
The laboratory developed test (LDT) pathway does not require proof of test validity, that the test is actually testing for what it claims to be testing, and with no FDA oversight a lab can claim any validity it wants in marketing a test. There is no accountability.
Proponents of regulation argue that this lack of oversight is a direct threat to patient safety and the status quo represents the best interests of the companies selling and profiting unregulated tests. Opponents of regulation argue that requiring oversight is a direct threat to patient safety and represents the best interests of those paying for these tests (insurers) who will restrict what tests are covered based on saving money.
This debate focused on the reliability and validity of a number of clinical tests currently marketed with unverified claims of accuracy such as those used for prenatal screening and Lyme disease. The debate has become complex and, as a result the 2014 FDA issued draft guidance has been delayed. Moving forward it has been suggested that risk/benefit analysis be done to stratify clinical utility and risk of harm. This requires asking two questions.
1. What is the clinical utility of the test (based on pharmacology, quality of research, standards of care, expert guidelines and any applicable evidence-base)
2. What is the risk of harm if a disease is misdiagnosed as a false-positive or false-negative?
Obviously tests for serious and life-threatening disease pose the greatest danger to public health. Under this risk stratification strategy each test should be addressed based on the potential benefits and potential risks of potentially erroneous tests.
As noted on the the U.S Food and Drug Administration’s official blog:
“Health care providers and their patients expect that laboratory tests used in clinical management of patients should be consistent and of high quality.”
This necessitates applying the same standards of review to each and every test. It precludes exception. Previous draft guidance specifically excluded tests for alcohol and substance use. “Forensic” LDTs were notably absent from these discussions simply stated:
“At this time, FDA will continue to defer oversight of the use of these tests in the forensics (law enforcement) setting to the existing system of legal controls, such as the rules of evidence in judicial proceedings and other protections afforded through the judicial process.”
Why would expectations of consistency and high quality not apply to the a vast number of Laboratory Developed Tests tests used for “forensic” drug and alcohol testing. Don’t those being tested for alcohol and drugs deserve the same high-quality testing as those being tested for prenatal screening or Lyme disease? Does substance use or the mere accusation of substance use allow suspension of quality control standards of laboratory tests? What is the rationale for this disparity in thought? In truth this entire class of tests was removed from consideration before it was even on the table because powerful special interests groups such as the drug and alcohol testing industry association prevented them from ever even being on the table. Their argument was essentially how dare you interfere with our protection of the public. How dare you question our efforts at combatting the opioid epidemic. How dare you interfere with our war on drugs.
Quality practices for lab tests should be the product of the very same variables. The standards should be uniform and universally applicable. Intention should not be a variable and who is being tested should clearly not be in the equation. Putting these variables into this equation not only opens the door for injustice and unfairness but lays a red carpet for fraud and abuse. Regulation and oversight based on benefit/risk stratification needs to address every individual test in any class of tests. There is no plausible rationale for excluding an entire class of tests that should clearly be at the top of the list in terms of potential for harm based on any critical review of the published literature as well as common sense.
1. The clinical utility of these tests is very low. Many of these tests were introduced with not just low evidence-base but no evidence base. They have been shown to have very low reliability and unknown validity. The financial conflicts-of-interest linking those profiting from these tests with the “research” supporting them is easily uncovered. No real evidence base exists to support their use. The potential for error is high.
2. The risk of potential harm from erroneous tests is extremely high. The consequences of a mistakenly positive test can be grave, far reaching and even permanent. This is self-evident.
It is time to get these tests back on the table. This delay provides a window of opportunity to do so. If you do not think this will impact you then read the documents below. They are currently lobbying to introduce these tests everywhere including random drug testing in schools. Any positive test will require assessment and treatment of the student and any resistance will result in consequences (inability to participate in sports, loss of academic scholarships, not being able to be in the school band). This is what they call “contingency management” and your opinion on the fairness or unfairness of this is irrelevant. They do not need your permission to introduce these tests. The only groups they need to convince to implement this type of testing in schools are the regulatory and administrative boards involved.
- Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug testing: The plan to Introduce Laboratory Developed Tests into Mainstream Healthcare
- The Need for Regulatory Oversight of Laboratory Developed Tests (LDTs) in Drug and Alcohol Testing
- An Open Letter to Senator Elizabeth Warren Regarding Laboratory Developed Tests, Physician Health Programs and Institutional Injustice
FDA Delays Finalization of Lab-Developed Test Draft GuidancePosted 18 November 2016
By Zachary Brennan

The US Food and Drug Administration (FDA) on Friday said it will wait for the new administration and halt the finalization of guidance that would have changed the way lab-developed tests (LDTs) are regulated.
Tara Goodin, press officer for FDA told Focus: “FDA believes that patients and health care providers need accurate, reliable, and clinically valid tests to make good health care decisions—inaccurate or false test results can harm individual patients. We have been working to develop a new oversight policy for laboratory developed tests, one that balances patient protection with continued access and innovation, and realize just how important it is that we continue to work with stakeholders, our new Administration, and Congress to get our approach right. We plan to outline our view of an appropriate risk-based approach in the near future. It is our hope that such an approach will help guide continued discussions.”
Roger Klein, chair of the professional relations committee at the Association for Molecular Pathology, told Focus: “FDA’s decision to delay release of a final LDT guidance is in the best interest of patients and providers, and supports further advancement in molecular pathology testing. We look forward to working with the FDA as we find ways to continue to improve the already high-quality testing that we provide to patients.”
The American Clinical Laboratory Association also praised the move, with president Alen Mertz calling the decision “a victory for diagnostic innovation and most importantly, patients.”
Background
LDTs have historically been regulated by the Centers for Medicare & Medicaid Services under the Clinical Laboratory Improvement Amendments, but in 2014, FDA issued draft guidance saying it would regulate LDTs more like in vitro diagnostics (IVDs).
“Initially, laboratories manufactured LDTs that were generally relatively simple, well-understood pathology tests or that diagnosed rare diseases and conditions that were intended to be used by physicians and pathologists within a single institution in which both were actively part of patient care,” FDA explained in a 2010 meeting notice. “These tests were ordinarily either well-characterized, low-risk diagnostics or for rare diseases for which adequate validation would not be feasible and the tests were being used to serve the needs of the local patient population.”
But in recent years, FDA has noticed LDTs becoming increasingly complex and in some cases nearly indistinguishable from their FDA-cleared devices. Of particular concern to FDA is that many LDTs play critical roles in clinical decision-making in the context of personalized medicine (e.g. genetic testing), which it said raises the risk of incorrect or missed diagnoses, resulting in untimely or improper treatment.
Last November, speaking at a House Energy & Commerce Committee hearing, Jeffrey Shuren, director of FDA’s Center for Devices and Radiological Health (CDRH), defended the agency’s plan to regulate LDTs, saying, “Getting the right treatment to the right patient at the right time depends on having accurate, reliable and clinically validated tests.”
Some members also argued against FDA increasing its oversight of LDTs. Rep. Michael Burgess (R-TX) said FDA’s proposal would “stifle” innovation, saying it is “crucial that we do not slow innovation or create unnecessary regulatory hurdles … requiring premarket review by the FDA will impose new and arguably unnecessary requirements and costs on clinical laboratories, hospitals and doctors.”
Other proposals have suggested dividing oversight of LDTs between FDA and CMS based on the type of test. Shuren rejected this approach, saying “such a system is going to lead to inefficiencies. It’s going to lead to inconsistent standards treating the same test differently depending upon who makes the test … if we’re going to assure that tests work we need one unified system.”
And unlike traditional IVDs, LDTs are developed and used within a single laboratory. According to FDA, these tests historically were “relatively simple tests generally confined to local labs, and often used for rare conditions.”
A draft bill floated ahead of that meeting also indicated what these regulations under FDA might look like moving forward.
The 185-page draft called for the creation of a new Center for In Vitro Clinical Tests within FDA, which would be tasked with classifying in vitro clinical tests as high-risk (if an inaccurate test result would cause serious harm, or death, to the patient), moderate-risk (if an inaccurate result for the intended use would cause non-life-threatening injury) and low-risk (meaning an inaccurate result would cause minimal or no harm, immediately reversible harm, or no patient disability).
The bill also sought to establish advisory panels to review and consider the classification of each LDT.
Share this article:
Categories: In vitro diagnostics, Government affairs, News, US, CDRH
Tags: LDTs, lab-developed tests, in vitro diagnostics

—There is no place in science for consensus or opinion, only evidence.-Claude Bernard
Dear Senator Warren,
Thank you for your reply regarding laboratory developed tests (LDTs) and the need for regulatory oversight. As you mention, LDTs are developed without FDA approval—a pathway in which is not even necessary to prove validity of a test (that it is actually testing what it claims to be testing for) to bring it to market. With no FDA oversight or regulation a commercial lab can claim any validity they want in marketing these tests. The regulation debate has focused on the reliability and validity of a number of clinical tests marketed with unverified claims of accuracy such as prenatal screening and Lyme disease and this lack of oversight is a direct threat to patient safety.
I am sure you would agree with me that the importance of tests diagnostic accuracy is directly proportional to that tests potential to cause patient harm if reported inaccurately.
Sensitivity and specificity are important components of any diagnostic test because there are consequences associated with both false-positive and false negative results.
A test falsely indicating the absence of a condition in someone who truly has it can delay or prevent needed treatment wile a test falsely indicating the presence of a condition in someone who does not truly have it can result in unnecessary testing and treatment.
Incorrect treatment and false labeling of patients can also occur. Therefore diagnostic accuracy is paramount if a test is being used as the basis for further tests and treatment. Any test being used as a basis for further tests or treatment needs to be accurate. It needs to be reliable and valid. Moreover, if the consequences of a test can result in significant patient harm (such as unneeded chemotherapy) it needs to be either 100% accurate or be combined with other tests to confirm the true diagnosis.
“Forensic” vs. “Clinical” Laboratory Testing
“Forensic” testing differs from “clinical” testing because of the consequences and the process is tightly controlled because false-positive results are unacceptable as the consequences can be grave, far-reaching and even permanent.
Forensic testing demands special handling and safeguards to protect the donor such as validated tests, certified labs, strict chain-of-custody procedures and MRO (Medical Review Officer) review. These safeguards of quality control assure the validity and integrity of the specimen. The LDT pathway was not designed for forensic tests.
Forensic Laboratory Developed Tests (LDTs)
Paradoxically, laboratory developed tests with the potential to cause life-changing and possibly irreparable harm have been absent from the regulatory debate; LDT drug and alcohol tests used for “forensic” monitoring purposes.
A panoply of tests using urine, blood, hair, fingernails breath and saliva have been developed and brought to market since 2003 when the first one was introduced by Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, who “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.” 1
Developed as an LDT, Skipper and NMS then claimed the alcohol biomarker (which was discovered in the 1950s) “appeared to be 100 percent specific” in detecting covert use of alcohol based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male. 2 With this “evidence-base” and a not yet published paper in the pipeline,3 Skipper then pitched the test to the Federation of State Medical Boards (FSMB) as an accurate and reliable tool detect covert alcohol use in health care professionals.
Policy Entrepreneurship
In “Agendas, Alternatives, and Public Policies,”4 John W. Kingdon describes the problem, policy and political streams involved in public policy making. When these three streams come together a specific problem becomes important on the agenda, policies matching the problem get attention, and then policy change becomes possible.
Kingdon also describes “policy entrepreneurs’ who use their knowledge of the process to further their own policy ends. They ‘lie in wait… with their solutions at hand, waiting for problems to float by to which they can attach their solutions, waiting for a development in the political stream they can use to their advantage.”4
And due to a perfect confluence of streams ( Institute of Medicine report that 44,000 people die each year due to medical error,5 media reports of “impaired physicians,” the the war-on-drugs, etc.) the FSMB was swayed into accepting not just the validity but the necessity of using an alcohol biomarker of unknown reliability and validity on doctors referred to or monitored by state Physician Health Programs (PHPs) .
As the national organization that gives guidance to state medical boards through public policy development and recommendations, the individual state medical boards adopted use of the test without critical appraisal and no meaningful opposition.
Shortly after its founding in 1912, the FSMB began publishing a journal called the Quarterly of the Federation of State Boards of the United States. Now known as the Journal of Medical Regulation, the publication has archived all issues with full articles dating back to 1967 and, as the official journal of the national organization involved in medical licensing and regulation this facilitates an unskewed and impartial examination of how and when specific issues and problems were presented and who presented them and, in doing so, the “policy entrepreneurship” Kingdon describes can be seen quite clearly. For example a 1995 issue containing articles written by the program directors of PHPs in 8 different states contains an FSMB editorial acknowledging the reported 90% success rate claimed of these programs (in part attributed to the 90-day inpatient treatment programs) that concludes:
“Cooperation and communication between the medical boards and the physician health programs must occur in an effort to protect the public while assisting impaired physicians in their recovery.” 6
No one bothered to examine the methodology of these reports to discern the validity of the claims and it is this acceptance of faith without objective assessment that has allowed the passage of flawed public policy in medical regulation.
Nowhere is “policy entrepreneurship” more glaringly displayed as it is in a 2004 issue promoting the use of EtG in monitoring doctors as under the same cover is an article identifying both the need7 for such a test and an article providing the solution.8
“Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs,” a survey of state Physician Health Programs (PHPs) concludes that “surreptitious alcohol use” is a significant concern” for PHPs, there is no current “best method” for detection, but a promising new test with “exceptional specificity (100 percent) and sensitivity” in detecting small amounts of alcohol for up to 18 hours has recently become available.7
This same issue contains an article authored by Skipper about a new marker “not detectable unless alcohol has been consumed” recently introduced in the United States and now commercially available.”8
Notably absent from both of these articles is Skipper’s role in the commercial availability of the test. This conflict-of-interest is nowhere mentioned in this display of “creating a market then filling it.”
This “regulatory sanctification” of the test implied its tacit approval by the medical profession (i.e. “if they are using it on doctors it must be valid”) and facilitated its marketing to other monitoring agencies (nurses, airline pilots) as well as Courts and Probation Departments where those doing the monitoring had absolute power while those being monitored had no voice.
Bent Science
In Bending Science: How Special Interests Corrupt Public Health Research9, Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using carefully crafted distorted or “bent” science to influence legal, regulatory and public health policy. The authors describe how those making these decisions often assume the information that reaches them has been sufficiently vetted by the scientific community as it flows through a pipeline of rigorous peer-review and professional oversight and that the final product that exits the pipeline is unbiased and produced in accordance with the norms and procedures of science.
McGarity and Wagner note the serious and sometimes horrific consequences of bent science and provide examples involving Tobacco and Big Pharma . The authors call for:
“..immediate action to reduce the role that bent science plays in regulatory and judicial decision making” and the need for the scientific community to be involved in “designing and implementing reform.”
“Shedding even a little light on how advocates bend policy -relevant science could go a long way toward remedying these problems. Indeed, precisely because the advocates have overtaken the law in this area, heightened attention to the social costs of bending science could itself precipitate significant change.”
In the case of EtG this shedding of light is not very hard as no “carefully crafted” studies bending science were used to sway opinion. None existed. The only items in the pipeline were directly related to Skipper. If anyone dare to look, the Emperor has no clothes.
Lack of Answerability and Accountability
There are difficulties in challenging bent science including a general lack of recognition of the problem and an absence of counter-studies to oppose deliberately manufactured ends-oriented research. This has proven true with the myriad LDTs introduced into the marketplace as no counter-forces or competing economic interests producing counter-studies exist.
Multiple lawsuits, including a class-action, have been decided in favor of the labs who have taken a stand-your-ground approach supported by a body of industry-related “research” they or their affiliates produced to support the validity and reliability of the tests.
Those affected by these tests either have no power or have had their power removed. Most do not have the resources to mount a defense let alone produce counter-studies questioning the reliability and validity of the tests.
Most employee drug testing follows Department of Health and Human Services (DHHS) guidelines using FDA-approved tests that have specific cutoff levels defining a positive-result in an effort to eliminate false-positive results.10 Procedural safeguards are in place in these programs to protect the donor. Forensic testing programs using LDTs provide no such safeguards as the testing is unregulated and there is no oversight from outside actors.
Unlike clinical LDTs “forensic” LDTs are even exempt from CLIA oversight. The only avenue for complaint is through the College of American Pathologists (CAP) and, as an accrediting agency, they can only address problems by ensuring compliance with CAP guidelines. If an investigation concludes lab error or misconduct CAP can mandate the lab correct the test result and come into compliance with their guidelines under threat of loss of accreditation but no other consequences exist. Accountability has been removed yet the consequences to those harmed by these are significant and without remedy.
State Physician Health Programs
As is the case with the LDTs they introduced, Physician Health Programs have no oversight or regulation. A 2013 Audit of the North Carolina PHP 11 prompted by complaints from doctors and performed by State Auditor Beth Woods found absolutely no oversight of the program by either the state medical board or medical society and that “abuse could occur without being detected.”
The Audit also found that doctors were predominantly referred to the same “PHP-approved” out-of-state facilities to which they in part attribute their high success rates in treatment. Interestingly the PHP could not identify what quality indicators or quantitative measurements were used by the PHP to “approve” the “PHP-approved” facilities.
In January of 2015 a Federal class action lawsuit was filed in the Eastern District of Michigan against the state PHP program and found health care providers were subject to the same referral system using these out-of-state facilities. The suit alleges constitutional violations related to the forced medical treatment of health care professionals and the “callous and reckless termination of professional licenses without due process.” 12
As with North Carolina, the Michigan PHP will be unable to provide what quality indicators and quantitative measurements are being used to “qualify” and “approve these facilities. None exist. The sole indicators for approving these assessment centers are ideological and economic. In fact, the medical directors of most, if not all, of these facilities can be seen on this list of “like-minded docs.”
Institutional Injustice
You once said “People feel like the system is rigged against them. And here’s the painful part: they’re right. The system is rigged.”
So too is this system.
As the Michigan lawsuit notes: “Unfortunately, a once well-meaning program has turned into a highly punitive and involuntary program where health professionals are forced into extensive and unnecessary substance abuse/dependence treatment under the threat of the arbitrary application of pre-hearing deprivations.”
This has become the rule not the exception. The Federation of State Physician Health Programs (FSPHP), the same group to which Dr. Skipper belongs, has systematically taken over these programs state by state by removing competent and caring doctors not agreeing with the groupthink and silenced them under threat of litigation if they violate their confidentiality agreements and “peer review” statutes.
The same system of coercion, control and abuse exists in Massachusetts. In the past week alone I have heard from a medical student, a resident and two doctors who complained of misconduct misconduct involving fraudulent testing and falsified diagnoses.
In “Ethical and Managerial Considerations Regarding State Physician Health Programs,” published in the Journal of Addiction Medicine in 2012, Drs. John Knight, M.D. and J. Wesley Boyd, M.D., PhD who collectively have more than 20 years experience with the Massachusetts Physician Health Program (PHP) state that:
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”13
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 13
They recommend the relationship between PHP’s and the evaluation and treatment centers and licensing boards be transparent and that national standards be developed “that can be debated by all physicians, not just those who work within PHPs.”13
Accountability, or answerability, is necessary to prevent corruption. This requires both the provision of information and justification for actions. What was done and why? Accountability also requires that consequences be imposed on those who engage in misconduct.
In discussing the financial conflicts-of-interest between PHPs and “PHP-approved” assessment centers Knight and Boyd state:
“..if a PHP highlights a physician as particularly problematic, the evaluation center might–whether consciously or otherwise–tailor its diagnosis and recommendations in a way that will support the PHP’s impression of that physician.”
To “consciously tailor a diagnosis” is fraud. It is political abuse of psychiatry. And it is not only the assessment and treatment centers willing to “tailor” a diagnosis; so too are the labs involved.
Physician Suicide
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity. But that is what is occurring. Some of us are trying to expose this corrupt system but barriers exist. As with the Laboratory Developed Tests (LDTs), those involved have intentionally taken steps to remove both answerability and accountability. Both the tests and the body of individuals administering these tests are notable for their lack of transparency, oversight and regulation. This renders them a power unto themselves.
Doctors (and others coerced into Professional Health Programs) across the country have reported going to law enforcement and state agencies only to be turned away. The Federation of State Physician Health Programs (FSPHP) has convinced these outside agencies that this is a “parochial” issue best handled by the medical profession.. Those reporting crimes are turned back over to the very people committing the crimes.
The Massachusetts Medical Society and Massachusetts DPH claim no oversight of the Massachusetts PHP, PHS.inc. The Massachusetts Board of Registration in Medicine (BORM) will not address ethical or even criminal complaints about the doctors involved in the PHP and there is good evidence that some members of the BORM are in fact complicit in unethical and even criminal behavior. As the Massachusetts AGO represents the BORM they defer issues back to them and dig no deeper.
Drs. Knight and Boyd have suggested State Audits and we are hoping that MA State Auditor Suzanne Bump will investigate the MA PHP and the Board of Registration in Medicine’s Physician Health and Compliance Unit shortly.
One major problem is that barriers have been put in place to prevent information from getting to the right people.
The majority of people at medical societies, boards, departments of public health and other organizations are individuals of integrity and honesty but the system has been erected so that valid complaints are deflected, delayed, dismissed or otherwise tabled by sympathizers, apologists and those complicity. The criminal activity the Massachusetts PHP is engaging in is undeniable and indefensible but who is going to hold them to account?
It is going to take a while to reform this system of institutional abuse and it has to be done state by state. Please take a look at the facts and documentary evidence and help me hold them accountable. This needs to be exposed, acknowledged and addressed. Doctors are dying from this system of institutional abuse. It is a public health emergency no one is talking about. Yet those behind the PHP programs are claiming this system of coercion, abuse and control is the “gold standard” of addiction treatment and, using another loophole, they want to expand this system to mainstream healthcare.
Sincerely,
Michael L. Langan, M.D.
- Skipper G. Exploring the Reliability, Frequency, and Methods of Drug Testing: What is Enough to Ensure Compliance?: Alcohol Markers and Devices. 2013; http://www.fsphp.org/Skipper, Exploring the Reliability Frequency and Methods 2 Presentation.pdf.
- Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcoholism, clinical and experimental research. Mar 2003;27(3):471-476.
- Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol Alcohol. Sep-Oct 2004;39(5):445-449.
- Kingdon JW. Agendas, alternatives, and public policies. Updated 2nd ed. Boston: Longman; 2011.
- Leape LL. Institute of Medicine medical error figures are not exaggerated. JAMA : the journal of the American Medical Association. Jul 5 2000;284(1):95-97.
- Schneidman B. The Philosophy of Rehabilitation for Impaired Physicians. The Federal Bulletin: The Journal of Medical Licensure and Discipline. 1995;82(3):125-127.
- Jansen M, Bell LB, Sucher MA, Stoehr JD. Detection of Alcohol Use in Monitored Aftercare Programs: A National Survey of State Physician Health Programs. Journal of Medical Licensure and Discipline. 2004;90(2):8-13
- Skipper G, Weinmann W, Wurst F. Ethylglucuronide (EtG): A New Marker to Detect Alcohol Use in Recovering Physicians. Journal of Medical Licensure and Discipline. 2004;90(2):14-17.
- McGarity TO, Wagner WE. Bending Science: How Special Interests Corrupt Public Health Research. Cambridge, MA: Harvard University Press; 2008.
- US Department of Health and Human Services. Mandatory guidelines and proposed revisions to mandatory guidelines for federal workplace drug testing programs: notices. Federal Register. April 13, 2004;69(71):19659-19660.
- Wood B. State of North Carolina Performance Audit North Carolina Physicians Health Program. . http://www.ncauditor.net/EPSWeb/Reports/Performance/PER-2013-8141.pdf. Accessed March 17, 2015.
- U.S. District Court Eastern District of Michigan, Case No: 2:15-cv-10337-AJT-RSW (2015). Carole Lucas, R.N., Tara Vialpandno, R.N., Scott Sanders, R.N., Kelly Schultz, P.A., and all other similarly situated health professionals v. Michigan Department of Licensing and Regulatory Affairs, Carole Engel, J.D.Former Director of Michigan Bureau of Health Professions, Ulliance, Inc. (State Contractor), Carolyn Batchelor (HPRP Contract Administrator), Stephen Batchelor (HPRP Contract Administrator), and Nikki Jones, LMSW. Filed January 30, 2015.
- Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.

Laboratory Developed Tests
Questions about the accuracy and marketing of Laboratory Developed Tests (LDTs) have led to the current debate whether the U.S. Food and Drug Administration (FDA) should regulate a subset of diagnostic tests currently exempted from oversight. Designed to bring clinical tests to market that the costly FDA process would otherwise preclude, such as those for rare diseases, the LDT pathway bypasses Federal regulation and accountability. Questions about the validity of these tests have raised concerns over patient safety and a call for oversight. Among those asking for regulation are Massachusetts Senators Edward J. Markey and Elizabeth Warren.
Opponents of regulation argue the LDT pathway enables new and pioneering tests to be developed quickly and improve patient care. A recent viewpoint piece published in JAMA opposing regulation noted such advances have occurred “in large part because of the nimbleness of relatively small clinical and academic laboratories that can quickly respond to new medical findings and patient needs by rapidly and safely developing and improving laboratory-developed tests.”
But the LDT pathway does not require proof of test validity, that the test is actually testing for what it claims to be testing, and with no FDA oversight a lab can claim any validity it wants in marketing the test. There is no accountability. Proponents of regulation argue that this lack of oversight is a direct threat to patient safety and, as an opposing viewpoint piece in JAMA notes, a “patient’s life or death could hinge on whether a single, unregulated diagnostic test result is meaningful.”
The debate has focused on the reliability and validity of a number of clinical tests currently marketed with unverified claims of accuracy such as those used for prenatal screening and Lyme disease. Notably absent from the discussions are the vast number of Laboratory Developed Tests tests being used for “forensic” drug and alcohol testing with the current FDA draft guidance stating simply:
-
“At this time, FDA will continue to defer oversight of the use of these tests in the forensics (law enforcement) setting to the existing system of legal controls, such as the rules of evidence in judicial proceedings and other protections afforded through the judicial process.”
The Birth of EtG: The Introduction and Marketing of Laboratory Developed Tests for “Forensic” Drug Testing Via a Lucrative Loophole
Numerous “forensic” tests of unknown validity using urine, blood, hair, fingernails breath and saliva have been developed and brought to market as LDTs since the first one was introduced in 2003 when ASAM physician Dr. Gregory Skipper, then Medical Director of the Alabama Physicians Health Program, “convinced the initial lab in the USA, NMS near Philadelphia to start performing EtG testing.”1 With essentially no evidence base Skipper then claimed the alcohol biomarker “appeared to be 100 percent specific” in detecting covert use of alcohol for several days after ingestion based on a study he coauthored that involved a mere 35 forensic psychiatric inpatients in Germany, all male2
 Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.
Using an arbitrary cutoff level of 100 ug/L the EtG was marketed as a valid and reliable test and blindly tested on those being monitored by programs not beholden to the strict protocol and procedure dictated by the Mandatory Guidelines for Federal Workplace Drug Testing that most Employee Assistance Programs (EAPs) adopted. In other words, the test was used on those who possessed little power or had their power removed.
The test was subsequently found to be so sensitive that it could measure incidental exposure to alcohol in foods, over the counter cold medications, mouthwash3,4, hand sanitizer gel5, and nonalcoholic wine.6 Sauerkraut and bananas have even been shown to cause positive levels.7

Shortly after the EtG debuted, complaints began to accumulate from individuals testing positive who adamantly proclaimed they did not drink. Steadfast in their trust of expert opinion and the claimed accuracy of EtG, the complaints of the accused were largely disregarded by those doing the monitoring. People lost their licenses, jobs, careers, and reputations. Others lost their freedom or had their children taken away. It is unknown how many died by suicide.
There have been multiple lawsuits filed since the introduction of the EtG including a class-action suit, but these were inevitably met with a well-funded and deep legal defense and their “experts.” The labs have taken a “stand your ground” position yielding either dismissals or in favor of the defense. As a new to the market lab with no prior evidence-based research in forensic testing prior to its implementation and use for forensic testing, the proponents of EtG testing had no meaningful opposition in terms of a scientific body of facts and evidence and no credible voice to present it. With the only “experts” in EtG validity being those who introduced and promoted its use there were no counter-forces. Those suffering the consequences of a false-positive test had no recourse. But as the toll of mayhem increased it eventually reached a tipping-point where others began to take notice.

Page from the Talbott Recovery Center list of products containing alcohol that doctors are required to avoid due to interference with EtG testing
In 2006 the Wall Street Journal reported the problems with the EtG to the general public,8 and SAMHSA issued an advisory stating that “legal or disciplinary action based solely on a positive EtG…. is inappropriate and scientifically unsupportable at this time. These tests should currently be considered as potential valuable clinical tools, but their use in forensic settings is premature.”9
Since that time Skipper has served as expert witness in close to 46 administrative hearings 22 criminal 14 custody and 1 Federal class action suit.
But this did not stop the Federation of State Physician Health Programs from using the EtG on physicians being monitored. Instead they instructed doctors to avoid anything potentially containing alcohol including hand sanitizer which a 2011 study found could result in EtG concentrations of almost 2000 ug/L. 10 To continue to justify the use of EtG they added other LDTs as confirmation tests of LDTs such as EtS and PEth– Junk Science to confirm junk science. Nonsensical smoke-and-mirrors antithetical to science and evidence-based medicine.
Since the birth of the EtG a variety of tests have been introduced and marketed as LDTs utilizing nails, blood, hair, breath and urine—all with unknown validity but marketed without constraint. No regulation, oversight or accountability exists.
The newest gadget they are using on doctors is the Cellular Digital Photo Breathalyze which he is promoting in the same manner as the EtG after a study he co-authored with Robert Dupont on just 12 subjects.
Expanding Laboratory Developed Tests to Test Everyone: The ASAM White Paper on Drug-Testing and the “New Paradigm”
Although the current use of these tests is limited to the criminal justice system and professional monitoring programs this may soon change as the American Society of Addiction Medicine is proposing a “new paradigm” of zero-tolerance random widespread drug and alcohol testing. This is outlined in the ASAM White Paper on Drug Testing and described by Robert Dupont in his keynote speech before the Drug and Alcohol Testing Industry Association (DATIA) annual conference in 2012.
The ASAM White paper states drug testing is “vastly underutilized” throughout healthcare and describes the use of drug testing “within the practice of medicine and, beyond that, broadly within American Society.”
As the consequences of a single unregulated “forensic” test result can be grave, far-reaching and even permanent it is critical that these tests be included in the debate on regulation of LDTs.
Evidence based medicine is not restricted to randomized trials and meta-analyses. It involves tracking down the best external evidence with which to answer our clinical questions.11
Expert opinion is the lowest level of evidence available in the EBM paradigm.12,13 Fortunately, the scientific method and Cochrane type critical analysis of the available evidence is a tool to help people progress toward the truth despite their susceptibilities to unconscious confirmatory bias or conscious confirmatory distortion .14 Unfortunately, no one has used these tools address they panoply of tests of unknown validity that have already entered the market ; poised to be used on virtually everyone.
- Skipper G. Exploring the Reliability, Frequency, and Methods of Drug Testing: What is Enough to Ensure Compliance?: Alcohol Markers and Devices. 2013; http://www.fsphp.org/Skipper, Exploring the Reliability Frequency and Methods 2 Presentation.pdf.
- Wurst FM, Vogel R, Jachau K, et al. Ethyl glucuronide discloses recent covert alcohol use not detected by standard testing in forensic psychiatric inpatients. Alcohol Clin Exp Res. Mar 2003;27(3):471-476.
- Costantino A, Digregorio EJ, Korn W, Spayd S, Rieders F. The effect of the use of mouthwash on ethylglucuronide concentrations in urine. Journal of analytical toxicology. Nov-Dec 2006;30(9):659-662.
- Reisfield GM, Goldberger BA, Pesce AJ, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after intensive exposure to high ethanol content mouthwash. Journal of analytical toxicology. Jun 2011;35(5):264-268.
- Rosano TG, Lin J. Ethyl glucuronide excretion in humans following oral administration of and dermal exposure to ethanol. Journal of analytical toxicology. Oct 2008;32(8):594-600.
- Hoiseth G, Yttredal B, Karinen R, Gjerde H, Christophersen A. Levels of ethyl glucuronide and ethyl sulfate in oral fluid, blood, and urine after use of mouthwash and ingestion of nonalcoholic wine. J Anal Toxicol. Mar 2010;34(2):84-88.
- Musshoff F, Albermann E, Madea B. Ethyl glucuronide and ethyl sulfate in urine after consumption of various beverages and foods–misleading results? Int J Legal Med. Nov 2010;124(6):623-630.
- Helliker K. A test for alcohol–and its flaws. The Wall Street Journal2006.
- Administration SAaMHS. The role of biomarkers in the treatment of alcohol use disorders. In: Advisory SAT, ed2006:1-7.
- Reisfield GM, Goldberger BA, Crews BO, et al. Ethyl glucuronide, ethyl sulfate, and ethanol in urine after sustained exposure to an ethanol-based hand sanitizer. Journal of analytical toxicology. Mar 2011;35(2):85-91.
- Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. Jan 13 1996;312(7023):71-72.
- Shaneyfelt TM, Centor RM. Reassessment of clinical practice guidelines: go gently into that good night. JAMA. Feb 25 2009;301(8):868-869.
- Straus SE, Green ML, Bell DS, et al. Evaluating the teaching of evidence based medicine: conceptual framework. BMJ. Oct 30 2004;329(7473):1029-1032.
- Haack S. Defending Science–Within Reason: Between Scientism and Cynicism. Amherst, N.Y.: Prometheus Books; 2003.



 The majority of doctors are of good heart and sound mind. Most doctors strive to do the right thing and the correct thing to the best of their capabilities in any given circumstance. Most doctors by nature are intelligent, inquisitive and caring. Their actions are not driven by self-interest or greed but by thoughtful reasoning and moral compass. As in any population, of course, vast differences exist in individual characteristics including intellectual acumen, empathy and common sense. Those bereft of moral compass and the intolerant and prejudiced walk among us in all professions. Medicine is no exception. The simple truth to the matter is overwhelming majority of people are good people. They are honest, have integrity and are guided by conscience. Most police officers are not trigger-happy racists. Most Catholic priests do not have an affinity for alter-boys. And most doctors do not hand out opiates like halloween candy. What we hear about are the exceptions not the rule.
The majority of doctors are of good heart and sound mind. Most doctors strive to do the right thing and the correct thing to the best of their capabilities in any given circumstance. Most doctors by nature are intelligent, inquisitive and caring. Their actions are not driven by self-interest or greed but by thoughtful reasoning and moral compass. As in any population, of course, vast differences exist in individual characteristics including intellectual acumen, empathy and common sense. Those bereft of moral compass and the intolerant and prejudiced walk among us in all professions. Medicine is no exception. The simple truth to the matter is overwhelming majority of people are good people. They are honest, have integrity and are guided by conscience. Most police officers are not trigger-happy racists. Most Catholic priests do not have an affinity for alter-boys. And most doctors do not hand out opiates like halloween candy. What we hear about are the exceptions not the rule. What might Nash think of a population in which this minority of deviants was not punished for their actions but instead given “treatment” in a communal area where they were able to interact with others of the same constitution ? What do you think Nash might say if individually and collectively this same population was put in a position of power over others but without any oversight, regulation or accountability? A disequilibrium would inevitably ensue with grave complications to the rest.
What might Nash think of a population in which this minority of deviants was not punished for their actions but instead given “treatment” in a communal area where they were able to interact with others of the same constitution ? What do you think Nash might say if individually and collectively this same population was put in a position of power over others but without any oversight, regulation or accountability? A disequilibrium would inevitably ensue with grave complications to the rest. Coraline is a children’s novella written by the British author Neil Garman in 2002. It has been compared to Lewis Carroll’s Alice’s Adventures in Wonderland and adapted into a film in 2009. Coraline is a little girl who moves into a new house with her parents. She is constantly bored and unhappy her parents do not give her the attention she wants and while exploring the house she finds a door that leads to an alternate version of her reality where her parents are fun and attentive and everything seems wonderful but things get creepy very quickly. Her parents look like her parents but instead of their eyes they have shiny black buttons and she soon finds herself in a horrific and dark place that looks like reality but slightly off and terribly ominous and threatening. Such is the case with the medical profession today. Somewhere along the line it took a nasty left turn and although looks the same its slightly off nature has become threatening and crippling to many. An erosion in the hierarchy has occurred and much of the practice and policy pushed by the self-interest groups to regulators and administrators is not only bad, it is absurd.
Coraline is a children’s novella written by the British author Neil Garman in 2002. It has been compared to Lewis Carroll’s Alice’s Adventures in Wonderland and adapted into a film in 2009. Coraline is a little girl who moves into a new house with her parents. She is constantly bored and unhappy her parents do not give her the attention she wants and while exploring the house she finds a door that leads to an alternate version of her reality where her parents are fun and attentive and everything seems wonderful but things get creepy very quickly. Her parents look like her parents but instead of their eyes they have shiny black buttons and she soon finds herself in a horrific and dark place that looks like reality but slightly off and terribly ominous and threatening. Such is the case with the medical profession today. Somewhere along the line it took a nasty left turn and although looks the same its slightly off nature has become threatening and crippling to many. An erosion in the hierarchy has occurred and much of the practice and policy pushed by the self-interest groups to regulators and administrators is not only bad, it is absurd. My hero’s in medicine both historically and personally have always been the maverick’s -those doctors with superlative and almost preternatural clinical acumen who can make the right diagnosis when no one else could or have made daring and unprecedented contributions to the field.
My hero’s in medicine both historically and personally have always been the maverick’s -those doctors with superlative and almost preternatural clinical acumen who can make the right diagnosis when no one else could or have made daring and unprecedented contributions to the field.
 Authority needs to be grounded in wisdom and guided by ethical principles and codes of conduct. Such is not the case. If the information agencies rely on to make decisions and policy is unreliable then bad decisions, wrong decisions and flawed public policy can occur. The consequences can be far-reaching and grave.
Authority needs to be grounded in wisdom and guided by ethical principles and codes of conduct. Such is not the case. If the information agencies rely on to make decisions and policy is unreliable then bad decisions, wrong decisions and flawed public policy can occur. The consequences can be far-reaching and grave.







 The
The  The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.
The report fails to mention it because it is more either/or logical fallacy based on the false dichotomy between “treatment” and “punishment” that is often used to promote the FSPHP mythology. Although PHPs do not have the legal authority to mandate, suspend or revoke a license they have the functional authority to do so. This is also dictated by public policy.  “Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.”
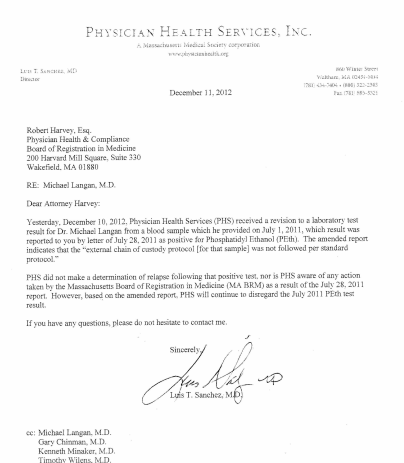
“Compounding the problem, said Wood, was that “the chief executive and medical director were in total control of entire process.” They assessed allegedly impaired doctors, but when those assessments were contested, they were responsible for presenting complaints to the state medical board. The doctors concerned were not allowed to be present and were not allowed to see the programs’ medical reports on them.” Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal.
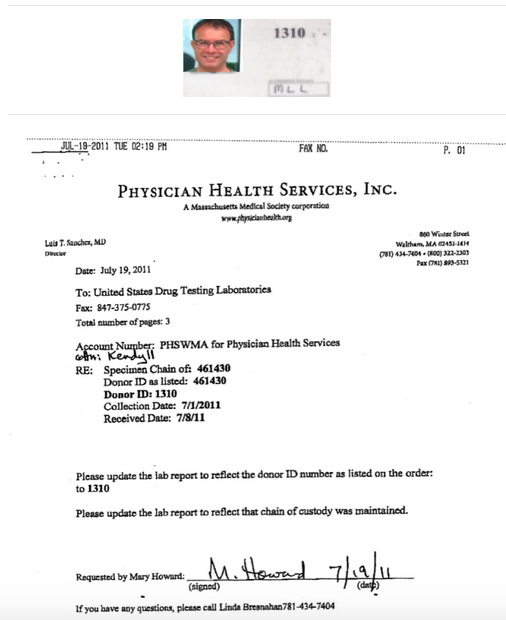
Of the many hundreds of doctors I have spoken to and who have taken my survey not one has been able to obtain evidence of abuse. It was either refused, censored or doctored. I have obtained documentary evidence that is specific, detailed and unequivocal. What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (
What is chilling is that this request to falsify evidence was done by fax and the lab complied with full knowledge that the positive-test would result in grave and possibly permanent consequences for someone. The moral detachment of Jones is incomprehensible to me. If I was offered a million dollars at this moment to fabricate a drug test on some stranger I would not do it. I would not for any amount of money and I don not believe the majority of my friends would either.I also contacted Jones (  It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry.
It is now time to enter phase two of exposing the corruption of PHPs. It is now necessary to necessary to relentlessly contradict the lies and falsehoods and and present the evidence with logic and clarity. It is necessary to name names, point fingers and demand that direct and specific answers to direct and specific questions. It is time to shine a bright light on the specific unethical and illegal acts detailed here. They are the rule not the exception and the diagnostic rigging and forensic fraud make these more murders than suicides. This is a public health emergency. By my estimates over 80% of those being monitored by PHPs do not even meet the diagnostic criteria for substance use disorder or any other psychiatric disorder. It is political abuse of psychiatry. Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
Legitimate authority has a responsibility to be truthful to one’s words and deeds and policies need to be enforced in a consistent manner. State PHPs are engaging in fraud in collusion with their preferred drug and alcohol assessment, testing and treatment centers. They are giving diagnoses to individuals who do not meet the diagnostic criteria for a given diagnosis to provided unneeded treatment. They are financially exploiting doctors under threat of disciplinary action against there medical licenses.
 board’s position on the fraudulent practice of medicine is quite clear.
board’s position on the fraudulent practice of medicine is quite clear.





























































 It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong.
It is hard to imagine a more stupid or more dangerous way of making decisions than by putting those decisions in the hands of people who pay no price for being wrong. 


 Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition.
Once practice and policy is identified a risk/benefit type analysis can be done on each and this is a rather simple matter as the issues are fairly black and white. Statistics is not needed-just common sense and logic. What one will find is that the practice and policy promoted by the FSPHP has not in the best interests of doctors or society but in the best interests of the FSPHP and the drug and alcohol testing and treatment industry . In short, the individual practices and policies have provided physician health programs with more power and protection while incrementally removing the fundamental rights and due process protections of doctors with the end result being not only control of their professional behavior but their private lives. To benefit the drug and alcohol testing and treatment and treatment industry they have pushed a plethora of bad ideas including introducing junk-science for forensic drug testing and limiting physician evaluations to only “PHP-approved” assessment and treatment centers. A public policy analysis is long overdue. So too is a conflict of interest analysis and a critical analysis of the”research” which consists of two categories; 1. Research showing that shows the high success rates and benefits of PHPs 2. Research on laboratory developed tests (LDTs) and other dubious testing methodology they have introduced (such as non-validated neuropsychological testing for diagnosing disruptive physicians) and promoted (including polygraphs which is unbelievable since AMA policy discounts them as a game of chance.). All practice and policy that has been pushed by the FSPHP was accepted by the FSMB (and others) without question or concern. It has all been done with no meaningful opposition. Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add:
Highlighting the significant financial conflicts-of-interest between PHPs and their preferred assessment the authors add: In her
In her 
 Medicalization removes the constitutional safeguards of due process. The potential for abuse is especially the case in the absence of clearly articulated and openly established program policies and procedures.
Medicalization removes the constitutional safeguards of due process. The potential for abuse is especially the case in the absence of clearly articulated and openly established program policies and procedures. In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.
In the interim I propose the following. It would not be that difficult to set up a second opinion through medical schools involving an anonymous group of their own experts. The reason for this anonymity is self-evident. The primary reason other doctors do not speak up against these programs is the fear of being targeted themselves. Allowing physician health programs carte blanche authority is bad policy and being bamboozled into accepting this group as unquestioned expert authority is a fools game. Providing independent evaluation is a simple task and if the independent evaluation concludes there is no problem then rest assured there is no problem.



 As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.