From http://zdoggmd.com/



From http://zdoggmd.com/

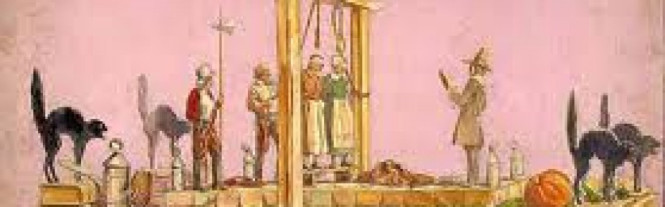
 From the late 15th century through the early 17th century a confederacy of “authorities” calling themselves demonologists assisted in identifying witches. Shaping ecclesiastical orthodoxy they set the standards that cooperating political authorities could follow in criminalizing, persecuting and punishing heretics.
From the late 15th century through the early 17th century a confederacy of “authorities” calling themselves demonologists assisted in identifying witches. Shaping ecclesiastical orthodoxy they set the standards that cooperating political authorities could follow in criminalizing, persecuting and punishing heretics.
Behavioral manifestations included living alone, cultivating strange herb and saying hello to a neighbors cat.Witches were blamed for everything—plague, crop failure, and erectile dysfunction.
Using the nebulous “witch label” anyone with a grudge or suspicion could accuse anyone of witchcraft .
Propaganda, threats, misinformation, guilt assumed from the start.
 Physician oversight of witch persecution was standard.
Physician oversight of witch persecution was standard.
During the European witch-hunts the legal notion of crimen exceptum (an exceptional and most dangerous crime] allowed for the suspension of normal rules of evidence to punish the guilty.
Because of the nature of the enemy the evidentiary bar was lowered and any witness, no matter what his credentials, could testify against the accused.
Belief in the seriousness of the situation rationalized cruelty.

The Devil’s mark (Stigmata diaboli) was taken as the mark of a witch entailing close inspection.
Professional witch-prickers used needles, pins and bodkins to poke the skin with lack of bleeding confirming the accusation. The accused did not bleed due to retractable needles and sleight of hand. False accusations, if exposed, were excused if they were a result of “zeal for the faith.”
The consequences of being branded a heretic by questioning the existence of witches essentially silenced any dissenting voices and the notion of crimen exceptum freed the consciences of those involved.

Sanctimony, feigned piety and hypocritical devoutness was used as justification. After all–Torture and torment are a small price to pay when it comes to protecting the public and saving souls.
Through the witch trials clerics, doctors, and lawyers used their expertise as witnesses to increase their prestige. Witch hunts developed into a means of economic profit. Some gained a lot of money from the witch trials. The witch or her relatives paid for the salaries of those who worked the witch trials including judges, court officials, torturers, physicians, clergymen, scribes, guards, attendants. Even the people who made the stakes and scaffolds for executions gained from the conviction and death of each witch.
 “Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.”
“Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.”
Context, characters and circumstances may differ but the mechanics do not. The mosaic remains the same. The Malleus shows how false constructs come to be regarded as irrefutable and the creation and chains of causation are timeless.




 Reblogged on WordPress.com
Reblogged on WordPress.com
Source: Do physician health programs increase physician suicides? —Pamela Wible, MD

The “impaired physicians movement” often uses William Halsted as an example of how doctors can continue practicing medicine while impaired and how the “code of silence” allows it.
Multiple sources document his behavior when he was addicted to cocaine including his behavior in the OR. This is what led him to treatment at Butler in Providence where Morphine replaced cocaine.and to which he was addicted to until he died. No evidence of impairment was reported during those years but his achievements are prolific and numerous.In all likelihood Halsted’s morphine intake was a constant measured dose that allowed him to function on a daily basis– s maintenance dose that was consistent. Whatever the case may be it is absurd to interpret the situation a century later in our current social, cultural and intellectual context.
Halsted changed medicine forever and made this world a better place. His contributions to public health and aseptic infection control alone saved untold lives. He is a hero and a legend..
But from the point of view of some people he was just an addict with a “disease” and noting else matters.
Black and white thinking, false dichotomies and either or thinking abound in this groupthink.
Thank God this group wasn’t around when Halsted was. But the question is how many Halsted’s are we losing today—snuffed out by zealots and self-appointed experts
How do we care for the people who care for us? As doctors, we’re immersed in pain and suffering — as a career. We cry when our patients die. We feel grief anxiety, depression — even suicidal — all occupational hazards of our profession.
A recent Medscape article on physician health programs suggests the people who are here to help us may actually be doing more harm than good. And they may even be increasing physician suicides.
Here’s one of them:

Dear Some, My family, I…
View original post 30,859 more words

But in this Court, what Diff’rence does appear! For every one’s both Judge and Jury here; Nay, and what’s worse, an Executioner. William Congreve, The Double-dealer Regulatory cap…

And as far as I can find, these documents are the most elaborate and complete representation of the mechanics of forensic fraud available and show the sequential steps between the requesting party and complicit lab. The documents also show how easy laboratory misconduct is accomplished as well as the moral detachment of the involved parties.Bertram knows these are crimes. I have also informed him that since 2011 there have been multiple suicides related to allegedly falsified alcohol tests at the same lab seen here and the ongoing concealment of laboratory fraud is equally abhorrent as those who engage in it. I am unclear of his motive in defending a cover-up of forensic fraud in the wake of other lab scandals but one other thing is for certain. When this racket is exposed the record will show who knew about it and when.

EDS and Chronic Pain News & Info
ABMS accepts “Addiction Medicine “ – 3/14/2016 – update/correction to a previous post
The American Board of Medical Specialties (ABMS) officially recognized Addiction Medicine as a subspecialty at its October 2015 Board Meeting in Dallas, Texas.
The American Board of Preventive Medicine (ABPM), a Member Board of ABMS, sponsored the application for the subspecialty to allow physicians certified by any of the 24 ABMS Member Boards to apply for the new certificate
However, a previous article (and blog post) shows exactly how flimsy the requirements are to become an “Addiction Medicine” specialist.
With little training in anything but the 12-step model, such specialists are supremely unqualified to deal with the complexities and social consequences of addiction.
View original post 953 more words

Link to Medscape article by Pauline Anderson Here:
Link to illegible, post-dated and undated documents submitted as evidence and mentioned in article can be seen here> board-records-obtained-june-2016
Link to document written June 6, 2013 but date-stamped as being received in 2012 ( both by hand and apparently by the Board’s Document Imaging Unit (DIU) > Back to the Future: Massachusetts Board of Registration in Medicine
Source: Medscape Article Now Live! Please comment and tell your stories now!

 Link to Medscape article by Pauline Anderson Here:
Link to Medscape article by Pauline Anderson Here:
Link to illegible, post-dated and undated documents submitted as evidence and mentioned in article can be seen here> board-records-obtained-june-2016
Link to document written June 6, 2013 but date-stamped as being received in 2012 ( both by hand and apparently by the Board’s Document Imaging Unit (DIU) > Back to the Future: Massachusetts Board of Registration in Medicine


Michael Langan, MD, a Boston-based internal medicine specialist who has fought the Massachusetts Physician Health Service (PHS) and Board of Registration in Medicine for years to reinstate his license, has suffered a setback but is bolstered by a new development.
A justice of the Supreme Judicial Court of Massachusetts has denied Dr Langan’s petition to invalidate the 2013 suspension of his medical license for not meeting conditions to have his license reinstated.
However, a new law has enabled Dr Langan to access his records. According to Dr Langan, these documents show that the court did not consider key evidence in his case, as demonstrated by the fact that his hearing occurred after the date of receipt that is stamped on the documents. This may offer an opportunity to reopen his case.
The court decision, which was handed down in December by Associate Justice Geraldine Hines, states that although Dr Langan completed required psychiatric evaluations, he “did not submit a suitable worksite or substance abuse monitoring plan. In combination with his violation of the LoA [Letter of Agreement] meeting requirement, the board’s decision to affirm its prior suspension of petitioner’s license to practice medicine is supported by the record. The board’s decision to deny reinstatement in the absence of an acceptable plan is affirmed.”
“It’s unbelievable; everyone is dumbfounded,” said Dr Langan of the decision.
Dr Langan is appealing the denial of his petition, a process that will take an estimated 6 months.
He maintains that the PHS committed “forensic fraud” and concealed doing so.
“If I couldn’t win with all the direct evidence of felony crimes that you don’t need to be a lawyer to recognize, then I don’t think anyone can,” he told Medscape Medical News.
The PHS is a confidential resource for physicians and medical students seeking help for a variety of physical and behavioral health concerns, which may include difficulties with substance use.
In 2007, Dr Langan was at Massachusetts General Hospital (MGH) and Harvard University when he approached the PHS to help him with his dependence on Vicodin, an opioid analgesic.
He became dependent on Vicodin after a bout of chickenpox during residency, when he developed shingles. He stressed that there were no work-related problems associated with use of this drug.
According to Dr Langan, there were no problems until mid-2011, when a report from the US Drug Testing Laboratories found he was positive for phosphatidylethanol (PEth), a blood marker for chronic alcohol use.
The level detected was 365.4 ng/mL, which “is the equivalent of drinking a half gallon of whisky a day,” or a sign of end-stage alcoholism, said Dr Langan, who insists he has never had an alcohol problem.
“That the test was invalid at this point should have been self-evident,” said Dr Langan.
Lab Fraud?
Suspecting that there had been “lab fraud” and that he would “end up being admitted for 3 months,” Dr Langan said he requested, but was denied, an independent evaluation outside the 12-step PHP-approved list of facilities. Because his request was denied, he attended one of the approved facilities, Hazelden Addiction Treatment Center, in Minnesota, where he “was cleared.”
An independent investigation by James G. Flood, PhD, who has been chief of toxicology at MGH for nearly 30 years, concluded in a November 5, 2012, letter to Dr Langan’s lawyer “that there is a purposeful and intentional act by PHS” to show Dr Langan’s test as valid “when in reality this test was invalid and involved both fatal laboratory errors” and inadequate review of the results.
Any confirmatory, positive finding based on the July 2011 test “should be reversed, rectified and remediated,” Dr Flood writes.
Dr Flood claims the sample was directed to the wrong laboratory, where it sat for several days. The storage conditions of the sample while at that laboratory were not documented.
Following an investigation by the College of American Pathologists, in October 2012, Dr Langan’s laboratory test result was corrected from having a positive result to being an invalid test, but he said he did not learn of this change until months later.
Dr Sanchez noted that, on the basis of the revised report, “PHS will continue to disregard the July 2011 PEth test result.”
Dr Langan requested the record of the chain of custody pertaining to his testing. This document showed that the test was “not only invalid but falsely created,” said Dr Langan. He added that it included a fax from the PHS requesting that his identification number be added to an already positive test and that the chain of custody be updated.
“You can’t update a chain of custody, as it is generated in real time,” said Dr Langan. “This is forensic fraud. It clearly shows collusion between the PHS and the lab.”
In an October 2012 letter, Dr Sanchez alleged that Dr Langan did not attend required peer support group meetings, but according to Dr Langan, this claim is “without fact or support.” Dr Langan maintains that he attended all required meetings. He also maintains that the PHS actions were in “retaliation” for requesting the chain of custody record.
Massachusetts PHS Director Dr Sanchez did not respond to a request from Medscape Medical News for clarification.
“The AG’s [Attorney General’s] Office often defends state agencies in litigation and we typically do not comment on behalf of our clients, who in this case is the Board of Registration in Medicine,” Emily Snyder, deputy press secretary, Office of Massachusetts Attorney General, told Medscape Medical News in an email.
Intentional Delay?
Dr Langan alleges that the PHS “intentionally delayed” his efforts to undergo a psychiatric evaluation that was necessary to have his license reinstated. He said the PHS insisted he get this evaluation out of state, even though he suggested three Boston-area board-certified experts.
Dr Recupero’s November 2013 report determined that Dr Langan “is safe to return to the practice of medicine without further supervision,” that he “has an excellent prognosis and a very low risk of relapse,” and he “has not had an alcohol use, abuse or dependence problem.”
Many of the conflicts between the PHS and Dr Langan revolve around positive test findings, Dr Recupero notes in her letter.
Dr Langan acknowledges he used hand sanitizers in the course of his work as a physician. Owing to severe allergies, he also uses prescribed asthma inhalers, which contain alcohol as a propellant.
Dr Recupero also notes that “almost without exception,” Dr Langan’s test findings have been below the minimum level to declare a test positive and that positive findings “are not a sign of relapse.”
Dr Langan said that since it suspended his medical license, the board has “engaged in a persistent pattern of ignoring my every reasonable effort at trying to be reinstated” and has “abused the administrative law process to accomplish this.”
Medscape Medical News contacted the Massachusetts medical board as well as its counsel, Deb Stoller, but received no response.
“Close to Homeless”
A memorandum to the Supreme Judicial Court, filed May 13, 2016, proposed a settlement between Dr Langan and the board. In return for the immediate reinstatement of Dr Langan’s license, he would be monitored for a maximum of 3 months by Dr Recupero and Timothy E. Wilens, MD, codirector of the Center for Addiction Medicine at MGH.
That memorandum was accompanied by letters from Dr Recupero and Dr Wilens agreeing to the terms, but according to Dr Langan, it has been “ignored.”
“The board did not acknowledge or address the proposals in any way,” said Dr Langan.
Dr Langan maintains that he “never ever” had any patient care or malpractice problems during his 15 years at MGH. In fact, his supervisors and colleagues reported that his work performance has been “superlative” on all counts, he said.
Many in the addiction medicine and psychiatric community support Dr Langan. He has letters from high-profile physicians in the field who verify that he is safe to practice medicine.
A first petition was filed in the Supreme Court on October 22, 2014, but the judge dismissed it because it had not been filed within the required 60-day period. Dr Langan’s most recent petition was filed July 3, 2015.
The past few years, he said, have taken a toll on his family. They have lost their home and health insurance because of his inability to practice his profession.
Disheartened by this latest setback, Dr Langan is looking into the possibility of becoming licensed in another state and leaving Massachusetts.
But Dr Langan has renewed hope. Under Massachusetts’ new Public Records Reform Law, which went into effect January 1, 2017, “the board was forced to comply with my request for records within 10 days,” and has done so, he said.
According to Dr Langan, these records show some irregularities that may bolster his case.
“A letter dated December 15, 2011, introducing exculpatory evidence was date-stamped January 17, 2012, almost 1 month after the hearing where it was submitted as evidence. All of the other documents had either illegible or absent date-stamps,” he said.

Post by @mllangan1. Martin Luther King Day 2017
Source: “There comes a time when silence is betrayal.” ― Martin Luther King Jr.


 and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.
and alcohol testing labs have no FDA oversight as the tests are non-FDA approved. Other than accreditation agencies such as the College of American Pathologists there is no agency to investigates error or misconduct. CAP cannot sanction. The assessment and treatment centers have little oversight or regulation. In sum this system refuses to provide information and even if they did provide information they do not have to justify it to anyone and no agency exists to punish them even if they could not justify it. Zero accountability.