coercive than voluntary), and “cured” (defined as abstinent). The billion dollar assessment and treatment industry and the drug and alcohol testing industry lucratively profits from this model which has grown to monopolize addiction treatment in the United States.
The goal of the ABAM Foundation is to “gain recognition of Addiction Medicine as a medical specialty by the American Board of Medical Specialties (ABMS).” A monopoly defined by self-appointed experts without recognized specialty training will soon likely Robber baron their way to being accepted as a true specialty.
Physician Health Programs, Regulatory Agencies, and Treatment Centers
Physician Health Programs (PHPs) meet with, assess, and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Unless being monitored by one, PHP practices are unknown to most physicians and operate outside the scrutiny of the medical community. Initially funded by State Medical Societies and staffed by volunteer physicians, PHPs served the dual function of helping sick doctors and protecting the public.
As the populations of ASAM physicians proliferated in the 1980s, many joined their state Physician Health Programs. PHP doctors who did not agree with the ASAM groupthink were gradually removed and they organized under the Federation of State Physician Health Programs (FSPHP). Other ASAM physicians found employment at treatment centers as staff physicians and medical directors.
The FSPHP cultivated a relationship with the Federation of State Medical Boards (FSMB) and the state PHPs formed alliances with their state medical boards. Promoting themselves as offering “treatment” rather than”punishment” they offered an alternative to disciplinary action. They then began promoting their successful outcomes in rehabilitating “impaired physicians”, and this history can be seen by examining the archives of the Journal of Medical Regulation and similar publications. In 1995 the Washington PHP claimed a success rate of 95.4%, Tennessee claimed 93% and Alabama 90%.
Part of this success was attributed to the specialized treatment centers for doctors directed by their ASAM colleagues such as Ridgeview Institute in Atlanta created by G. Douglas Talbott. Talbott, who helped organize and serve as past president of the ASAM claimed a 92.3 percent recovery rate. He also put forth a Medical Urban Legend–the proposition that doctors were a different species, separate from the rest of society, who needed special treatment three times longer than anyone else. Amazingly, this dicto simpliciter argument that can, in fact, be refuted simply by pointing it out was allowed to enter regulatory medicine unopposed. Simply because, sadly, no one ever pointed out the logical fallacy. It is now entrenched. Three months or more of treatment is standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value.
A 1995 issue of the FSMB publication The Federal Bulletin: The Journal of Medical Licensure and Discipline contains reports on eight separate state PHPs. The “almost 90% success rate” was applauded by the editor, who added “cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” And more recent reports suggest PHPs reduce malpractice claims. They are now being promoted as a replicable model to be used in other populations.
The problem is no one bothered to examine the methodology to discern the validity of these claims. There has been no critical analysis or Cochrane type review of any of these studies which are invariably small, methodologically flawed, and biased.
The FSMB has accepted them as expert authority and their authoritative opinion as fact. It is this acceptance of faith without objective assessment that has allowed the ASAM and FSPH to advance their agenda. By confusing ideological opinion with professional knowledge, the FSMB and state Medical Boards have acted as willing gulls each step of the way. No counter-forces existed. And they still don’t. Junk science and unvalidated neuropsychological testing is used by these groups unconstrained and willfully. There is no regulation, oversight, or accountability. They are using polygraph testing (despite the AMA’s previous public policy statement deeming it junk) to both condemn “disruptive” surgeons and deem convicted pedophiles fit to return to work. They have introduced junk-science in drug and alcohol testing and unvalidated “neuropsychological” testing to detect “character-defects” by getting regulatory agencies to accept the validity of these tests not by the Scientific Method or Evidence Based Research but by (to coin a term) “Regulatory Sanctification”
To paraphrase one FSPHP member, “Who needs evidence-based medicine when the boards have already accepted these tests as valid?” Who indeed?
The ideological bias and financial conflicts of interest between PHPs and the treatment centers was also not recognized. It still isn’t. The spotlights are apparently all on Big Pharma in this regard. Some sunlight needs to be exposed in the direction of the billion dollar drug and alcohol testing and assessment industry as well.
Doctors were held at Ridgeview three times longer than the rest of the population (and at three times the cost) under threat of loss of licensure. Although there is no evidence base or plausible explanation why an entire profession would have a three-times longer length of stay than the rest of the population this continues to be the reality. There is no choice.
in 2011 The ASAM issued a Public Policy Statement on coordination between PHPs, regulatory agencies, and treatment providers recommending that only “PHP approved” treatment centers be used in the assessment and treatment of doctors. It specifically excludes non “PHP -recognized” facilities. And what defines a “PHP approved” treatment center? In addition to finding essentially no oversight by the state medical society and medical board, a recent audit of the North Carolina PHP found financial conflicts of interest and no documented criteria for selecting the out of state treatment centers they used. The common denominator the audit missed was that the 19 “PHP-approved” centers were all ASAM facilities just like Ridgeview whose medical directors can be seen on this list.
The appeal to authority logical fallacy has enabled the FSPHP to become the expert authority on physician impairment through the eyes of the medical boards. It has also allowed them to increase their scope.
The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their 2011 annual meeting distinguishing “impairment” and “illness” stating that Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness.”
According to the FSPHP, physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years.”
The policy extends PHP authority to cover physical illnesses affecting cognitive, motor, or perceptive skills, disruptive physician behavior, and “process addiction” (compulsive gambling, compulsive spending, video gaming, and “workaholism”). It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
G. Douglas Talbott defines “relapse without use” as “emotional behavioral abnormalities” that often precede relapse or “in A A language –stinking thinking.” AA language has entered the Medical Profession and no one even blinked. It will get worse.
The ASAM has monopolized addiction treatment in the United States. It has imposed it on doctors through the FSPHP. The FSPHP political apparatus exerts a monopoly of force. It selects who will be monitored and dictates every aspect of what that entails. It is a, in fact, a rigged game.
Inherent in this model is the importance of external control. It gives them power to exert control over the individual regardless of whether they need to be treated.
By bamboozling regulatory medicine this was accomplished. And the maintenance of this relationship is necessary as this presentation by an FSPHP physician warns, “guard this relationship jealously.”
Moral Panics and Moral Crusades
By introducing and fueling moral panics the ASAM/FSPHP political apparatus has been able to expand in both scope and power.
The Medscape article “Drug Abuse Among Doctors: Easy, Tempting, and Not Uncommon” published in the “Business of Medicine” section in January 2014 is characteristic example of the authoritative opinion, propaganda, and misinformation spun to maintain a pervasive climate of fear. Proof by anecdote. Physicians are “5 times as likely as the general public to misuse prescription drugs” according to Lisa Merlo, PhD. “Given the epidemic of prescription addiction sweeping the nation, that’s a grim statistic.”
Described as a “researcher at the University of Florida’s Center for Addiction Research and Education,” Merlo’s research involving 55 doctors being monitored by their state Physician Health Program published in the Journal of Addiction Medicine in October 2013 found “most physicians who abuse prescription drugs” do so to “relieve stress and physical or emotional pain.” Nowhere is it mentioned on Medscape that Merlo is the Director of Research for the Florida state PHP Professionals Research Network. Physician access to medications through prescriptions, “networks of professional contacts, and proximity to hospital and clinic supplies” gives them “rare access to powerful, highly sought-after drugs” says Marvin D. Seppala, chief medical officer at Hazelden. This access “sets them apart” and “not only foment a problem” but”perpetuate it” says Seppala. “Access “becomes an addict’s top priority” and they “will do everything in their power to ensure it continues.”
“They’re often described as the best workers in the hospital,” he says. “They’ll overwork to compensate for other ways in which they may be falling short, and to protect their supply. They’ll sign up for extra call and show up for rounds they don’t have to do.” Physicians are intelligent and skilled at hiding their addictions, he says. Few, no matter how desperate, seek help of their own accord.” In reality this is absurd. And if you look at any of the current “moral panics” that are being used to suggest random suspicion-less drug testing of all doctors or promoting the Physician Health Programs as the “New Paradigm” you will inevitably find a doctor, just like Marv Seppala who is on this list as an author or interviewee. It is a given.
The terms “impaired physician” and the “disruptive physician” are used as labels of deviancy. As deviants who allegedly threaten the very core of medicine (patient care) and the business of medicine (profit) they must be stopped at all costs. Belief in the seriousness of the situation justifies intolerance and unfair treatment. The evidentiary standard is lowered. Aided by a “conspiracy of silence” among doctors in which impaired colleagues are not reported necessitates identification of them by any means necessary. Increase the grand scale of the hunt.
In this way these front-groups have successfully acted as moral entrepreneurs to make and enforce rules and put forth new definitions and mandates that serve their own interests. A retrospective non -blinded non-randomized cohort study with serious underlying methodological errors involving 904 physicians being monitored by PHPs is now being used to “set the standard for recovery.”

Across the Country doctors are going to the media, law enforcement, the AGO, and the ACLU only to be turned a deaf ear. Many consider this a “parochial” issue best handled by the medical community. Doctors reporting crimes are turned back over to the very perpetrators of the crimes. The Medical Societies and professional organizations contribute to the problem by willful ignorance. Accusations are used to disregard the claims of the accused. It is a system of institutional injustice that is driving many doctors to suicide. Hopeless, helpless, and feeling entrapped many are taking this route. And no one is talking about it. This cannot be avoided any longer.
The next target is the “aging physician.” And as they have done with the “impaired” and “disruptive” physician” the FSPHP and their affiliates are setting the stage for another “moral crusade.”






The juxtaposed documents in and of themselves reveal a number of red flags. How does one “revise” a chain-of-custody”? If you do a google search you will not find “chain-of-custody” as an object of the verb revise. It is an oxymoron. A document or opinion can be revised. A chain-of-custody, by its very definition, cannot. This collusion to fabricate a positive test has coined a new oxymoron—“revised chain-of-custody.” Go ahead and look it up. It is a novel one. As it should be.
What these documents show is, in fact, indefensible ethically, procedurally and legally. The first document signed by Dr. Luis Sanchez, past President of the FSPHP and past Medical Director of Physician Health Services, Inc. (PHS) was sent to the Board of Registration in Medicine on December 11, 2012 and is notable for two statements. The letter from Dr. Sanchez asserts that “Yesterday, December 10, 2012, Physician Health Services, PHS received a revision of a laboratory test result,” but it did not matter because PHS was {unaware} ” of any action taken by the Massachusetts Board of Registration in Medicine as a result of the July 28th, 2011 report. However, based on the amended report, PHS will continue to disregard the July 21st PEth test result.”
The second document, addressed to Dr. Luis Sanchez, is dated October 4, 2012 (67 days earlier) and shows the first document to be a bald-faced lie.
On July 28h 2011 Dr. Luis Sanchez reported to the Medical Board that I had a positive alcohol test.
Although I knew that Dr. Sanchez had fabricated the test I had no way of proving it. I requested the “litigation packet,” which records “chain-of-custody” from collection to analysis in August of 2011. At first they refused. PHS then tried to dissuade me (“it will be costly, involve attorneys, etc). Finally they agreed but threatened me with “unintended consequences.”
I was finally able to get a copy of the “litigation packet” in December of 2011. Remarkably, it showed that Sanchez had requested my ID # and a “chain-of-custody” be added to an already positive specimen. I reported this to the Board but they ignored it. I also filed a complaint with the College of American Pathologists.
On October 23, 2012 Sanchez reported to the Medical Board that I was “noncompliant” with requirements with A.A. meetings that I was supposed to go to as a direct result of the positive test and my license to practice medicine was suspended as a result in December 2012.
On December 10, 2012 I contacted the College of American Pathologists who told me the test was “amended” from “positive” to “invalid” on October 4, 2012. I confronted Sanchez and PHS and they said they did not know anything about it.
The following day, December 11, 2012, they sent out a letter saying that the test was invalid but that they were “unaware of any action taken against my license as a result of the test.”
The documents show that on July 19th, 2011 Sanchez requested my ID # 1310 and a “chain-of-custody” be added to an already positive specimen and on October 4th 2012 the test was “appended” to “external chain of custody not followed per standard protocol.”
Please note again that Dr. Sanchez stated on December 11, 2012 that he “just learned” about this on December 10, 2012. He reported me to the Board as “noncompliant” on October 23, 2012 and my license was suspended in December 2012. These documents show he had full knowledge that the test was invalid and as an agent of the Board this is under “color of law.” Both he, and PHS, need to be held accountable for this.

Lies, Lies, and More Lies
10:19:12-Verbal Compliant Noncompliance f:u written 10:19:12–BORM Complaint Committee
The contradictory documents from Sanchez alone constitute a crime (withholding information in concealment and providing false information to a state agency). But what he did is far far worse.
I just obtained the October 4th document. Although I knew it existed, PHS suppressed it and refused to acknowledge it. But in response to a complaint I filed against PHS and the labs it was revealed by USDTL that the test in question (phosphatidyl-ethanol) was not sent as a “forensic” specimen but collected as a “forensic” specimen, then changed to a “clinical” specimen at the request of PHS Program Director, Linda Bresnahan. The specimen was kept at the collecting lab (Quest) for 7 days as a “clinical” specimen, then sent to the analyzing lab (USDTL) with specific instructions from Quest to process it and report it as a “clinical” specimen. PHS then used it as a “forensic” specimen by reporting me to the Board of Registration in Medicine and requesting I undergo an evaluation for alcohol abuse.
As a “clinical” specimen it is rendered “Protected Health Information” (PHI) and thus under the HIPAA Privacy-Rule. So with the help of the College of American Pathologists I requested my PHI from both Quest and USDTL. Quest refused (for obvious reasons) but USDTL complied. And that is how I was able to obtain the October 4th document revealing that Dr. Sanchez lied to the Medical Board. I would love to hear him, or PHS MRO Wayne Gavryck, defend the indefensible (and unconscionable).
Dr. Sanchez is correct when he pleads ignorance of any action taken by the Board as a result of the July 21st PEth result. It was his report to the Medical Board that I was “noncompliant” with attending AA meetings (that I was supposed to go to as the direct and sole result of the positive test) that he reported to the Board just two weeks after the October 4th appended test.
The test was sent as a “clinical” specimen intentionally. PHS is not a clinical provider but a monitoring agency. They cannot send clinical samples. But since clinical samples are “protected health information” and under HIPAA the lab had to give me the records and here you have them.
The distinction between “forensic” and “clinical” drug and alcohol testing is black and white. PHS is a monitoring program not a treatment provider. The fact that a monitoring agency with an MRO asked the lab to process and report it as a clinical sample and then used it forensically is an extreme outlier in terms of forensic fraud. The fact that they collected it forensically, held it for 7 days and changed it from “forensic” to “clinical” to bypass strict “chain-of-custody” requirements deepens the malice. The fact that they then reported it to the Board as a forensic sample and maintained it was forensic up until now makes it egregious. But the fact that the test was changed from “positive” to “invalid” on October 4th, 2012 and Sanchez then reported me to the Board on October 23rd 2012 for “noncompliance,” suppressed it and tried to send me to Kansas for damage control makes it wantonly egregious. (they didn’t think I’d ever find out).
Add on that the fact that I’ve been questioning the validity of the test since day 1 and they violated the HIPAA Privacy Rule over and over and this is reckless and major health care fraud.
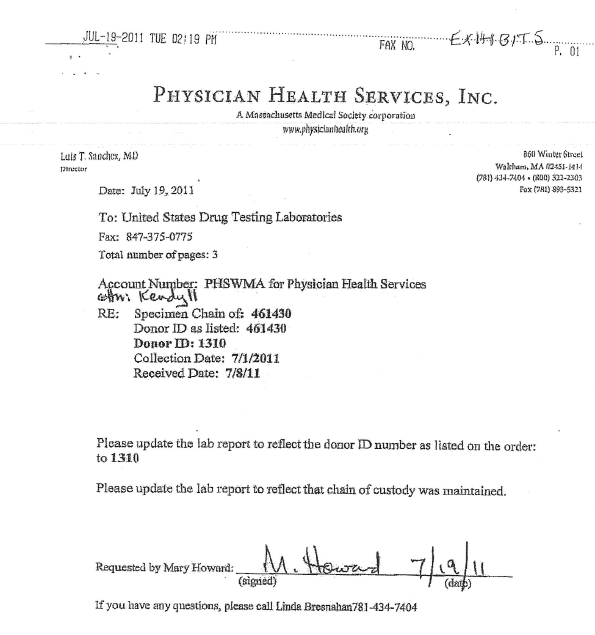
Fax from PHS to USDTL on July 19th, 2011 asking that my ID #1310 be added to an already positive test and a “chain-of-custody” be “updated”

USDTL complies with PHS request to and adds my ID #1310 and a date of collection (July 1, 2011) to an already positive specimen

No date of collection, no unique identifier linking specimen to me. Multiple “fatal flaws.”

I file complaint with CAP January 12, 2102. CAP forces USDTL to amend test from “positive” to “invalid” which they do on October 4, 2012. PHS conceals this fact until December 11, 2012
Letter from Chief of Toxicology at MGH–Ignored by PHS, USDTL, and the BORM 11:5:12-Dr. Flood Letter–Ignored by PHS:USDTL:BORM





{kind=link}