


“Because I can Biotches! That’s right..because I can!”
He states that “Impaired doctors must first acknowledge their addiction and overcome their ‘terminal uniqueness’ before they can deal with a drug or alcohol problem.”
 This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.
This dicto simpliciter argument can, in fact, be refuted simply by pointing it out! Sadly, no one ever did so the ASAM front-group hasbeen able to establish this caricature of the arrogant paternalistic know it all needing 3 months or more of treatment as standard of care for our profession. They did this by getting medical boards and the FSMB to accept fantasy as fact by relying on board members tendency to accept expert evidence at face value–which they always do and that is a personality characteristic that I would argue is not dicto simpliciter.Physicians are unique only insofar as the unique elements required of the profession to become and be a physician such as going to medical school and completing the required board examinations.
Any and all doctors referred to a PHP for assessment will spend at least 3 months in treatment if the facility feels it is indicated. It is inevitable. No one has challenged a patently absurd generalization that has absolutely no evidence base or plausible scientific or medical explanation. Of course those sentenced to the 3 or more months have complained but by that time they are de-legitimized and stigmatized. No one to complain to. After all, these are just redeemed altruistic non-profit good guys protecting the public and helping colleagues forge a path to salvation!

Leslie Kane
June 17, 2014
Good Doctors Have Some Bad MomentsDoctors’ personalities have become a hot topic, not only because warmth and pleasantness count toward patient satisfaction, but also because positive patient interactions have a role in better outcomes.Physicians’ personalities are under the microscope as patients post reviews of doctors on numerous Websites. In some reviews, the word “arrogant” has shown up. But calling doctors arrogant is nothing new.Are there really so many arrogant doctors? No doubt, some physicians deserve the label, but it seems to be a stereotype that has blossomed and taken on its own life.”Arrogance among doctors is not the norm”, says Marion Stuart, PhD, co-author of The 15 Minute Hour: Therapeutic Talk in Primary Care, and Professor Emeritus in the Department of Family Medicine at UMDNJ-Robert Wood Johnson Medical School. “Someone who has done the hard work and has gone into medicine because they care about people, and are interested in helping peoples’ lives and making the world a better place, is not going to be arrogant.”So how did the arrogant doctor epithet arise?In the past, doctors were considered authorities who told compliant patients what to do and treated them with a paternalistic attitude. Some doctors may retain those behaviors today.Another possibility is overgeneralizing. A patient sees a doctor who has a difficult personality and assumes that the trait is more widespread within the profession than it really is.
Arrogance or Self-confidence?
“Arrogance is totally different from self-confidence,” says Dr. Stuart. “When you’re confident, that’s your assessment of your own competence. You have the experience and the wisdom, you know what you can do, and your confidence says that. It’s your relationship to yourself and your own expertise,” she says.
Arrogance is a different ballgame. “This has to do with your judging that other people are inferior,” she says. “It has more to do with not seeing other people as being up to your standards.”
Could the confidence that comes with being accomplished and successful make someone arrogant? Typically no, says Dr. Stuart. The trait of arrogance develops or resides within a person at a much earlier stage, arising from one of two paths:
“I am indeed better.” Someone who has always lived a privileged life, feels entitled to all of the finer things, or has always been looked up to may take it as a given that he or she is better than others. “People who had a sheltered, protected existence with no perception of what the real world is like for other people may consider themselves an elite group, entitled to feel superior,” says Dr. Stuart.
“I made it, so why can’t you?” By contrast, a person who was deprived as a child and worked very hard to pull himself up by the bootstraps may then look down on others who don’t have the same perseverance or initiative to take charge of their life and create similar success.
Doctors Are Harried and Pressured; Patients Are More Demanding
Some doctors have admitted that at times it’s hard to maintain their patience, and frustration triggers a snappish response. Throw into the mix the fact that doctors may have less time to see each patient and answer questions, and you have the ingredients for a negative interaction.
“I’ve had eight years of medical education and I’ve been trying to get my patient to make healthy lifestyle changes, and he comes in with a page ripped out of a tabloid, convinced that the information is right…there’s a limit to how much time I can spend ‘educating’ or convincing them that their ‘cure’ has no scientific basis,” one physician told me.
People have come to expect the stance of “the customer is always right” and get annoyed if doctors don’t accede to all of their requests. But because of new medical practice guidelines, a doctor may not readily give the patient the test or medication they ask for. “Now, with healthcare insurers and companies setting limits on doctors, many times the patient feels that the doctor is not so much on their side, and this could be perceived as arrogant,” says Dr. Stuart.
Is There an Outbreak of Rudeness?
Barry Silverman, MD, a cardiologist and coauthor with pediatrician Saul Adler, MD, of Your Doctors’ Manners Matter: Better Health Through Civility in the Doctor’s Office and in the Hospital, says, “While most doctors are appreciated and respected by their patients, there’s a general perception that professionalism has declined.
“Patients are often more informed, ask detailed questions, and demand a high level of service, while demands on the doctor’s time increase and reimbursements fall,” says Dr. Silverman. “What patients interpret as arrogance is many times a rushed and harried doctor, not an uncaring one. Medicine can be mentally and physically exhausting, but the bottom line is that the doctor must listen and communicate with the patient to deliver quality medical care.”
Still, remaining pleasant and calm is easier for some doctors than for others. There’s no uniform physician personality; many doctors have a natural “people person” inclination, while others are more stoic.
Are doctors expected to smile and be nice in every circumstance, no matter what?
“Professionalism is not about putting on a happy face or being someone you are not; it is about providing quality care for the patient,” says Dr. Adler. “Patients are more informed and have access to more information than ever before. Much of that information is incorrect and sometimes harmful. That means that part of the professional duty is to teach as well as treat.
“Patients understand that doctors have significant restraints on their time, and it is not unreasonable for doctors to use preprinted written materials, educational resources outside the doctor’s personal office, and honest and informative Websites,” says Dr. Adler. “However, under no circumstances should the doctor be rude or abrupt; a smile and kind, considerate behavior is always appropriate.”
It would be naive to say that there aren’t arrogant doctors. But there are far more doctors trying to do their best for patients and relate to them.
Medscape Business of Medicine © 2014 WebMD, LLC









 Accountability needs to be rooted in organizational purpose and public trust.
Accountability needs to be rooted in organizational purpose and public trust. ce of unchecked power. The only two factors that constrain corruption are moral virtue and deterrence.
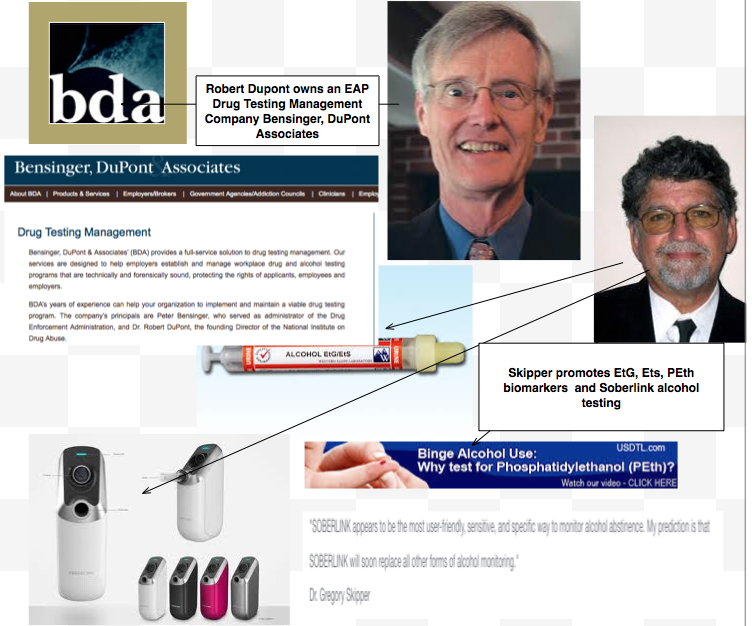
ce of unchecked power. The only two factors that constrain corruption are moral virtue and deterrence. arketed it as the PEthStat.
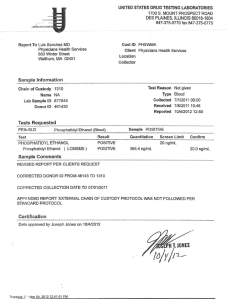
State Physician Health Programs are now using the EtG and adding the PEth to confirm alcohol ingestion. And just as they did with the EtG the claims of reliability are grand but without foundation.
All speculative A=B oversimplified thinking that ignores the myriad other factors involved. The science is empty if you remove the dregs of filler and puff. And the conflicts of interest are mind-boggling.
arketed it as the PEthStat.
State Physician Health Programs are now using the EtG and adding the PEth to confirm alcohol ingestion. And just as they did with the EtG the claims of reliability are grand but without foundation.
All speculative A=B oversimplified thinking that ignores the myriad other factors involved. The science is empty if you remove the dregs of filler and puff. And the conflicts of interest are mind-boggling.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}