Pharmacard: A Prescription Drug Monitoring System Designed to Record Drug Histories and Reduce the Incidence of “Drug Misadventuring.”
As a medical student in 1990 I saw a 79 year old woman in the emergency room with intractable nausea and vomiting. Earlier that week she had seen her primary care physician for nausea and a mild cough. Diagnosed with bronchitis, she was given a prescription for erythromycin. Her husband brought in her medications including digoxin which can cause nausea
when blood levels are too high. A markedly high level came back on the blood draw indicating digitalis toxicity. I spoke to her primary care physician who was unaware of her digoxin prescription; completely clueless that she was prescribed the foxglove plant extract by a cardiologist for an irregular heart beat.
Digitalis was first described by William Withering in 1785 for heart conditions and this is considered the beginning of modern therapeutics. Sometime after erythromycin became available in 1952 it was discovered that taking the two drugs together increased digoxin levels. This simplest type of drug interaction is called interference and occurs when one drug either accelerates of slows down the metabolism or excretion of the other.
Based on the progression of symptoms her husband reported and the elevated levels on admission this woman undoubtedly had elevated digitalis levels when she was seen by her doctor earlier in the week. Unaware of the digitalis he inadvertently worsened her condition by giving her a medication that elevated her levels even further. She was lucky.
The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).
Digitalis toxicity in those who die outside of the hospital often goes unrecognized as most are elderly and assumed to have died from age related causes.
Seeing several more cases of drug related problems caused by ignorance of current medications and lack of communication prompted an interest in drug misadventures. I also became interested in developing a computerized up to date and accurate record accessible by all health care providers in real time , a closed loop system of “portable” information easily transferred among all health care providers be they primary doctors, pharmacists or emergency room personnel.
Research pharmacologist Dr. Edward Gallaher and I brainstormed over ideas and eventually came up with a computer program using WORM (write-once-read-many) optical technology used in compact disc systems. much like a CD-R but without the spinning disc. The credit-card sized disk could store up to two megabytes of data on an optical layer that could be written once and never changed. An optical card-reader interfaced with any IBM compatible PC. The plan was to place card readers at pharmacies, medical offices and emergency rooms. We called it Pharmacard.
Pharmacard System Developed. ASTI Connections. Vol 4. Eugene, OR: Advanced Science and Technology Institute; 1992.
Although computerized medical records existed in 1992 they were predominantly stand alone with many just replicating the paper record without word search capability. Moreover these programs did not communicate with one another so no information portability existed between the entities involved. Communication of information from pharmacy to doctors to emergency room was not an option. The system was fragmented and the search for information long.
But drug mishaps were a real problem. As with digoxin they could be fatal. Multiple reports of drug induced morbidity and mortality were found in literature searches. An obvious problem existed. . Many were drug interactions such as that with digitalis and erythromycin. From my viewpoint the need for addressing the problems caused by inadequate and and incomplete records was not only self-evident but a priority. Solutions however were few. “Brown-bag” sessions in which patients bring in a paper bag containing all of their meds were held periodically. Little booklets titled “patient medication records” were given to patients to update and record their new and current prescriptions.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
An available baseline EKG was decided based on its presence making it much easier to detect a problem by looking for differences. A baseline EKG would conceivably facilitate the timing and accuracy of diagnosis. In addition it would save money because without a comparison the default is admission.
We then applied for multiple research grants for funding to do a pilot study. All were rejected and contained comments suggesting we pitch our wares to the computer people not the medical people-this is computer science not medical science.
We received very little interest at an AMA poster presentation in Washington D.C. Few people would even read the poster with most taking a quick glance and redirecting straight ahead as if they were avoiding a street-corner pollster. Those who did read it were either non-plussed, perplexed or cynical.
A research psychopharmacologist M.D.,PhD from France asked permission to give me some advice. He then told me it would not work. He said the idea was great, it would work as intended and probably help prevent drug related problems. But that did not matter because no one
gets it yet.”
Aside from a handful of people intimately involved in the research most everyone else finds this useless as do most people at the conference. This means nothing to them.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
In 1999 the Institute of Medicine published To Err is Human: Building a Safer Health Care System placing patient safety high on the nation’s health care agenda. Medical errors, adverse drug reactions and interactions were deemed a big problem. Identifying ways to keep track of medications became a priority and multiple business ventures popped up and got their hats in the ring. Suddenly everyone not only recognized the problem but imparted the sense they knew it all along. Seven years had gone by and our project had then fallen by the wayside. In addition our optical platform was obsolete.
As with firefighter arson this illustrates the most crucial step in addressing a problem is admitting the problem exists. Firefighter arson had been documented for over a century but not properly addressed. The extent of the problem was not publicly recognized until a Special Report: Firefighter Arson was done by the Department of Homeland Security, the United States Fire Administration and the National Fire Data Center in 2003. The most crucial step was admitting the problem exists. The second was defining the problem. The third was having zero tolerance for those engaged in the problem. States that have taken this approach have found a marked reduction in firefighter arson.
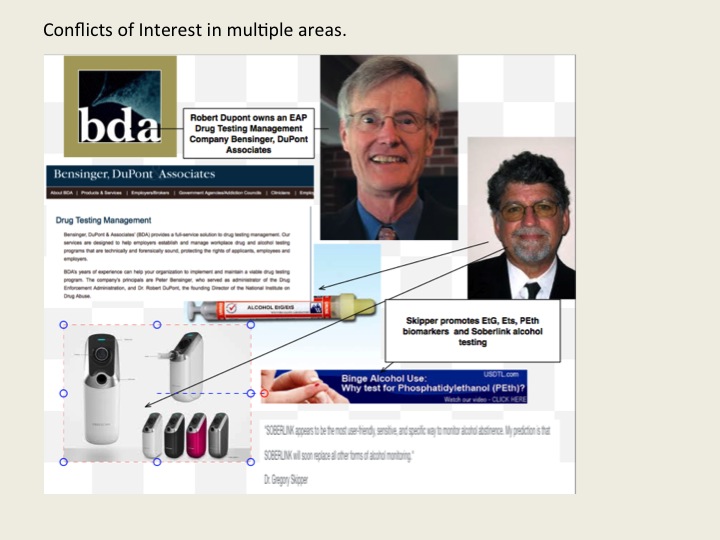
The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.
Skipper’s introduction of junk science drug and alcohol testing and use of cutoff points he pulls out of a hat and then moves upward as the problems are exposed is shameful. The fact that he unleashed this on other doctors knowing full well what would happen in a zero tolerance program needs to be revealed.
My survey is revealing many suicides as a direct result of these tests, including those of medical students and residents. And most of those who have died were not even remotely addicts or alcoholics. They were reported anonymously, given one of these tests and asked to be evaluated at a “PHP-approved” assessment center where a diagnosis was confirmed followed by 3-4 months of inpatient treatment. I am finding out most of the doctors referred to PHPs do not have any problems but the PHPs and their affiliates are giving false diagnoses, false drug testing and using threats to control them and there is little they can do about it. Skipper’s complete lack of empathy for his victims as he continues to put coins in his purse is abhorrent. Meanwhile the death count continues to rise.
The article below was published in the now defunct magazine Gray Areas almost twenty years ago. (Vol. 4, No. 1, Spring 1995 pp. 75-77). It is not a research article but a critique of the use of polygraphy written for a general audience.
Antipolygraph.org founder George Maschke noted in 2008 that the article “makes a good introduction to the pseudoscience of polygraphy” and “the criticisms of polygraphy remain valid today.” The basic assumption of any good test is that is has construct validity; that it is actually measuring what it is purported to measure. Polygraphy is purported to detect lies but the specificity and sensitivity are about the same as a toss of a coin and has the potential to cause a great deal of harm to those who are judged dishonest by its results. Heads I win, tails you lose.
In the article I suggest that state laws regarding polygraph use must change and call upon the medical and scientific communities to educate lawmakers and policy makers about the absence of construct validity in this pseudoscientific instrument and “put the greater than 3000 anachronistic polygraph examiners in the United States out of business.” The Employee Polygraph Protection Act of 1988 (EPPA) generally prevents employers from using polygraphs for pre-employment screening or during the course of employment, A 2003 report by the National Academy of Sciences found that the majority of polygraph research was “unreliable, unscientific and biased.” In 2004 the American Psychological Association (APA) issued a position paper finding little evidence to support polygraphy in detecting deception concurring with the 1986 American Medical Association’s (AMA’s) Council on Scientific Affairs conclusions that there is little evidence base for this test and it is unscientifically supportable.
Alas, in 2016 the polygraph examiners are still in business and there are now approximately 5000 of them. The American Polygraph Association is still claiming 90% accuracy and the test is used extensively by prosecutors, defense attorneys, and law enforcement agencies. In U.S. courts judges have expanded the instances in which polygraph testing is mandated or admitted as evidence.
The Employee Polygraph Protection Act of 1988 (EPPA) applies only to private industry, not the government and, ironically, state medical boards and their national organization,, the Federation of State Medical Boards condone their use on medical doctors despite the fact that the American Medical Association likened their accuracy to a coin-toss and recommended against their use in the 1980s. This is due to the influence of the Federation of State Physician Health Programs (FSPHP). The alliance between the FSMB and FSPHP has resulted in bad policy and decision making as physician health programs have bamboozled medical boards into complete deference to their perceived authority and expertise in evaluating physicians for just about anything. This has resulted in the acceptance of non-FDA approved drug and alcohol testing, non-validated psychological instruments and lie-detectors. Polygraphs serve an important purpose for those involved in the PHP and rehab racket. They are used in disruptive physician evaluations to “confirm” (i.e. “tailor”) diagnoses in physicians referred to gulags such as Acumen, the Professional Renewal Center and Vanderbilt. Polygraphs and adherence to 12-step doctrine is also being used as leverage to regain medical licenses and apparently the medical boards agree with this methodology.
Take for instance, Dr. James Peak, M.D., a child psychiatrist who was sent to prison on a federal child pornography conviction and taken under the wing of the Montana PHP. Michael J. Ramirez, clinical coordinator for the Montana Professional Assistance Program, says “Peak’s remorse for his crimes is genuine.” Peak, who primarily saw adolescent boys in his practice maintains he only looked at child pornography of young boys but never physically abused any and a polygraph confirmed that he was only a “looker” but never a “toucher.” He spent just 10 months in Federal prison for a crime that could get up to ten years and thanks to the PHP his license was reinstated lickety-split.
Peak’s treatment includes going to one AA meeting and one 12-step sex addict meeting per week.
Legitimate policy must be based on recognized institutions and experts. The science must be reliable and unbiased. Regulatory changes demand methodologically sound science and evidence-based facts arrived at through rigorous peer review and professional. Decision are currently being made by illegitimate carney hucksters and irrational clowns.
The Art of Deception: Polygraph Lie Detection
By Michael Lawrence Langan, M.D.
I’d swear to it on my very soul, If I lie, may I fall down cold.”
– Rubin and Cherise
(Hunter/Garcia)
The accuracy of polygraphic lie detection is slightly above chance. Nevertheless, State and local police departments and law enforcement agencies across the United States are devoted proponents of this unscientific and specious device. In addition, the American public seems to lend an implicit credence to the “lie detector” as evinced by its ubiquitous use on television crime shows and in “whodunit” literature. It is given overt attributions of credibility on tabloid type talk shows and news shows. For example, in the highly publicized case of Tonya Harding a reporter stated, not with removed objectivity but with sardonic grin and mocking emphasis, that the accused had failed two polygraph tests. The implied assumption is that if the person has failed the polygraph test, then therefore he or she is guilty regardless of other evidence. Bottom line. Culpa ex machina. End of story.
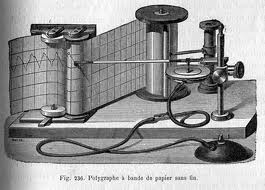
Lie detection by the polygraph is based on the premise that the act of telling a lie causes specific, universal, and reproducible physiological responses as manifested by the autonomic nervous system. (Saxe, 1991) These physiological responses, which are largely outside the influence of voluntary control, are then measured by the polygraph instrument. The polygraph itself is simplistic in design. It consists of several devices which are attached to the subject to record blood pressure, pulse, respiration, and galvanic skin response (which is related to perspiration). The results are then recorded on a moving paper by a “kymograph.” Hence any change of one of the autonomic nervous system variables will be recorded on the paper as a change from baseline. The polygraph examiner then interprets the tracing. A characteristic change from baseline on a relevant question is interpreted as a lie.
In fact, the polygraph test does measure autonomic nervous system activity. The role of the autonomic nervous system with its sympathetic and parasympathetic branches is well defined within the field of medicine, and was well described by the French physician Claude Bernard over a century ago. The primary role of the autonomic nervous system is to maintain bodily homeostasis to allow the individual to exist in a changing environment.
Simplistically described, the autonomic nervous system is a part of the peripheral nervous system which consists of a variety of outgoing nerve pathways that regulate important physiological functions generally outside of voluntary and conscious control. Thus, respiration, body temperature, heart rate, digestion, sweating, and blood pressure are all, partly or entirely, regulated by the autonomic nervous system. It is divided into sympathetic and parasympathetic branches which have contrasting functions in terms of effect. The sympathetic branch increases heart rate, respiratory rate, blood pressure, and perspiration. It is active at all times but varies with the constantly changing environment, and is especially active during rage or fright and prepares the body for the so called “fight or flight” phenomenon. Many of these reactions are caused by the release of epinephrine. The parasympathetic nervous system, on the other hand, is primarily involved with conservation and restoration. It is the sympathetic branch of the autonomic nervous system that the polygraph measures in terms of its activity. Thus, from a medical perspective it is entirely valid that the polygraph will accurately measure sympathetic nervous system activity with its instrumentation.
The false assumption of the polygraph test is that dishonesty is the sole cause of sympathetic arousal during a polygraph examination. Deception is a cognitive phenomenon that cannot be measured. Indeed, throughout the entire history of medicine there has not been a single scientific study that demonstrated evidence that a cognitive phenomenon (such as love, hatred, truth, altruism, jealousy) could be measured. Since, in the complex realm of truth and deception, there is no known physiological response that correlates with lying, then there is no validity to the test. Although the act of lying can elicit fear and anxiety via the sympathetic nervous system, so can multiple other confounding and complex emotional factors including stress, embarrassment, anger, and fear. “Deception itself cannot be measured directly.” (Steinbrook, 1992) In addition, each individual differs in autonomic lability. Some people stay calm with a gun at their head. While others get autonomically excited, with heart thumping and palms sweating at simply shaking someone’s hand.
In reality, the examination itself is inherently designed to elicit fear and anxiety. It is an interrogation. If this fear and anxiety are recorded on a relevant question, then you have failed that question according to the polygraph “experts.”
The polygraph technique begins with a pre-test. After a sixth-grade level lecture on the nervous system and a proclamation of the test’s infallibility, the examiner will go over all of the questions that have been formulated.
These questions consist of control questions, relevant questions, and irrelevant questions. The subject will then be attached to the polygraph equipment and the formal testing begins.
The most crucial questions on the polygraph examination, or “Control Question Test,” are the control questions and relevant questions. The control questions are garnered from the suspect by asking him an innocuous question which could not be truthfully denied. For example, “Have you ever thought of hurting someone?” or “Have you ever lied to anyone?” The responses to the control questions will elicit some degree of autonomic activity which can then serve as a baseline for which to compare subsequent questions. The relevant questions pertain to the actual investigation at hand. The magnitude of responses to relevant questions and control questions as compared with the irrelevant questions is then interpreted, in a non-blinded manner, by the examiner. The assumption is, that if you are prevaricating, the relevant questions will cause a greater response than the control questions. So if the question “Have you ever been late for an appointment?” (control question) elicits less of an emotive response on the polygraph equipment than “Did you murder and rape your girlfriend?” (relevant question) you have failed the test. And, according to the American Polygraph Association (APA) you are lying. Assuming the subject is innocent, it is fairly obvious that he would respond with more emotional autonomic activity to a question regarding a recently deceased loved one than he would an inquiry about punctuality. Obvious to everyone, that is, but the APA.
The APA is a professional organization for polygraph examiners who have complete faith in the accuracy of the test. They have their own trade journal Polygraph in which they report scientifically worthless studies and brandish anecdotes of the wonders of their trade. The majority of these members can pride themselves on completing a 6 week to 6 month post- high school training course in the art of polygraphy. They have no formal training in medicine, psychology, physiology, or behavior; the very disciplines on which the testing is based. The majority of them cater to the legal system wherein their economic livelihood depends.
Since they are primarily paid to identify guilty suspects, motivational factors may play a part in their eagerness to find the guilty suspect. (Kleinmuntz, 1987)
The accuracy of any test is determined by that test’s sensitivity (ability to find a positive) and specificity (ability to find a negative). A polygraph examiner will ardently tell you that the exam has somewhere in the neighborhood of a 95% sensitivity rate. This means that if 100 guilty suspects are given a polygraph exam, 95 of them will be detected through the test. Only five of the 100 will be a false negative and not be detected by this miraculous method. Likewise they will claim a similar specificity rate, and state that if you are telling the truth then you have almost a 100% chance of being cleared by the test. John Reid, the inventor of the Control Question Test claimed 99% accuracy. (Reid and Inbau, 1977)
This is clearly not accurate. The polygraph was not subjected to much critical and scientific investigation until the last two decades. (Saxe, et al., 1983) Since this time there have been a number of studies of sound scientific design and methodology which clearly refute the high specificity and sensitivity that polygraph advocates claim. These studies have appeared in reputable peer-reviewed journals and not trade publications. Horvath, for example, reported a sensitivity of 76 percent and a specificity of 52 percent. (Horvath, 1977) This means that out of 100 liars 76 of them will be detected by the polygraph. What is astonishing though is the specificity of 52 percent. This means that out of 100 people who are not lying, 52 will be identified as telling the truth while 48 of the honest individuals will be branded as liars. The odds are similar to that of a coin toss which would have a specificity of 50 percent. Barland and Raskin’s study actually demonstrated a specificity of 45%. Worse than a coin toss. (Barland and Raskin, 1976) Multiple other studies have shown similar results. (Brett, et al., 1986, Kleinmuntz and Szucko, 1984, Lykken, 1984).
The polygraph examiner likens his “skill” to that of the radiologist reading a chest X-Ray or a cardiologist interpreting an EKG. (Barefoot, 1974) This analogy is not only ridiculous but, in fact, if a medical test had a similar sensitivity and specificity to that of the polygraph examination it would simply not be used in the field of medicine. They will cite the fact that the polygraph has been used in the United States for greater than 70 years as if longevity is directly related to validity. They will state that they have personally administered hundreds or thousands of these tests, and have almost never been wrong, as if total number of tests given constitutes accuracy.
They are so convinced of the accuracy of the polygraph that they regard opponents of polygraphy as communists and do-nothing professors. (Arther, 1986) It doesn’t occur to them that someone with a Ph.D. and years of research experience, in the very subjects they ignorantly dabble in, may know something more than they do.
It is astounding that the criminal justice system has institutionalized and perpetuated a so called “technology” that lacks scientific evidence and is in fact rejected by the scientific community. It is as ludicrous as procuring the so called “love meter” machine from the amusement park which measures galvanic skin response and placing it in the courtroom. But in a backward legal system which has been known to use psychics to help with unsolved murders and has allowed the mentally retarded to serve as jurors, it is not entirely surprising.
The tool is useful to them, however, in that 25 to 50 percent of examinees will, under the tense psychological pressure of the exam, confess to the misdeed at hand. (Lykken, 1981, Lykken, 1991) Persuaded that they have been proven dishonest by “scientific” means they give up hope. It is usual for the polygraph examiner to interrogate the subject who has failed the test. They will state that there is no way now to deny the objective guilt demonstrated by this impartial and unbiased scientific device, and that the only available option is to confess.
The assessment by the polygrapher is genuinely convincing because, sadly, he believes it himself. Thus the instrument is clearly useful as a confession inducing device. One wonders, over the past 70 years, how many false confessions have been obtained in this way from innocent persons.
In summary, the polygraph is a ludicrous implementation of pseudo-science at its worst. The members of the APA are non-scientists practicing science, and the consequences are often dire. Lykken reports the cases of three men who were convicted of murder largely due to the polygraph examiner’s testimony that in their “expert opinion” they had failed the test. All three were subsequently found to be innocent. (Lykken, 1991) Polygraph examiners ignore such cases or rationalize that they are due to the rare incompetence of some examiners.
The continued use of polygraphic lie detection has the potential to cause much harm to those who are judged dishonest by its results. The specificity and sensitivity are not dissimilar to that of a coin toss. Innocent suspects have about a 50/50 chance. One failure is all it takes to ruin your life. Since the 1923 Federal Court decision of Frye vs United States (293 F 1013 [DC Cir 1923]), polygraph evidence has not been admissible in federal court cases because there was deemed a lack of scientific validity to the test. This travesty however is still used widely by the state court system. Furedy characterizes the continued use of polygraphy as a serious “social disease.” (Furedy, 1987) State laws regarding abuse of the polygraph must change, and it is time for the medical and scientific communities to educate lawmakers and policy makers about the true validity of this perversion of science. It must be forever banished to the same realm of parapsychology as the Ouija Board, phrenology, and palmistry. The relatively conservative American Medical Association’s Council on Scientific Affairs recommended that the polygraph not be used in pre-employment screening and security clearance. (Council on Scientific Affairs, 1986) It is time to extend this recommendation across the board, and put the greater than 3000 anachronistic polygraph examiners in the United States out of business.
Meanwhile, if you are asked to take a polygraph test–don’t do it. Those involved in the criminal justice system, including lawyers, are largely uneducated in the realm of scientific scrutiny and experimental methodology.
They may not separate science and pseudo-science, and erroneously believe that the polygraph is an accurate scientific instrument. Their interactions are with polygraph examiners who proselytize its use, and they have little or no interaction with scientists, psychologists, and physicians who refute its use. Refuse to take the test and educate them. Cite the Frye doctrine, go to the medical library, copy the scientific articles which belie its validity, and present them to whomever requested you to take the test. State that the principles and assumptions underlying polygraphy are not supported by our understanding of psychology, neurology, and physiology. Then put the burden of proof on their heads. Tell them to present you with scientific evidence that corroborates the validity of the test. There is simply no rational basis for a machine to detect liars.
References
Arther RO. 1986. The polygraph’s enemies: An update. Journal of Polygraph Science. 20: 133-136.
Barefoot J. 1974. The Polygraph Story. Cluett Peabody and Co., New York.
Barland, G, Raskin D. 1976. Validity and reliability of polygraph examinations of criminal suspects (Report 76-1, Contract 75 NI-99-0001).
Brett AS, Phillips M, Beary JF. 1986. Predictive power of the polygraph: Can the “lie detector” really detect liars? The Lancet. 1: 544-547.
Council on Scientific Affairs. 1986. Polygraph. Journal of the American Medical Association. 256: 1172-1175.
Furedy JJ. 1987. Evaluating polygraphy from a psychophysiological perspective: a specific-effects analysis. Pavlovian Journal of Biological Sciences.22: 145-151.
Horvath F. 1977. The effect of selected variables on interpretation of polygraph records. Journal of Applied Psychology. 62: 127-136.
Kleinmuntz B. 1987. The predictive power of the polygraph: The lies lie detectors tell. Journal of the American Medical Association. 257: 189-190.
Kleinmuntz B, Szucko J. 1984. A field study of the fallibility of polygraphic lie detection. Nature. 308: 449-450.
Lykken D. 1984. Polygraph Interrogation. Nature. 307: 681-684.
Lykken DT. 1981. A tremor in the blood: Uses and abuses of the lie detector. McGraw-Hill, New York.
Lykken DT. 1991. Why (some) Americans believe in the lie detector while others believe in the guilty knowledge test. Integrative Physiological and Behavioral Science. 26: 214-222.
Reid JE, Inbau FE. 1977. Truth and deception: The polygraph (“lie detector”) technique. Williams & Wilkins, Baltimore.
Saxe L. 1991. Science and the CQT polygraph: A theoretical critique. Integrative Physiological and Behavioral Science. 26: 223-231.
Saxe L, Dougherty D, Crosse T. 1983. Scientific validity of polygraph testing: a research review and evaluation. Conference: OTA-TM. U.S. Congress Office of Technology Assessment.
Steinbrook R. 1992. The polygraph test – A flawed diagnostic method. The New England Journal of Medicine. 327: 122-123.
“While certification does not certify clinical skill or competence,” the Board explained, “it does identify physicians who have demonstrated knowledge in diagnosis and treatment of alcoholism and other drug dependencies.”
“With one arm around the shoulder of religion and the other around the shoulder of medicine, we might change the world.”—Twelve Steps and Twelve Traditions, AA World Services, Inc (1953).
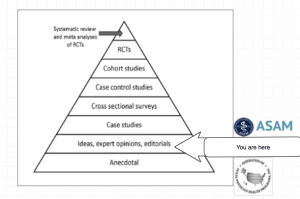
In order to comprehend the current plight of the medical profession and the dark clouds that lie ahead it is necessary to understand the history of the “impaired physician movement” and the American Society of Addiction Medicine (ASAM).
In 1985 the British sociologist G. V. Stimson wrote:
“The impaired physician movement is characterized by a number of evangelical recovered alcoholic and addict physicians, whose recovery has been accompanied by an involvement in medical society and treatment programs. Their ability to make authoritative pronouncements on physician impairment is based on their own claim to insider’s knowledge.”1
The impaired physician movement emphasizes disease and therapy rather than discipline and punishment and believes that addiction is…
One thing is for certain. When society gives power of diagnosis and treatment to individuals within a group schooled in just one uncompromising model of addiction with the majority attributing their very own sobriety to that model, they will exercise that power to diagnose and treat anyone and everyone according to that model. The birth of Addiction Medicine as an ABMS accepted discipline is sure to be a success for the drug and alcohol testing and 12-step treatment industry, but its spawn is sure to be an inauspicious mark on the Profession and Guild of Medicine and a bane of society for years to come.
Educational and Professional Standards in Medical Specialties and Subspecialties
The increasingly rapid growth and complexity of medical knowledge in twentieth century American medicine resulted in the creation of specialties and subspecialties.
A related development was the creation of “boards” to “certify” physicians as knowledgeable and competent in the specialties and subspecialties in which they claimed to have expertise. The American Board of Ophthalmology, organized in 1917, was the first of these.
As the number of medical specialties proliferated an umbrella organization was formed to accomplish this task. The Advisory Board for Medical Specialties was created in 1933 and reorganized as the American Board of Medical Specialties (ABMS) in 1970. This non-profit organization oversees board certification of all physician specialists and sub-specialists in the United States.
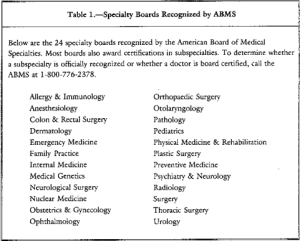
The ABMS recognizes 24 medical specialties in which physicians can pursue additional training and education to pursue Board Certification.
There is enormous inertia—a tyranny of the status quo—in private and especially governmental arrangements. Only a crisis—actual or perceived—produces real change. When that crisis occurs, the actions that are taken depend on the ideas that are lying around. That, I believe, is our basic function: to develop alternatives to existing policies, to keep them alive and available until the politically impossible becomes politically inevitable.-Milton Friedman
“It is easier to believe a lie one has heard a hundred times than a truth one has never heard before.” –Robert S. Lynd
1980s–Your Money or Your Medical License
Ridgeview Institute was a drug and alcohol treatment program for “impaired physicians” in Georgia created by G. Douglas Talbott, a former cardiologist who lost control of his drinking and recovered through the 12-steps of Alcoholics Anonymous. Up until his death on October 18, 2014 at the age of 90, Talbott owned and directed a number of treatment facilities for impaired…
State physician health programs (PHPs) play a key role in helping doctors with substance abuse problems. But the current PHP system is inconsistent and prone to potential conflicts of interest and ethical issues, according to a new review.
The review is available as publish ahead of print content from the December 2012 issue of Journal of Addiction Medicine, the official journal of the American Society of Addiction Medicine. The journal is published by Lippincott Williams & Wilkins, a part ofWolters Kluwer Health.
In the article, Drs J. Wesley Boyd and John R. Knight of Harvard Medical School point out “substantial variability in states’ PHP policies and practices, often raising serious ethical and managerial questions.” Collectively the authors served as PHP associate directors for more than 20 years; based on that experience they write, “We recommend that the broader medical community begin to reassess PHPs as a whole in an objective and thoughtful manner.”
‘Coercive’ Nature of PHP System Raises Ethical and Managerial Issues
Most states currently have PHPs, which help physicians with substance abuse disorders. State PHPs meet with, assess, and monitor doctors referred for substance abuse or other mental and behavioral health problems. hey also make provisions for follow-up and monitoring of treated physicians, including random drug testing.
The PHP system achieves good results in treating substance abuse disorders in physicians, with much higher success than reported for other groups of patients. However, Drs Boyd and Knight identify several ethical concerns related to the “coercive” nature of the system. They write, “Once a PHP recommends monitoring, physicians have little choice but to cooperate with any and all recommendations if they wish to continue practicing medicine.”
One issue is the high cost of evaluation and treatment. Insurance sometimes does not reimburse physicians for evaluations recommended by PHPs — a cost sometimes exceeding $4,500. If treatment is recommended, the cost may be prohibitive: as high as $39,000 for a “standard” 90-day length of treatment. That’s much longer than the 20- to 28-day stay typical for other patients undergoing substance abuse treatment — despite a lack of evidence that health care professionals need longer treatment.
Many centers who provide PHP-recommended evaluations also provide treatment, thus raising the potential for financial incentives for treatment recommendations. Drs Boyd and Knight note that close relationships between treatment centers and state PHPs are “replete with potential conflicts of interest.”
The authors also point out problems related to the practice of some PHPs that “any and all” positive test results be reported to the state licensing board — even if they don’t indicate substance abuse or relapse. Today’s highly sensitive tests can give a positive result even in a person who has used alcohol-based hand sanitizer, as well as some types of asthma inhalers and pain medications. PHPs may instruct doctors to avoid these exposures to simplify interpretation of test results, “rather than what might be in the best interests of the physician.”
Use of information about physicians in research by PHPs and their closely intertwined relationships with state licensing boards raise concerns as well. Because most doctors know little about them, PHPs “operate outside the scrutiny of the medical community at large,” the authors write. “Physicians referred to PHPs are often compromised to some degree, have very little power, and are therefore not in a position to voice what might be legitimate objections to a PHP’s practices.”
Drs Boyd and Knight outline recommendations to address the perceived problems. They believe that some form of independent ethical oversight of PHPs should be considered, along with a formal appeals process and a nationwide system for licensing and periodic auditing. They also call on specialty organizations such as the American Society of Addiction Medicine “to review PHP practices and recommend national standards that can be debated by all physicians, not just those who work within PHPs.”
Story Source:
The above post is reprinted from materials provided by Wolters Kluwer Health. Note: Materials may be edited for content and length.
THURSDAY — September 10th: 1st hour > The Myth of America’s Unaccountable Judiciary
GUEST: Attorney Zena Crenshaw-Logal*, Executive Director of The Law Project @www.njcdlp.org
2nd hour: Are Ethics An Occupational Hazard?
GUESTS: Zena Crenshaw-Logal; Dr. Andrew D. Jackson, Deputy Director of The Law Project (TLP); Dr. Sandra Nunn, TLP Board Member as well as CFO and Business Ethics Expert; Dr. Jill Jones-Soderman, TLP Board Member and Executive of The Foundation for Child Victims of the Family Courts @ http://www.fcvfc.org/ and Dr. Michael Langan, TLP Board Member and Author of “Disrupted Physician” @ http://disruptedphysician.com/blog/
Physician Health Programs (PHP) claimed “gold standard” for addiction treatment. “80% success rate” being used to promote “new paradigm” to other populations.
PHPs are essentially Employee Assistance Programs (EAPs) for doctors. The vast majority of people know little or nothing about Physician Health Programs (PHPs).
Physician Health Programs (PHPs) are being called the “gold-standard” for EAPs. Claims of unparalleled success are being used to promote PHPs to other populations as a “replicable model of recovery.”
Drs. Robert Dupont and Gregory Skipper are promoting PHPs as “A New Paradigm for Long-Term Recovery” claiming an 80% success rate in doctors.
Before the 2012 Drug and Alcohol Testing Industry Association (DATIA) annual conference, former Nixon Drug Czar Dr. Robert Dupont delivered a speech entitled “Drug Testing and the Future of American Drug Policy.” Dupont describes a “New Paradigm” for substance abuse treatment that enforces “zero tolerance for alcohol and drug use” enforced by monitoring with frequent random drug and alcohol tests in which positive tests are “met with swift, certain, but not draconian, consequences.” The paradigm is based on the current Physician Health Programs blueprint. Dupont states:
“…physician health programs , have set the standard for effective use of drug testing. These pioneering state programs provide services to health care professionals with substance use disorders. The programs are run by physicians, some of whom in recovery themselves. PHPs feature relatively brief but highly focused treatment followed by active lifelong participation in the 12-step fellowships of Alcoholics Anonymous and Narcotics…
“The belief that there are such things as witches is so essential a part of the faith that obstinately to maintain the opposite opinion manifestly savors of heresy.”
So begins Malleus Maleficarum , a witch hunters manual published in 1486 that launched a new paradigm for all those concerned with the identification and extirpation of witches. Used as a judicial case-book the Malleus set forth definitions of witchcraft, rules of evidence and the canonical procedures by which suspected witches were tortured and put to death. Written by Inquisitors for Inquisitor, the Malleus construct came to be regarded as irrefutable truth and contributed to the identification and execution of as many as 60,000 “witches”, predominantly women. The 29th and last edition was published in 1669.
Because of the nature of the enemy the evidentiary standard was lowered and any witness, no matter what his credentials, could testify against the accused.Using the nebulous “witch label” anyone with a grudge or suspicion could accuse anyone of witchcraft.
From the 15th century through the early 17th century a confederacy of “authorities” calling themselves “demonologists” existed and made money off the misery of others
Identification of witches was detailed in the Malleus including both physical and behavioral clues. Physical signs included things such as bushy eyebrows and thin lips. The Malleus declared that witches have a “Devil’s mark (stigmata diaboli) or Devils seal (sigilum diaboli) which was usually a scar, birthmark, or blemish. An extra nipple (polythelia) was a tell-tale sign. Behavioral manifestations included living alone, cultivating strange herbs in the garden, public singing or dancing and saying hello to a neighbors cat.
Physician oversight of witch persecution was standard. So too was the involvement of “witch-prickers” who were able to provide their expertise and “medical” testing in the assessment and diagnosis of the witch. Pricking them with needles, awes, and bodkins to prove they were indeed nefarious and non-human was a surefire way to line one’s pockets but for the pedophiles and pervs there was an added bonus—a thorough searching for that stigmata diaboli on someone else’s dime.
Through the witch trials clerics, doctors, and lawyers used their expertise as witnesses to increase their prestige. Witch hunts developed into a means of economic profit. Some gained a lot of money from the witch trials. The witch or her relatives paid for the salaries of those who worked the witch trials including judges, court officials, torturers, physicians, clergymen, scribes, guards, attendants.Even the people who made the stakes and scaffolds for executions gained from the conviction and death of each witch.
“Witch hunting,” wrote the historian Rossell Hope Robbins, “was self-sustaining and became a major trade, employing many people, all battening on the savings of the victims.” The costs of a witch trial were usually paid for by the estate of the accused or their family.
.And what my friend Laura Tompkin’s describes here in no different; except in place of “demonologists” we now have “addictionologists.” Both faulty paradigms with a lot of people making money hand over fist.
In 1592 Father Cornelius Loos wrote:“Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.”




 The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).
The Boston Collaborative Drug Surveillance Program found digoxin to be the second most commonly implicated drug in causing death in hospitalized patients and the most commonly implicated drug implicated in hospital admissions (N Engl J Med 291:824–828, 1974).

 In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG.
In addition to an up to date medication list we decided to put in the bare but essential elements of the medical record that would be needed in an emergency; these consisted of demographics, emergency contacts, a basic problem list, allergies and a baseline EKG. They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file.
They don’t see the problem and they don’t see a need for a solution. Many believe it is the patient’s responsibility to keep track of their medications and that any problem associated with not providing their medication list up to date were self-inflicted.” He said it will be a different story in five or ten years when the problem is acknowledged and accepted by the rank and file. The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.
The problem of not recognizing problems as problems can also be applied to individuals; Bill Cosby comes to mind. So too does FSPHP self-appointed drug-testing expert Dr. Gregory Skipper whose irresponsible introduction of junk-science drug testing into the marketplace through a loophole has undoubtedly caused many more deaths than Dr. Harold Shipman who killed more than 250 patients in the U.K. by injecting them with morphine.