“This physician may be clinically competent; indeed, he may be technically superior. However, no one wants to refer patients to him. No one wants to assist him in surgery. He is the one who screams at nurses, belittles medical students and makes criticisms that go beyond the bounds of fair professional comment. However, he is not always loud. He can be the passive physician who will not answer the pager while on call, who does not show up at meetings and will not help find solutions to departmental problems. Indeed, this physician is not always male, but more often than not that seems to be the case.”
“This physician may be clinically competent; indeed, he may be technically superior. However, no one wants to refer patients to him. No one wants to assist him in surgery. He is the one who screams at nurses, belittles medical students and makes criticisms that go beyond the bounds of fair professional comment. However, he is not always loud. He can be the passive physician who will not answer the pager while on call, who does not show up at meetings and will not help find solutions to departmental problems. Indeed, this physician is not always male, but more often than not that seems to be the case.”
So begins “The Dreaded Task of Confronting Disruptive Physicians,” 1 a call to arms by Dr. Graeme M. Cunningham, M.D. (Fellow of the American Society of Addiction Medicine) published in the Journal of Medical Licensure and Discipline in 2004 (The official publication of the Federation of State Medical Boards (FSMB)) that helped launch a new paradigm for all those concerned with the physician “who has long eluded regulatory action, even though his behavior may have posed a risk to patient care and created chaos in his workplace for a number of years.”1
“These experiences lead us to the tentative conclusion that disruptive behavior, if not dealt with properly, is often the symptom of a greater underlying problem that will impede the safe practice of medicine. What may seem to be largely an annoyance could be a symptom, endangering patients. If identified early, disruptive physicians can be effectively treated and should be referred to appropriate programs for treatment.” 2

The American Society of Addiction Medicine and Federation of State Physician Health Programs (PHPs) set forth definitions of disruptive behavior, rules of evidence and regulation and the administrative procedures by which suspected doctors were “evaluated” and removed from practice.3
Written by the PHP doctors for PHP doctors, the disruptive physician construct came to be regarded as irrefutable truth and contributed to the identification and removal of an undetermined number of medical doctors. Although there was a general belief in “disruptive physicians” at the time of this call to arms they were not regarded as evil or life threatening. Society did not fear them and hospital administration and regulatory medicine did not feel the need to hunt them down. There were many scholars who publicly doubted this epidemic of disruptive physicians at the time. That would soon change.

On July 9, 2008 the Joint Commission became so concerned about “behaviors that undermine a culture of safety” that it issued a “Sentinel Event Alert” on the topic and developed a “Leadership Standard” requiring all hospitals to have a code of conduct as well as a process for managing disruptive and inappropriate behaviors.4-6

In 2011 the Federation of State Medical Boards issued an updated “Policy on Physician Impairment” giving full authority to physician health programs in the evaluation, treatment and ultimate fate of these doctors. The FSMB House of Delegates adopted an updated Policy on Physician Impairment at their annual meeting distinguishing “impairment” and “illness” stating that
“Regulatory Agencies should recognize the PHP as their expert in all matters relating to licensed professionals with “potentially impairing illness.”

According to the FSPHP, physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years.” The policy extends PHP authority to cover physical illnesses affecting cognitive, motor, or perceptive skills, disruptive physician behavior, and “process addiction” (compulsive gambling, compulsive spending, video gaming, and “workaholism”). It also defines “relapse without use” as “behavior without chemical use that is suggestive of impending relapse.”
From the mid 1980s until present day a confederacy of “authorities” calling themselves “addiction medicine” specialists assisted in identifying disruptive physicians. Shaping clinical and legal orthodoxy they set the standards that cooperating regulatory authorities could follow in criminalizing, persecuting and punishing heretics.
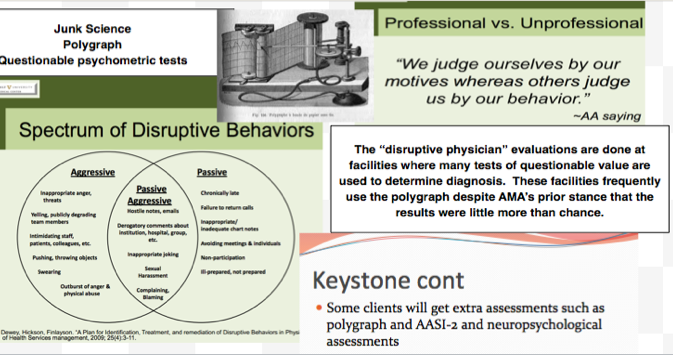
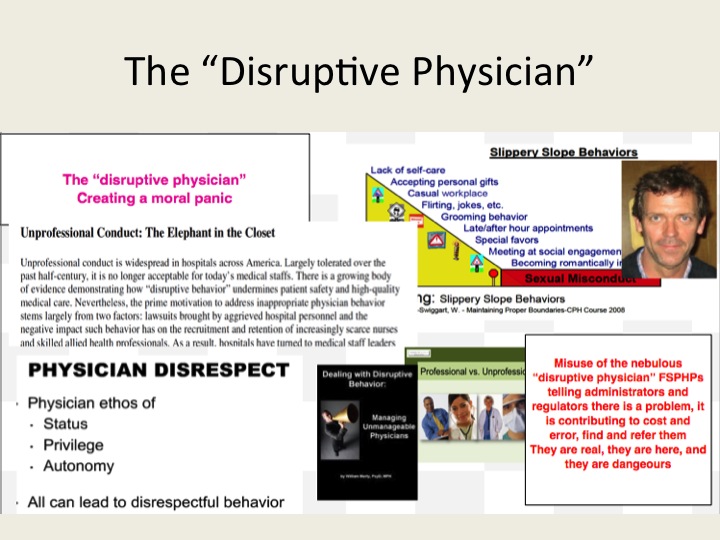
Behavioral manifestations included not answering pages on time, untimely or illegible chart notes, being late for meetings and questioning hospital authority. Disruptive physicians were blamed for everything—patient morbidity and mortality, increasing malpractice costs and decreased hospital revenue.
Using the nebulous “disruptive physician” label, anyone with a grudge or suspicious could accuse anyone of misbehavior, malice and mayhem.
Propaganda, threats, misinformation, guild assumed from the start, PHP oversight of disruptive physician persecution was standard.
During the state PHP “disruptive physician” with-hunts the legal notion of crimen exceptum (an exceptional and most dangerous crime) allowed for the suspension of normal rules of evidence to punish the guilty.
Because of the nature of the enemy the evidentiary bar was lowered and any witness, no matter what his credentials, could report a doctor to the state PHP.
Belief in the seriousness of the situation rationalized cruelty.
Professional experts used lie-detector tests (polygraphs), non-validated neuropsychological instruments, and non-FDA approved drug and alcohol tests to confirm the accusations. The accused often did not pass these tests due to “tailoring” the results to fit the PHPs wishes and often received positive biomarker tests due to the ubiquity of the chemicals tested for. Bananas, sauerkraut, bakers yeast, urinary tract infections and hand sanitizer were often the cause. False accusations, if exposed, were excused if they were a result of “zeal for the faith.”
The consequences of being branded a heretic by questioning the existence “disruptive physicians” essentially silenced any dissenting voices and the notion of crimen exceptum freed the consciences of those involved.
Sanctimony, feigned piety and hypocritical devoutness was used as justification. After all–Torture and torment are a small price to pay when it comes to protecting the public and saving souls.
Through the “disruptive physician” trials clerics, “addiction medicine” specialists, psychologists, neuropsychologists, commercial drug-testing labs, assessment and rehabilitation facilities and lawyers used their expertise as witnesses to increase their prestige. The “disruptive physician” developed into a means of economic profit. Some gained a lot of money from the “disruptive physician”. The accused doctor and his or her relatives paid out of pocket for those who worked the “disruptive physician” trials including those doing the testing, assessment and treatment.
“Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.” So too is hunting the “impaired,” “disruptive” and “aging” physician and the costs are usually paid by the accused.
Their property was lost to pay the revolving door of testing, assessment and treatment and those overseeing it raked in increasingly large sums of money as well as other reliable assets. A doctor accused could easily be ruined permanently.
In 1592 Father Cornelius Loos wrote:
“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.”
And in 2015 nothing has changed.
Context, characters and circumstances may differ but the mechanics do not.
The mosaic remains the same.
False constructs come to be regarded as irrefutable and the creation and chains of causation remain timeless

- Cunningham GM. Editorial: The Dreaded Task of Confronting Disruptive Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):6-7.
- Summer GL, Ford CV, Lightfood WM. The Disruptive Physician, I: The Alabama Physicians Recovery Network. Federation Bulletin. 1997;84(4):236-243.
- Bohigian GM, Bondurant R, Croughan J. The impaired and disruptive physician: the Missouri Physicians’ Health Program–an update (1995-2002). Journal of addictive diseases. 2005;24(1):13-23.
- Grenny J. Crucial conversations: the most potent force for eliminating disruptive behavior. Physician executive. Nov-Dec 2009;35(6):30-33.
- Huff DJ, Cline LE. Another reason to be on your best behavior: the Joint Commission’s new disruptive physician standard. Journal of the Medical Association of Georgia. 2009;98(2):17-18.
- Leiker M. Sentinel events, disruptive behavior, and medical staff codes of conduct. WMJ : official publication of the State Medical Society of Wisconsin. Sep 2009;108(6):333-334.



“The belief that there are such things as witches is so essential a part of the faith that obstinately to maintain the opposite opinion manifestly savors of heresy.”
So begins Malleus Maleficarum , a witch hunters manual published in 1486 that launched a new paradigm for all those concerned with the identification and extirpation of witches. Used as a judicial case-book the Malleus set forth definitions of witchcraft, rules of evidence, and the canonical procedures by which suspected witches were tortured and put to death. Written by Inquisitors for Inquisitor, the Malleus construct came to be regarded as irrefutable truth and contributed to the identification and execution of as many as 60,000 “witches”, predominantly women. The 29th and last edition was published in 1669.

Although there was a general belief in witches at the time theas published they were not regarded as evil or life threatening. Society did not fear them and Church and Political authority certainly did not feel the need to hunt them down. There were many scholars who publicly doubted the existence of witches at the time. That would soon change.

After being snubbed by secular and ecclesiastical authorities in his witch-hunting pursuits, the Dominican friar and German Inquisitor Heinrich Kramer told Pope Innocent VIII of a dangerous outbreak of witches that had occurred in the region. This diabolical conspiracy hell-bent on destroying humanity needed to be identified and destroyed for the public good, but church authorities were not cooperating.
On December 5th, 1484 Pope Innocent VIII issued the papal bull Summis Desiderantes affectibus giving full authority to proceed with “correcting, imprisoning, punishing, and chastising” such persons “according to their deserts,” and threatening to sanction or excommunicate those who hindered the pursuit.
 From the late 15th century through the early 17th century a confederacy of “authorities” calling themselves demonologists assisted in identifying witches. Shaping ecclesiastical orthodoxy they set the standards that cooperating political authorities could follow in criminalizing, persecuting and punishing heretics.
From the late 15th century through the early 17th century a confederacy of “authorities” calling themselves demonologists assisted in identifying witches. Shaping ecclesiastical orthodoxy they set the standards that cooperating political authorities could follow in criminalizing, persecuting and punishing heretics.
Behavioral manifestations included living alone, cultivating strange herb and saying hello to a neighbors cat.Witches were blamed for everything—plague, crop failure, and erectile dysfunction.
Using the nebulous “witch label” anyone with a grudge or suspicion could accuse anyone of witchcraft .
Propaganda, threats, misinformation, guilt assumed from the start.
 Physician oversight of witch persecution was standard.
Physician oversight of witch persecution was standard.
During the European witch-hunts the legal notion of crimen exceptum (an exceptional and most dangerous crime] allowed for the suspension of normal rules of evidence to punish the guilty.
Because of the nature of the enemy the evidentiary bar was lowered and any witness, no matter what his credentials, could testify against the accused.
Belief in the seriousness of the situation rationalized cruelty.

The Devil’s mark (Stigmata diaboli) was taken as the mark of a witch entailing close inspection.
Professional witch-prickers used needles, pins and bodkins to poke the skin with lack of bleeding confirming the accusation. The accused did not bleed due to retractable needles and sleight of hand. False accusations, if exposed, were excused if they were a result of “zeal for the faith.”
The consequences of being branded a heretic by questioning the existence of witches essentially silenced any dissenting voices and the notion of crimen exceptum freed the consciences of those involved.
Sanctimony, feigned piety and hypocritical devoutness was used as justification. After all–Torture and torment are a small price to pay when it comes to protecting the public and saving souls.
Through the witch trials clerics, doctors, and lawyers used their expertise as witnesses to increase their prestige. Witch hunts developed into a means of economic profit. Some gained a lot of money from the witch trials. The witch or her relatives paid for the salaries of those who worked the witch trials including judges, court officials, torturers, physicians, clergymen, scribes, guards, attendants. Even the people who made the stakes and scaffolds for executions gained from the conviction and death of each witch.
 “Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.”
“Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.”
The costs of a witch trial were usually paid for by the estate of the accused or their family.
Far from the conventional image of a penniless hag, a significant proportion of accused witches, especially in Germany, were wealthy and male.
Their property was seized to pay the clergymen, judges, physicians, torturers, guards, scribes, and laborers who raked in increasingly large sums of money as well as other reliable assets.
With a single member accused, a moderately wealthy family could be ruined permanently.
In 1592 Father Cornelius Loos wrote:
Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.

Context, characters and circumstances may differ but the mechanics do not.
The mosaic remains the same.
The Malleus shows how false constructs come to be regarded as irrefutable and the creation and chains of causation are timeless.