According to Erich Fromm rational authority is based on competence, experience, and mutual respect. Irrational authority is often disguised as benevolent paternalism and is designed to perpetuate or intensify conditions of inequality through the use or threat of force, deceptiveness, and secretiveness.
The Federation of State Physician Health Programs (FSPHP) has has operated as an unexamined authority for the past 25-years . They have pushed practice and policy unquestioned and without opposition that has gravely harmed individual doctors, the medical profession itself and the public at large. Everything they have done has been done to benefit themselves and their drug and alcohol assessment, testing and treatment affiliates in the provision of protections, power and profits.
Examining the specific practice and policy pushed reveals a body of false-claims making designed to facilitate the systemic use of coercion and threats, remove all due process protections and fundamental rights from physicians and prevent, block and eliminate the evidence. This practice and policy collective has created a culture of impunity, immunity and deference that is able to successfully conceal ethical violations and crimes. Uncovering their wrongdoing is a nearly impenetrable gauntlet. It is a system of institutional injustice that is undoubtedly a major contributor to the suicide epidemic in the profession. They have been able to conceal the truth, avoid investigation and prevent punishment for years by removing themselves from all accountability and outside inquiry. Direct and specific questioning appears to be their Achille’s heel as the recent spat of articles critical of these programs is showing just how much of an illegitimate authority they really are.
In her rebuttal to Pauline Anderson’s article “Physician Health Programs: More Harm Than Good?” FSPHP President Doris Gunderson dismissed the accusations of fraud and abuse in one fell swoop as “allegations rather than facts” and second hand anecdotes. Countering allegations of an absence of oversight and regulation she states:

“In fact, we operate under a microscope, answering to individual practitioners, medical boards, malpractice carriers, defense attorneys, state attorneys, medical societies, hospitals, medical schools and residency training programs. We are also accountable to patient safety entities and a Board of Directors.”
Untrue. Accountability demands both provision of information and justification for actions to outside entities capable of punishing misconduct. . What was done and why? No such entity exists and no pathway for appeal or grievance redressal exists either. Zero accountability. Ditto for the “PHP-approved” assessment and treatment centers. As cash only out-of-pocket facility they remove themselves from the prying eyes of insurers.
 The North Carolina PHP Audit found the past FSPHP President and NC PHP director Warren Pendergast could not identify the qualitative or quantitative indicators used for “approving” PHP-approved facilities. The best he could come up with is “reputation” and “word of mouth” yet state medical boards mandate evaluations of doctors at these facilities and specifically exclude non-“PHP-approved” facilities.This is enforced by the Federation of State Medical Boards Policy on Physician Impairment. Each state managed by the FSPHP utilizes the same dozen or so facilities and each state medical board mandates it under threat of disciplinary action. It is in fact a rigged game.
The North Carolina PHP Audit found the past FSPHP President and NC PHP director Warren Pendergast could not identify the qualitative or quantitative indicators used for “approving” PHP-approved facilities. The best he could come up with is “reputation” and “word of mouth” yet state medical boards mandate evaluations of doctors at these facilities and specifically exclude non-“PHP-approved” facilities.This is enforced by the Federation of State Medical Boards Policy on Physician Impairment. Each state managed by the FSPHP utilizes the same dozen or so facilities and each state medical board mandates it under threat of disciplinary action. It is in fact a rigged game.
Denying accusations of coercion Gunderson states in her rebuttal to Anderson’s article:
“The detractors of PHPs interviewed for the article maintain that PHPs are coercive. Yet the report fails to mention that PHPs have no authority to mandate treatment and monitoring, suspend or revoke licensure, or otherwise discipline physicians.”
 The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy. (ASAM Policy on Coordination Between Treatment Providers, Professionals Health Programs, and Regulatory Agencies).
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy. (ASAM Policy on Coordination Between Treatment Providers, Professionals Health Programs, and Regulatory Agencies).
Legitimate authority articulates ethical, evidence-based, or internally consistent arguments when challenged. Legitimate authority does not simply delegitimize one’s opponent and use logical fallacy and obfuscation to avoid addressing the substance of an argument. In her rebuttal Gunderson claims the NC Audit was favorable to them because no evidence of abuse was found. This is akin to a serial killer claiming victory because no bodies were found in his dungeon replete with torture devices and restraints. State auditor Beth Wood set this straight when she told the BMJ in Physician Health Programs Under Fire that the holes were big enough in the program “you could drive a truck through them” and it would be “difficult, if not impossible, to defend” oneself against an incorrect assessment” as no ability to “appeal a diagnosis or assessment” existed.
 “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
Multiple Barriers Removing Accountability at Multiple Levels
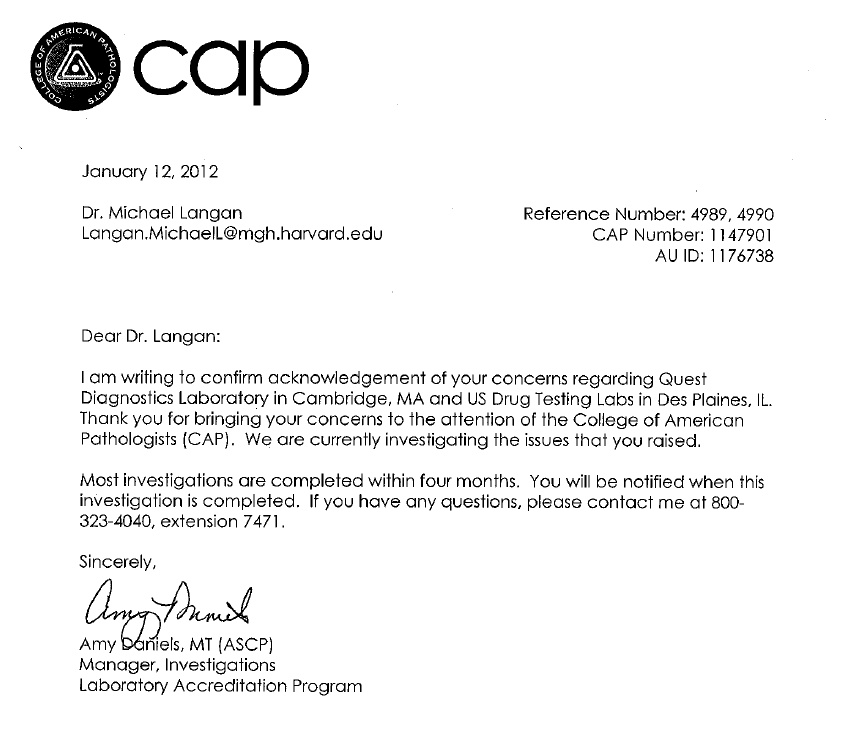
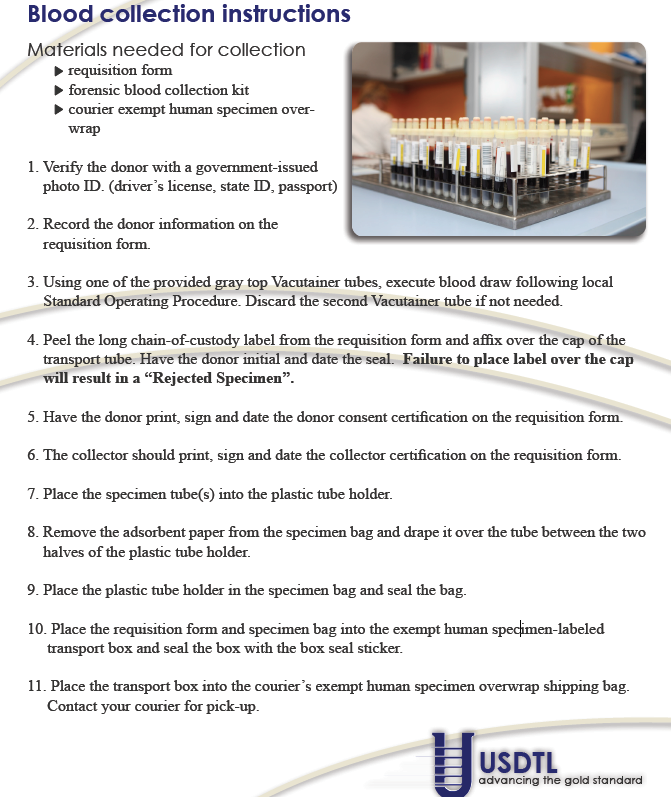
The inability to obtain one’s own medical records or lab reports is the first obstacle one must overcome. The second barrier is that even if documents are obtained there is no one to give them to. The third is the existence of “point people” who deflect, block and otherwise dismiss valid complaints. The only oversight provided to the involved labs is an an accreditation agency, the College of American Pathologists (CAP) They can investigate and correct but do not have the ability to sanction.
 Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
It is therefore critical it be recognized for what it shows and it is morally imperative that those involved be held to account as the documents illustrate clearly and undeniably a collusion between a state PHP and its drug testing lab to fabricate evidence. The corruption is top-down as it involves another former FSPHP President Luis Sanchez and the VP of Laboratory operations at USDTL Joseph Jones. As explicit and detailed as it is in revealing unequivocal black and white crimes it has been ignored by the usual channels.
Research on street criminals suggests the certainty of punishment has the strongest deterrent effect (basically will I be caught) and the more people think they will be arrested for a crime the less likely they are to commit it. Criminals weigh their actions against possible gains and consequences and the risk of consequences in this system have been essentially zero. Diagnosis rigging, coercion, threats and abuse are rampant because they have no fear of punishment. The Chairman of the commission that examined the causes of the 2008 financial collapse compared the relatively small fines paid by corporations to “someone who robs a 7-Eleven, takes $1,000 and being able to settle for $25 and no admission of wrongdoing.” He added,“Will they do it again? Absolutely, because it pays.” This is like someone who robs a 7-Eleven, takes $1,000 and never gets caught so he goes to the next 7-Eleven and takes $2000 then hits as many 7-Elevens as he can for as much as he can.
Multiple Crimes, Multiple Felonies and Egregious Misconduct. Fabrication, Falsification, Concealment and Perjured Evidence. Color-of-Law Abuse, Civil Rights Violations
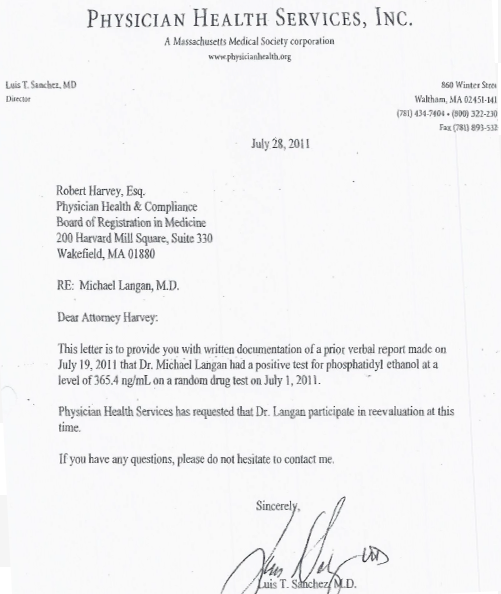
In June of 2011 I signed a patent-license agreement with a company to bring an epinephrine auto-injector to FDA approval within three years. It was recently mentioned in an NBC news article in the wake of Mylan’s Epipen price hike and the patent documents can be seen here and a slideshare overview here. This was successfully derailed the following month when I was asked by the state PHP to have an alcohol test. This was for no apparent reason. I have never been accused of having an alcohol problem and my work performance at MGH was reported as “impeccable.” There were no issues in any arena. The events are described in detail here, here, and here.
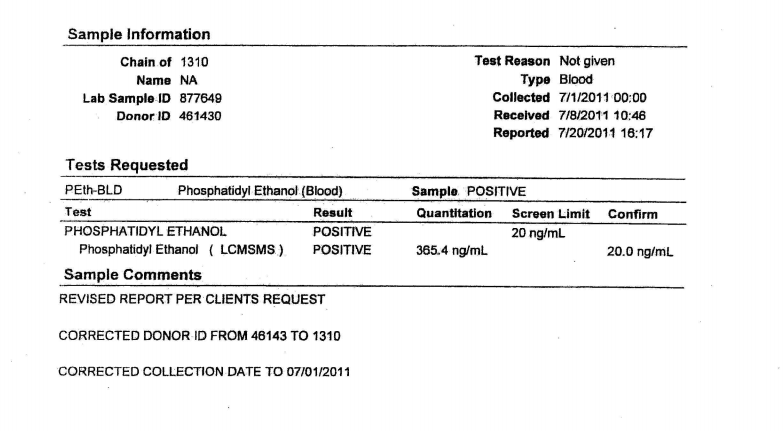
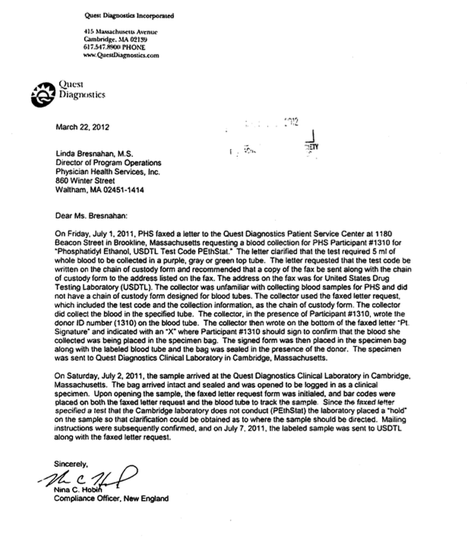
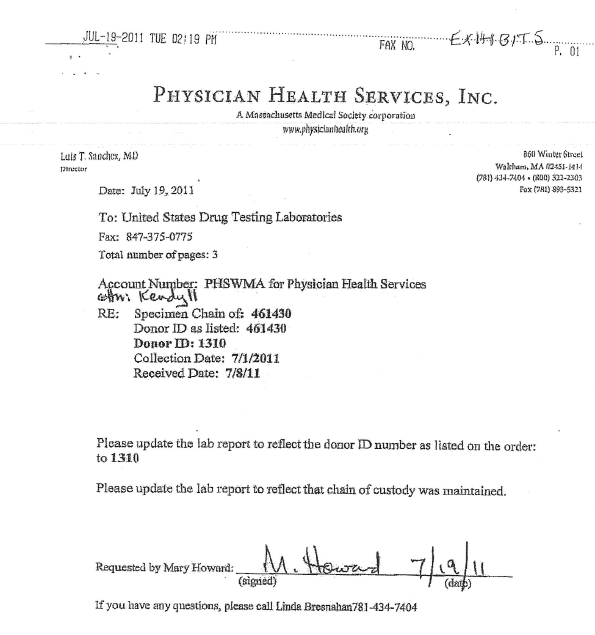
The blood test was reported positive to the medical board on July 19, 2011 as seen here: positive-peth-july-19-2011 I requested records but PHS refused but relented in December 2011 and I obtained the USDTL Litigation Packet which contained a faxed request from PHS to the lab requesting my unique identification number and a “chain-of-custody” be added to an already positive report See key docs here.:12:3:2011 Litigation Packet (Selected)
The records showed falsely created and fabricated evidence. Clear fraud. I filed a complaint with the College of American Pathologists CAPLetter. They investigated and forced USDTL to correct the test as reported in an October 4, 2012 letter from the lab to Sanchez. Instead of revealing the correction the two concealed the revision and reported “non-compliance” two weeks later and board took disciplinary action against my license. In December 2012 CAP contacted me to followup on the outcome of the revised test which I was unaware of. I informed them they did not tell me and confronted PHS but they claimed no knowledge of it.. On December 11, 2012 Sanchez reports to the board that he just found out that the test was revised but it had nothing to do with the disciplinary action taken by the board.. Sanchez and Jones deny there was any correction 67-days earlier and stand by their guns.
In August of 2014 I was able to obtain the complete USDTL documents under new HIPPA-Privacy Rule for labs which removed PHS approval. Full docs can be seen here: August 6, 2014 to Langan with health materials. The October 4, 2012 correction from USDTL to Sanchez contradicting Sanchez claim of not finding out about the correction until December is included.Note the language used in the Letter claiming Sanchez was informed of the revised test 67-days after he actually was.
Recently obtained documents under records reform act – Langan PDF copy They show documents entered as evidence date-stamped and entered into the administrative record after the hearings at which they were to be heard. Multiple others missing and never addressed. It is now clear that Stoller concealed all documents relating to PHS misconduct since December of 2011.
Specific and detailed evidence of criminal activity was provided to Board Attorney Deb Stoller over the course of more than five-years. This showed clear collusion between the state physician health program and one of their preferred national drug testing labs. It is important to recognize the gravity of what this means. I provided a state officer with evidence of crimes similar to Annie Dookhan–clear fabrication and collusion to fabricate evidence. She suppressed it. This is much much worse than Annie Dookhan as the lab is used by state physician health programs across the country and over the past five-years their have been multiple suicides of doctors who have allegedly been given fabricated drug and alcohol tests just like mine. Many of these doctors were given positive tests right before they were to complete a 5-year contract and this is a pattern that seems to be occurring as the rule rather than the exception. Facing five more years of abuse some doctors have chosen to end their lives rather than continue with the PHP.
Specific and detailed evidence of the fraud was given to Deb Stoller over the course of five-years and she did nothing about it to protect Sanchez. The impact of this is much greater and the consequences much more severe than what occurred with Dookhan. As The documents clearly showed felony crimes this is egregious and indefensible.
 What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones ( August 6, 2014 to Langan with health materials ) and told him of the severe consequences this was having for my family but he did not respond. Had it not been for the new HIPAA -Privacy rule I would never have obtained these documents and without the record reforms act I would never have obtained the evidence implicating Stoller ( Langan PDF copy )
What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones ( August 6, 2014 to Langan with health materials ) and told him of the severe consequences this was having for my family but he did not respond. Had it not been for the new HIPAA -Privacy rule I would never have obtained these documents and without the record reforms act I would never have obtained the evidence implicating Stoller ( Langan PDF copy )
 It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
 Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
The Board claims no crimes were committed because no one has been charged with any crimes. No, Dr. Sanchez has committed very serious crimes including multiple felonies. This can no longer be ignored. These crimes can be determined by the documentary evidence alone. They are self-evident.
To settle the matter once and for all I am offering over $25,000.00 in cool prizes to the first person who can disprove my claim that Dr. Sanchez committed multiple felonies. My claim is that by simply looking at the dates and documents multiple felonies are clear. They are not equivocal. The first person to disprove this assertion may collect each and every item pictured below. You can even write up a legally binding contract and I will sign it. There is something for everyone and if anyone has any questions about any of it feel free to ask.
To summarize, I can find multiple clear felonies in the documents that need no further inquiry. They are black letter law and involve fraud, concealment, perjury and other crimes. Policies and laws need to be enforced equally. The Board cannot play favorites and give allowances to its friends when it comes to criminal activity. Sanchez is licensed by the medical board just as I am and the  board’s position on the fraudulent practice of medicine is quite clear.
board’s position on the fraudulent practice of medicine is quite clear.
One felony would be demand the board address what is seen here. Multiple felonies make it inexcusable to ignore and if it is ignored it will be relentlessly addressed again and again and again. As it is so difficult to obtain evidence it is necessary that this be addressed with full measure as a precedent. People just like this are harming good doctors across the country and unless you are profiting from the drug and alcohol testing and treatment racket you should be disgusted at what is seen here. The fact that Sanchez pontificates on the behavior of others makes this particularly egregious. Moreover, Jones also tests newborns and other groups with these same tests. If he is this unethical who knows what amount of damage has occurred. Anyone of integrity and conscience should be outraged by what is seen here. As it is one of the clearest and most specific examples of laboratory fraud I am going to be asking for help getting this out–it should be used to show how this type of drug and alcohol testing can be abused.
Direct and specific questions deserve direct and specific answers. This will need to be addressed directly as it is not going away and neither am I. If cannot disprove fewer than three felonies than they need to be addressed. Suspect similar point-people in other agencies protecting them.
If multiple felonies were not committed then you would think at this very moment there should be people knocking on the door trying to get my attention so they can collect these prizes. I don’t hear anybody knocking, do you?
Prizes as Below



























































 Link to Medscape article by Pauline Anderson
Link to Medscape article by Pauline Anderson