“The surest way to work up a crusade in favor of some good cause is to promise people they will have a chance of maltreating someone. To be able to destroy with good conscience, to be able to behave badly and call your bad behavior ‘righteous indignation’—this is the height of psychological luxury, the most delicious of moral treats.” Aldous Huxley -Chrome Yellow 1921
A letter of agreement with the BORM, drafted at the behest of Physicians Health Service Inc., and signed by me 1/20/12 under threat of loss of my medical license specifically mandates participation “in a minimum of three 12-step meetings per week” and submit proof to PHS, “develop an “active 12-step sponsor relationship with someone who is not a healthcare professional.”
These requirements were made because I requested an independent evaluation at a non-biased non-12-step assessment center not affiliated with the ASAM. The choices PHS gave me were all 12-step facilities with Medical Directors who can be seen on this list. My request for an independent evaluation was justified as the MRO for PHS is on the same list. The same MRO who allowed PHS to misrepresent the positive EtG tests and fabricate a confirmatory positive PEth.
The PHS monitoring contract states that positive laboratory reports will be reported to the Board “with the exception of those medications that have been properly prescribed for a legitimate medical purpose and of which PHS has been informed in advance or of which PHS has approved” and that positive drug results are reportable to the Board “unless PHS is provided with advance verification of such medications.”
PHS claimed that I had been told to discontinue medications used to control and treat lifelong asthma. I had not. I provided the Board with multiple documents contradicting PHS claims.
An August 24, 2009 from Dr. Luis Sanchez, M.D. to the Board states:
“Dr. Langan has informed PHS that he is being prescribed two asthma inhalers. By FDA mandate, the inhaler manufacturers changed to ethyl alcohol propellants in January of this year. Dr. Langan has provided documentation of this medication. Physician Health Services (PHS) will be working with Dr. Langan to determine whether there are alternative options for asthma treatment that do not utilize ethanol as a propellant. Meanwhile, PHS has advised him to continue to use this medication as needed and as directed by his treatment providers.”
After discussing alternative options with my PHS associate director, John Knight, M.D., it was decided to continue them as prescribed. This decision was based on the history and severity of my asthma and the good control and treatment these mediations provided. As a child and young adult I had multiple emergency room visits and was hospitalized several times for asthma, but the medications had prevented any serious asthma attacks for the previous 10 years.
A letter dated January 1, 2010 from Louis Sanchez acknowledges continued use of the asthma inhalers. He writes: “Dr. Langan has provided PHS documentation of this medication. PHS has concluded that there was no evidence of relapse at this time.”
The documentary evidence shows that PHS acknowledged the prescribed medications, considered me compliant, and advised I continue to use them.
A February 10 2010 letter to my Chief, Dr. Kenneth Minaker, M.D. acknowledges the relationship between the medication and the alcohol biomarker Etg and affirms compliance with my PHS contract:

No EtG tests were done until June 20 and June 30, 2011. PHS reported these as “positive” by claiming I was told to discontinue my asthma medications. I provided the Board with multiple documents that contradict this claim and suggested that Dr. Knight be contacted to verify this was untrue. I also requested written documentation to support PHS claim. The Board ignored the contradictory documentation, did not contact John Knight, and neither PHS nor the Board could provide any documentation to support the claim that I was told to discontinue the medication. They still haven’t.
Reporting a positive test to the Board for a prescribed and acknowledged medication would be in violation of the PHS monitoring contract. Claiming the medications were discontinued allowed PHS to report these tests as true positives and also do a “confirmatory” test. The Etg was used as a stepping-stone to order a blood being used by Physician Health Programs to differentiate “incidental” exposure from drinking.
They were aware of the medications, aware they contained ethanol, and aware that they caused positive Etg levels but reported it anyway under the pretext that I was told to discontinue the medication. This misrepresentation was then “confirmed” by fraud.
There is no known cutoff level for Etg to differentiate incidental exposure from drinking. It should be noted that the use of ethanol containing metered dose inhalers is not “incidental” exposure but “direct” exposure and reporting them as positive violates all established protocols and guidelines. PHS then used forensic fraud for confirmation.
On July 1st, 2011, Dr. Gary Chinman of PHS informed me that I had positive EtG tests on June 20th, and June 30th, 2011. I was told to go to Quest Laboratories to obtain a confirmatory blood test. On July 19th, 2011 I was informed that the test was positive at a markedly high level of 365. The cutoff level of PEth is 20 and a level of 365 suggests heavy sustained alcohol use. Common sense would have dictated this to be erroneous at this point based on my appearance, work performance, and all collateral information.
I immediately requested evaluations from my PCP and the Chief of Addiction Medicine at MGH. They both did full evaluations (including speaking with my supervisors and colleagues, physical exams, and laboratory tests ) and wrote letters to the Board contradicting PHS claim. The Board was well aware that no other pretext existed to suggest alcohol use except for these tests. The Board ignored all outside information and continued to support PHS.
Suspecting the test was fabricated I requested the “litigation packet.” PHS initially refused. I persisted in obtaining the results and PHS finally agreed but threatened me with “unintended consequences.” I received the “litigation packet” in December of 2011 and it revealed fraud. A fax dated July 19, 2011 from PHS to USDTL requested that my ID # (1310) and a chain-of-custody be added to an already positive specimen 19 days after it was collected.
This evidence of fraud was provided to the Board in December of 2011. This was followed by a letter from the Chief of Toxicology at MGH opining that the positive test was an intentional and purposeful act by PHS to misrepresent an invalid test as valid.11:5:12-Dr. Flood Letter–Ignored by PHS:USDTL:BORM
The test has since been invalidated as a result of a complaint filed with the College of American Pathologists (CAP), an accrediting agency for the labs.
To sum this up I knew that the test was fabricated at the time and it was subsequently verified as fabricated ), I simply wanted a fair and objective evaluation from an assessment facility with no conflicts of interest. Marworth, Hazelden, or Bradford were the three choices given–all heavily indoctrinated ASAM facilities with close ties to the state Physician Health Programs.
Both PHS and the Board denied this request in violation of the Establishment Clause of the 1st Amendment. The Board’s Complaint Committee found I was in violation of my Letter of Agreement because I did not immediately enter into one of the three programs offered. On December 21st, 2011 the Board concurred that I was in violation of my LOA and chose to “resolve the matter” by extending my contract by two years and “fortifying certain provisions” including

BORM 12:22:2011
Interestingly, PHS had mandated thrice weekly 12-step meetings for a duration of three months. The Board took it upon themselves to extend it from three months to 2-years–an ultra vires act outside the scope and power of the Board and an obvious Establishment Clause violation. The Board also gave PHS carte blanche managerial prerogative to “submit proof of said participation” at the thrice weekly 12-step meetings. PHS chose names and telephone numbers of fellow attendees at anonymous meetings as the burden of proof! I informed the Board that obtaining unique identifiers such as names and telephone numbers to provide to a State substance abuse monitoring agency would be a tall order as “anonymous” is half its name. They did not take this into consideration. PHS also mandated under threat of my license that I could no longer use the asthma inhalers that had been controlling my asthma for the past decade.

PHS Letter 12:6:11-phone numbers:claims lab will support test
PHS Letter March 2012 Requesting Signatures
But the requirement that I humiliate myself by attending meetings at which I don’t belong and try to convince anonymous attendees to breach their anonymity wasn’t enough. I had to do it while wheezing. The Board forbade me from any of my asthma MDIs and essentially all of the propellants were replaced with ethanol by Federal mandate to protect the Ozone. Dr. Knight and I looked into alternatives previously and decided that due to the severity of my asthma and the control achieved by my current medications I would continue them as prescribed. As cold and exercise were two major contributors to asthma attacks I had to stop going to the gym and I had 19 major asthma attacks during that winter. My PCP documented the wheezing and shortness of breath at my checkups.
And to kick a wheezing fellow asking inappropriate requests at A.A. while he’s down, the Board extended PHS requirement of thrice weekly mandated AA meetings from 3 months to 2 years on their own accord. This is an inappropriate ultra vires act by the Board. It is outside the scope of their authority and an obvious Establishment Clause violation.
PHS had fun with the phone numbers. This is all documented in multiple e-mails such as these:


It soon became apparent that my attorney was doing nothing. At a meeting with PHS I told them that getting names and phone numbers at 12-step meetings was inappropriate and that Dr. Chinman was asking personal questions. My attorney turned to me and said “Well they have to ask questions. They need to make sure you’re not just paying somebody to say you were at a meeting? It then dawned on me that he had insisted on blaming the positive PEth test on my asthma inhalers and never even contacted the labs. He also refused to call Hazelden to verify that they had not made the request for phone numbers. I was told that this is the case with most PHPs. They refer you to a few attorneys who they know well and give a lot of business who will not bite the hand that feeds them. Another component of this rigged game.
On October 9th I received the following e-mail from my attorney:
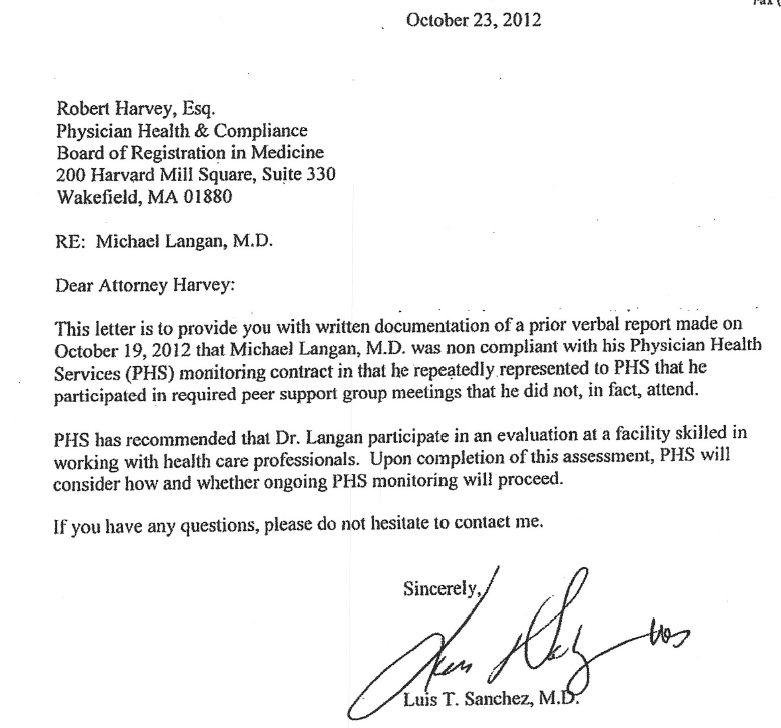
And on October 23, 2012 PHS formally reported my “noncompliance” with 12-step meetings to the Board

It has now become clear why this occurred at this time. Nevertheless the Board has outlined the decision making process from beginning to end right here in the February 6th, Board Order.
The modified Letter of Agreement specifically states that I must attend 3 “12-step” meetings per week and obtain a “sponsor.” No alternatives were offered and it is well established that mandated AA or 12-step by the State is in violation of the 1st Amendment. The Board then suspended me for allegedly not complying with the 12-step requirement. My suspension was, in fact, an Establishment Clause violation.
On April 8th, 2013, Attorney William Burgess of the Appignani Legal Center wrote a letter to PHS and The Board identifying the Establishment Clause violations and requested written response in how they would be remedied. This can be seen here:Secular_substance_abuse_treatment_options_for_MA_doctors
Board attorney Barbara replied on April 19th, 2013 with “the physician who you named in your letter currently has an open matter with the Board and, therefore it would be inappropriate for the Board members to receive your letter. Additionally, as you are not the attorney of record for the physician, I am unable to comment on the assertions you have made regarding the physician and his interaction with the Board and PHS.” The letter can be seen here: boardresponse5:1:13
This non-response is unacceptable. The Establishment Clause violations have been pointed out to the Board. Whether or not I have an open matter with the Board is irrelevant. Who identifies the violation is irrelevant as the law is clear on this matter.

The Proof PHS required was the name and phone number of a fellow attendee who they could call to verify my attendance. PHS mandated thrice weekly 12-step meetings per week for 3 months then once per week. The Board then again violated the Establishment Clause by taking it upon themselves to lengthen my sentence. and extended it from 3 months to 2 years.
A “12-step” program is a set of guiding or “spiritual principles” outlining a course of action for recovery from addiction, compulsion, or other behavioral problems. Originally proposed by Alcoholics Anonymous (AA) as a method of recovery from alcoholism.1 The Twelve Steps were first published in the book Alcoholics Anonymous: The Story of How More than One Hundred Men Have Recovered from Alcoholism in 1939.2 The 12-step ideology has been adopted by other groups such as Narcotics Anonymous and Overeaters Anonymous and that, except for the identified problem source, are carbon copies of one another

The proof of attendance at 12-step groups, as documented in the attached letters from PHS, mandated that I “provide PHS with the phone number of a consenting meeting participant” which is against the “suggested Alcoholics Anonymous (AA) policy regarding “cooperation with the courts.” The suggested AA policy is to sign “first name only to a card,” and even this “is not always accepted.”
According to Alcoholics Anonymous General Services3 “while most meetings will sign your court card, some will not. It is up to each individual group to decide. Since AA is not allied with the court system, AA is not required to do the courts work. We are not court employees. If a meeting chairperson or group member offers to sign your court card they will probably just sign their first name or initials. We are personally anonymous,” and “regardless of an A.A. member’s vocation, reporting on the “progress” of another A.A. member is strictly outside the scope of what A.A. does.”
The act of obtaining phone numbers at anonymous meetings not only violates the rights of the person being forced to do it but the rights of the other attendees. The basic tenet of AA is that it is for people who desire to be there and the spiritual foundation of is anonymity. Anonymity, by definition, refers to an individual’s personal identity, or personally identifiable information, being unknown. Signing a first name to a card provides anonymity. Providing a first name and a telephone number most assuredly does not as it is a unique identifier, not unlike a social security number or driver’s license number, and can easily be used to uniquely identify that person. Consequently, trolling for phone numbers to be given to an unfamiliar non-governmental state affiliated agency from anonymous members of a categorically anonymous group that considers anonymity as the spiritual core of its existence, presents a tall order.
Nevertheless, despite being half of its name, the BORM accepted the statement from PHS that obtaining names and phone numbers at 12-step meetings was accepted without question and I was not allowed to challenge or question the decision before the BORM.
Difficult as it was, I was able to provide them with phone numbers despite PHS’ attempts to make it as difficult as possible as documented in the attached e-mails and letters that include my concern that this Sisyphean task was merely designed as a failsafe to deem me noncompliant with the BORM should the need arise. It was.
In addition to coercion PHS continued to engage in threats, intimidation, and “torture” (an act committed by a person acting under the color of law specifically intended to inflict severe physical pain or suffering upon another person within his custody or physical control).
On 11/8/2012 the BORM found I was in violation of this agreement and referred the case to the full Board for sanction based on alleged “noncompliance” with the ordered attendance.
The First Amendment states in the “Establishment Clause that “Congress shall make no law respecting an establishment of religion.” Acts of direct coercion, threats backed by legal sanctions, are barred by the Establishment Clause.
Legally, Alcoholics Anonymous is established as a religious organization. And so is Narcotics Anonymous. This is well established and as far as United States courts are concerned AA and NA are, beyond a doubt, organizations that engage in religious activities and their meetings qualify as religious services.
Applying a standard three-part test to determine whether my constitutional rights have been violated
- Has the state acted?
- Was there coercion?
- Was the object of the coercion religious rather than secular?
As to point one the answer is clearly affirmative. PHS’ recommendations to the BORM were that I do the following:
- Participate in a minimum of (3) PHS approved 12 step meetings per week for the next 3 months including at least 1 physician meeting a week and document your participation with the signature of a consenting attendee and a phone number for the consenting attendee. After 3 months you must attend at least 1 PHS approved support meeting a week and 1 physician meeting a month
- Develop an active sponsor relationship and provide consent for this sponsor to confirm twice a year with PHS that he/she is your sponsor.
The Board wrote this up in the letter of agreement without offering any other options.
Coercion-point two—also is clearly present by force of law and threat of penalty. The elements of coercion are 1. A forced choice, 2. Threat of sanction, 3. Coercive ijntent.
The BORM states if I attempt to negotiate or dispute PHS’ recommendation I will be “immediately suspended.” Your money or your life.
Point three is now well established. (see notes below)
Mandating phone numbers as proof of attendance makes this particularly egregious as they inappropriately demanded I engage in a religious based program and violate the basic principles of the program (anonymity).
Moreover, the request for mandated 12-step attendance was not made out of “good faith” or beneficence. It was a retaliatory act designed to punish me because I questioned the results of a drug test that was done on July 1st, 2011 and reported as a confirmatory positive for alcohol use.
As a result of this test PHS requested an evaluation at a facility of their choosing. They were all -12-step facilities with medical directors they knew well. All ASAM/LMD and in 12-step recovery themselves
Because PHS had previously (2008) misrepresented the results of a drug test to justify sending me to an out of state facility for an evaluation where the facility fabricated neuropsychological testing to support “denial and cognitive impairment” resulting in forced inpatient rehabilitation I requested that the BORM allow an evaluation at an independent facility that did not have a referral relationship with PHS (and the inherent conflicts of interest that exist).4 The BORM would not consider the requests, said I had to go to one of the choices I was given, and added to more years to my contract because I had the audacity to request an alternative.
I also requested the laboratory (USDTL) “litigation packet.” Considered a legal document, this record is generated in any forensic (as opposed to clinical) laboratory -testing, and records the collection, shipping, handling, and testing of the sample. It is done to document that a drug test was done correctly on the person it was supposed to done on. It follows a specific protocol that involves strict chain of custody followed by MRO review.
PHS was resistant to my request for the “litigation packet,” but I eventually got it and, as Dr. Flood’s opinion letter shows, the test was fabricated. Chain of custody was nonexistent. The BORM refused to look at it. I filed a complaint with the College of American Pathologists (CAP) and an investigation was done which showed that the test was manipulated. Although the lab was sanctioned under threat of losing accreditation by CAP, as a non-governmental organization with no regulations and accountable to no one, PHS continued to support the validity of the test.
On December 4th, 2012 I got the following e-mail documenting that the laboratory issued an amended report mandated by CAP that showed the external chain of custody was not followed and thus making it an invalid test.
The amended report was issued on October 4th, 2012. I called Linda Bresnehan at PHS to ask for a copy of the amended report. She said she just got the report that day and issued a letter to the BORM December 11, 2012 stating that they just received the revision to the lab test but they “did not make a determination of relapse following the positive test,” they were not “aware of any action taken” by the BORM, and that they would continue to “disregard it.”
The BORM did not consider the logic that the very basis for my forced attendance at AA meetings and all of the other negative consequences thrown at me was this very test. Nor did they take into consideration the fact that the amended report was issued in October and the temporal relationship to them finding me out of compliance with AA meetings.
Instead, the BORM found me out of compliance with PHS which is essentially a lie (noncompliance) based upon a lie (saying that Hazelden recommended 3x per week AA meetings with phone numbers) based upon a lie (a fabricated test).
But the forensic fraud, “color of law” abuse, Civil rights violations, harassment, intimidation, and abuse qualifying as criminal harassment under 42 U.S.C. § 1983 -subject to a systematic scheme of harassment and intimidation Personal humiliation, embarrassment and mental distress) and arguably a violation of the Bill of Rights under cruel and unusual punishment are irrelevant. So too is the arrogant over-the-top bizarrely inappropriate request for phone numbers. Even without these factors entering the picture the Establishment Clause violations are clear. And the fact that they ignored the request to remedy a Civil rights violation is indefensibly unconscionable. They acted with malice, willfulness, and callous and reckless indifference to the safety and rights of my family and me. The “Right to be secure in one’s person” is an aspect of liberty protected by the due process clauses of both the Fifth and Fourteenth Amendments. And “Liberty” is Constitutionally protected by both the Fifth and Fourteenth Amendments, and also a protectable deprivation of due process. The liberty interest is violated and actionable by any conduct of persons acting under color of law that “shocks the conscience” (Massachusetts Civil Rights Act is M.G.L. c. 12 § 11I).

Notes:
The First Amendment states in the “Establishment Clause that “Congress shall make no law respecting an establishment of religion.” Acts of direct coercion—threats backed by legal sanctions—are barred by the Establishment Clause.
Three federal courts have held that coerced participation in 12-step programs like AA and NA violates the First Amendment. In Kerr v. Ferry, 95 F.3d 472 (7th Cir 1996), the Seventh Circuit held that requiring an inmate to attend NA meetings or risk suffering adverse effects for parole eligibility violated the Establishment Clause. The Second Circuit reached a similar conclusion in Warner v. Orange County Department of Probation, 115 F.3d 1068 (2d Cir. 1997), striking a probation condition requiring attendance at AA meetings.
In 2007 the Ninth Circuit Court of Appeals held that a parole officer’s demand that a convicted drug offender attend Narcotics Anonymous violated the First Amendment rights of the offender who claimed to be a Buddhist (Inouye v. Kemna, 504 F.3d 705 (9th Cir. 2007)).
Moreover, the case ruled that “any coercing authority” can be held individually, civilly liable for the First Amendment constitutional rights violation that they perpetrate on people unwillingly and involuntarily forced to go to 12-step programs and the offender was free to sue the parole officer for damages, even though state officials are often immune form such suits.
In both the Warner and Inouye cases, the courts found the law sufficiently clearly established to abrogate the officer’s qualified immunity. Qualified immunity shields government officials from liability for civil damages “insofar as their conduct does not violate clearly established statutory or constitutional rights of which a reasonable person would have known. (Harlow v. Fitzgerald 4567 U.S.C. 1983)
Warner and Inouye were able to go forward with lawsuits against their officers for damages for violation of their constitutional rights under 42 U.S.C. 1983. (Civil action for deprivation of rights). Numerous federal and district courts and state supreme courts have reached the same conclusion.
What this means is that you can sue a judge, a prison warden, a parole officer, a “counselor, a medical board member, or anyone else in a position of authority who forces you to go to AA meetings.
In cases like this the courts found that the government had forced the person to attend AA or NA. In other cases, where state of local officials simply made participation in AA one option for substance abusers, courts have no found any Establishment Clause violation.
[29] “For the government to coerce someone to participate in religious activities strikes at the core of the Establishment Clause of the First Amendment, whatever else the Clause may bar.” Inouye v. Kemna, 504 F.3d 705, 712 (9th Cir. 2007). The Ninth Circuit articulated the following test in Inouye v. Kemna “with regard to determining whether [Plaintiff] was [subject to] governmental coercion of religious activity . . . : ‘first, has the state acted; second, does the action amount to coercion; and third, is the object of the coercion religious rather than secular?’” Id. at 713. “First, [Crofoot] acted in his official state capacity as a parole officer to order [Plaintiff into a 12-step program that contained religious components]. That the state did not run the program itself is ‘of no moment.’” Id. (quoting Kerr v. Farrey, 95 F.3d 472, 479 (7th Cir. 1996)). It is undisputed that Crofoot, Wilding, and Jallins were acting in their official state capacities when they required Plaintiff to participate in the 12-step drug treatment program as a condition of his parole, and subsequently removed and incarcerated him for not participating in the program.
[30] Further, the Parole Defendants’ “action was clearly coercive: [Plaintiff] could be imprisoned if he did not attend and he was, in fact, ultimately returned to prison in part because of his refusal to participate in the program.” Inouye, 504 F.3d at 713 (emphasis added). The Parole Defendants argue Plaintiff was returned to prison because he was “disruptive” in the program. This argument rings hollow in light of the undisputed facts showing Plaintiff was only “disruptive” in the program “‘in a congenial way’” and “was ‘sort of passive aggressive.’” (Partial Mot. SUF ¶¶ 12, 13.) It is also undisputed that Plaintiff communicated his objection to participation in the Empire program and that Crofoot told Plaintiff he “should continue to participate in the Empire Program or he would be returned to prison.” (Id. ¶ 10.) It is further undisputed that Crofoot and Wilding concluded that “the right thing to do” was to refer Plaintiff to the Board of Parole Hearings “on a parole violation for failing to participate in the BPH-ordered program.” (Id. ¶ 15.) It is also undisputed that Deputy Commissioner Jallins authorized Plaintiff to be returned to prison because of Plaintiff’s failure to participate in the program. (Id. ¶¶ 18-19, 24.)
[31] “The final element requires somewhat more discussion.” Kerr, 95 F.3d at 479. It is undisputed that “Empire used a 12-step program that included references to God and a ‘higher power.’” (Partial Mot. SUF ¶ 3.) Further, Plaintiff’s following averments in his declaration have not been controverted:
[32] Shortly after arriving at Empire, I discovered that Empire used a “12-step” recovery program based [on] the principles of Alcoholics Anonymous (“AA”) and Narcotics Anonymous (“NA”), which contains religious components. Among other features, the “12-step” method used by Empire made references to God, involved acknowledgment of a “higher power,” and included prayer. [¶] I am an atheist, and was one in 2007. The substantial religious components to the “12-step” program administered by Empire conflicted with my beliefs. Prior to my release on parole, I had notified correctional authorities of my Atheism, and requested placement in a treatment facility that did not contain religious components.
[33] (Hazle Decl. ¶¶ 2, 3.) The Parole Defendants do not dispute that the Empire’s 12-step program contained religious components. “As such, on this summary judgment record and given the lack of dispute between the parties in question, . . . the third prong of [Plaintiff’s] Establishment Clause test has been met as well.” Inouye, 504 F.3d at 713-14. Therefore, “the program runs afoul of the prohibition against the state’s favoring religion in general over non-religion,” because of the program’s use of a religious concept of a Higher Power through references to God and prayer. Kerr, 95 F.3d at 480. Accordingly, Plaintiff’s partial motion for summary judgment against the Parole Defendants is granted.
[34] B. Plaintiff and Westcare’s cross motions for summary judgment on Plaintiff’s Establishment Clause claim
It is beyond dispute that, at a minimum, the Constitution guarantees that government may not coerce anyone to support or participate in a religion or its exercise (Lee v Weisman 505 U.S)
Legally, Alcoholics Anonymous is established as a religious organization. And so is Narcotics Anonymous. This is well established and as far as United States courts are concerned AA and NA are, beyond a doubt, organizations that engage in religious activities and their meetings qualify as religious services.
Applying a standard three-part test to determine whether my constitutional rights have been violate
- Has the state acted?
- Was there coercion?
- Was the object of the coercion religious rather than secular?
As to point one the answer is clearly affirmative. PHS’ recommendations following my evaluation at Hazelden (See PHS letter dated 10/27/2011) include:
- Participate in a minimum of (3) PHS approved 12 step meetings per week for the next 3 months including at least 1 physician meeting a week and document your participation with the signature of a consenting attendee and a phone number for the consenting attendee. After 3 months you must attend at least 1 PHS approved support meeting a week and 1 physician meeting a month
- Develop an active sponsor relationship and provide consent for this sponsor to confirm twice a year with PHS that he/she is your sponsor.
Coercion-point two—also is clearly present by force of law and threat of penalty. The elements of coercion are 1. A forced choice, 2. Threat of sanction, 3. Coercive intent.
Motion to Take Judicial Notice of Adjudicative Facts Pertaining to Violation of the Establishment Clause of the First Amendment
Motion to Take Judicial Notice of Adjudicative Facts
Motion to Take Judicial Notice of Law
BORM 11:8:2012 12:4:12-BORM Letter 12:21:11-BORM Board Order 12:22:11-BORM Violation LOA 12:27:2011-BORM LOA American Humanist Letter to BORM boardresponse5:1:13 BORM 12:22:2011 BORM Agreement Emergency Petition to Return to Practice.011013 letter re secular substance abuse treatment options for MA doctors (reply to PHS) v2-1 Liebert Letter to BORM 11:14:2011– Ltr JLH to Harvey.122812.01 Secular_substance_abuse_treatment_options_for_MA_doctors EMAILSLIEBERT