I’m hearing from more and more doctors via my survey, emails and phone calls. At this point the patterns are becoming crystal clear and they involve the same “physician wellness” actors, the same “PHP-approved” assessment and treatment facilities and the same commercial “forensic” drug testing labs.
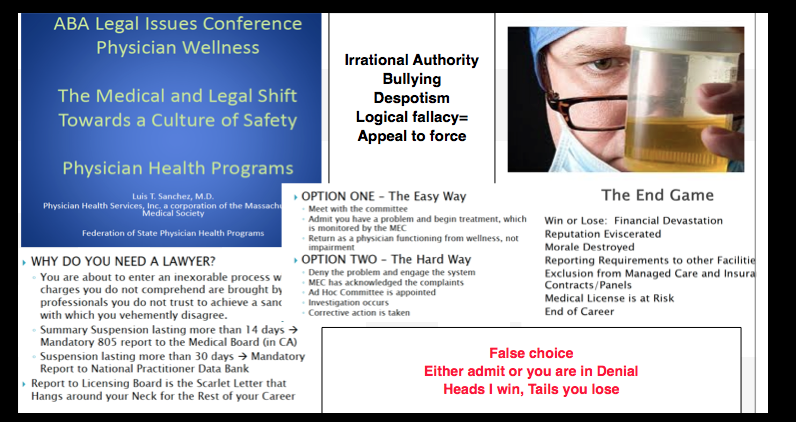
It is all the same M.O. A false accusations is made followed by misrepresentation of laboratory developed tests (LDTs) or outright forensic fraud. A referral is then made for an “evaluation” at one of the “PHP-approved” facilities where an “assessment” is “tailored” to fit a pre-determined diagnosis. The PHP then says do anything and everything we say or we will “end you.” And all too often that is exactly what they do. It is Political Abuse of Psychiatry plain and simple. It does not get any more egregious than this folks.
The Doctors dying from this system of institutional injustice are not dying by suicide. This is more akin to murder and the murderers have removed themselves from all aspects of accountability including answerability, justification for actions and the ability to be punished by third party actors truly outside the system. It is a rigged game.
The sociopaths responsible for ordering false assessments and falsified drug and alcohol testing as well as those complying with it in the drug and alcohol testing, assessment and treatment industry need to be held accountable.
Those ordering the falsified tests and assessments are essentially putting guns to the heads of doctors. The labs and rehab centers complicit in this fraud are pulling the trigger. Simple as that.
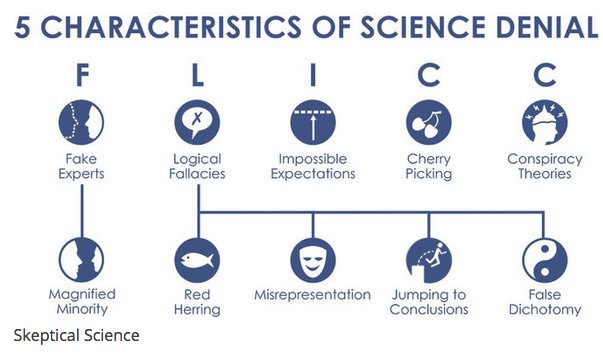
Science denial has real, societal consequences. Denial of the link between HIV and AIDS led to more than 330,000 premature deaths in South Africa. Denial of the link between smoking and cancer has caused millions of premature deaths. Thanks to vaccination denial, preventable diseases are making a comeback.
Denial is not something we can ignore or, well, deny. So what does scientific research say is the most effective response? Common wisdom says that communicating more science should be the solution. But a growing body of evidence indicates that this approach can actually backfire, reinforcing people’s prior beliefs.
When you present evidence that threatens a person’s worldview, it can actually strengthen their beliefs. This is called the “worldview backfire effect”. One of the first scientific experiments that observed this effect dates back to 1975.
The essay below found on 123HelpMe.com called The “Doctor Who Saved Boston.” is about Dr. William J. Morgan, the brilliant hand surgeon who helped the Red Sox win the World Series for the first time in 86 years. Morgan performed surgery on Curt Schilling’s severely damaged ankle that allowed him to pitch in game 6 of the ALCS against the Yankees when we were down three games to two.
No known medical or surgical options existed to allow Schilling the functionality to pitch. But just as things were looking bleak Dr. Morgan miraculously performed an unprecedented procedure he invented that allowed Schilling to pitch seven innings winning the game 4-2. He created a wall of stitches to hold Schillling’s torn tendon sheath in place before game 6’s win and again before game 2 of the World Series that we also won.
And October 27. 2004 is a magical date for red sox fan. Watching it unfold with my wife and daughters and the joy and excitement that followed is a vivid memory for me that I will never forget and it should be noted that without Dr. Morgan that night would never have happened. Without Dr. Morgan the curse would not have been reversed. He is a true Boston hero. But, as with all of us, he is not perfect. In November of 2003 he was arrested for driving under the influence and, as a Massachusetts doctor, he was mandated to Physician Health services (PHS) under a monitoring contract. According to news sources from February of 2010 Dr. Morgan was forced to give up his right to practice medicine in Massachusetts as a result of “unspecified allegations” and reading these reports the assumption that he must have done something very wrong is assumed–a logical and rational conclusion based on how we assume the world works.
I was reminded of doctor Morgan because today is opening day for the Red Sox. Over the past couple weeks I have been contacted on average four time a day by doctors who are currently suffering under their state physician health programs or by those who wanted to tell me of the circumstances surrounding the suicides of doctors they loved. The stories I have been hearing are heartbreaking and unreal but the patterns are the same. One of the most bothersome facts is that I have yet to hear from anyone who was truly an addict or alcoholic. Like Dr. Morgan, some life event bought them a one-way ticket into a PHP and from that point on their lives and locus of control was placed in the hands of others. Most of the doctors I have spoken to are good and kind doctors who were referred for situational factors and one-offs–mistakes or circumstances that were transient. Many were given positive tests using the non-FDA approved laboratory developed tests (LDTs) and pulled out of practice resulting in suicide.
The “unspecified allegation” leading to Dr. Morgans 2010 loss of license was that he had a positive Phosphatidyl-ethanol (Peth) test ordered by Dr. Luis Sanchez and reported as positive by USDTL. And as seen here, these two cannot be trusted. Intentional fraud perpetrated in this manner requires zero tolerance. It also brings into question the validity of all testing done by PHS and performed by USDTL. It is extremely concerning that criminal acts done under color of law is not being addressed by the state medical society and the Department of Health (DPH).
The sociologist Stanley Cohen’s States of Denial: Knowing about Atrocities and Suffering (Polity Press, 2001) systematically analyzes processes of denial by both individuals and governments and describes five methods of denial:
1. Deny responsibility: “I don’t know a thing about it.”
2. Deny injury: “It didn’t really cause any harm.”
3. Deny the victim: “They had it coming to them.”
4. Condemn the condemner: “They’re corrupt hypocrites.”
5. Appeal to higher loyalties: “I owe it to my mates.”…
None of these apply here. I happen to know that the positive test given to Dr. Morgan was not the result of anything he did. Sanchez and Jones claim professionalism and high ethical standards but the undeniable evidence shows they are unethical individuals engaging in criminal acts. These need to be exposed and those involved need to be held accountable.
Schadenfreude is a word taken from German and literally means “harm-joy.” Along with psychopathy and narcissism. schadenfreude seems to be a common characteristic of those involved in PHPs. Deriving pleasure in the misfortunes of others and particularly if that person is someone who represents what they could never be. I understand they took particular pleasure in bringing down Dr. Morgan and he deserves to be restored to his status as a true Boston hero. The city of Boston and Red Sox fans everywhere have the responsibility to make sure they be charged criminally by law enforcement. We owe it to Dr. Morgan and any others who have been victimized by the Massachusetts PHP.
The Doctor Who Saved Boston
The memories of the Red Sox run to the 2004 World Series championship this year will remain in the minds of Sox fans forever. It is about Dr. William J. Morgan, a brilliant hand surgeon who performed a risky
Whether it is David Ortiz’s walk off performances against the Angels and Yankees, Manny Ramirez’s tape measure home runs, or Derek Lowe winning the clinching games of all three playoff series, Red Sox nation will not soon forget the memories that the “bunch of idiots,” as centerfielder Johnny Damon dubbed this year’s Sox club,provided them, nor will they forget the Sox all out assault on baseball and Boston sports history.
But of all the images the fans retain, of all the feelings they experienced, of all the heroes Sox nation put on an altar and worshipped – the most memorable has to be Curt Schilling pitching three games on an inured ankle, blood from broken sutures seeping through his sock and a look of obvious discomfort on his face, winning two, and capturing the heart’s of every member of Red Sox nation.
But to understand the elation of the Nation and the reason that it has turned Curt Schilling into a God in the church that Cy Young, Ted Williams, and Carl Yaztremski built, we have to take a step back and remember the predicament that the Red Sox were in just over two months ago.
It was October 12, and the Yankees had beaten the Red Sox in Game one of the ALCS. It was only one game, but that familiar feeling was back. That familiar feeling that Red sox fans have of doom and gloom lingering just over the horizon returned.
Curt Schilling, the hired gun, the man who Sox management had brought in to beat the Yankees in just this situation, had not only lost the game, but looked utterly ineffective in doing so, allowing six runs in just three innings of work and the media was reporting that Schilling may not pitch again.
On June 10, reports came out on ESPN and in the Boston papers that Schilling had a minor injury to his ankle but that he would pitch through it and make his start that night and would not have to go on the disabled list.What came out later on in the papers was that Schilling had made the majority of his starts in the 2004 season only after undergoing shots of marcaine, which sportsinjuries.com describes as a long lasting local anesthesia that is used for pain management and works by blocking nerve sensations.The attitude that the Red Sox seemed to take toward Schilling’s injury was no harm, no foul, and after June little was heard about Schilling’s ankle, that is until October 5.October 5 was the beginning, and almost the end, of the Red Sox 2004 playoff run. It was a glorious, and infamous, day in Red Sox history. Curt Schilling pitched 6 and 2/3 strong innings at Anaheim, allowing just two runs and scattering nine hits as the Red Sox cruised to a 9-3 victory.
But late in the sixth inning, Schilling pulled up lame after fielding a slow roller down the first base line and throwing the ball over first baseman Kevin Millar’s head. He was favoring that same right ankle that had been hurting him all year.
Back to October 12, and the feelings of anxiety that every Sox fan from Maine to Rhode Island no doubt had in the pit of their stomachs. Questions were swirling around Boston. Just how serious was Schillings injury? Could he pitch again? Would he pitch again? Is there a God?
Jamie Musler, an assistant clinical specialist at Northeastern, put the injury into perspective.
Musler said that Schilling tore the tissue that covers his peroneal tendon, which sits in a small groove in the fibula and is partly responsible for moving and planting the foot. Musler said that this type of injury is caused by a traumatic event to the foot or ankle, like a significant ankle sprain, and when Schilling was moving his foot, the tendon was slipping out and causing an uncomfortable, but not necessarily painful, snapping sensation because the tendon was snapping across the fibula. This, Musler said, would directly affect foot mechanics and cause a huge problem in Schilling’s delivery.
And it would present a huge road block in Boston’s attempt to win a World Series title.
Schilling meant more to the 2004 Red Sox club than any other player. He was the tone setter and the ace, and without him the Sox would have no chance against the hated Yankees.
The Red Sox needed Schilling, because number two starter Pedro Martinez is not the fire balling Dominican dandy he used to be. And the Yankees, it seemed, had his number of late after he lost two late season starts to them, prompting Pedro to say in a press conference after one of those losses that he could “just tip my hat and call the Yankees my daddy.”
After Pedro, things got even bleaker, with inconsistent and fragile Derek Lowe, aging and unpredictable knuckleballer Tim Wakefield, and young, playoff inexperienced Bronson Arroyo filling out the rotation. These four hurlers are serviceable and talented major league pitchers, but they were not the automatic win that Schilling had proved himself to be in postseason’s past, especially in 2001, when he garnered co-MVP honors after defeating the Yankees in the World Series.
So in comes the man from behind the scenes. The man who would help the Red Sox end 86 years of playoff futility, Red Sox team doctor Bill Morgan, who talked about the injury and treatment in “Faith Rewarded,” the DVD that the New England Sports Network (NESN) recently released.
“It was a very unique situation. Either we did this or (Schilling) didn’t pitch,” Morgan said. “And he was determined that he was going to pitch, no matter what it took.” But what could Morgan do?
What followed was possibly the most publicized treatment of a sports injury in history. One could not turn on a New England news program or open up a New England paper without the top story being about Curt Schilling’s right ankle.
First, according to boston.com, the Red Sox front office brought in Dr. George H. Theodore, chief of foot and ankle service at Massachusetts General Hospital, to help Dr. Morgan try to create a brace to immobilize Schilling’s ankle while he pitched. The idea was that by eliminating movement of the ankle he would eliminate movement of the tendon and eliminate the sensation. But the problem, Schilling insisted, was that the sensation was altering his delivery, and that became apparent after his struggles in Game one of the ALCS. File that idea in the circular cabinet.
Next on the block, according to boston.com, was pair of customized cleats. Morgan had Reebok play around with different styles of cleats, from high tops to low tops, raised bottoms to lowered bottoms, in an attempt to find Schilling a comfortable medium. No dice. Schilling still could not get comfortable.
According to the Massachusetts Medical Board’s website, Dr. William Morgan is an orthopedic surgeon who specializes in hand surgery. He has his own private practice in Brighton, but his primary work setting is in hospitals. Morgan works out of several area hospitals and rehabilitation centers, including St. Elizabeth’s Medical Center of Boston and New England Baptist Hospital, New England Rehabilitation Services of Central Massachusetts, Worcester Medical Center, and University of Massachusetts Memorial Medical Center. Morgan also works out of the Massachusetts Hospital School.
Morgan got his degree from the Texas Medical College and Hospital in Galveston, Texas. He received post graduate training at the University of Massachusetts Medical Center. He continued his post grad training in hand and upper extremity surgery at the Roosevelt Hospital in New York, Brigham and Women’s Hospital, New England Baptist Hospital, and the Kantonspittal in Basle, Switzerland.
Morgan performed successful wrist surgery on one former Boston Red Sox superstar shortstop Nomar Garciaparra, allowing him to come back from what could have been a career altering injury as the All Star he was before he was injured.
The point is that Morgan is not some shaky med student on his first hospital residency. He has been around the block a few times and he knows his orthopedic surgery.
Musler said that with any injury, a doctor has to analyze it by thinking “what is the injury? What can we do to keep the tendon in place? If the feeling is throwing (Schilling) off, how do we help that?”
Morgan, it would seem, did just that, and came up with a new treatment, which he based off of the usual treatment for Schilling’s injury. Musler said that the usual treatment for the injury is to go in and deepen the groove that the peroneal tendon sits in. Musler showed me a video of the procedure in which surgeons cut away the tissue surrounding the tendon and the tendon sheath and then used a surgical drill and chisel to physically deepen the groove in the fibula that the tendon sits in. The surgeons then sutured the sheath back in place and closed the opening.
But Morgan and the Sox didn’t have that much time. They had four days. They went in, did the procedure, gave Schilling another marcaine shot, and, as they say, the rest is history.
Schilling came back and won game six against the Yankees. After the game, Morgan took out the sutures, Musler said, to avoid infection.
Morgan did the procedure again before Game two of the World Series, and Schilling would later say that had the series gone past four games he and Morgan had decided not to do the procedure again and that Schilling would shut it down for the rest of the series.
This time, Schilling was pitching on what is the biggest stage in sports, the World Series, against the best hitting team in baseball, the St. Louis Cardinals, whose line up featured Albert Pujols, the best young hitter in baseball and an MVP candidate, Scott Rolen, the RBI leader in the NL during the regular season, hard hitting and speedy shortstop Edgar Renteria, and two probable Hall of Famers in outfielders Larry Walker and Jim Edmonds.
Schilling was dominant. He made the heralded and hyped Cardinal offense look like a team of Little Leaguers as he pitched six strong innings allowing no earned runs and only four hits.
The rest, as they say, is history. The Sox would go on to sweep the Cardinals in four games, ending their 86 year dry spell of World Series titles and sending New England into a euphoria that it has still not recovered from.
But one has to wonder if there will be any lingering effects from the injury. Will Schilling be alright to pitch next year as the Sox try to repeat as champs?
Mary J. Hickey, an Assistant Clinical Specialist in the Northeastern department of Physical therapy, thinks so.
“Curt made an informed choice about his ankle. I don’t think there will be any long lasting damage,” Hickey said.
But Schilling is not out of the woods yet. Hickey said that Schilling faces at least four to six weeks in a cast, during which he will be seen often by Morgan and the Red Sox medical staff, and Musler said that Schilling faces five to six months of rehab to get back his range of motion, endurance, strength, and sports’ skill. Musler said that this could risk further injury if Schilling is not properly prepared for next season and presses when he is not ready.
Regardless of rehab and healing time, Curt Schilling and Red Sox fans are on cloud nine. The Red Sox are World Series champions for the first time in 86 years, and Sox fans have a new hero and new memories.
The memory of Curt Schilling, of him pitching hurt, grimacing in the dugout, bloody sock and all, will remain with everyone who saw it, even Yankees fans, forever. Schilling billed himself as the hired gun, a man who said in an interview with the Boston Herald before the ALCS that “he was not sure of any scenario more enjoyable than making 55,000 people from New York shut up.” But in the end he was so much more than just a hired gun, he was a hero in real red socks. And he made more than 55,000 people from Boston stand up and applaud as he became the newest Red Sox player to be canonized in the church of Red Sox nation, alongside Yaz, the Kid, Pudge and Cy.
And not to be forgotten is the man behind the scenes, the quiet and unassuming surgeon who made it all possible, Dr. William Morgan, whose name will be forever linked to Curt Schilling, the Red Sox and the 2004 World Series. He may not have thrown a pitch or swung a bat, but William Morgan saved the 2004 Boston Red Sox from being another team that just missed. And he saved Red Sox fans from finally having to utter those awful words – “wait ‘til next year.” But because of Bill Morgan and the entire Red Sox medical staff, next year is this year.
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”
The American Society of Addiction Medicine’s mission is to “establish addiction medicine as a specialty recognized by professional organizations, governments, physicians, purchasers, and consumers of health care products, and the general public.”
In this they have succeeded.
And in the year 2014 Stimson’s characterization of the “impaired physician movement” remains as accurate and apt as it was in 1985. But the “number of evangelical recovered alcoholic and addict physicians” has increased dramatically (outnumbering Addiction Psychiatry by 4:1) and their involvement in “ medical society and treatment programs” has been realized and enforced through the state Physician Health Programs and their “PHP-approved’ assessment and treatment centers.
Their“ability to make authoritative pronouncements on physician impairment…based on their own claim to insider’s knowledge”has become public policy and sanctified by Regulatory Medicine.
And the 1953 Alcoholics Anonymous prophecy that “With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world” is also coming to pass.
Although no reliable statistics exist, anecdotal reports suggest an alarming upsurge in physician suicide. This necessitates a reappraisal of known predisposing risk factors such as substance abuse and depression but also requires a critical examination of what external forces or vulnerabilities might be unique to doctors and how they might be involved in the descent from suicidal ideation to suicidal planning to completed suicide.
Depression and Substance Abuse Comparable to General Population
Depression and substance abuse are the two biggest risk factors for suicide. The prevalence of depression in physicians is close to that of the general population 1,2 and, if one looks critically at the evidence based literature, substance abuse in medical professionals approximates that of the general population. Controlled studies using DSM diagnostic criteria suggest that physicians have the same rates (8-14%) of substance abuse and dependence as the rest of the population 3 and slightly lower rates compared to other occupations.4,5 Epidemiological surveys reveal the same. Hughes, et al.6 found a lifetime prevalence of drug or alcohol abuse or dependence in physicians of 7.9%, markedly less than the 14.6% prevalence reported in the general population by Kessler.7
State Physician Health Programs
Perhaps it is how physicians are treated differently when they develop a substance abuse or mental health problem.
Physician Health Programs (PHP) can be considered an equivalent to Employee Assistance Programs (EAPs) for other occupations. PHPs meet with, assess and monitor doctors who have been referred to them for substance use or other mental or behavioral health problems. Originally developed as “impaired physician” programs, the PHPs were created to help doctors who developed problems with substance abuse or addiction an alternative to disciplinary action by State Medical Boards. These programs existed in almost every state by 1980. Often staffed by volunteer physicians and funded State Medical Societies, these programs served the dual purpose of helping sick colleagues and protecting the public. Preferring rehabilitation to probation or license revocation so long as the public was protected from imminent danger, most medical boards accepted the concept with support and referrals. Most EAPs were developed with the collaboration of workers unions or some other group supporting the rights and interests of the workers. As there is no such organization representing doctors, PHPs developed in the absence of regulation or oversight. As a consequence there is no meaningful accountability.
“Because PHP practices are unknown to most physicians before becoming a client of the PHP, many PHPs operate out- side the scrutiny of the medical community at large. Physicians referred to PHPs are often compromised to some degree, have very little power, and are, therefore, not in a position to voice what might be legitimate objections to a PHP’s practices.”8
Noting that “for most physicians, participation in a PHP evaluation is coercive, and once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine,” Knight and Boyd raise serious ethical and managerial questions about current PHP policies and practice including conflicts of interest in referrals for evaluation and treatment, lack of adherence to standards of care for forensic testing of substances of abuse, violations of ethical guidelines in PHP research, and conflicts of interest with state licensing boards.
Knight and Boyd recommend “that the broader medical community begin to reassess PHP’s as a whole” and that “consideration be given toward the implementation of independent ethical oversight and establish and appeals process for PHP clients who feel they are being treated unfairly.” 8 They also recommend the relationship of PHP’s between the evaluation and treatment centers and licensing boards be transparent and that national organizations review PHP practices and recommend national standards “that can be debated by all physicians, not just those who work within PHPs.”8 Unfortunately this has not happened. Most physicians have no idea that the state physician health programs have been taken over by the “impaired physicians movement.”
In his Psychology Todayblog, Boyd again recommends oversight and regulation of PHPs. He cites the North Carolina Physicians Health Program Audit released in April of 2014 that reported the below key findings:
As with Knight and Boyd’s paper outlining the ethical and managerial problems in PHPs, the NC PHP audit finding that abuse could occur and not be detected generated little interest from either the medical community or the media.
Although state PHPs present themselves as confidential caring programs of benevolence they are essentially monitoring programs for physicians who can be referred to them for issues such as being behind on chart notes. If the PHP feels a doctor is in need of PHP “services” they must then abide by any and all demands of the PHP or be reported to their medical board under threat of loss of licensure.
LDTs bypass the FDA approval process and have no meaningful regulatory oversight. The LDT pathway was not designed for “forensic” tests but clinical tests with low risk. Some are arguing for regulation and oversight of LDTs due to questionable validity and risk of patient harm.13
These same physicians are claiming a high success rate for PH programs9 and suggesting that they be used for random testing of all physicians.14
As with LDTs, the state PHPs are unregulated, and without oversight. State medical societies and departments of health have no control over state PHPs.
Their opacity is bolstered by peer-review immunity, HIPPA, HCQIA, and confidentiality agreements. The monitored physician is forced to abide by any and all demands of the PHP no matter how unreasonable-all under the coloration of medical utility and without any evidentiary standard or right to appeal.
The ASAM has a certification process for physicians and claim to be “addiction” specialists. This “board certification” is not recognized by the American Board of Medical Specialties and is not a recognized medical specialty. The goal of the ASAM is to be recognized as the experts in addiction medicine with the consensus expert opinion based on the 12-step prohibitionist brain disease model. The ASAM has aligned itself with a number of inpatient drug treatment centers (Hazelden, Talbott, Marworth, Bradford,etc) and are heavily funded by the drug testing industry. It is in fact a “rigged game.”
State PHPs are non-profit non-governmental organizations and have been granted quasi-governmental immunity by most State legislatures from legal liability.
By infiltrating “impaired physician” programs they have established themselves in almost every state by joining, gaining power, and removing dissenters. Groupthink and 12-step indoctrination are the goals. By advertising as advocates for doctors who are “caring,” “confidential resources,” “giving help,” and advocating for “colleagues in need” the outward appearance is one of benevolence.
The biggest obstacle is that this system allows them to throw the normal rules of conduct under the imperative of a higher goal assumed to trump all other consideration. Those outside of programs either defend or ignore the reports of ethical and criminal violations, complacent in their trust of these “experts” claiming they are just helping sick doctors and protecting the public.
With no oversight or regulatory body involved this is all done with impunity, immunity, and undercover. They use the accusation of substance abuse as an indication to disregard the claims of the accused. The physician is left without rights, depersonalized, and dehumanized. The imposition of confinement, stigmatization, lack of oversight of the organizations, peer-review protected confidentiality, and lack of procedural protection is a one-way train to hopelessness and despair.
By establishing a system that of coercion, control, secrecy, and misinformation, the FSPHP is claiming an “80% success rate” 15and deeming the “PHP-blueprint” as “the new paradigm in addiction medicine treatment.
The ASAM/FSPHP had a major influence on the DSM-V where drug abuse and dependence are no longer separate entities. They are also working behind the scenes to get legislation to randomly drug test all physicians.
They are now after the “disruptive physician” and the evidentiary criteria are fairly low and red flags include “deviating from workplace norm in dress or conduct” and being tardy for meetings.
They have identified “the aging physician” as a potential problem because “as the population of physicians ages,””cognitive functioning” becomes “a more common threat to the quality of medical care.”
The majority of physicians are unaware that the Federation of State Medical Boards House of Delegates adopted an updated Policy on Physician Impairment in 2011 that uses addiction as an example of a “potentially impairing illness.” According to the Federation of State Physician Health Programs …”physician illness and impairment exist on a continuum with illness typically predating impairment, often by many years. This is a critically important distinction. Illness is the existence of a disease. Impairment is a functional classification and implies the inability of the person affected by disease to perform specific activities.”
“Process addiction” was added as a potentially impairing illness including compulsive gambling, compulsive spending, compulsive video gaming, and “workaholism.” According to the FSPHP “the presence of a process addiction can be problematic or even impairing in itself, and it can contribute to relapse of a physician in recovery. As such, process addictions should be identified and treated.” They define three levels of relapse including the novel “relapse without use.”
Bullying, Helplessness, Hopelessness and Despair
Perceived helplessness is significantly associated with suicide.16 So too is hopelessness, and the feeling that no matter what you do there is simply no way out17,18 Bullying is known to be a predominant trigger for adolescent suicide19-21 One study found that adolescents in custody who were bullied were 9.22 times more likely to attempt suicide than those were not bullied.22
Heightened perceptions of defeat and entrapment are known to be powerful contributors to suicide.23,24 The “Cry of Pain” model 25,26 specifies that people are particularly prone to suicide when life experiences are interpreted as signaling defeat which is defined as a sense of “failed struggle” or loss of social position and resources.. The person is unable to identify an escape from or resolution to a defeating situation, a sense of entrapment proliferates with the perception of no way out, and this provides the central impetus for ending ones life.
There is also evidence that rescue factors such as social supports may play a role in preventing suicide. These rescue factors act buffers to protect against suicide in the face of varying degrees of life stress.27,28 The study of female physicians revealed meetings to discuss stressful work experiences as a potential protective factor, 29 and support at work when difficulties arose appeared to be a protective factor for the male physicians.30 Research involving Finnish physicians found that control over one’s work and organizational justice were the most important determinants of work-related wellbeing.31,32 Organizational justice is related to fairness and refers to an individuals perception of an organizations behaviors, decisions, and actions and how these influence one’s own attitudes and behaviors and has been identified as a psychosocial predictor of health and wellbeing3334 Low organizational justice has been identified as a notable risk factor for psychological distress and depression.35,36
A recent report indicates that job stress, coupled with inadequate treatment for mental illness may play a role in physician suicide..
Using data from the National Violent Death Reporting System the investigators compared 203 physicians who had committed suicide to more than 31,000 non-physicians and found that having a known mental health disorder or a job problem that contributed to the suicide significantly predicted being a physician.1
Physicians were 3.12 times more likely to have a job problem as a contributing factor. In addition, toxicology testing showed low rates of medication treatment. The authors concluded that inadequate treatment and increased problems related to job stress are potentially modifiable risk factors to reduce suicidal death among physicians.
They also warned that the database used likely underestimated physician suicides because of “underreporting and even deliberate miscoding because of the stigma attached.”
I can think of nothing more institutionally unjust than an unregulated zero-tolerance monitoring program with no oversight using unregulated drug and alcohol testing of unknown validity.
We have heard of numerous suicides due to these institutionally unjust programs. Three doctors died by suicide in Oklahoma in a one month period alone (August 2014). All three were being monitored by the Oklahoma PHP. I went to an all boys high-school of less than 350 students yet a classmate a couple years ahead of me died by suicide a few months ago. He was being monitored by the Washington PHP. His crime? A DUI in 2009–a one-off situational mistake that in all likelihood would never have recurred. But as is often the case with those ensnared by state PHPs he was forced to have a “re-assessment” as his five-year monitoring contract was coming to an end. These re-assessments are often precipitated by a positive Laboratory Developed Test (LDT) and state medical boards mandate these assessments can only be done at an out-of-state “PHP-approved” facility. Told he could no longer operate and was unsafe to practice medicine by the PHP and assessment center he then hanged himself. And at the conclusion of Dr. Pamela Wible’s haunting video below are listed just the known suicides of doctors; many were being monitored by their state PHPs–including the first name on the list– Dr. Gregory Miday.
None of these deaths were investigated. None were covered in the mainstream media. These are red flags that need to be acknowledged and addressed! This anecdotal evidence suggests the oft-used estimate of 400 suicides per year (an entire medical school class) is a vast underestimation of reality—extrapolating just the five deaths above to the entire population of US doctors suggests we are losing at least an entire medical school per year.
As physicians we need to demand transparency, oversight, regulation and auditing by outside groups. This is a public health emergency.
To wit:
They first came after the substance abusers and I did not speak out because I was not a substance abuser.
They then came for those with psychiatric diagnoses and I did not speak out because I was not diagnosed with a psychiatric disorder.
They then came after the “disruptive physician” and I did not speak out because I was not disruptive.
They then came after the aging physician and I did not speak out because I was young.
They then came after me and there was no one else to speak out for me.
Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the precursors study. Archives of internal medicine. Jul 13 1998;158(13):1422-1426.
Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. The American journal of psychiatry. Dec 1999;156(12):1887-1894.
Brewster JM. Prevalence of alcohol and other drug problems among physicians. JAMA : the journal of the American Medical Association. Apr 11 1986;255(14):1913-1920.
Anthony J, Eaton W, Mandell W, al. e. Psychoactive Drug Dependence and abuse: More Common in Some Occupations than in Others? Journal of Employee Assistance Res. 1992;1:148-186.
Stinson F, DeBakely S, Steffens R. Prevalence of DSM-III-R Alcohol abuse and/or dependence among selected occupations. Alchohol Health Research World. 1992;16:165-172.
Hughes PH, Brandenburg N, Baldwin DC, Jr., et al. Prevalence of substance use among US physicians. JAMA : the journal of the American Medical Association. May 6 1992;267(17):2333-2339.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. Jun 2005;62(6):593-602.
Boyd JW, Knight JR. Ethical and managerial considerations regarding state physician health programs. Journal of addiction medicine. Dec 2012;6(4):243-246.
DuPont RL, McLellan AT, White WL, Merlo LJ, Gold MS. Setting the standard for recovery: Physicians’ Health Programs. Journal of Medical Regulation. Mar 2010;95(4):10-25.
Skipper GE, Weinmann W, Thierauf A, et al. Ethyl glucuronide: a biomarker to identify alcohol use by health professionals recovering from substance use disorders. Alcohol and alcoholism. Sep-Oct 2004;39(5):445-449.
Skipper GE, Thon N, Dupont RL, Baxter L, Wurst FM. Phosphatidylethanol: the potential role in further evaluating low positive urinary ethyl glucuronide and ethyl sulfate results. Alcoholism, clinical and experimental research. Sep 2013;37(9):1582-1586.
Skipper GE, Thon N, DuPont RL, Campbell MD, Weinmann W, Wurst FM. Cellular photo digital breathalyzer for monitoring alcohol use: a pilot study. European addiction research. 2014;20(3):137-142.
Sharfstein J. FDA Regulation of Laboratory-Developed Diagnostic Tests: Protect the Public, Advance the Science. JAMA : the journal of the American Medical Association. Jan 5 2015.
Pham JC, Pronovost PJ, Skipper GE. Identification of physician impairment. JAMA : the journal of the American Medical Association. May 22 2013;309(20):2101-2102.
McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. Bmj. 2008;337:a2038.
Rivers I, Noret N. Potential suicide ideation and its association with observing bullying at school. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S32-36.
Lester D, Walker RL. Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega. 2007;55(4):321-324.
Beck AT. Hopelessness as a predictor of eventual suicide. Annals of the New York Academy of Sciences. 1986;487:90-96.
Hinduja S, Patchin JW. Bullying, cyberbullying, and suicide. Archives of suicide research : official journal of the International Academy for Suicide Research. 2010;14(3):206-221.
Hertz MF, Donato I, Wright J. Bullying and suicide: a public health approach. The Journal of adolescent health : official publication of the Society for Adolescent Medicine. Jul 2013;53(1 Suppl):S1-3.
Kim YS, Leventhal B. Bullying and suicide. A review. International journal of adolescent medicine and health. Apr-Jun 2008;20(2):133-154.
Kiriakidis SP. Bullying and suicide attempts among adolescents kept in custody. Crisis. 2008;29(4):216-218.
Taylor PJ, Gooding P, Wood AM, Tarrier N. The role of defeat and entrapment in depression, anxiety, and suicide. Psychological bulletin. May 2011;137(3):391-420.
Lester D. Defeat and entrapment as predictors of depression and suicidal ideation versus hopelessness and helplessness. Psychological reports. Oct 2012;111(2):498-501.
Williams JMG. Cry of Pain. Harmondsworth: Penguin; 1997.
Williams JMG, Crane C, Barnhofer T, Duggan DS. Psychology and suicidal behavior: elaborating the entrapment model. In: Hawton K, ed. Prevention and treatment of suicidal behavior: from science to practice. Oxford: Oxford University Press; 2005:71-89.
Borowsky IW, Ireland M, Resnick MD. Adolescent suicide attempts: Risks and protectors. Pediatrics. 2001;107(485).
Clum GA, Febbraro GAR. Stress, social support and problem-solving appraisal/skill: Prediction of suicide severity within a college sample. Journal of Psychopathology and Behavioral Assessment. 1994;16:37-46.
Fridner A, Belkic K, Marini M, Minucci D, Pavan L, Schenck-Gustafsson K. Survey on recent suicidal ideation among female university hospital physicians in Sweden and Italy (the HOUPE study): cross-sectional associations with work stressors. Gender medicine. Apr 2009;6(1):314-328.
Fridner A, Belkic K, Minucci D, et al. Work environment and recent suicidal thoughts among male university hospital physicians in Sweden and Italy: the health and organization among university hospital physicians in Europe (HOUPE) study. Gender medicine. Aug 2011;8(4):269-279.
Lindfors PM, Meretoja OA, Toyry SM, Luukkonen RA, Elovainio MJ, Leino TJ. Job satisfaction, work ability and life satisfaction among Finnish anaesthesiologists. Acta anaesthesiologica Scandinavica. Aug 2007;51(7):815-822.
Heponiemi T, Kuusio H, Sinervo T, Elovainio M. Job attitudes and well-being among public vs. private physicians: organizational justice and job control as mediators. European journal of public health. Aug 2011;21(4):520-525.
Elovainio M, Kivimaki M, Vahtera J. Organizational justice: evidence of a new psychosocial predictor of health. Am J Public Health. Jan 2002;92(1):105-108.
Lawson KJ, Noblet AJ, Rodwell JJ. Promoting employee wellbeing: the relevance of work characteristics and organizational justice. Health promotion international. Sep 2009;24(3):223-233.
Hayashi T, Odagiri Y, Ohya Y, Tanaka K, Shimomitsu T. Organizational justice, willingness to work, and psychological distress: results from a private Japanese company. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. Feb 2011;53(2):174-181.
Lang J, Bliese PD, Lang JW, Adler AB. Work gets unfair for the depressed: cross-lagged relations between organizational justice perceptions and depressive symptoms. The Journal of applied psychology. May 2011;96(3):602-618.


 The sociopaths responsible for ordering false assessments and falsified drug and alcohol testing as well as those complying with it in the drug and alcohol testing, assessment and treatment industry need to be held accountable.
The sociopaths responsible for ordering false assessments and falsified drug and alcohol testing as well as those complying with it in the drug and alcohol testing, assessment and treatment industry need to be held accountable.